
Abstract
Background:
Quality of life (QoL) is of paramount importance in the management of patients with chronic myeloid leukemia (CML), as most patients receive lifelong treatment. Despite this, information on patient experiences and involvement in treatment decision making is lacking.
Objectives:
The global Chronic Myeloid Leukemia Survey on Unmet Needs (CML SUN) evaluated the unmet needs and concerns of patients diagnosed with CML in chronic phase (CP) and their treating physicians. Here, we present the results of the CML SUN survey from respondents in South Korea.
Design and methods:
Patients with CML-CP (aged ⩾18 years; receiving a second- or later-line tyrosine kinase inhibitor [TKI]) and hematologists (treated ⩾10 patients with CML-CP over the last year) were invited to complete an online survey. Separate surveys were used for patients and physicians, with both covering CML diagnosis, treatment, impact on everyday life, and shared decision making.
Results:
Forty patients and ten physicians in South Korea completed the surveys. Patients’ top treatment goals were maintaining QoL and stopping or slowing down disease progression, while physicians emphasized achievement of molecular responses. More than half of physicians reported making treatment decisions with little or no input from their patients. Between 17% and 31% of patients reported that their physician only described one treatment for them. Although most patients were satisfied with their current treatment, a significant proportion believed it impacted their QoL. The top factors for patients when considering a treatment switch were maintaining QoL and living normally, while physicians again focused on achieving molecular responses.
Conclusion:
The results highlight the significant impact of ATP-competitive TKIs on patients’ QoL and provide useful insights into CML treatment in South Korea. The differences in patient and physician perspectives emphasize the need for shared treatment decisions that balance efficacy and tolerability to enhance QoL and to minimize unnecessary treatment switching.
Introduction
Although ATP-competitive tyrosine kinase inhibitors (TKIs) have substantially improved the life expectancy of patients with chronic myeloid leukemia (CML), managing resistance and intolerance to treatment remains challenging and often requires TKI switching.1–13 Consolidated data from 11 pivotal studies on first-line treatment of CML show that at least half of patients do not achieve major molecular response (MMR, BCR::ABL1IS ⩽0.01%) within the first year of treatment 14 ; furthermore, between 28% and 64% of patients discontinue their first TKI treatment due to resistance (inherent or acquired) or intolerance. Quality of life (QoL) is of paramount importance in the management of CML, as most patients receive lifelong treatment.6,15–18 Long-term treatment with ATP-competitive TKIs has been associated with a significant impact on QoL, with patients experiencing Grade ⩾3 and/or persistent low-grade adverse events (AEs) that often lead to treatment switching.18,19 Nevertheless, sequential treatment switching does not always resolve intolerance issues or result in improved QoL,10,17,20 and may lead to resistance to ATP-competitive TKIs due to the emergence of new mutations. 21 In addition, treatment success rates decrease with each treatment line.22,23
The majority of data concerning QoL and the impact of CML and its treatment on patients is derived from randomized clinical trials whose strict eligibility criteria often do not reflect clinical practice. 24 The few published reports on the patient journey in CML highlight differences in perspective between patients and physicians, alongside challenges in patient management. A survey of patients with CML based in the US and Canada revealed a high disease burden, with CML impacting patients’ ability to work and enjoy their social lives, and dissatisfaction with treatment side effects. 25 Worryingly, a recent series of interviews in the UK found that patients with CML often do not discuss the side effects they experience with their physicians. 26 Furthermore, the global TARGET survey on real-world management of patients with CML revealed that physician awareness of the management of persistent Grade 1 or 2 AEs was low. 27
Despite these reports, information about patient experiences and their involvement in treatment decision making are generally lacking and may not accurately reflect local cultural specificities of South Korea. Patient-physician interactions in Asia have often been described as asymmetrical, with physicians viewed as authoritative figures who should not be questioned.28,29 The well-documented patient preference for alternative medicine may also impact the patient relationship with physicians practicing Western medicine.28,30 These and other factors may influence how patients and physicians based in South Korea report their experiences.
