
Abstract
Objective:
This study aimed to investigate the recurrence patterns of diffuse large B-cell lymphoma (DLBCL) and assess the significance of clinical manifestation consistency at the time of recurrence.
Methods:
A total of 141 patients who were newly diagnosed with DLBCL between January 2015 and October 2024 and who initially achieved complete remission but eventually developed relapsed disease during follow-up were retrospectively identified, their recurrence circumstances were assessed, and their clinical manifestations at diagnosis and recurrence were compared. The timing of recurrence was categorized as within 1 year of postchemotherapy or later.
Results:
A total of 113 (80.1%) patients presented with clinical manifestations leading to the diagnosis of recurrence. A total of 87 (61.7%) patients presented similar clinical manifestations at recurrence to those observed during initial diagnosis. Importantly, for patients who relapsed within 1 year of chemotherapy, those with inconsistent manifestations at recurrence had significantly poorer prognoses and lower survival rates (complete remission (CR) rate, 7.4%; 1-year overall survival (OS), 37.5%; 1-year progression-free survival (PFS), 18.5%) than those with consistent manifestations (CR rate, 20.8%; 1-year OS, 34.0%; 1-year PFS, 22.6%; PFS, p = 0.046; OS, p = 0.049). In contrast, for patients whose recurrence occurred more than 1 year postchemotherapy, consistent manifestations were associated with better survival outcomes (CR rate, 44.1%; 1-year OS, 61.8%; 1-year PFS, 52.9%).
Conclusion:
The timing of recurrence and the consistency of clinical manifestations are important factors influencing the prognosis of DLBCL. Specifically, early recurrence with inconsistent manifestations is associated with worse outcomes, whereas recurrence with consistent manifestations 1 year postchemotherapy is correlated with an improved prognosis.
Introduction
Diffuse large B-cell lymphoma (DLBCL) is the most common type of non-Hodgkin lymphoma, accounting for 30%–40% of all cases.1,2 Combined immunochemotherapy is the cornerstone of management and consists of the anti-CD20 antibody rituximab (R) combined with cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP) (7;1), which results in long-term remission in 60%–70% of patients. 3 Despite improvements in cure rates for patients with DLBCL, up to 40% of patients relapse, mostly within 18 months of treatment. 4 Regular follow-up appointments are crucial for detecting recurrences early, when interventions may be more effective and potentially lead to better outcomes.5,6
Current guidelines recommend clinical review every 3 months for the first 2 years after treatment, every 6 months for the following 3 years, and annually thereafter. 7 Routine CT,6,8 Positron Emission Tomography-Computed Tomography (PET/CT)9,10 or B-mode ultrasound is not recommended during follow-up. There remains no consensus on the most suitable approach for postremission surveillance. Medical history, a physical examination, and blood tests, including complete blood count (CBC), serum chemistry, and lactate dehydrogenase (LDH) evaluations, were performed during every regular follow-up visit. However, the guidelines for medical history and physical examination are somewhat ambiguous. DLBCL is a heterogeneous disease characterized by a wide array of pathological morphologies and clinical manifestations, 11 which often lead to poor reproducibility among different patients. Consequently, it is challenging to ascertain which symptoms and physical signs are indicative of DLBCL recurrence. Therefore, this study aimed to systematically investigate the clinical symptoms experienced by DLBCL patients at the time of recurrence, focusing on the relationship between symptom consistency and the timing of relapse. We hope to enhance the understanding of DLBCL recurrence and provide insights that may improve follow-up strategies and clinical management for affected individuals.
