
Abstract
Diabetes mellitus is a serious health problem that affects over 350 million individuals worldwide. Diabetic retinopathy (DR), which is the most common microvascular complication of diabetes, is the leading cause of new cases of blindness in working-aged adults. Diabetic macular edema (DME) is an advanced, vision-limiting complication of DR that affects nearly 30% of patients who have had diabetes for at least 20 years and is responsible for much of the vision loss due to DR. The historic standard of care for DME has been macular laser photocoagulation, which has been shown to stabilize vision and reduce the rate of further vision loss by 50%; however, macular laser leads to significant vision recovery in only 15% of treated patients. Mechanisms contributing to the microvascular damage in DR and DME include the direct toxic effects of hyperglycemia, sustained alterations in cell signaling pathways, and chronic microvascular inflammation with leukocyte-mediated injury. Chronic retinal microvascular damage results in elevation of intraocular levels of vascular endothelial growth factor A (VEGF), a potent, diffusible, endothelial-specific mitogen that mediates many important physiologic processes, including but not limited to the development and permeability of the vasculature. The identification of VEGF as an important pathophysiologic mediator of DME suggested that anti-VEGF therapy delivered to the eye might lead to improved visual outcomes in this disease. To date, four different inhibitors of VEGF, each administered by intraocular injection, have been tested in prospective, randomized phase II or phase III clinical trials in patients with DME. The results from these trials demonstrate that treatment with anti-VEGF agents results in substantially improved visual and anatomic outcomes compared with laser photocoagulation, and avoid the ocular side effects associated with laser treatment. Thus, anti-VEGF therapy has become the preferred treatment option for the management of DME in many patients.
Keywords
Epidemiology, socioeconomic burden and natural history of diabetic retinopathy and diabetic macular edema
Diabetes epidemic
Diabetes mellitus is a global health problem associated with serious long-term micro- and macrovascular complications and premature death [Centers for Disease Control and Prevention, 2011; International Diabetes Federation, 2011]. In 2011, an estimated 366 million individuals worldwide had diabetes [International Diabetes Federation, 2011], and by 2030, this number is expected to increase to 552 million [International Diabetes Federation, 2011]. According to 2010 estimates, diabetes is the seventh leading cause of death in the USA [Murphy et al. 2012], and affects approximately 25.8 million Americans or 8.3% of the population [Centers for Disease Control and Prevention, 2011]. An additional 79 million American adults aged 20 years and over are considered prediabetic based on fasting blood glucose or hemoglobin A1c levels [Centers for Disease Control and Prevention, 2011]. The estimated total cost of diabetes in the USA was US$245 billion in 2012; US$176 billion (72%) was associated with direct medical costs, while US$69 billion (28%) was attributable to indirect costs (e.g. work-related absenteeism, chronic disability leading to unemployment, and premature mortality) [American Diabetes Association, 2013]. The estimated worldwide healthcare cost attributable to diabetes is projected to total at least US$490 billion in 2030 [Zhang et al. 2010a].
Diabetic retinopathy (DR) is the most common microvascular complication of type 1 and type 2 diabetes [Fong et al. 2004; American Diabetes Association, 2012], and is more prevalent in patients who have had diabetes for a longer duration [American Diabetes Association, 2012]. In the USA, DR is the leading cause of incident blindness in working-aged adults aged 20−74 years [Centers for Disease Control and Prevention, 2011]. An estimated 28.5% of Americans with diabetes aged over 40 years have DR and one in 12 patients with diabetes has advanced vision-threatening DR [Kempen et al. 2004; Centers for Disease Control and Prevention, 2011]. A nationally representative sample of adults in the USA with diabetes aged 40 years and over participating in the National Health and Nutrition Examination Survey found that the prevalence of DR and vision-threatening DR is especially high among racial/ethnic minorities, particularly non-Hispanic black individuals [Zhang et al. 2010b]. The World Health Organization has identified DR as a priority eye disease with respect to the prevention of blindness and visual impairment in industrialized countries [World Health Organization, 2010].
Diabetic macular edema (DME) is an advanced, vision-limiting manifestation of DR in which swelling of the central retina causes loss of central vision [Frank, 2004; Johnson, 2009]. The Wisconsin Epidemiologic Study found that the prevalence of DME increases from 0−3% in recently diagnosed individuals to 28−29% in those living with type 1 or 2 diabetes for at least 20 years [Klein et al. 1984]. The long-term incidence of DME (over a 10-year period) in the Wisconsin study was highest (25.4%) in older-onset patients (diagnosed with diabetes at ≥30 years of age) with type 2 diabetes who required insulin and lowest (13.9%) in older-onset patients with type 2 diabetes who did not take insulin [Klein et al. 1995].
The microvascular complications associated with DR and DME are thought to be caused by chronic hyperglycemia, which results in damage to, and dysfunction of, capillary endothelial cells located in the retina, as well as the other metabolic abnormalities common in diabetes, such as diabetic dyslipidemia, hypertension, and vascular inflammation [Bloomgarden, 2007; Morello, 2007]. Over time, ongoing microvascular damage triggers a well defined succession of pathogenic events in the retina, including capillary nonperfusion and inner retinal ischemia, upregulation of vascular endothelial growth factor A (VEGF), macular edema, and retinal neovascularization; these events can cause loss of vision and, eventually, blindness [Burditt et al. 1968; Kohner, 1972; 1991; Morello, 2007; American Academy of Ophthalmology, 2008].
Pathogenesis and natural history of diabetic retinopathy
DR is classified into several stages based on the level of disease severity (Figures 1 and 2) [Ulbig and Hamilton, 1993; American Academy of Ophthalmology, 2008]. Preretinopathy is characterized by hemodynamic changes and vascular permeability with no apparent retinopathy on clinical examination [Ulbig and Hamilton, 1993; American Academy of Ophthalmology, 2008]. Mild nonproliferative DR (NPDR) is characterized by the appearance of microaneurysms, which at moderate stages can develop into intraretinal microvascular abnormalities (IRMAs), intraretinal hemorrhages, and cotton-wool spots, which represent focal infarcts of the retinal nerve fiber layer [Ulbig and Hamilton, 1993; American Academy of Ophthalmology, 2008]. Increased permeability of the retinal vasculature can lead to retinal edema and the formation of protein and lipid-rich deposits, referred to as hard exudates [American Academy of Ophthalmology, 2008]. In severe NPDR, the retinal vasculature gradually closes, which impairs perfusion and leads to retinal ischemia, characterized by venous caliber abnormalities, IRMAs (essentially, neovascularization within the retina), and widespread vascular leakage [Kempen et al. 2004; American Academy of Ophthalmology, 2008]. Neovascularization on the surface of the retina, optic nerve, and other structures (such as the iris, in severe cases) characterizes the most advanced stage of DR, known as proliferative DR (PDR; Figure 2) [Morello, 2007]. The abnormal new vessels are fragile and can bleed into the vitreous, causing sudden loss of vision. In some cases, spontaneous contraction of the retinal neovascular membranes detaches the retina from its support structures, a condition known as tractional retinal detachment [Morello, 2007]. Although surgery can be performed to attempt to reattach the retina, vision loss in such cases is frequently significant and irreversible.