Chronic Myeloid Leukemia Survey on Unmet Needs (CML SUN) was a global survey conducted to comprehensively understand unmet needs and concerns around CML from the perspectives of patients diagnosed with CML in chronic phase (CP) and treating physicians.31,32 Here, we aim to provide insights into the patient experience and patient-physician decision making in South Korea by analyzing the survey results from respondents in this country. The survey assessed the potential differences in treatment goals between patients and physicians, shared decision making between patients and physicians, the impact of treatment on patients’ QoL, the influence of side effects on treatment switch, and discrepancies in the exchange of information during discussions on treatment switching.
Methods
Surveys
The CML SUN survey consisted of two phases: a qualitative and a quantitative phase (Supplemental Figure 1). 32 The qualitative phase involved 60-minute in-depth interviews with 21 patients and 24 physicians from four countries (France, Germany, Japan, and the United States) to identify topics for the quantitative surveys. Following the qualitative interviews, 60-min cognitive interviews were conducted in a small sample of patients (n = 6) and physicians (n = 3) to eliminate any ambiguities and ensure respondents could answer survey questions and were not overwhelmed. Surveys were revised according to the feedback received and used in the next phase. The quantitative phase involved online surveys with 361 patients and 198 physicians from 11 countries. Data received was checked manually every day to ensure logic and technical potential errors were avoided; IP addresses were collated to prevent a single participant from entering multiple responses. The surveys had separate questionnaires for patients and physicians and covered topics such as diagnosis, treatment, impact on everyday life, treatment switching, and shared decision making; each of these surveys had a screener and six individual sections, and took approximately 40 min for patients and 30 min for physicians to complete. An external steering committee comprising physicians and advocates of patients with CML provided guidance throughout the process.
In the information at diagnosis section, patients were asked to rank 17 possible areas of information that they considered important to receive at diagnosis. These areas were: information about CML (e.g., how the disease will progress and how it will impact daily life); how to understand blood test results; treatment goals; impact of comorbidities on treatment selection; available treatments for CML; CML treatments in development or used in clinical trials; information on specific CML treatments (e.g., what they are, how to take them, and what to expect); treatment side effects; follow-up visits (e.g., frequency and tests that will be taken); treatment-free remission; fertility and family planning; self-care (e.g., nutrition and exercise); financial support or health insurance; patient support groups; treatment-related food or meal restrictions; concomitant medication use; any other information. The full survey questionnaire can be found in the Supplemental Appendix.
Recruitment
Patient recruitment took place through patient databases, physician and nurse referrals, and patient advocacy groups; physicians were recruited independently through online physician panels. Patients and physicians participating in the survey were eligible to receive compensation according to fair market values; they were given the option to donate said compensation to an international patient organization or to decline it.
Eligible survey participants were (1) patients with CML-CP aged ⩾18 years old, who had 1–3 prior TKI treatments, and were currently receiving a second, third, or fourth TKI; (2) physicians (transplant specialists, hematologists and/or oncologists) in practice for 3–35 years who were personally responsible for treatment decisions for patients with CML. Eligible physicians must have spent ⩾50% of their time caring for patients, treated ⩾10 patients with CML-CP (>30% of whom were receiving their second or third TKI) over the last year, and have switched patients’ treatment from second line to third line. Patients and physicians were excluded from participating in the survey if they were employed by a market research company, an advertising agency, or a pharmaceutical or biotechnology company.
Analysis
Analysis of the qualitative and quantitative data was conducted using transcripts and descriptive statistics, respectively. Means and medians were used to summarize continuous variables. No formal hypotheses were tested and results are presented in a descriptive way only.
Ethics
All participants provided informed consent. Records were anonymized and analyzed by research specialists at Ipsos SA. Institutional review board exemption was obtained before fieldwork commenced for all research materials used in qualitative and quantitative surveys.
Results
Survey population
A total of 10 physicians and 40 patients based in South Korea participated in the survey from November 2022 to March 2023. Patient and physician demographics are presented in Supplemental Table S1. The median age of patients was 40 years (range, 22–69); most patients were female (55%) and were receiving their second TKI (85%). All participating physicians were hematologist-oncologists, with a median time in practice of 18 years (range, 8–28).
