
Abstract
Diffuse large B-cell lymphoma (DLBCL) is the most common adult non-Hodgkin lymphoma (NHL) and is highly invasive, with a poor prognosis. The main clinical treatment for DLBCL involves chemotherapy or a combination of chemotherapy and targeted drugs. CD56 expression is considered as an indicator of poor prognosis in patients with acute myeloid leukemia and anaplastic large cell lymphoma; however, its role in DLBCL remains unclear. We report on a patient with CD56-positive DLBCL/leukemia with BCL6/MYC double-hit, and DDX3X, LRP1B, SIN3A, and GNA13 gene mutations (stage IVA, prognostic index aaIPI = 2 points). The patient was treated with cyclophosphamide and prednisone pre-chemotherapy plus R-Hyper-CVAD AB and DA-EPOCH regimens. Lumbar puncture combined with intrathecal injection was performed to prevent central nervous system infiltration during hospitalization, and complete remission was confirmed. We also reviewed the literature to clarify the relevance of the unique clinical features associated with this case.
Introduction
Diffuse large B-cell lymphoma (DLBCL) is the most common adult non-Hodgkin lymphoma (NHL), and is highly invasive with a poor prognosis. CD56 is expressed on natural killer (NK) cells and on CD4 and CD8 T lymphocytes, and is considered as an indicator of a poor prognosis in patients with acute myeloid leukemia and anaplastic large cell lymphoma. However, the role of CD56 in DLBCL remains unclear, although a few studies indicating CD56-positive expression have indicated a poor prognosis. 1 Heterogeneous phenotype detection may help with the comprehensive diagnosis of the disease. However, whether CD56-positive DLBCL with BCL6/MYC(+) double-hit represents a rare new lymphoma subtype and its implications for patients’ long-term prognosis requires the investigation of more cases. We report on such a case, including the histopathological, bone marrow cell morphology, immunophenotypic features, and corresponding treatment outcomes, and conducted a review of the literature, to facilitate a better understanding of the unique clinical features of this case.
Case report
A 14-year-old male patient with a complaint of recurrent nasal congestion for 2 months and a swollen left neck for 10 days presented to his local hospital. He had no symptoms of fever, night sweats, or weight loss. However, he had a 2-month history of bilateral nasal congestion, especially in his left nostril, and suffered from right nasal bleeding without hemoptysis or sputum, which he and his family had ignored. About 1 month before he reported to the hospital, the patient suffered from low back pain of unknown cause extending to his right leg and gradually to other parts of his body. The intermittent occurrence of these symptoms prompted the patient to report initially to the Orthopedics Department at his local hospital. However, his symptoms were not resolved.
Ten days before the patient reported to his local hospital for a second visit, he incidentally detected a tender swelling on the left side of his neck, with headache and dizziness, but without fever, chills, or other symptoms. He was treated with antibiotics but his clinical signs and symptoms did not improve. The hospital then conducted nasopharyngeal magnetic resonance imaging (MRI) with enhancement and a left nasopharyngeal space-occupying lesion in the left neck, parapharyngeal space, and multiple enlarged lymph nodes were detected. The clinicians suspected lymphoma or nasopharyngeal cancer and therefore referred him to a tertiary hospital in Fujian Province for further treatment.
One week later, the patient attended the Outpatient Department at our hospital and was admitted to the Otorhinolaryngology Department with a suspected diagnosis of a nasopharyngeal tumor. Physical examination revealed the following: body temperature 36.9°C, conscious, visible left posterior wall of the nasopharynx with a smooth surface blocking the bilateral posterior nostrils, bilateral torus, and pharyngeal crypt, and pharyngeal mouth compression. The left pharynx was slightly swollen from the right side, the bilateral tonsils were swollen (grade II), the posterior pharynx was not congested, and no lymphoid follicles were detected. The bilateral piriform fossa was symmetrical with no effusion and the left submandibular area had multiple small, smooth lymph nodes. The remaining lymph nodes were not felt. A 3-cm × 4-cm tender mass with a smooth surface was detected in the left neck. No other clear abnormalities were detected on physical examination.