Patients and methods
We conducted a retrospective review of patients with DLBCL who were diagnosed and regularly followed up at the First Affiliated Hospital of Wenzhou Medical University. Data collection was conducted in compliance with institutional ethics requirements. From January 2015 to October 2024, we identified 1047 histologically confirmed de novo DLBCL patients who were treated with frontline R-CHOP (or R-CHOP-like) therapy at our institution, which was approved by the Institutional Review Board of the First Affiliated Hospital of Wenzhou Medical University and performed in accordance with the principles of the Declaration of Helsinki. This is a retrospective study, so the requirement for written informed consent was waived. Following a clinicopathologic review, 141 DLBCL patients with histologically confirmed DLBCL (WHO 2016 criteria) with complete diagnostic workup including (a) immunohistochemistry, (b) Baseline PET/CT or contrast-enhanced CT staging, (c) Received at least three cycles of frontline R-CHOP or equivalent therapy who achieved a CR after initial chemotherapy (which was confirmed by CT scans or PET/CT scans) and subsequently experienced relapse during the follow-up period were included in the current analysis. Documented first relapse with (a) histologic confirmation when feasible, (b) radiologic progression meeting Lugano 2014 criteria, (c) complete relapse evaluation including clinical symptom documentation, (d) minimum 12 months follow-up postrelapse unless death occurred earlier. Patients with transformation from indolent lymphoma, primary refractory disease (progressed during frontline therapy), concurrent active malignancies, insufficient clinical documentation at either diagnosis or relapse, HIV-associated lymphoma, and posttransplant lymphoproliferative disorders were excluded from the study.
For each patient, we collected baseline characteristics, including sex, performance status, age, chief complaints, and physical signs, as well as laboratory data such as serum LDH levels, the number of extranodal sites, the international prognostic index (IPI) score, primary therapy received, results of CT scans or PET/CT imaging, and bone marrow aspiration and biopsy findings. The follow-up data included the date and site of relapse, chief complaints, physical signs at the time of relapse, biopsy results, imaging results from CT scans or PET/CT scans, and the cause and date of death.
Clinical manifestations include both symptoms and physical signs. Symptoms may include lymphadenopathy, fever, night sweats, weight loss, fatigue, abdominal pain or distension, cough or shortness of breath, and itching (NCCN lymphoma assessment guidelines). Physical signs include lymphadenopathy, splenomegaly, hepatomegaly, and skin changes (National Comprehensive Cancer Network (NCCN) lymphoma assessment guidelines). “Symptom consistency” refers to the presence of the same chief complaints in the same system at the time of diagnosis and relapse, whereas “symptom inconsistency” indicates different chief complaints especially in different system at these time points. “Physical sign consistency” means that lymphoma infiltrated the same system, whereas “physical sign inconsistency” means that different systems were infiltrated between the two time points. For cases where relapse was detected radiologically during routine surveillance in the absence of any new symptoms (asymptomatic relapse), these were systematically categorized as “inconsistent manifestation.” This classification was chosen because the clinical presentation (asymptomatic) differed from the initial symptomatic presentation at diagnosis. Overall, “clinical manifestation consistency” refers to either symptom consistency, physical sign consistency, or both. All physical examinations in this study were performed by a core team of Haige Ye and Shujuan Zhou experienced hematologists following standardized protocols to minimize interobserver variability. Key findings (e.g., lymphadenopathy, organomegaly) were further verified by imaging or biopsy when clinically indicated, reducing reliance on subjective assessment alone.
Patients were evaluated weekly for their response during chemotherapy. Weekly evaluations included symptom assessment, physical examination, and complete blood counts, with imaging reserved for suspected progression or protocol-specified timepoints. Following treatment, evaluations were conducted every 3 months for the first 2 years, every 6 months for the subsequent 3 years, and annually thereafter, in accordance with institutional policy, to monitor for potential relapse of DLBCL. During each regular follow-up visit, CT scans of the area of initial tumor involvement were performed, with or without additional scans of the chest, abdomen, or pelvis. The decision to conduct PET/CT or B-mode ultrasound was based on the physician’s discretion. Each visit also included a review of the medical history, a physical examination, and blood tests encompassing CBC, serum chemistry, and LDH levels. For patients at risk of relapse or progression of DLBCL, additional imaging, including FDG-PET/CT and/or CT scans of other areas, was employed. Relapse determination incorporated both clinical context and diagnostic findings. For patients presenting with new symptoms, relapse required: (a) Biopsy confirmation when feasible or (b) Radiologic progression (PET/CT) correlating anatomically with symptoms. For asymptomatic patients with abnormal surveillance scans, relapse is required: (a) Histologic confirmation or (b) PET-avidity (Deauville 4–5) plus subsequent clinical progression within 3 months.