Fundus photographs of a normal retina and a retina with diabetic retinopathy. (a) Normal eye anatomy. (b) Fundus photograph of a normal retina. (c) Fundus photograph of a patient with mild proliferative diabetic retinopathy. Arrow indicates area of neovascularization at baseline. Fundus photographs provided by the University of Wisconsin Fundus Photograph Reading Center.

Pathogenesis of diabetic retinopathy (DR). BM, Bruch’s membrane; CH, choroid; DR, diabetic retinopathy; GL, ganglion layer; INL, inner nuclear layer; IPL, inner plexiform layer; NF, optic nerve fibers; ONL, outer nuclear layer; OPL, outer plexiform layer; PDR, proliferative diabetic retinopathy; RA, retinal artery; RC, rods and cones; RPE, retinal pigment epithelium; RV, retinal vein.
Pathogenesis of diabetic macular edema: role of vascular endothelial growth factor
The microvascular injury discussed previously may lead to retinal vascular leakage with accumulation of excess extracellular fluid manifested as DME [Miller et al. 2012]. While the molecular pathogenesis of DME is not fully elucidated, it appears that VEGF plays a critical role. VEGF is a potent, diffusible, endothelial-specific mitogen typically found as a homodimer with a molecular weight of approximately 45 kDa [Miller et al. 2012]. It mediates many important physiologic processes (Figure 3), including the development and maintenance of the vasculature [Ferrera et al. 2003], regulation of blood coagulation and vascular tone through the production of nitric oxide and prostacyclin I2 [He et al. 1999], regulation of the podocytes necessary for glomerular filtration by the kidneys [Eremina et al. 2003], and maintenance of integrity of epithelial cell layers during normal wound repair [Nissen et al. 1998].
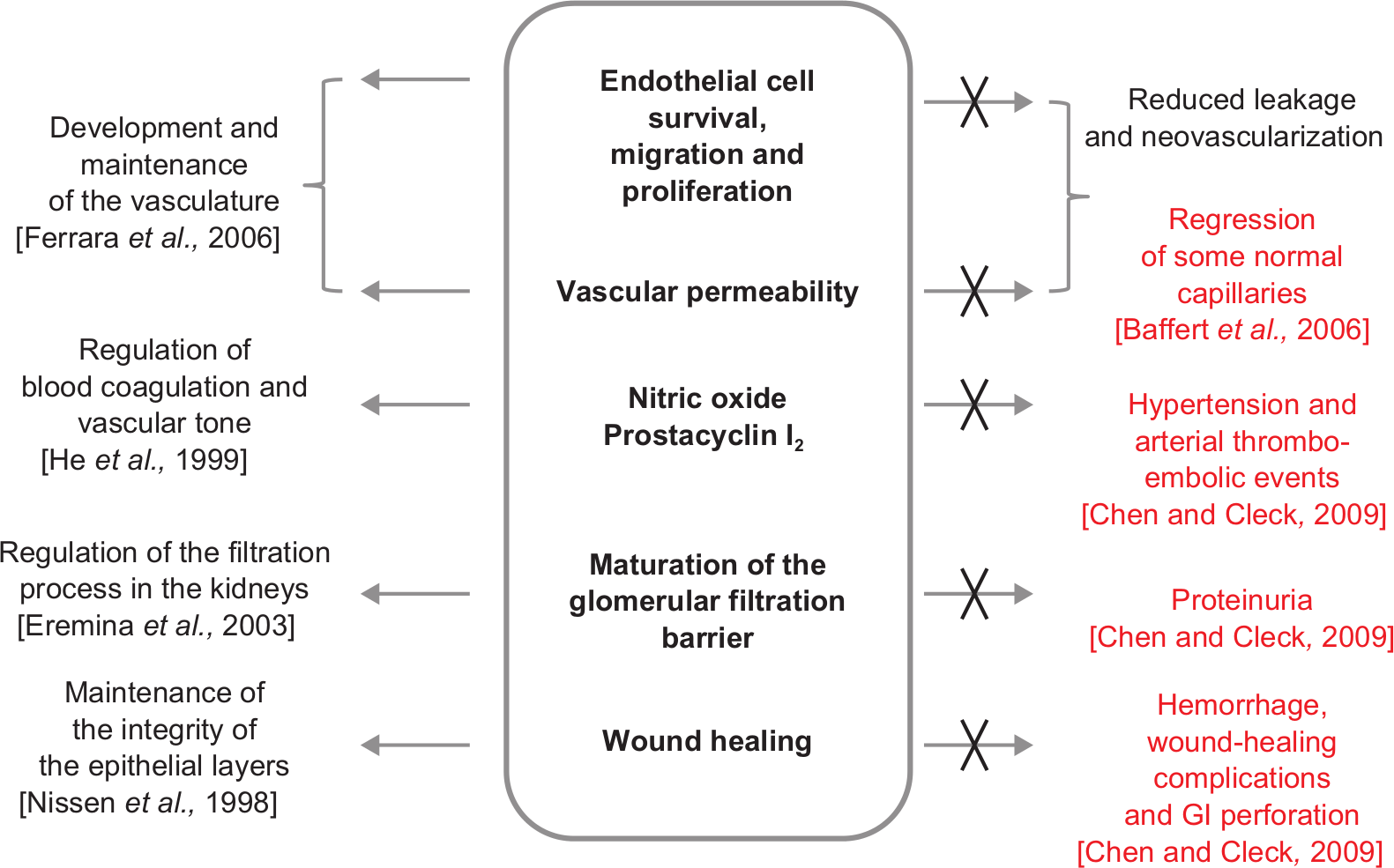
Physiology of vascular endothelial growth factor inhibition. GI, gastrointestinal.
The human VEGF family comprises five related glycoproteins: VEGF-A (commonly known as VEGF), VEGF-B, VEGF-C, VEGF-D and placental growth factor [Ferrera et al. 2003, 2006; Papadopoulos et al. 2012; Stewart, 2012]. VEGF-A is the best characterized, and is mainly responsible for the angiogenic and vasopermeability activities in adults [Papadopoulos et al. 2012; Stewart, 2012]. Alternative splicing and/or proteolytic cleavage of the eight-exon VEGF-A gene gives rise to four main VEGF-A isoforms: VEGF121, VEGF165 (which appears to be the most abundant), VEGF189, and VEGF206 [Ferrera et al. 2003; Miller et al. 2012; Stewart, 2012]. All VEGF family members signal through three trans-membrane tyrosine kinase receptors (VEGFRs): VEGFR-1, VEGFR-2, and VEGFR-3 [Ferrera et al. 2003; Papadopoulos et al. 2012; Stewart, 2012]. Most of the mitogenic, angiogenic and vascular-hyperpermeability responses to VEGF-A are mediated through VEGFR-2, which is expressed by the vascular endothelium [Miller et al. 2012]. Neuropilin 1, an isoform-specific receptor for VEGF165, is widely expressed in human adult tissues and has been demonstrated to promote the binding of VEGF165 to VEGFR-2 [Miller et al. 2012].
