
Abstract
Fungating testicular germ cell tumours represent a rare and extreme manifestation of neglected testicular cancer. These cases typically arise after significant delays in presentation, reflecting advanced local disease and, in many instances, concurrent metastatic spread. We present the case of a 41 year-old man with a year-long history of a progressively enlarging, ulcerated scrotal mass. Biopsy confirmed seminoma without evidence of metastasis. Given the extent of local disease, the patient received neoadjuvant etoposide-cisplatin chemotherapy, resulting in dramatic tumour regression. This facilitated a radical orchidectomy and wide local excision with primary closure and clear margins. He remains disease-free 12 months post-treatment. To better understand the management and outcomes of this rare presentation, a narrative review was performed, indentifying 19 comparable cases of fungating GCTs over the past 28 years. The median age at presentation was 36, with a median diagnostic delay of 6 months. Non-seminomatous subtypes, particularly embryonal carcinoma, predominated and carried a higher risk of metastasis. While upfront surgery was attempted in ten cases, it frequently required extensive resections and yielded positive margins. In contrast, six patients received neoadjuvant chemotherapy, leading to marked tumour regression in five, improved surgical outcomes, and no reported positive margins. These findings highlight the potential advantages of neoadjuvant chemotherapy in managing extensive, locally advanced GCTs, even in Stage I disease. While concerns exist regarding infection risk in the setting of fungating tumours, these were not borne out in the reviewed cases. Multidisciplinary input is invaluable in optimising sequencing of therapy in such complex presentations.
Introduction
Globally, testicular cancer is the 20th leading cancer type, and the most common malignancy in men aged 15–44, with an incidence rate of up to 10/100,000. 1 The majority (>95%) are germ cell tumours (GCT), with roughly equal prevalence of seminoma (SGCT) and non-seminoma (NSCGT). 2 The implementation of cisplatin based chemotherapy regimens and improved surgical technique has translated into a commendable cure rate of >95% for all testicular GCT, and 90% in those with metastatic disease. 3