The response and relapse criteria were as defined according to a previous publication. 12 Complete response (CR) reflect best achieved response to first salvage therapy, assessed using Lugano 2014 criteria (including PET/CT confirmation when available). Overall survival (OS) was defined as the time from relapse to death from any cause. Progression-free survival (PFS) was defined as the time from relapse to progression. OS and PFS were calculated via the Kaplan–Meier method, and survival curves were compared via the log-rank test. Categorical data were compared via chi-square analysis. All analyses were performed with SPSS software (version 13.0; SPSS Inc., Chicago, IL, USA). Each value was two-sided, and p values <0.05 were considered to indicate statistical significance.
Results
Patient characteristics and pattern of relapse
A total of 141 patients who achieved a CR after initial chemotherapy and subsequently experienced relapse during the follow-up period were included in the study. The median age of the patients was 61 years (range, 25–86 years), and the male-to-female distribution was 80:61. The main characteristics of the patients at diagnosis are summarized in Table 1. Advanced-stage disease (Ann Arbor stage III or IV) was observed in 84 patients (59.6%), and extranodal involvement was noted in 100 patients (70.9%), including bone marrow infiltration in 27 patients (19.1%). Elevated serum LDH levels were present in 50.4% of patients. According to the IPI, the distribution was as follows: 49 low-risk patients (34.8%), 32 low/intermediate-risk patients (22.7%), 27 high/intermediate-risk patients (19.1%), and 33 high-risk patients (23.4%). The initial immunochemotherapy regimen was R-CHOP for 120 patients (85.1%), infusional dose-adjusted rituximab, etoposide, prednisone, vincristine, cyclophosphamide, and doxorubicin (DA-R-EPOCH) regimen for eight patients (5.7%), and other therapies (due to the presence of high-risk factors) for 13 patients (9.2%).
Patient characteristics at diagnosis and follow-up.

Other therapies for 13 patients appear in Supplemental File.
66.6% (n = 94) of patients showed concordant LDH status (elevated/normal) at both diagnosis and relapse, using institutional upper limits of normal (ULN: 250 U/L).
CT, computed tomography; DA-R-EPOCH dose-adjusted rituximab, etoposide, prednisone, vincristine, cyclophosphamide and doxorubicin; ECOG, Eastern Cooperative Oncology Group; GCB, germinal center B cell; IPI, international prognostic index; LDH, lactate dehydrogenase; PET, positron emission tomography; R-CHOP, rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone.
Relapse was detected clinically in 113 patients (80.1%) with symptoms, the clinical characteristics at initial diagnosis and relapse, including detailed symptoms and physical signs, are summarized in Table 2. In contrast, subclinical relapse was identified via PET-CT 7 patients (5%), CT in 12 patients (8.5%), and B-mode ultrasound in 8 patients (5.7%); only 1 patient (0.7%) had a relapse detected through blood tests. The median time to relapse was 9 months after completing chemotherapy, and 71.6% of relapses occurred within 2 years. No significant difference was observed in the median relapse time between patients with consistent and inconsistent clinical presentations (8 months vs 11 months, respectively; p = 0.183). Relapse (<12 months) occurred in 55.5% of inconsistent vs 60.9% of consistent presentations (χ² p = 0.529).
Clinical symptoms and signs at diagnosis and at relapse.

Recurrence manifestation consistency
Among the patients included in this study, a significant proportion (61.7%) presented consistent clinical manifestations before and after recurrence, either in terms of symptoms, physical signs, or both. Specifically, 41.8% of patients reported identical symptoms before and after relapse, whereas 53.1% demonstrated consistent physical signs. Additionally, 66.6% of the patients had matching LDH levels between initial diagnosis and relapse (Table 1). We were particularly interested in identifying which patients might exhibit altered clinical manifestations after relapse. However, our analysis did not reveal any significant relationships between inconsistent clinical manifestations and patient characteristics, such as the primary site of origin, Ann Arbor stage, IPI score, number of extranodal involvements, LDH levels, or other factors (Table 3).