In patients with diabetes, chronic hyperglycemia leads to the upregulation of VEGF, resulting in angiogenesis, increased vascular permeability, and the production of proinflammatory cytokines (e.g. intracellular adhesion molecule 1 and tumor necrosis factor α) [Stewart, 2012]. Thickening of the basement membrane and pericyte loss, which are key hallmarks of DR, as well as sheer stress on endothelial cells, may further stimulate VEGF production [Stewart, 2012]. DME occurs when the retinal circulation deteriorates as a result of DR and the resultant ischemia, together with the breakdown of the blood–retinal barrier, leads to extravascular accumulation of serum resulting in macular thickening (Figure 4) [Do et al. 2012; Stewart, 2012]. DME is considered clinically significant (CSME) if it involves or threatens to spread to the center of the macula, the portion of the retina responsible for sharp, central vision [Early Treatment Diabetic Retinopathy Study Research Group, 1985; Ryan, 2007].

Pathogenesis of diabetic macular edema. ICAM, intercellular adhesion molecule; PKC, protein kinase C; VEGF, vascular endothelial growth factor.
Data supporting the key role of vascular endothelial growth factor in diabetic retinopathy and diabetic macular edema
VEGF and its receptors, VEGFR-1 and VEGFR-2, are constitutively expressed in normal vascularized intraocular tissues, including the conjunctiva, iris, retina, and choroid-retinal pigment epithelium (RPE) complex [Kim et al. 1999]. In vitro and in situ studies have demonstrated that human RPE cells can synthesize and secrete VEGF [Adamis et al. 1993], and VEGF is upregulated in human RPE cells in response to hypoxia [Shima et al. 1995]. In multiple nonhuman primate models of ocular angiogenesis, VEGF expression is associated temporally and spatially with development of intraocular neovascularization [Miller et al. 1994]. In addition, injections of recombinant human VEGF165 into the vitreous of a nonhuman primate are sufficient to produce intraocular neovascularization [Tolentino et al. 1996], while inhibition of VEGF by intravitreal administration of a neutralizing anti-VEGF monoclonal antibody [Adamis et al. 1996] or antigen binding fragment [Krzystolik et al. 2002] prevents neovascularization in this nonhuman primate model.
Intraocular levels of VEGF are elevated in patients with DR and DME. A study evaluating undiluted vitreous samples from 20 eyes of 20 patients (8 with PDR, 12 with other conditions requiring vitrectomy) found that VEGF levels were significantly higher (p = 0.006) in the eyes of patients with PDR compared with the eyes of patients without PDR [Adamis et al. 1994]. Furthermore, the vitreous concentrations of VEGF in patients with PDR were considered to be physiologically relevant and most likely produced by retinal ischemia [Adamis et al. 1994]. In a comparative, cross-sectional study of undiluted aqueous humor samples taken from 54 eyes of 54 patients with DME undergoing cataract surgery, the aqueous levels of VEGF were significantly (p < 0.001) associated with the severity of DME [Funatsu et al. 2002]. These results demonstrate that VEGF is produced in the intraocular tissues of patients with diabetes and is involved in the pathogenesis of DME [Funatsu et al. 2002].
Management of diabetic retinopathy and diabetic macular edema
Management of blood sugar levels, blood pressure, and blood lipids
Intensive glycemic control, blood pressure control, and blood lipid level control are widely accepted ways to reduce the risk of DME [Diabetic Retinopathy Clinical Research Network, 2008]. This concept was illustrated in the Steno-2 study, in which intensive management of hyperglycemia, hypertension, dyslipidemia, and microalbuminaria, together with secondary prevention of cardiovascular disease, significantly reduced the risk of developing DR compared with conventional treatment in accordance with national guidelines (hazard ratio 0.42; 95% confidence interval 0.21−0.86) [Gaede et al. 2003]. The importance of hyperglycemia as a risk factor for DR has been demonstrated in an analysis of the Diabetes Prevention Program cohort [Diabetes Prevention Program Research Group, 2007]. In this analysis, 7.9% of patients with elevated fasting glucose and impaired glucose tolerance, and no known history of diabetes developed retinopathy consistent with DR. Among patients with new-onset diabetes (< 3 years in duration), the prevalence of DR was significantly higher at 12.6%. The results from this analysis suggest that retinopathy may occur over a wide range of glucose levels, even in the absence of a diagnosis of diabetes [Diabetes Prevention Program Research Group, 2007]. The importance of strict glucose control was further demonstrated in the 9-year multicenter, randomized Diabetes Control and Complications Trial (DCCT), which found that maintaining near-normal blood glucose levels substantially reduced the risk of DR development or progression in patients with type 1 diabetes compared with conventional therapy [Diabetes Control and Complications Trial Research Group, 1995]. Follow up of the DCCT cohort showed that intensive insulin therapy was associated with a significantly lower incidence of DR progression compared with conventional treatment, and these benefits were maintained for 10 years [White et al. 2008].
Controlling hyperglycemia in patients with type 2 diabetes is also associated with slowing DR progression, as has been demonstrated in the UK Prospective Diabetes Study (UKPDS) [UK Prospective Diabetes Study (UKPDS) Group, 1998a]. This randomized, controlled clinical trial in which a sulfonylurea or insulin was used to tightly control blood glucose levels (< 108 mg/dl) in 3,867 patients with newly-diagnosed type 2 diabetes showed that both agents decreased the risk of microvascular complications [UK Prospective Diabetes Study Group, 1998a]. A subset of these patients with diabetes who also had hypertension (n = 1148) were randomized to receive the antihypertensive agents captopril or atenolol [UK Prospective Diabetes Study Group, 1998b]. Tight blood pressure regulation (< 150/85 mmHg) with either agent resulted in clinically meaningful reductions in the risk of DR progression by at least two-step progression from baseline [34% reduction (p = 0.004) by a median of 7.5 years of follow up] and a 47% reduction (p = 0.004) in the risk of worsening visual acuity by 15 letters (three lines) on the Early Treatment of Diabetic Retinopathy Study (ETDRS) eye chart (Figure 5) at 9 years of follow up [UK Prospective Diabetes Study Group, 1998b].