Fungating GCT masses, a rare and extreme form of presentation, are typically associated with a protracted delay in seeking medical assistance. Such masses signify very advanced local disease with a high risk of metastases at presentation. There are currently no guidelines or recommendations on how best to manage such cases, including how to optimally sequence surgery and chemotherapy for non-metastatic disease.4,5,6
Case report
A 41 year-old male, presented with a malodorous right-sided fungating scrotal mass progressively enlarging over 1 year. On examination, a 15 cm fixed mass extended along the ipsilateral inguinal canal and anterior abdominal wall. (Figure 1(a)). The right hemiscrotum was characterised by extensive ulceration and necrosis. The penis and left testis were not involved and there were no systemic or infective symptoms. There was no history of cryptorchidism, previous scrotal surgery or other significant past medical history. (a) Fungating inguino-scrotal mass at presentation; (b) Axial CT at presentation and (c) Coronal CT at presentation.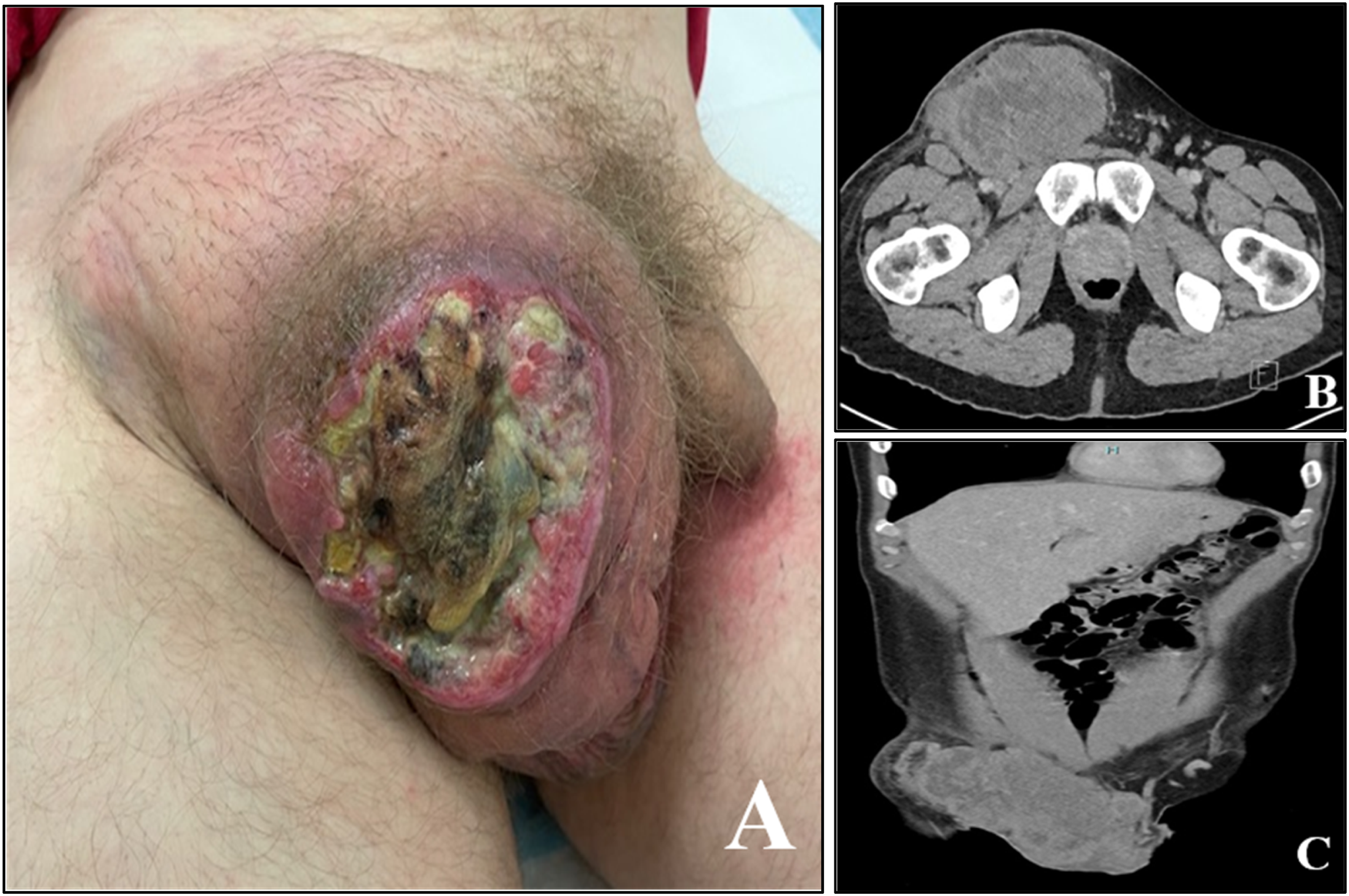
Assessment of germ cell tumour (GCT) markers revealed high LDH (16,558 U/L), slightly elevated β-hCG (23 mIU/mL) and normal AFP (1.12 ng/mL). Several 4 mm punch biopsies, taken from the fleshy (non-necrotic) component of the ulcerated mass, were consistent with seminoma (SGCT). Immunohistochemistry demonstrated strong diffuse staining for PLAP, OCT4 & c-KIT, and negative staining for CKAE1/E3 and CD30. Cross-sectional imaging (CT and MRI) reported tumour involving the anterior abdominal wall but not invading adjacent critical structures (Figure 1(b) and (c)). FDG PET showed avidity only within the primary tumour, although there were non-avid sclerotic bone lesions at T4 and L3. A subsequent biopsy of the bone lesions excluded cancer.
Given the absence of metastatic disease, the merits of upfront chemotherapy versus orchidectomy with wide local excision were debated at both a local and statewide testicular-oncology multidisciplinary meeting. Although there was some concern regarding risks of sepsis and poor wound healing, neoadjuvant chemotherapy (NACT) was collectively thought preferable. It was expected to down stage the tumour and optimise operative outcomes, enabling clearance of surgical margins and minimising the soft tissue defect size which would potentially require flap closure.