Information exchanged at diagnosis
Patients were presented with 17 possible areas of information that they considered important to receive at diagnosis and ranked them on a scale of 1–5, with 1 being the most important. Physicians could select any information they provided to patients from the areas of information presented, without ranking them.
At diagnosis, patients wished to learn about potential side effects associated with CML treatment (60% of patients), receive information about their CML treatment (55%), and information about available CML treatments in general (43%) (Supplemental Figure 2). In contrast, at diagnosis, physicians offered information on the goals of treating CML with medication (100% of physicians), followed by information about comorbidities and their impact on treatment (90%), information about self-care, such as nutrition (80%), and potential side effects of CML treatment (80%). Although all physicians reported providing information on at least one topic at diagnosis, 48% of patients wished they had received more information at this time.
Top treatment goals
Overall, treatment goals were similar between patients and physicians (Figure 1); however, patients’ top priorities were maintaining QoL, having manageable side effects, and stopping/slowing down disease progression, while physicians emphasized achievement of molecular responses. Maintaining QoL was not as important for patients receiving their third TKI (reported by 33% of patients, compared with 53% and 55% receiving their first or second TKI, respectively); for physicians, the importance of maintaining QoL and manageable side effects also decreased in later therapy lines.

Top five treatment goals of patients and physicians by number of TKIs. Patients ranked their three most important treatment goals by number of TKIs; physicians selected any goals that they had by number of TKIs. The top five goals reported by patients and physicians are presented here, by treatment line.
Shared decision making
More than half of physicians reported making treatment decisions with little or no input from their patients, particularly in the first line (Figure 2). Consistent with this finding, only 17%–40% of patients across treatment lines reported that treatment decisions had been made together with their physician. No patients reported finding information independently about different treatments and asking their physician about them.
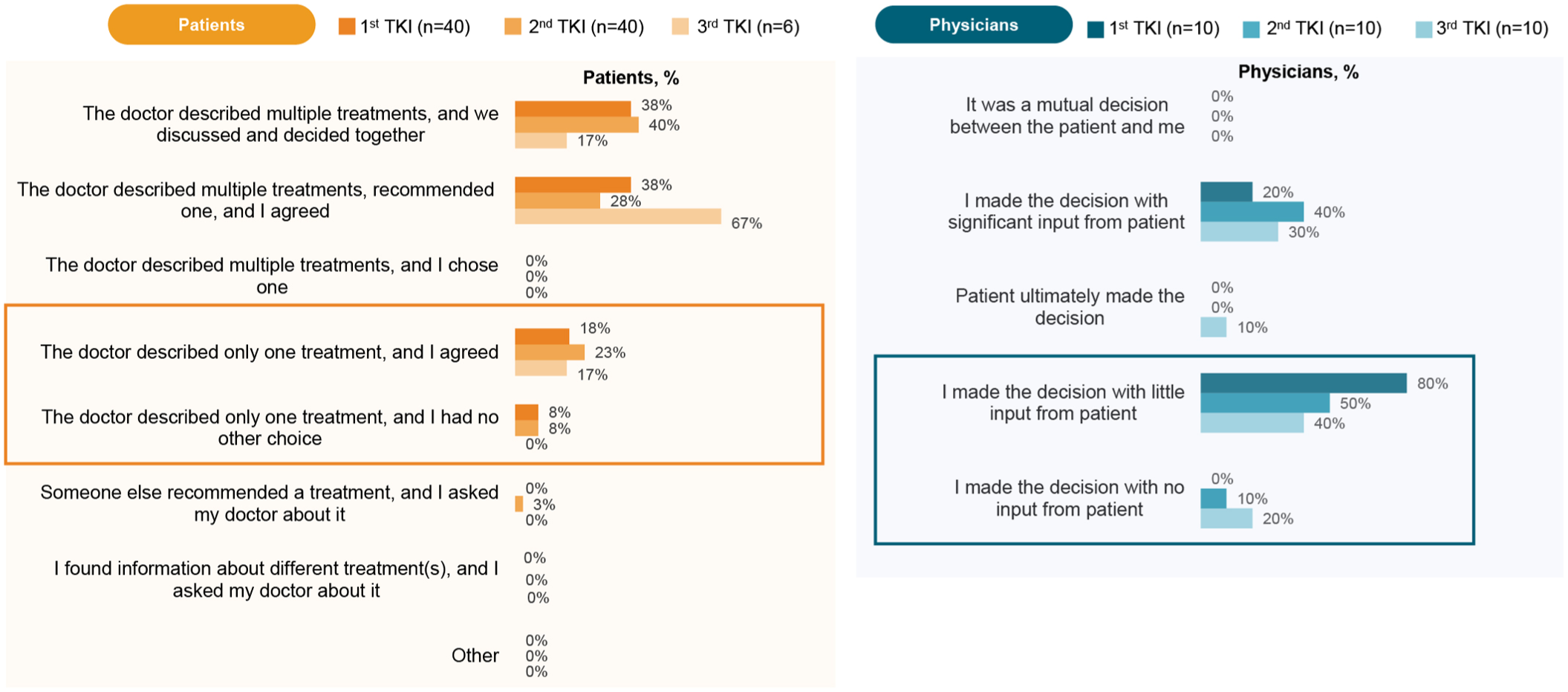
Patient and physician input on treatment selection. Roles in treatment decision making as reported by patients and physicians by number of TKIs.