After admission, the patient received antibiotics, rehydration, nutritional support, and symptomatic treatment. He also underwent head, and cervical and lumbar spine MRI scans and was examined by an orthopedic surgeon and a hematologist. The MRI scans revealed the following: a spotted abnormal signal on the right side of the pons, suggesting demyelinating lesions; no obvious abnormalities in the cervical vertebrae and spinal canal; T12/L1 and S3 vertebral bone abnormalities, indicating possibility lymphoma bone marrow infiltration or other blood diseases; and nasopharyngeal and oropharyngeal mass, left parapharyngeal abscess, and posterior pharyngeal space with left neck space, indicating the possible presence of enlarged lymph nodes.
Further investigations were also carried out. Routine blood test results showed: white cell count 9.70 × 109/L, red cell count 4.15 × 1012/L, hemoglobin 120 g/L, platelets 449 × 109/L, and mean corpuscular volume 83.4 fL. Examination of his white blood cells revealed 78% lobular nuclei and 16% lymphocytes. Blood biochemistry analysis showed uric acid 477 µmol/L and lactate dehydrogenase 514 IU/L. Routine examination of the patient’s urine and stool, pre-transfusion screening and coagulation function analysis revealed no abnormalities. The results for Epstein–Barr virus (EBV) VCA IgA, EA IgA, and Rta IgG were all negative. Antinuclear antibody was weakly positive, anti-U1-Nrnp antibody was strongly positive, C-reactive protein was 19.3 mg/L, procalcitonin was 0.066 ng/L, and rubella virus IgG and cytomegalovirus IgG were positive. Laryngoscopy showed a large mass in the nasopharynx. An electrocardiogram showed normal results, pure-tone audiometry showed that both ears were generally normal, acoustic impedance indicated that the binaural tympanic curve was C. The right tibia was lateral, with no obvious abnormality. About 11 days after admission, peripheral blood cell morphology examination showed 1% rod-shaped nuclei, 71% lobulated nuclei, 20% mature lymphocytes, 6% mature monocytes, and 2% lymphoma cells. Conventional bone marrow examination showed 34.5% lymphoma cells (Figure 1). Pathological examination of the nasopharyngeal mass biopsy revealed CD56-positive DLBCL based on immunohistochemical examination (Figure 2): CD56++, CD20+++, CD10+++, Bcl-6+++, Bcl-2−, Mum1−, CD99−, TDT−, TIA-1−, perforin−, CD30−, ALK−, CD2−, CD3−, CD5−, CD21−, c-Myc about 80%+; and in situ hybridization EBV-encoded small nuclear RNAs−. Pathological examination of a bone marrow biopsy (Figure 3) (hematoxylin–eosin and periodic acid-Schiff) revealed post-sputum active bone marrow hyperplasia (70%), reduced proportion of red pigment, mainly in the mid and early stages, megakaryocytes with mainly lobulated nuclei, and medium to large lesions, with abundant cytoplasm and deep nuclear staining. Pseudo-enveloped bodies were seen in the nuclei, with no obvious nucleoli, and scattered plasma and tissue cells. Immunohistochemical examination revealed CD20+, CD79a+, CD10+, Bcl-6+, Bcl-2−, c-Myc+, TdT−, Ki-67 approximately 95+, and possible bone marrow infiltration of invasive B-cell lymphoma. Additionally, paraffin-embedded nasopharyngeal tissue samples were subjected to fluorescence in situ hybridization (FISH) to detect MYC, BCL2, and BCL6 gene rearrangements and revealed c-Myc+, Bcl-6+. Bone marrow specimens were subjected to lymphoma hot spot genetic testing in EDTA anticoagulant tubes, and revealed DDX3X, LRP1B, SIN3A, and GNA13 gene mutations. Flow cytometry immunophenotyping showed that 17.5% of cells (all nucleated) expressed CD10, CD19, CD20, CD22, CD38, FMC7, CD79b, IgM, CyCD79a, and lambda Ig, indicating mature B-cell lymphoma/leukemia.