Patient characteristics and consistency.

The total N = 141 (87 consistent + 54 inconsistent) includes: 113 clinically detected relapses (classified by symptom patterns) 28 asymptomatic relapses (automatically inconsistent).
Other therapy include Polatuzumab, Glofitamab, radiotherapy, and CAR-T.
CR rates reflect best achieved response to first salvage therapy, assessed using Lugano 2014 criteria (including PET/CT confirmation when available).
ASCT, autologous stem cell transplant; CR, complete remission; ECOG, Eastern Cooperative Oncology Group; IPI, international prognostic index; LDH, lactate dehydrogenase.
Manifestation consistency and prognosis
The most clinically significant finding of our study was the prognostic impact of recurrence manifestation consistency, with patients demonstrating consistent manifestations achieving superior outcomes across all measured parameters. Specifically, the consistent manifestation cohort exhibited a significantly higher complete response rate (35.6% vs 16.7%; p = 0.015), improved OS (2y-OS: 32.2% vs 18.5%; p = 0.041), and better PFS (2y-PFS: 29.9% vs 11.1%; p = 0.010) compared to those with inconsistent manifestations (Figure 1 and Table 4). This prognostic relationship was further modified by relapse timing, where early relapsers (⩽12 months) with inconsistent manifestations showed particularly dismal outcomes (CR: 7.4%; 1y-OS: 37.0%; 1y-PFS: 18.5%), while late-relapsing patients with consistent manifestations demonstrated the most favorable prognosis (CR: 44.1%; 1y-OS: 61.8%; 1y-PFS: 52.9%; Table 5; Figures 2 and 3). These findings collectively establish manifestation consistency as both a prognostic factor and a clinically useful stratification marker that interacts significantly with relapse timing.

Kaplan–Meier curve of PFS (a) and OS (b) according to manifestation consistent and inconsistent patients.
Consistency and prognosis.

CR, complete remission; PFS, progression-free survival; OS, overall survival.
Consistency and relapse time and prognosis.

CR, complete remission; OS, overall survival; PFS, progression-free survival.

Kaplan–Meier curve of PFS (a) and OS (b) according to early relapse and late relapse in manifestation inconsistent patients. Kaplan–Meier curve of PFS (c) and OS (d) according to early relapse and late relapse in manifestation consistent patients.
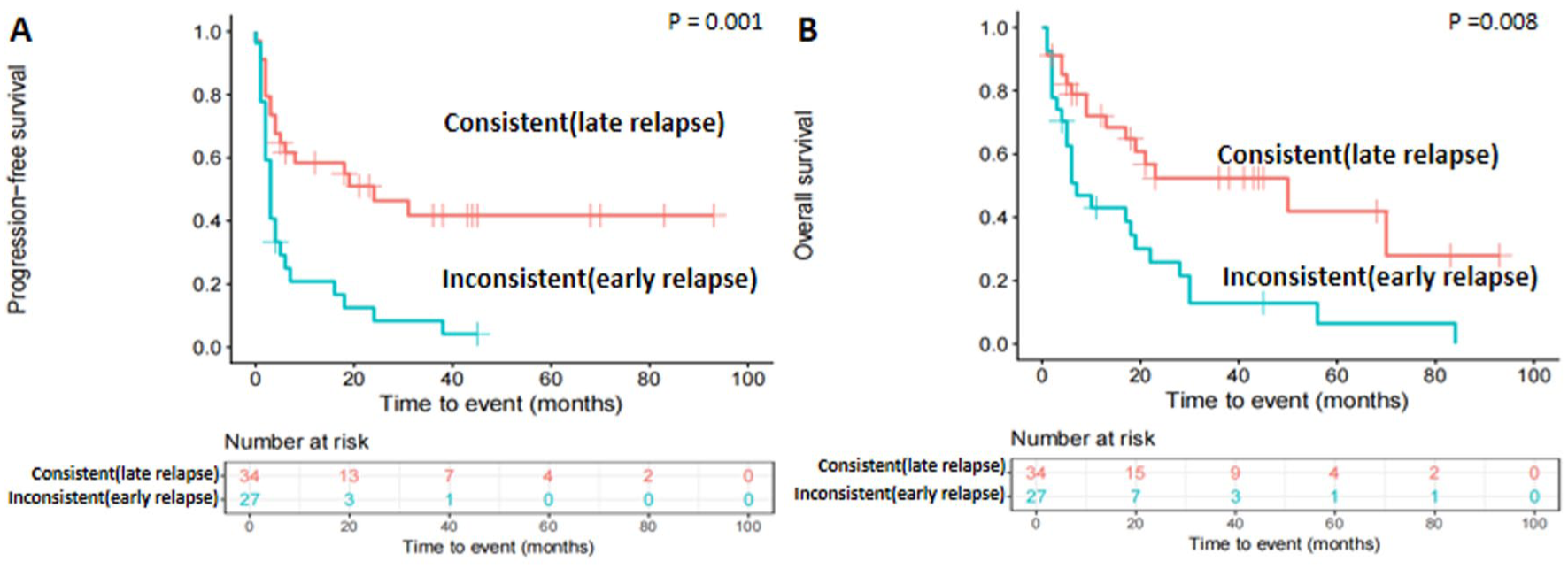
Kaplan–Meier curve of PFS (a) and OS (b) according to late relapse in manifestation consistent patients and early relapse in manifestation inconsistent patients.