Overall, 80% of physicians considered themselves the ultimate decision maker (Figure 3); however, 70% of physicians appeared open (responded “neither agree nor disagree”) to patients being more involved in their disease management and treatment decisions. Between 17% and 31% of patients reported that their physician only described one treatment for them (Figure 2), and the vast majority of physicians reported describing only one treatment to their patients (Figure 4). Most of these physicians felt that patients were unable to make an informed decision, as they did not understand the details associated with treatment choices. This was in agreement with 90% of physicians believing that patients understand some but not all of the information provided to them about their treatment (Supplemental Figure 3); this percentage of physicians remained constant across treatment lines. However, patient understanding of information about treatment increased across therapy lines, with 83% of patients switching to their third treatment reporting a good understanding of their therapy (Supplemental Figure 3).

Physicians’ perspectives on the management of CML-CP. Physicians ranked statements on a scale of 1–7, where 1 means strongly disagree and 7 means strongly agree (disagree: 1–3; neither agree nor disagree: 4; agree: 5–7).

Number of treatment options described to patients by physicians. The number of treatment options for which physicians provide details and the reasons for describing just one treatment are shown, as reported by physicians and presented by number of TKIs.
Burden of disease and treatment satisfaction
Although most patients expressed satisfaction with current TKI treatments, a significant proportion of patients reported that their current treatment affected their QoL (Figures 5 and 6); this comprised all aspects of their lives, including their mental health, financial situation, work, studies, and social life. Patients reported feeling physically and emotionally fatigued (86% and 81%, respectively), with treatment limiting their activities and causing constant stress (Figure 5). Overall, 34% of patients reported not being satisfied that their treatment maintained or improved their QoL, while only 58% reported that their treatment had manageable or no side effects (Figure 6). Significant proportions of patients reported that they were not satisfied or were neither satisfied nor dissatisfied with the impact of their current treatment on their work life (42%), studies (39%), social life (34%), financial situation (46%), and their mental health (44%). On the other hand, whereas all physicians were satisfied with the currently available CML treatment options, most hoped for more efficacious options in the future (Figure 3).