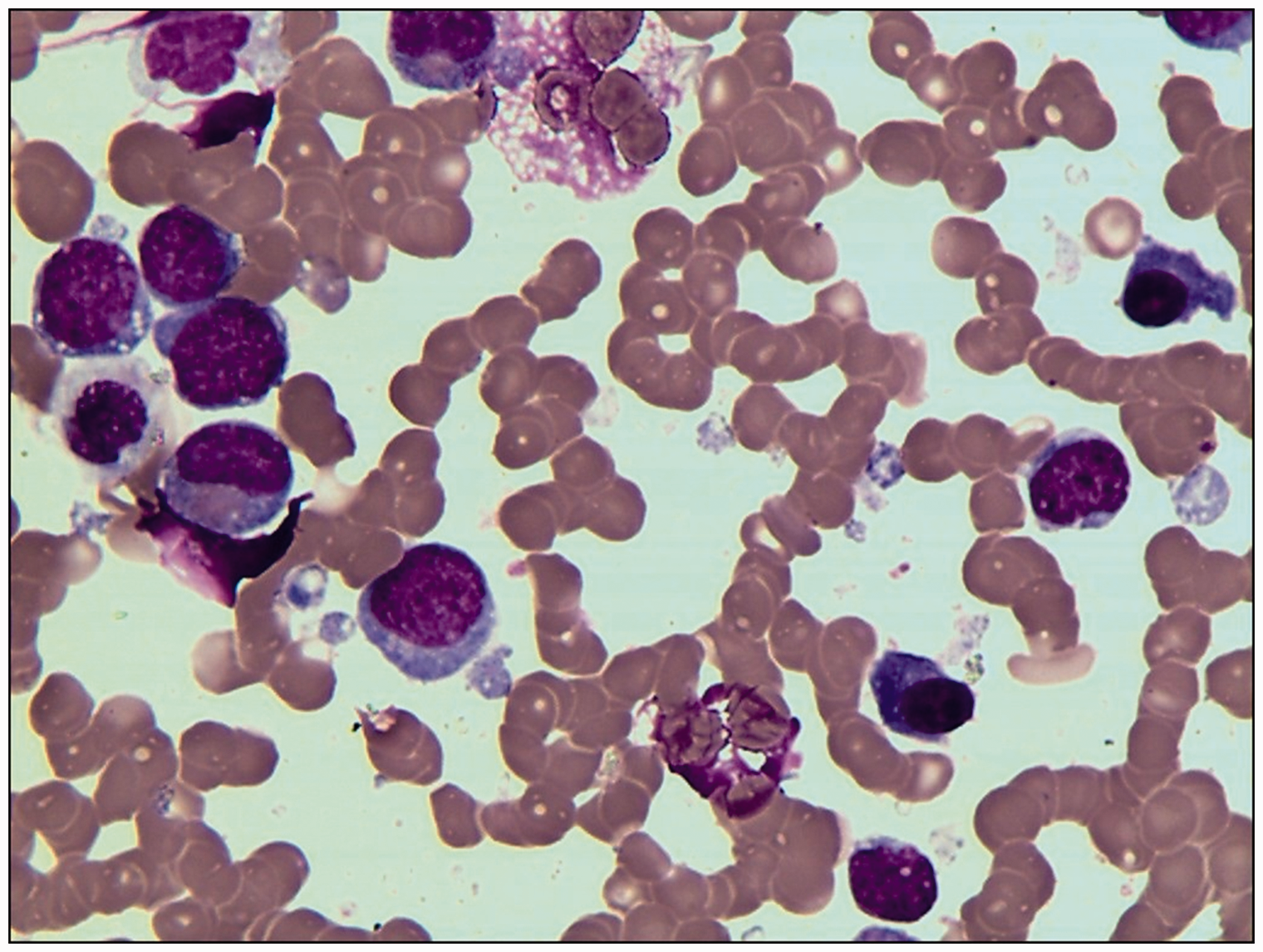
Bone marrow smear. Wright–Giemsa stain, ×1000.

Nasopharyngeal tissue biopsy. (a) Hematoxylin–eosin ×200; (b) CD20 (+++); (c) CD56 (++); (d) CD10 (+++); (e) Bcl-6 (+++); (f) Mum1 (−); (g) Bcl-2 (−); (h) c-Myc (+); (i) Ki67 (95%+) (b–i, immunohistochemical staining ×200). All images 200×.

Bone marrow biopsy. (a) Hematoxylin–eosin ×40, (b) hematoxylin–eosin ×400.