Standard ETDRS chart: example of 15-letter gain (three lines on the ETDRS chart) and 20/40 BCVA Snellen equivalent (minimum driving vision). BCVA, best-corrected visual acuity; ETDRS, Early Treatment Diabetic Retinopathy Study.
Focal/grid laser photocoagulation
Historically, the primary technique used to treat vision-threatening complications of DR was laser photocoagulation surgery [Bloomgarden, 2007; American Academy of Ophthalmology, 2008]. Panretinal (scatter) photocoagulation (PRP), which is one type of laser treatment that places laser burns at the back of the eye to the peripheral retina to promote the regression of abnormal blood vessels, is the current standard of care for PDR [Bloomgarden, 2007; American Academy of Ophthalmology, 2008]. PRP and vitrectomy have been shown to improve the oxygenation of the inner retina [Stefánsson, 2001], and the efficacy of PRP in the treatment of intraocular neovascularization has been studied extensively. Data from large prospective randomized clinical trials support the use of these techniques in the treatment of neovascularization associated with PDR [Diabetic Retinopathy Vitrectomy Study Research Group, 1985, 1988; Diabetic Retinopathy Study Research Group, 1987]. While PRP reduces the rate of severe vision loss by 50% [Diabetic Retinopathy Study Research Group, 1987], the technique is associated with adverse effects due to the destructive nature of laser photocoagulation; these include peripheral visual field loss, abnormal color and night vision, and reduced central acuity from exacerbation of concomitant DME [Early Treatment Diabetic Retinopathy Study Research Group, 1991; American Academy of Ophthalmology, 2008].
Macular (focal/grid) photocoagulation has typically been used to manage DME; the exact mechanism by which macular laser has an effect remains poorly understood. The ETDRS randomized trial established focal/grid photocoagulation as the standard of care treatment by demonstrating that patients with clinically significant DME treated with macular laser experienced a 50% reduction in moderate vision loss after 3 years compared with untreated patients [Early Treatment Diabetic Retinopathy Study Research Group, 1985]. Patients treated with laser in this study also had an increased chance of gaining vision, and a decreased frequency of persistent DME compared with their untreated counterparts. However, less than 3% of patients treated with laser therapy experienced vision improvement of 15 letters from baseline, or three lines on the ETDRS eye chart [Early Treatment Diabetic Retinopathy Study Research Group, 1985]. While randomized, multicenter trials have demonstrated significant improvements in best-corrected visual acuity (BCVA) in eyes with center-involved DME and visual acuity (VA) up to 20/32 (Snellen equivalent) after laser treatment, these improvements tended to occur slowly (i.e. over a 2-year period) [Diabetic Retinopathy Clinical Research Network, 2008; Elman et al. 2011]. Although laser photocoagulation can reduce the risk of further vision loss in patients with DME, the procedure may also cause macular scarring over time with repeated treatment [Bloomgarden, 2007; Ryan, 2007].
Corticosteroids
The pathophysiology of DME provides a rationale for the use of treatments designed to counter anti-inflammatory and anti-VEGF effects within the retina. Intraocular corticosteroids have been evaluated for the treatment of DME because they have anti-inflammatory properties and have been shown to inhibit both VEGF and VEGF gene expression [Diabetic Retinopathy Clinical Research Network, 2008; Stewart, 2012]. Intravitreal administration of triamcinolone (off label) has been shown to reduce DME and improve vision [Stewart, 2012]; however, in randomized, prospective trials, this agent has not demonstrated better outcomes in patients with DME compared with laser photocoagulation [Diabetic Retinopathy Clinical Research Network, 2008; Elman et al. 2010].
Sustained delivery systems releasing either dexamethasone (DEX) (Ozurdex, DEX intravitreal implant, Allergan, Inc., Irvine, CA, USA) or fluocinolone acetonide (FA) (Iluvien, FA intravitreal implant, Alimera Sciences, Alpharetta, GA, USA) have also been, and continue to be, evaluated [Campochiaro et al. 2011, 2012; Callanan et al. 2013]. The Ozurdex DEX implant is a biodegradable copolymer that is placed in the vitreous cavity by intravitreal injection and releases DEX gradually for up to 6 months [Callanan et al. 2013]. The DEX implant is approved by the US Food and Drug Administration (FDA) for the treatment of macular edema following branch or central retinal vein occlusion (RVO) and for the treatment of noninfectious posterior segment uveitis (Ozurdex package insert). In the phase II PLACID trial, patients with diffuse DME experienced similar visual improvements (≥10 letters; two lines on the ETDRS chart) from baseline at month 12 whether treated with the DEX implant plus laser or sham implant plus laser [Callanan et al. 2013]. However, elevations of intraocular pressure and cataract-related adverse events (AEs) were more common in the DEX plus laser treatment group compared with sham.
The FA implant is a nonbiodegradable cylindrical polymide tube that is injected into the vitreous cavity and releases FA gradually for up to 3 years [Campochiaro et al. 2011, 2012; Alimera Sciences, 2013]. Iluvien is available in the UK for use in patients with chronic DME whose condition is considered refractory to existing therapies; however, it is not currently approved by the US FDA for this indication [Alimera Sciences, 2013]. In the phase III FAME study, a higher proportion of patients with persistent DME who were treated with the FA implant experienced vision improvements of at least 15 letters from baseline (three lines on the ETDRS chart) at month 24 [Campochiaro et al. 2011] and month 36 [Campochiaro et al. 2012] compared with patients receiving sham injection. However, serious AEs (SAEs), including cataract surgery, increased intraocular pressure, and glaucoma requiring incisional surgery, were more frequent in patients receiving the FA insert compared with sham treatment [Campochiaro et al. 2011, 2012]. Because of the AEs associated with corticosteroids, they are not routinely used for the treatment of DME in most patients at this time.