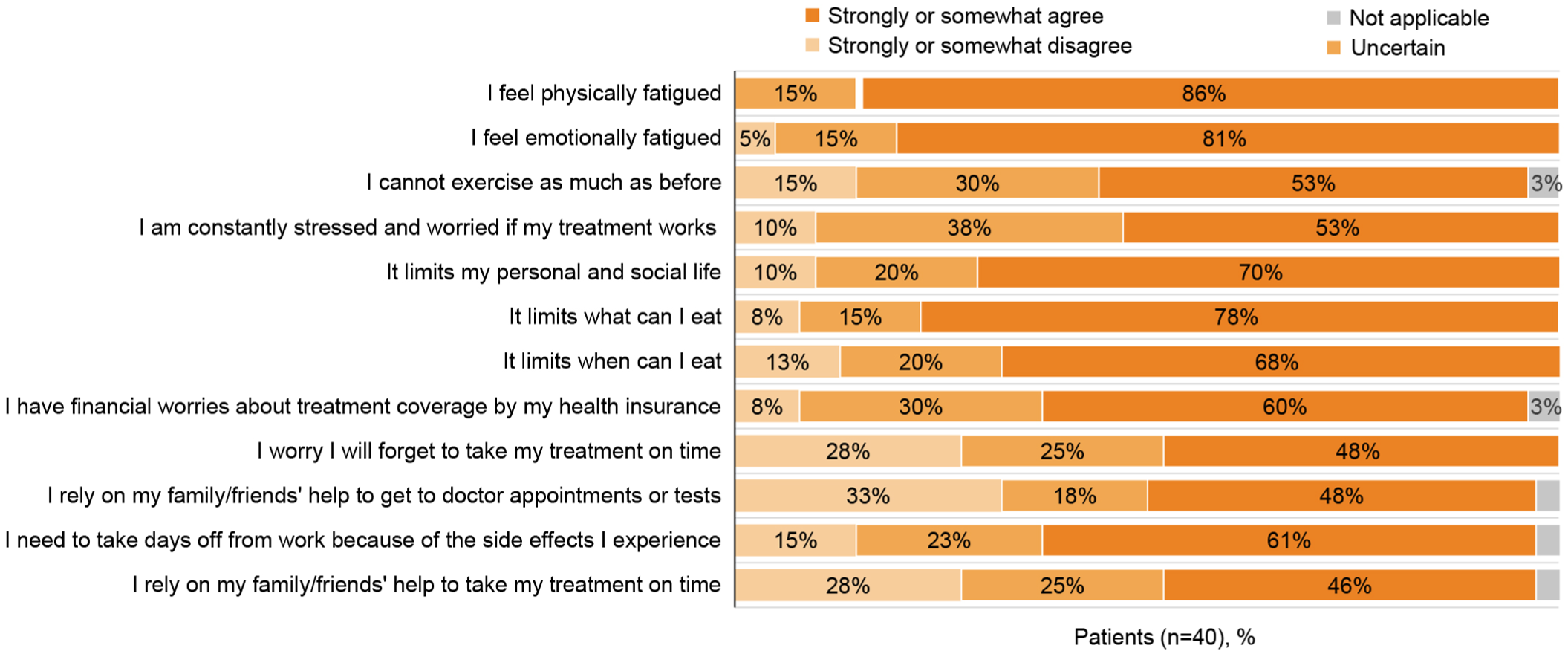
Patient perceptions of how treatment of CML-CP impacts their lives. Patients were asked how much they agreed with statements about how their current TKI treatment has affected their lives; they were asked to answer that they either strongly or somewhat agree, strongly or somewhat disagree, were uncertain, or found the topic not applicable.

Patient satisfaction with their current treatment. Patients ranked different topics on a scale of 1–10, where 0–3 is dissatisfied, 4–6 is neither dissatisfied nor satisfied, and 7–10 is satisfied. Values may not add up to 100% due to rounding.
Patients were also asked about their fears related to CML-CP and their impact on their daily lives (Supplemental Figure 4). The most common fears reported by patients included the possibility that there would be no available treatments for them (58%), that their current treatment would stop working (53%), and that they may have a blast crisis (53%), followed by the impact of long-term treatment on their bodies and side effects of treatment (50% each).
Treatment switching
Patients and physicians were asked who initiates discussions regarding treatment switching (Supplemental Figure 5). Most physicians (between 75% and 78%) reported initiating the discussion; this percentage remained constant across treatment lines. In contrast, 50% of patients reported initiating the discussion around treatment switch from their second to third TKI.
Among the reasons for treatment switch, patients reported side effects that led them to seek urgent medical care (28%–50%) or impacted their QoL (17%–48%) (Supplemental Figure 6). Approximately one-third of patients reported that the treatment was no longer working as a reason for switching. Physicians reported treatment resistance and intolerance as the most common reasons for switching TKI.