The patient was eventually diagnosed with CD56-positive DLBCL/leukemia with BCL6/MYC double-hit, and DDX3X, LRP1B, SIN3A, and GNA13 gene mutations. He initially received pre-chemotherapy with cyclophosphamide (CTX) and prednisone (CP), followed by chemotherapy with R-Hyper-CVAD AB regimens (A: rituximab 375 mg/m2 once daily on day 0, CTX 300 mg/m2 every 12 hours on days 1–3, vindesine 4 mg once daily on day 11, liposomal doxorubicin 40 mg on day 4, and dexamethasone 40 mg once daily on days 1–4 and 11–14; B: rituximab 375 mg/m2 once daily on day 1, methotrexate 1.0 g/m2 once daily on day 2, and cytarabine 3 g/m2 every 12 hours on days 3 and 4). The patient suffered from severe chemotherapy-related neutropenia and infection and the treatment was changed to R-DA-EPOCH (rituximab 375 mg/m2 once daily on day 0, etoposide 50 mg/m2 on days 1–4, doxorubicin 10 mg/m2 on days 1–4, vindesine 0.4 mg/m2 on days 1–4, dexamethasone 40 mg on days 1–5, and CTX 750 mg/m2 on day 5) for six courses. Mid-term evaluation by 18F-fluorodeoxyglucose positron emission tomography/computed tomography (PET/CT) revealed abnormal metabolism in the nasopharynx, increased fat metabolism in the bilateral neck, and no other abnormalities in other parts of the body.
According to the comprehensive assessment program, the administered chemotherapy regimens resulted in complete remission (CR) of the patient’s disease. Furthermore, to prevent the infiltration of lymphoma cells into the central nervous system (CNS), the patient underwent four courses of lumbar puncture combined with intrathecal injection of 5 mg dexamethasone and 50 mg cytarabine. PET/CT was repeated after eight courses of chemotherapy, and showed no abnormal lesions or signs of metastasis. Hot spot gene mutation detection for peripheral blood lymphoma was negative, and no chromosomal abnormalities were detected. Clinical efficacy evaluation showed CR of the disease, leading to discontinuation of the treatment. There were no abnormalities in the peripheral blood, bone marrow, or cerebrospinal fluid at 13 months of follow-up, according to examinations including MRI and PET/CT. The last evaluation of the patient was carried out in July 2019, when he was still in CR.
The patient and his parents provided written informed consent for publication of this report. The treatment was supervised by the ethics committee of our hospital. The ethics and consent forms are available upon reasonable request from the corresponding author.
Discussion
CD56 is a neural cell adhesion molecule and a member of the immunoglobulin super-family. CD56 is closely associated with the progression and metastasis of various tumors, and is currently widely used as a biomarker for the diagnosis, therapy, and prognosis evaluation of many malignant diseases, including small cell carcinoma, 2 striated muscle tumor, 3 thyroid cancer, 4 prostate cancer, 5 and hematological malignant tumors. 6 Among hematological malignancies, CD56 is a specific marker for NK/T-cell lymphoma and is found in plasmacytoma and microvillous lymphoma. However, its expression is usually lacking in B-cell NHL. Lymphomas with CD56 expression usually show characteristic adhesive growth, often involving tissues and organs outside the lymph nodes, 7 with an incidence of invasion of organs other than the lymph nodes of 45% to 60%. 8 The most frequent sites include Waldeyer’s ring and the gastrointestinal tract, tonsils, brain, spine, and bladder. 9 We report here on a case with invasion of the nasopharynx. This type of tumor could be differentiated from Burkitt’s lymphoma and extranodal nasal type NK/T-cell lymphoma by immunohistochemistry, FISH, and genetic testing.
Previous studies10–13 reported that CD56-positive NK/T-cell lymphoma often showed invasiveness and rapid progression, and CD56-positive acute myeloid leukemia was associated with a poor prognosis, complex nuclear structure, and extramedullary infiltration, while CD56-positive multiple myeloma usually presented with a better prognosis. CD56 expression in DLBCL is rare, and related studies 14 reported that CD56-positive B-cell lymphomas accounted for only 1.2% to 7% of DLBCLs and were more common in men (male to female ratio = 3:1), with possible geographical and ethnic differences. 6 CD56-positive DLBCL is often associated with CD10 and/or Bcl-6 expression, in addition to B-cell markers. Some studies found that Bcl-6 expression may be associated with a favorable prognosis and sensitivity to chemotherapy. 14 After a decisive diagnosis, the current patient received eight courses chemotherapy. Kawasaki et al. 9 reported a possible association between CD56 expression and CNS infiltration, potentially led to the occurrence of invasive neural nerve diseases. To prevent CNS infiltration leading to lymphoma during hospitalization, we treated the patient with four courses of lumbar puncture combined with intrathecal injection of dexamethasone and cytarabine. The patient’s condition improved greatly with no CNS infiltration, extranodal metastasis, or recurrence, and no abnormalities in his peripheral blood, bone marrow, or cerebrospinal fluid. The current comprehensive assessment of the patient’s condition indicated continued CR.