Inhibitors of vascular endothelial growth factor signaling
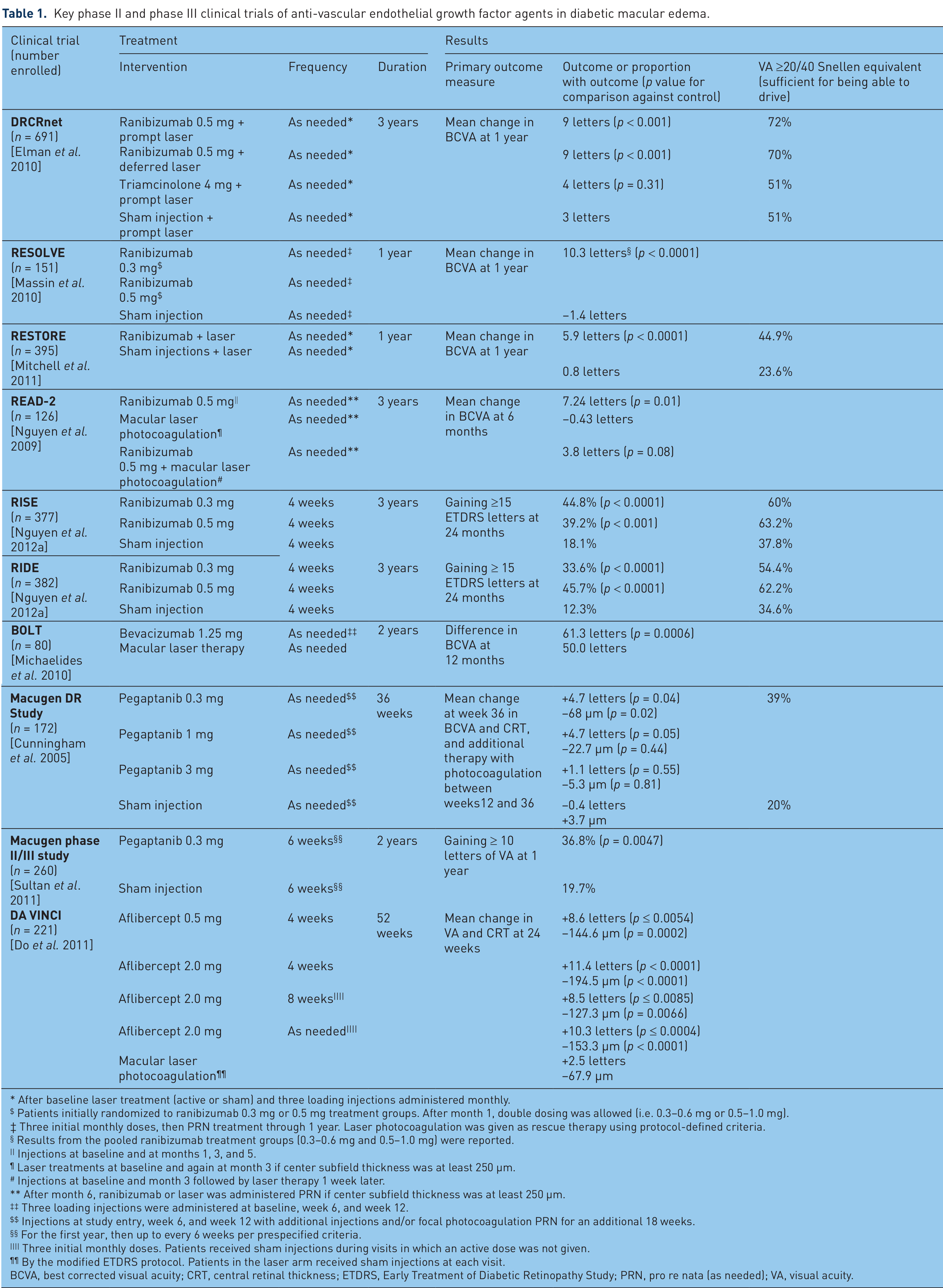
VEGF inhibitors have been shown to significantly improve vision and restore retinal anatomy in many patients [Nguyen et al. 2012a]. Additionally, an exploratory (post hoc) analysis suggests that VEGF inhibitors may also prevent or slow the further worsening of DR in many patients with DME [Ip et al. 2012]. Four anti-VEGF drugs, administered by intravitreal injection, have been tested in prospective, randomized clinical trials in adult patients (aged ≥ 18 years) with type 1 or type 2 diabetes (Table 1).
Key phase II and phase III clinical trials of anti-vascular endothelial growth factor agents in diabetic macular edema.
After baseline laser treatment (active or sham) and three loading injections administered monthly.
Patients initially randomized to ranibizumab 0.3 mg or 0.5 mg treatment groups. After month 1, double dosing was allowed (i.e. 0.3–0.6 mg or 0.5–1.0 mg).
Three initial monthly doses, then PRN treatment through 1 year. Laser photocoagulation was given as rescue therapy using protocol-defined criteria.
Results from the pooled ranibizumab treatment groups (0.3−0.6 mg and 0.5−1.0 mg) were reported.
Injections at baseline and at months 1, 3, and 5.
Laser treatments at baseline and again at month 3 if center subfield thickness was at least 250 µm.
Injections at baseline and month 3 followed by laser therapy 1 week later.
After month 6, ranibizumab or laser was administered PRN if center subfield thickness was at least 250 µm.
Three loading injections were administered at baseline, week 6, and week 12.
Injections at study entry, week 6, and week 12 with additional injections and/or focal photocoagulation PRN for an additional 18 weeks.
For the first year, then up to every 6 weeks per prespecified criteria.
Three initial monthly doses. Patients received sham injections during visits in which an active dose was not given.
By the modified ETDRS protocol. Patients in the laser arm received sham injections at each visit.
BCVA, best corrected visual acuity; CRT, central retinal thickness; ETDRS, Early Treatment of Diabetic Retinopathy Study; PRN, pro re nata (as needed); VA, visual acuity.
Ranibizumab (Lucentis, Genentech, Inc., South San Francisco, CA, USA) is currently approved by the US FDA for the treatment of neovascular age-related macular degeneration (wet AMD), macular edema secondary to RVO, and DME (Lucentis package insert). It is the only VEGF inhibitor approved for the treatment of DME. Ranibizumab is a 48 kDa humanized monoclonal anti-VEGF antigen binding fragment specifically designed and manufactured for use in the eye [Ferrara et al. 2006; Yu et al. 2011] (Lucentis package insert). Amino acid substitutions in the complementarity-determining region (i.e. the antigen-binding site) of ranibizumab enhanced its binding affinity to VEGF-A isoforms [Ferrara et al. 2006]. The ranibizumab molecule also lacks a Fc region, which allows for shorter systemic circulation and faster clearance [Ferrara et al. 2006]. Ranibizumab potently inhibits the biologic activity of all known isoforms of VEGF [Ferrara et al. 2006; Yu et al. 2011].
Bevacizumab (Avastin, Genentech, Inc.) is a 149 kDa, full-length, recombinant, humanized monoclonal anti-VEGF antibody that binds all isoforms of VEGF-A [Ferrara et al. 2006; Stewart, 2012]. Bevacizumab is neither designed nor manufactured for use in the eye; however, it is used off label, by intravitreal injection, for the treatment of intraocular vascular diseases, including wet AMD, RVO, and DME [Stewart, 2012].
Pegaptanib sodium injection (Macugen, OSI Eyetech, Inc., Cedar Knolls, NJ, USA) is a 28-base RNA aptamer covalently linked to two branched 20 kDa polyethylene glycol moieties (molecular weight of ~50 kDa) that binds potently and specifically to VEGF165 [Gragoudas et al. 2004] (Macugen package insert) Pegaptanib is approved for the treatment of wet AMD by the US FDA (Macugen package insert).