Patients and physicians were asked about the most important factors associated with a particular treatment when considering a switch (Supplemental Figure 7). The top factors for patients were that the treatment had few side effects, that it helped maintain or improve QoL, and allowed them to live normally. In contrast, the top factor for physicians was associated with achieving a molecular response. The least important factors when considering a treatment switch for patients were infrequent monitoring, once a day dosage, lack of impact on fertility, and lack of financial impact, whereas physicians reported lack of meal schedule restrictions, lack of impact on fertility, and their previous experience with that treatment (Supplemental Figure 8).
Management of side effects and treatment adherence
Despite the burden of side effects on QoL, 15% of patients on their first TKI did not tell their doctor about the side effects they were experiencing until they were asked (Supplemental Figure 9). Approximately one-third of patients reported that their physician discussed side effects with them after seeing abnormalities in their laboratory results.
Among patients who switched treatment due to side effects, approximately half of the patients reported that their physicians did not consider their side effects to be serious and expected them to continue with treatment (Figure 7). Only 54% and 50% of these patients on their first and second TKI, respectively, reported that their physicians showed empathy when discussing their side effects. Only 54% and 31% of patients on their first TKI reported that their physician gave them medication or advice to manage their side effects, respectively, while 23% of patients reported that their physician immediately reduced their TKI dose.

Physician response to side effects as reported by patients. Proportion of patients with different responses from their physicians about side effects recalled from their experience with their first and second TKIs.
Among patients who reported being non-adherent at least once (n = 6), 33% missed their current treatment dose because they did not like the side effects (Supplemental Figure 10). Other reasons reported by patients for missing their doses were forgetting to take the medication (50%) and wanting to feel “normal” (33%). Among physicians who thought patients may be non-adherent, most (88% to 90% across treatment lines) believed the reason was that patients forget to take the pills. Only 13% to 20% considered the impact of side effects as a reason for their patients to miss their treatment dose.
Discussion
As TKIs have improved the outcomes of patients with CML worldwide, the focus of treatment decisions is moving to improving or maintaining QoL during long-term treatment.17,18 However, data on the experiences of patients with CML and their role in treatment decision making are lacking. This report aimed to provide insights into the journey of South Korean patients with CML, their unmet needs, and their perspectives on treatment compared to those of their treating physicians. Asian patients face unique challenges in their journey: cultural factors influence their relationship with physicians, which has been described as deferential, with few patients questioning physicians’ decisions or raising concerns, resulting in low overall patient involvement in healthcare decision making.28,29,33 In addition, patience and self-control are desirable traits in Korean culture, 30 which could lead to patients not wishing to complain about side effects. The communal nature of many Asian cultures may also impact the patient-physician relationship, with patients avoiding confrontations with their treating physician to maintain a harmonious relationship. 29
Findings from South Korea were generally aligned with global results from the CML SUN survey.31,32 In South Korea, both patients and physicians mentioned maintaining or improving QoL as an important treatment goal. However, maintaining a good QoL was not as important for patients or physicians in third line or later (3L+), noting a shift of focus in disease management in this setting
Physicians’ top goals included achieving MMR and deep molecular response (DMR), something that patients did not often include as a priority. Similar results were observed in the global CML SUN survey and also in the TARGET survey, where achievement of early molecular response (EMR) and MMR were among the top goals of treatment for physicians.27,31,32 Among South Korean respondents in the TARGET survey, achieving MMR was the top treatment goal (30%), followed by prolonging overall survival and achieving EMR. 34 As previously noted, a decreasing proportion of physicians reported achieving MMR and maintaining or improving QoL as their top treatment goals as patients progressed to later lines of therapy. This highlights the need for effective treatments with a good tolerability profile that preserves or improves patient QoL in later treatment stages; it also underscores the need for novel treatments that are effective in earlier stages, preventing treatment switching and the challenges associated with managing patients in later treatment lines.