Discussion
In our comparative analysis of clinical manifestations at the initial presentation and recurrence of DLBCL, we observed significant patterns that underscore the importance of clinical symptoms in tracking disease progression. Our findings indicate that a substantial number of patients are diagnosed with relapse, primarily due to the emergence of clinical symptoms rather than through routine imaging tests such as CT, PET/CT, or ultrasound or through laboratory examinations. Most of the symptoms and signs observed at the time of relapse were found to be consistent with those at initial presentation. This finding highlights the crucial roles that symptom awareness and timely reporting play in the detection of relapse.
Routine imaging tests such as CT, PET/CT, and ultrasound, as well as laboratory evaluations, in the follow-up of patients with DLBCL may not be as important for diagnosing relapse as traditionally thought. Our observations suggest that the majority of recurrence diagnoses are made on the basis of clinical symptoms reported by patients rather than through findings from these conventional imaging methods or laboratory tests. This reliance on patient-reported symptoms raises important questions about the utility of imaging and laboratory assessments in routine follow-up scenarios. While imaging modalities are essential for initial staging and assessing treatment response,13 –15 their role in the surveillance of recurrence may need reconsideration.5,8,16 –18 Additionally, the financial burden 6 and potential risks 19 associated with frequent imaging can lead to unnecessary stress for patients without significantly improving clinical outcomes. Our research findings are similar to those of Truong et al., 20 they found that the majority of the relapses were detected by patient-reported symptoms or physical examination, or both, as opposed to surveillance imaging (77.9% vs 22.1%, p < 0.0001). There was no OS difference between the two groups (p = 0.66). Surveillance PET/CT contributed to more than 75% of follow-up health care costs in the first 2 years of monitoring for relapse. The surveillance imaging group had one reported case of iatrogenic pneumothorax. Therefore, a more balanced approach that prioritizes clinical symptoms while still selectively utilizing imaging and laboratory tests may be more beneficial in the surveillance of DLBCL patients.