Aflibercept (Eylea, Regeneron Pharmaceuticals, Inc., Tarrytown, NY, USA) is a 115 kDa recombinant fusion protein consisting of portions of the human VEGFR-1 and VEGFR-2 fused to the Fc domain of human immunoglobulin G1 domain [Holash et al. 2002] (Eylea package insert). Aflibercept binds all isoforms of VEGF-A, VEGF-B, and placental growth factor [Holash et al. 2002; Papadopoulos et al. 2012]. The drug is currently approved in the USA and Europe for the treatment of wet AMD and macular edema following central RVO (Eylea package insert; http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/002392/WC500135815.pdf).
Investigational agents targeting pathways beyond vascular endothelial growth factor
Although beyond the scope of this review, it is worth noting that many of the novel therapeutics for DME offer alternative entry points into pathways promoting angiogenesis and vascular permeability, and may complement existing anti-VEGF therapies to further improve vision. Ongoing, early clinical trials are investigating therapeutic agents with a variety of targets, such as a kinase downstream of multiple growth factors (including VEGF) [Afzal et al. 2007] [ClinicalTrials.gov identifier: NCT01565148], a suppressor of a vascular endothelial receptor tyrosine kinase [Moss, 2013] [ClinicalTrials.gov identifier: NCT01702441], a hypoxia-induced activator of a cellular stress pathway [Nguyen et al. 2012b] [ClinicalTrials.gov identifier: NCT01445899], integrins that mediate cell adhesion [Santulli et al. 2008] [ClinicalTrials.gov identifier: NCT01749891], and steroid hormone receptors that regulate endothelial cell permeability [Thomas et al. 2012] [ClinicalTrials.gov identifier: NCT01821677].
Key clinical trials of intravitreal anti-vascular endothelial growth factor inhibitors in diabetic macular edema
Assessment of efficacy
Assessments of efficacy in key clinical trials of ranibizumab, bevacizumab, pegaptanib, and aflibercept for the management of DME typically measure changes in a patient’s ability to distinguish detail (VA), measured using the standardized ETDRS eye chart (Figure 5). The most common measure used is BCVA, which corresponds to the best possible VA achieved using corrective lenses. Improved BCVA is indicated by the ability to distinguish individual letters in the rows further down the eye chart.
Common VA-based measures of clinical efficacy used in these studies include mean change from baseline in BCVA, clinically significant BCVA gain of at least 15 letters (three lines) based on the ETDRS eye chart, achievement of a Snellen equivalent of 20/40 or better (Figure 5), and maintenance of vision (i.e. loss of <15 ETDRS letters). An improvement of at least 15 letters on the ETDRS eye chart is considered clinically significant and has also been shown to correlate with clinically meaningful improvements in patient-perceived visual function as measured by the National Eye Institute standardized Visual Function Questionnaire (NEI VFQ-25) [Suñer et al. 2009]. Similarly, achievement or maintenance of a Snellen equivalent of 20/40 or better has important quality of life implications, as this is the minimum requirement (in at least one eye) for a driver’s license in most states in the USA [Steinkuller, 2010]. The change in retinal thickness from baseline measured by optical coherence tomography (OCT) is also commonly used to assess efficacy, as reductions in central retinal thickness (CRT) indicate resolution of macular edema (Figure 6).

Retinal thickness measured by optical coherence tomography. CFT, central foveal thickness (mean thickness at the point of intersection of six radial scans) on the OCT; FT, foveal thickness (mean thickness in the central 1000 μm diameter area); OCT, optical coherence tomography. Images provided by the University of Wisconsin Fundus Photograph Reading Center.
Review of efficacy findings
Ranibizumab
Several prospective clinical studies in patients with DME, including READ-2, RESOLVE, RESTORE, DRCR.net Protocol I, and RISE/RIDE have demonstrated that intravitreal ranibizumab reduces macular edema and sustainably improves vision in this patient population (Table 1) [Nguyen et al. 2009, 2010, 2012a, Elman et al. 2010, 2011, 2012; Massin et al. 2010; Mitchell et al. 2011; Do et al. 2013]. In several of these studies, ranibizumab was found to be significantly superior to macular laser therapy [Nguyen et al. 2009, 2010; Elman et al. 2010, 2011; Mitchell et al. 2011].
In the Diabetic Retinopathy Clinical Research Network (DRCR.net) Protocol I phase III study, ranibizumab combined with prompt or deferred (by ≥24 weeks) focal/grid laser generated significantly greater mean changes from baseline in BCVA after months 12 and 24 than laser alone or combined with corticosteroid (triamcinolone) (Table 1) [Elman et al. 2010, 2011]. These vision gains were generally maintained at month 36 in ranibizumab-treated patients, although prompt laser treatment provided no added benefit, and possibly worsened visual outcomes over time compared with deferred laser treatment [Elman et al. 2012]. Similarly, in the 12-month, phase III RESTORE study there was a significantly greater mean change in BCVA from baseline at month 12 for ranibizumab treatment alone or combined with laser therapy compared with laser monotherapy (Table 1) [Mitchell et al. 2011]. A significantly greater percentage of patients achieved a Snellen equivalent of 20/40 or better in the ranibizumab groups compared with laser alone, and demonstrated significantly greater reductions from baseline in CRT. Patients in the two ranibizumab groups also reported better health-related quality of life changes from baseline at month 12 versus laser alone, as assessed by the NEI VFQ-25 [Mitchell et al. 2011].
More recently, two parallel, methodologically identical, 3-year phase III clinical trials (RISE and RIDE) compared monthly ranibizumab 0.3 mg and 0.5 mg with sham injection [Nguyen et al. 2012a]. In both studies, significantly more ranibizumab-treated patients gained at least 15 letters from baseline at month 24 compared with the sham-treated group, and the percentage of patients achieving a Snellen equivalent of 20/40 or better was also significantly greater in ranibizumab-treated patients at month 24 versus sham (Table 1) [Nguyen et al. 2012a]. Macular edema was also significantly improved on time-domain OCT compared with sham treatment, while retinopathy was less likely to worsen and more likely to improve. Ranibizumab-treated patients also required significantly fewer macular laser procedures than sham-treated patients [Nguyen et al. 2012a]. The importance of early treatment with ranibizumab was highlighted at the month 36 endpoint of the RISE and RIDE trials, in which lesser BCVA gains were observed in patients who crossed over from sham to ranibizumab 0.5 mg after month 24 compared with the vision gains observed in patients who had been randomized to receive ranibizumab from the beginning of the studies [Brown et al. 2013].