DLBCL is the most common NHL in adults, with a slightly higher incidence in developing compared with developed countries. 15 DLBCL is heterogeneous in terms of morphological, immunological, and molecular cytogenetics analyses. However, primary CD56-positive DLBCL is a rare subtype of NHL and there is currently no relevant statistical data in China, few case reports, and no unified diagnostic criteria or treatment plan. High-dose treatment combined with targeted chemotherapy as the main treatment for this disease should actively prevent the risk of CNS infiltration and extranodal recurrence.
Recent experimental studies on gene and protein expression confirmed the significance of polygenic abnormalities in determining the poor prognosis of DLBCL. 16 This suggests that some protein markers may play a key role in tumor development and may be considered as independent prognostic factors for DLBCL.
Double-hit lymphoma (DHL) and triple-hit lymphoma (THL) are current research hotspots. DHL refers to lymphomas with MYC gene rearrangement with other genetic abnormalities, most commonly including BCL2 and BCL6. DHL accounts for about 2% of all B-cell malignancies and 0% to 12% of DLBCLs. DHL is an invasive disease with a poor prognosis and an average survival of only 0.5 to 1.5 years. 17 The 2016 edition of the World Health Organization Lymphoma Revision Classification classified DHL independently as a highly invasive B-cell lymphoma with MYC and BCL2 and/or BCL6 rearrangements. Similarly, some scholars 18 proposed the existence of “double expression lymphoma”, with Myc and Bcl-2 protein overexpression, and proposed the concept of a double-hit score to aid diagnosis of the disease. However, there are currently no large-scale reports and few reported cases of CD56-positive DHL worldwide.
CD56 expression is rare in B-cell lymphoma, as determined by flow cytometry. 19 CD56-positive B-cell lymphoma appears to be preferentially derived from the germinal center phase. 20 CD56 expression in a small number of lymphomas suggests a possible association between CD56 expression and the mechanism of lymphoma cell proliferation, adhesive growth, extranodal infiltration, and metastasis. 7 Similarly, Hus et al. 21 and Sekita et al. 22 found that a higher frequency of CD56-positive cells in the peripheral blood was associated with a greater tumor burden and greater invasiveness in patients with DLBCL. The current young male patient with nasopharyngeal CD56-positive DLBCL was admitted to our hospital and administered CP pre-chemotherapy followed by R-Hyper-CVADAB and DA-EPOCH regimens for a total of eight courses, together with four courses of lumbar puncture combined with intrathecal injection of dexamethasone 5 mg plus cytarabine 50 mg, resulting in CR. The patient continued to be followed up. Because CD56+ DLBCLs are rare hematological malignancies both in China and abroad, CD56 expression is not included in the routine immunohistochemical diagnosis of B-cell lymphoma. However, heterogeneous phenotypic testing may be essential for the comprehensive diagnosis of the disease. Further studies and monitoring of post-treatment minimal residual disease are needed to determine if CD56-positive BCL6/MYC double-hit DLBCL represents a rare new subtype of lymphoma and/or is associated with the long-term prognosis. Bone marrow morphology, immunophenotype, and molecular studies are required to clarify the biological role of CD56 in B-cell lymphoma, 23 including more cases and in-depth exploration.
Conclusion
We report the rare case of a young patient with CD56-positive DLBCL/leukemia with BCL6/MYC double-hit and multiple gene mutations, requiring diagnosis and treatment. Indicators of a poor prognosis in patients with hematological tumors remain to be identified and attention should be paid to patients with rare poor-prognosis hematological malignancies in terms of providing individualized therapy and routine monitoring of therapeutic outcomes to ensure optimal care.
Footnotes
Availability of data and material
All data generated in this study are included in the uploaded manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The study was funded by the National Natural Science Foundation of China (81800167), Joint Funds for the Innovation of Science and Technology, Fujian Province (2018Y9010, 2018Y9205); Fujian Provincial Health Technology Project (2016-ZQN-29, 2018-ZQN-40); Natural Science Foundation of Fujian Province (2017J05132); Construction Project of Fujian Medical Center of Hematology (Min201704); and sponsored by the National and Fujian Provincial Key Clinical Specialty Discipline Construction Program of China.