Although first salvage therapy after relapse of DLBCL affect patient prognosis, in our study, the overall treatment regimens were comparable between manifestation consistent and inconsistent patients. The consistency of symptoms between the initial presentation and recurrence of DLBCL has significant prognostic value. Our research revealed that patients who experienced recurrence within 1 year postchemotherapy and exhibited discrepancies between initial and recurrent symptoms were associated with poorer outcomes, decreased survival rates and reduced sensitivity to chemotherapy, which were confirmed by other studies. The CORAL and ORCHARRD studies,4,21 both demonstrated that patients with rel/ref DLBCL to first-line rituximab-containing chemoimmunotherapy (within 12 months) had a poor prognosis (3-year PFS rates: 23% and <20%, respectively). This phenomenon may suggest a biological shift in tumor behavior, reflecting an aggressive variant or the development of chemoresistance. The divergence in symptomatology could indicate an alteration in disease dynamics, possibly due to genetic mutations22 –24 or changes in the tumor microenvironment25,26 that render lymphoma less responsive to conventional treatments. Understanding these patterns is crucial, as they can guide therapeutic strategies and inform clinicians about the potential need for alternative treatment modalities or closer monitoring in patients exhibiting such as symptom discrepancies upon recurrence.
Conversely, patients who relapse more than 1 year postchemotherapy, particularly patients whose clinical manifestations are consistent with those at initial diagnosis, tend to have significantly better outcomes than those with early recurrence. Chen et al. 27 found that patients relapsing within 1 year showed an inferior risk profile at diagnosis. As expected, a worse OS was observed in the early relapse group. Multivariate analysis for OS showed that relapse within 1 year was an independent parameter for reduced OS (Hazard Ratio (HR) 0.241, p = 0.002). These patients exhibit higher CR rates to chemotherapy and extended OS. This correlation likely indicates that late relapses may reflect a less aggressive disease phenotype or a more indolent course, 28 allowing for a more effective therapeutic response. The consistency in symptoms may suggest a more stable tumor biology, which facilitates the maintenance of sensitivity treatments that were initially effective. 22 Understanding this relationship is crucial, as this information can guide clinicians in tailoring follow-up care and treatment strategies, emphasizing the importance of monitoring symptom patterns posttreatment.
Our comparative analysis of the clinical manifestations between the initial onset and recurrence of DLBCL yielded significant insights. However, it is important to acknowledge the limitations of our study. The retrospective nature inherently limits clinical consistency assessment, despite our standardization efforts. Prospective validation with structured symptom capture tools (e.g., PRO-CTCAE) would strengthen future studies. The sample size was determined by available cases rather than prospective power calculation while our post hoc analysis suggests adequate power to detect clinically meaningful differences, smaller effect sizes may have been missed. The observational design precludes causal inferences. While recurrence timing and symptom patterns are clinically useful indicators, their prognostic value should be interpreted in conjunction with molecular and pathological factors (e.g., cell-of-origin, MYC/BCL-2 alterations). Additionally, while our analysis highlights associations between symptom consistency and prognosis, it does not establish causality. Further research, including larger-scale studies and mechanistic investigations, is needed to validate our observations and elucidate the underlying biological mechanisms involved.
Conclusion
Our analysis of the clinical manifestations of newly diagnosed versus relapsed DLBCL revealed that most patients seek medical attention due to new symptoms and that relapse is diagnosed because of these symptoms rather than during routine imaging follow-up. Typically, relapse symptoms closely mirror those at diagnosis. The timing of recurrence and the consistency of clinical manifestations are critical factors influencing the prognosis of DLBCL. Specifically, early recurrence with inconsistent manifestations is associated with worse outcomes, whereas recurrence with consistent manifestations 1 year postchemotherapy is correlated with an improved prognosis. Early recognition of symptom patterns and individualized surveillance strategies may improve DLBCL outcomes, though further studies are needed to disentangle the relative contributions of clinical, biological, and treatment-related factors.
Supplemental Material
sj-docx-1-tah-10.1177_20406207251410405 – Supplemental material for The impact of clinical manifestations on the prognosis of diffuse large B-cell lymphoma
Supplemental material, sj-docx-1-tah-10.1177_20406207251410405 for The impact of clinical manifestations on the prognosis of diffuse large B-cell lymphoma by Siqian Wang, Xi Xu, Yongyong Ma, Shanhu Qian, Liyuan Tang, Lan Sun, Zhijian Shen, Haige Ye, Honglan Qian, Songfu Jiang and Shujuan Zhou in Therapeutic Advances in Hematology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.