Bevacizumab
Intravitreal bevacizumab has been compared to modified ETDRS macular laser therapy in 80 patients (80 eyes) with center-involved CSME in a 2-year single-center study (BOLT) [Michaelides et al. 2010; Rajendram et al. 2012]. Mean BCVA at month 12 (the primary endpoint) was significantly better in the group receiving bevacizumab compared with the macular laser-treated group (Table 1). Bevacizumab-treated patients also gained significantly more letters and had 5.1 times higher odds of gaining at least 10 letters (two lines on the ETDRS chart) over the 12-month study period compared with the macular laser arm [Michaelides et al. 2010]. There was also a greater reduction in central macular thickness at month 12 in the bevacizumab group, although this was not statistically significant [Michaelides et al. 2010]. The visual and anatomic improvements seen with bevacizumab treatment were maintained at 24 months [Rajendram et al. 2012].
Pegaptanib
In the 36-week, phase II, dose-ranging Macugen DR study, patients with diabetes with center-involved DME who received pegaptanib 0.3 mg every 6 weeks for a minimum of three injections had a significantly better gain in BCVA from baseline at 36 weeks compared with sham-injected controls and a significantly greater reduction in mean CRT compared with baseline (Table 1) [Cunningham et al. 2005]. However, while both the percentage of patients who gained at least 15 letters in BCVA at week 36 and the percentage of patients achieving a VA of 20/40 or better were numerically higher in the pegaptanib 0.3 mg group compared with sham-injected patients, these results were not statistically significant. Patients who received the pegaptanib 1.0 or 3.0 mg doses showed no statistically significant improvements versus the sham-treated group (Table 1) [Cunningham et al. 2005]. In a 2-year phase II/III clinical trial in 260 patients comparing pegaptanib 0.3 mg every 6 weeks with sham treatment, significantly more pegaptanib-treated patients gained at least 10 letters in BCVA compared with sham (Table 1), although there was no significant difference between the two groups in the percentage of patients with at least a 15-letter BCVA gain [Sultan et al. 2011]. After 102 weeks, change in BCVA from baseline was significantly greater in the pegaptanib group, while significantly fewer patients treated with pegaptanib required salvage grid laser photocoagulation at weeks 54 and 102 [Sultan et al. 2011].
Aflibercept
An exploratory study demonstrated that a single intravitreal injection of aflibercept improved VA and reduced retinal thickness in five patients with DME [Do et al. 2009]. More recently, four different doses and dosing regimens of intravitreal aflibercept were evaluated versus focal/grid laser photocoagulation in eyes with center-involved DME in the 1-year, phase II DA VINCI study (Table 1) [Do et al. 2011, 2012]. After 6 months of treatment, the mean change from baseline in BCVA was significantly greater in all the aflibercept dose groups compared with laser-treated patients (Table 1), as was the change from baseline in CRT [Do et al. 2011]. These benefits were maintained to 12 months [Do et al. 2012]. However, while the percentage of patients treated with aflibercept who gained at least 15 letters from baseline was numerically superior compared with laser, this difference was not significant at either 6 or 12 months [Do et al. 2011].
Two phase III, similarly designed, randomized, double-masked, active control studies of aflibercept for DME (VIVID-DME and VISTA-DME) are currently ongoing and the 1-year results were recently reported [ClinicalTrials.gov identifier: NCT01331681, NCT01783886; Regeneron, 2013]. In these studies, patients received either aflibercept 2.0 mg monthly or every 2 months following five monthly loading doses, or laser photocoagulation [Regeneron, 2013]. After 1 year of treatment, the mean change from baseline in BCVA was significantly greater with either aflibercept regimen compared with laser treatment alone [Regeneron, 2013].
Review of safety findings
All currently available ocular anti-VEGF treatments are administered via intravitreal injection. Effective treatment generally requires repeated injections over a prolonged period (months to years), leading to the potential for ocular complications. Commonly reported ocular AEs include endophthalmitis (which is usually a result of the injection procedure), subconjunctival hemorrhage, increased intraocular pressure, and intraocular inflammation. However, data from clinical trials to date indicate that ocular AE rates in patients treated with anti-VEGF agents are generally low and comparable to sham treatment, with most AEs being mild or moderate and self-limiting [Cunningham et al. 2005; Nguyen et al. 2009, 2012a; Elman et al. 2010, 2011, 2012; Massin et al. 2010; Michaelides et al. 2010; Do et al. 2011, 2012; Sultan et al. 2011; Rajendram et al. 2012; Brown et al. 2013]. The reported rates of ocular SAEs are also low [Cunningham et al. 2005; Nguyen et al. 2009, 2012a; Elman et al. 2010, 2011, 2012; Massin et al. 2010; Michaelides et al. 2010; Do et al. 2011, 2012; Sultan et al. 2011; Rajendram et al. 2012; Brown et al. 2013]. Furthermore, in patients with DME, rates of procedure-related complications are to a certain extent balanced by decreased rates of VEGF-mediated ocular complications of diabetes, such as proliferative retinopathy, vitreous hemorrhage, and neovascular glaucoma [Ip et al. 2012]. Patients with diabetes are more susceptible to systemic infections, so a potentially increased rate of endophthalmitis was a concern when DME studies were initiated; however, endophthalmitis has been reported infrequently, and at per-injection rates of around 0.05%/injection, were identical to those seen with intravitreal injections of anti-VEGF agents for wet AMD [Cunningham et al. 2005; Nguyen et al. 2009, 2012a; Elman et al. 2010, 2011, 2012; Massin et al. 2010; Michaelides et al. 2010; Do et al. 2011, 2012; Sultan et al. 2011; Rajendram et al. 2012; Brown et al. 2013].
The use of intravenous VEGF inhibitors in patients with various forms of cancer suggests that systemic inhibition of VEGF signaling may be associated with various AEs, including regression of some normal capillaries [Baffert et al. 2006], as well as hypertension and arterial thromboembolic events (myocardial infarction and cerebrovascular accidents), proteinuria, hemorrhage, wound-healing complications, and gastrointestinal perforation [Chen and Cleck, 2009]. Patients with DME are typically at higher risk of myocardial infarction and cerebrovascular accidents than patients with diabetes without DME [Hirai et al. 2008]. However, in general, rates of these categories of AEs were low in patients with DME treated with intravitreal anti-VEGFs, although the rates of AEs potentially related to systemic VEGF inhibition were higher in patients treated with intravitreal anti-VEGF than in sham-treated patients [Cunningham et al. 2005; Do et al. 2011; Sultan et al. 2011; Nguyen et al. 2012a; Brown et al. 2013].