Most physicians reported making treatment decisions with little or no input from patients, regardless of treatment line. The proportions of physicians who made clinical decisions with little input from patients were considerably higher in South Korea than the global survey average for patients receiving their first and second TKI (80% vs 38% with first TKI, 50% vs 42% with second TKI, respectively), while percentages for patients receiving their third TKI were similar (40% vs 38%, respectively).31,32 Nearly all physicians reported discussing only one treatment option with patients (vs between one-half and two-thirds in the global survey). This was in contrast with 40% of responding physicians agreeing that their patients have an active role in determining their treatment (vs 65% in the global survey). Only 20% of physicians agreed that patients should be more involved in their treatment decisions (vs 58% in the global survey), with 70% neither agreeing nor disagreeing with this statement (vs 29% in the global survey).31,32 These results are consistent with the patient-physician relationship being asymmetrical and suggest that patient empowerment and collaborative decision making may be insufficiently integrated into standard clinical practice in South Korea. 33
The most common reason provided by physicians for not taking into account the patients’ perspective was the perceived lack of knowledge from patients about their disease and its treatment; however, a substantial proportion of patients reported understanding everything related to the information received, particularly patients receiving their third TKI (83% vs 57% in the global survey). 32 A recent report highlighted that almost 20% of South Korean patients felt they could not ask questions or express concerns related to their healthcare. 33 These results suggest there is a lack of communication between patients and physicians, and that patients wish to be more involved in their treatment decisions. Involvement in healthcare decision making is dependent on the quality of the information received 29 ; physicians should therefore aim to provide clear information to patients, for example, in the form of a decision aid or other printed or digital materials. Physicians could also improve their communication skills to facilitate interactions with patients in a culture-specific way.
The effect of treatment on patient QoL is critical to making informed treatment decisions in CML. 35 Similar to what was observed in the global survey, South Korean patients reported a substantial impact of CML and its treatment on their QoL, affecting all aspects of their lives. Although most patients were satisfied with their treatment in terms of disease control, a considerable proportion of patients reported dissatisfaction in terms of impact on QoL, work, and social life, as well as mental health. Treatment satisfaction has been correlated with QoL in patients with CML. 36 This highlights the need for more tolerable treatment options for patients across treatment lines. A better understanding of treatment tolerability is also needed, which may help physicians to better manage patient expectations of the impact of treatment on their lives. Ultimately, the ongoing burden of CML and its management underscores the importance of patient participation in treatment decisions, given that the therapy will significantly influence their daily lives over an extended period of time.
The long-term nature of CML treatment gives particular importance to the management of side effects. Nearly half of patients across treatment lines reported that their treating physician did not show empathy about the impact of their side effects and expected them to continue with their treatment. These proportions are considerably higher than those reported in the global survey (20% for patients on their first TKI and 5% on their second TKI). 32 The results of our study are in agreement with those of the TARGET survey, where South Korean physicians were reluctant to switch treatment due to Grade 1 (0% and 2% for hematologic and non-hematologic events, respectively) or non-hematologic Grade 2 (9%) persistent events. 34 Fifteen percent of patients on their first TKI did not inform their physician about their side effects, a similar proportion to that reported in the global survey (18%). On the other hand, approximately one-third of patients reported that their treating physician discussed side effects with them after noticing abnormalities on their tests, a higher proportion than in the global survey (23% and 26% for the first and second TKI, respectively). 32
The impact of even low-grade side effects, when experienced for a long period of time, can lead to poor treatment adherence and discontinuation,35,37,38 which in turn can significantly impact patient outcomes in CML.37,39 Although forgetting to take the medication was the most common reason for missing doses from both patients’ and physicians’ perspectives, a larger proportion of patients than physicians reported side effects as the reason behind missed doses. Side effects were also cited as the second most common reason for treatment nonadherence in a survey of South Korean patients with CML. 40 These results suggest that engaging patients in discussions about their side effects from treatment and their management could help keep patients on therapy for longer, avoiding treatment switch and helping to maintain or improve QoL. Given that nonadherence to CML treatment correlates with increased total healthcare costs, 41 this approach could result in reduced economic burden.