A benefit–risk analysis of pooled 36-month efficacy and safety data from the RISE and RIDE trials in which patients were treated with intravitreal ranibizumab monthly for 36 months found both the ranibizumab 0.3 mg dose (approved by the US FDA; Lucentis package insert) and the 0.5 mg dose (approved by the European Medicines Agency) [European Medicines Agency, 2013] to be comparably effective [Brown et al. 2013]. Both doses demonstrated an acceptable overall risk–benefit profile; however, the incidence of several categories of AEs potentially related to systemic VEGF inhibition were higher in the 0.5 mg group compared with the 0.3 mg group [Brown et al. 2013]. The incidences of SAEs potentially related to systemic VEGF inhibition in the ranibizumab 0.3 mg and 0.5 mg groups, and the sham group through 24 months of treatment were 5.6%, 11.9%, and 10.6% in RISE and 9.6%, 5.6%, and 9.4% in RIDE respectively [Nguyen et al. 2012a]. The US product labeling for ranibizumab includes appropriate warnings and precautions regarding the rates of these events in patients with DME (Lucentis package insert).
An important question is the comparative efficacy, intraocular safety, and systemic safety of the three most commonly used anti-VEGF agents for DME because these molecules differ in design, potency of VEGF inhibition, and systemic exposure when administered intravitreally. The safety profiles of ranibizumab and bevacizumab in wet AMD have been directly compared in three major randomized trials [Martin et al. 2011, 2012; Chakravarthy et al. 2012; Krebs et al. 2013], and in large-scale analyses of Medicare claims databases [Gower et al. 2011; Curtis et al. 2012]. In the CATT trial, patients treated with bevacizumab experienced a significantly higher rate of SAEs through 2 years of follow up compared with patients treated with ranibizumab: 234/586 (39.9%) versus 190/599 (31.7%) respectively, p = 0.004 [Martin et al. 2011, 2012]. Data from the IVAN trial indicate that bevacizumab suppresses systemic VEGF levels to a greater extent than ranibizumab [Chakravarthy et al. 2012]. However, there is uncertainty whether such suppression has any link to the rates of SAEs. An ongoing, independent DRCR.net comparative effectiveness study will compare the efficacy and safety of intravitreal ranibizumab, bevacizumab, and aflibercept in patients with DME [ClinicalTrials.gov identifier: NCT01627249].
Summary of efficacy and safety findings
Taken together, the results from these key clinical trials in patients with DME demonstrate that intravitreal anti-VEGF inhibitors improve visual and anatomic outcomes better than the historic standard of care (i.e. macular laser) and represent an effective treatment option for the management of DME. Currently, ranibizumab is the only VEGF inhibitor approved by the US FDA and the European Medicines Agency for the treatment of DME.
Importance of screening, patient education, and compliance in the detection and management of diabetic retinopathy and diabetic macular edema
DR is often asymptomatic until vision loss develops [Bragge et al. 2011; Bursell et al. 2012]. Therefore, early referral to an eye care provider is critically important for preserving the vision of patients with diabetes. The American Diabetes Association recommends that patients with type 1 diabetes receive their first dilated and comprehensive eye examination performed by an ophthalmologist or optometrist within 5 years after diabetes onset, with yearly follow up thereafter [American Diabetes Association, 2012]. For patients with type 2 diabetes, the first dilated and comprehensive eye examination should take place shortly after diagnosis, with exams repeated annually thereafter [American Diabetes Association, 2012]. Follow-up exams can occur less frequently (every 2−3 years) following at least one normal exam, but are required more often if retinopathy is progressing [American Diabetes Association, 2012]. In particular, recent screening data from the UK suggest that patients with established DR in both eyes may worsen at higher rates compared with other patients and may require particularly close follow up [Stratton et al. 2012]. However, despite these guidelines, it is estimated that nearly 50% of patients with diabetes do not receive eye examinations on a regular basis [Bursell et al. 2012].
The detection and management of DR and DME requires prompt and effective communication and cooperation between primary care physicians, diabetologists, and ophthalmologists [Haas et al. 2012]. It also requires that healthcare providers educate their patients with diabetes about the need for annual preventative care (e.g. eye, foot, and dental examinations), which is effective in reducing the risk of diabetes-related complications, including vision loss [Bragge et al. 2011; American Diabetes Association, 2012; Yuen, 2012]. However, a recently published survey of patients with type 2 diabetes found that nearly 30% of respondents (44/147) had not received a dilated eye examination in the past year; approximately 23% of these individuals (10/44) were unaware that a dilated eye exam was recommended [Crosby and Shuman, 2011]. A separate study conducted by the Joslin Vision Network to evaluate patient awareness of their DR and timeliness of follow up (n = 2795) demonstrated that over 82% of patients with DR and over 78% of patients with vision-threatening DR did not know they had retinopathy despite continued eye care [Soliman et al. 2011].
Educating patients about the need for annual preventative care does increase patient compliance. A study among adults with diabetes (n = 253) found that patients were 4.3 times more likely to have an eye examination in the past 12 months if a healthcare professional recommended that they have their eyes checked once a year (p < 0.05) [Yuen, 2012]. Prevention programs geared toward improving eye care for patients with diabetes have been shown to result in substantial cost savings to the US federal budget and to help reduce the economic burden to society [Javitt and Aiello, 1996].
Conclusion
The previous standard of care for patients with DME has focused on the prevention of further deterioration in vision using macular laser once some degree of loss has already occurred, with very few patients experiencing any subsequent gains in vision. Studies of the pathophysiology of DME demonstrate a crucial role for VEGF in disease development and this has led to successful clinical trials of VEGF inhibitors. Data from several large, prospective randomized clinical trials indicate that, on average, intraocular inhibition of VEGF is associated with rapid resolution of DME (as indicated by reduction of the thickness of the retina) and significant VA gains, better than those achieved with focal/grid laser photocoagulation, demonstrating that the focus of treatment should be on improvements in vision and not the prevention of further worsening. Prior studies showed the importance of early diagnosis and treatment of clinically significant edema with laser and this remains the case with the new treatments that are being developed. Therefore, to ensure that patients who have vision loss as a result of diabetes have the best possible VA outcomes, it is important that they are promptly referred to an ophthalmologist (preferably a retina specialist) for diagnosis and appropriate treatment. In an era when new treatments are available for DME, it is crucial for all patients with diabetes mellitus to be appropriately screened for DR in order to prevent vision loss and to identify those at risk of losing vision.
Footnotes
Acknowledgements
Support for third-party writing assistance for this manuscript, furnished by Michelle Kelly, PhD, CMPP, of Envision Scientific Solutions, was provided by Genentech, Inc.
Funding
This work was supported by Genentech, Inc.
Conflict of interest statement
David S. Boyer: consultant (Alcon, Allegro, Allergan, Eyetech, Genentech, Inc., Novartis/QLT, Neurotech, Ohr, Pfizer, Regeneron), speakers bureau (Alcon, Allergan, Genentech, Inc., Pfizer), clinical research projects (Alcon, Allergan, Genentech, Inc., Pfizer, Regeneron); J. Jill Hopkins, Jonathan Sorof, and Jason S. Ehrlich are employees of Genentech, Inc., a member of the Roche Group, and hold equity and/or options in Roche.