The survey results for South Korea highlight the need for shared decision making and better communication, from which an improved patient experience could be expected. Approaches to address these issues include enhancing physician communication skills to improve patient-physician interactions.29,33 Physicians in South Korea have reported time constraints impacting healthcare needs, with average consultation times of approximately six or seven minutes33,42; such an environment is not conducive to effective and comprehensive patient engagement. However, a recent Korean study showed that shorter consultations do not necessarily preclude a patient-centered approach. 33 The length of the long-term patient-physician relationship could play a significant role in improving patient involvement in decision making: longer patient-physician relationships have been correlated with increased satisfaction with treatment, increased patient openness to physicians, and increased adherence to treatment in Korea. 43 Only a low proportion of patients in the Korean healthcare system have a usual care provider 43 ; an increase in this percentage could result in an improved patient-physician relationship. Involvement of non-physician healthcare team members, such as nurses, may also help improve interactions, where these team members could have a more open relationship with patients and relay information back to physicians. 29 Patient education, where patients are empowered to request information from their treating physician, may result in physicians providing further information that can help patients in decision making. 33 Overall, an increasing body of evidence points to a need for gradual change toward patient centricity and higher patient involvement in treatment decision making in South Korea. 28 A Korean version of a tool specifically designed for assessing patient-centered care has recently been validated 44 and can be expected to further promote patient-centered care among Korean healthcare professionals.
Limitations
A potential limitation of this study is the low number of responding physicians in South Korea, which may affect the generalizability of the results; future studies with a larger sample size will help confirm the results of the present survey. Selection bias may also have affected responses: since the survey was voluntary, respondents may have included a large proportion of highly motivated patients and/or patients with high levels of health literacy. On the other hand, responding physicians likely described their interactions with their average patients, rather than patients with high levels of motivation and health literacy; this should be considered when comparing patient and physician perspectives. The majority of patients were receiving second-line therapy, whereas most patients treated by responding physicians were newly diagnosed; it may therefore not be possible to generalize these results across different lines of therapy. Patient and physician surveys were conducted independently, and it was not possible to pair the responses of each patient with those from the treating physician. Physician responses may also have been influenced by their practice setting (e.g., community hospital or academic center). Social desirability biases may also have been at play, causing patients to underreport nonadherence to treatment or physicians to overreport their status as decision makers. The questionnaire was not formally validated, although the qualitative phase included feedback from patients and physicians that helped shape it in an effective way. Patient QoL was not assessed as comprehensively as with a validated patient-reported outcome instrument; future studies may include these tools to support cross-study QoL comparisons. Finally, responses may also have been influenced by poor recollection of events that occurred long before the survey.
Conclusion
Although previous surveys provided useful information on the management of patients with CML, CML SUN includes the perspectives of both patients and physicians, helping to visualize the patient journey with a more holistic approach. In conclusion, the CML SUN study underscores the significance of collaborative decision making that considers both patients’ and physicians’ goals regarding effectiveness and tolerability; the inherent differences in patients’ and physicians’ viewpoints should be recognized and actively incorporated into treatment planning and communication to improve patient-physician interaction and facilitate optimal outcomes. The results presented here provide important insights aimed at enhancing CML management in South Korea.
Supplemental Material
sj-docx-1-tah-10.1177_20406207251409297 – Supplemental material for Understanding disease management and the patient journey in chronic myeloid leukemia: results from the CML SUN survey in South Korean patients and physicians
Supplemental material, sj-docx-1-tah-10.1177_20406207251409297 for Understanding disease management and the patient journey in chronic myeloid leukemia: results from the CML SUN survey in South Korean patients and physicians by Jae Joon Han, Cristina Constantinescu, YoungIm Kim and Hawk Kim in Therapeutic Advances in Hematology
Supplemental Material
sj-pdf-2-tah-10.1177_20406207251409297 – Supplemental material for Understanding disease management and the patient journey in chronic myeloid leukemia: results from the CML SUN survey in South Korean patients and physicians
Supplemental material, sj-pdf-2-tah-10.1177_20406207251409297 for Understanding disease management and the patient journey in chronic myeloid leukemia: results from the CML SUN survey in South Korean patients and physicians by Jae Joon Han, Cristina Constantinescu, YoungIm Kim and Hawk Kim in Therapeutic Advances in Hematology
Footnotes
Acknowledgements
The authors would like to thank the patients and physicians who took part in the survey. Editorial assistance was provided by Vanesa Martinez Lopez, PhD, of Novartis Ireland Ltd., and was supported by Novartis Pharmaceuticals Corporation in accordance with Good Publication Practice (GPP 2022) guidelines (![]() ).
).
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.