In an outpatient setting, four cycles of EP (etoposide and cisplatin) chemotherapy were administered (foregoing bleomycin due to heavy smoking history). A charcoal-based absorbent dressing (Carbosorb, B Braun, Australia) was changed daily to manage exudate and reduce malodour associated with the fungating mass. He received several weeks of prophylactic antibiotics to minimise infection risk and remained systemically well throughout therapy. Tumour markers normalised during chemotherapy, with the increased β-hCG resolving after one cycle of EP, and LDH after 2 cycles of EP. Clinical and radiological assessments showed a dramatic regression of tumour size. There was near complete healing of the ulcerated component, with a remnant cutaneous cicatrix 2 weeks after completion of treatment (Figure 2(a) and (b)). (a) Post-chemotherapy, pre-operative improvement; (b) Axial CT post-chemotherapy, (c) Intra-operative dissection and (d) En-bloc surgical specimen of residual mass.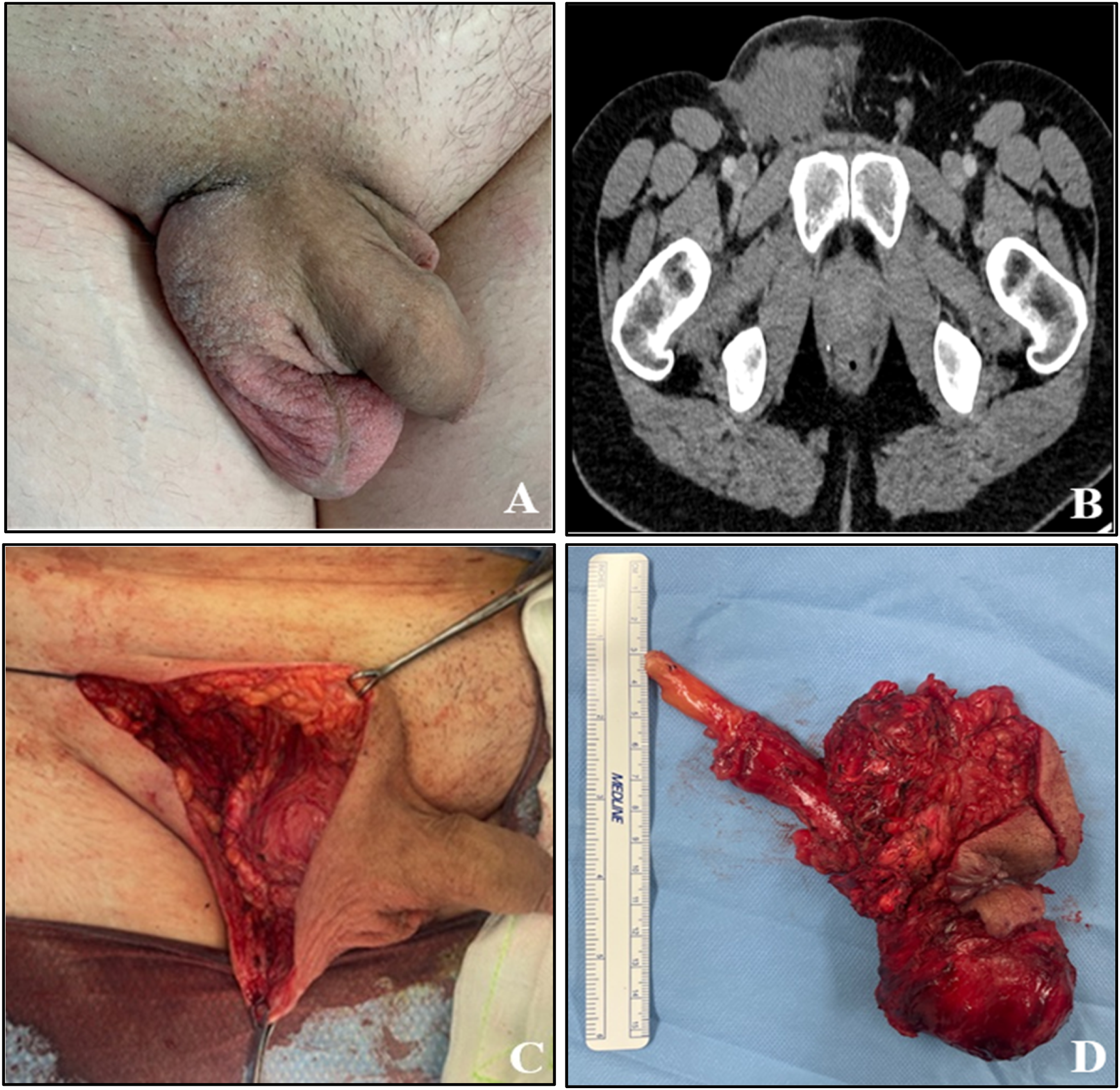
A radical right orchidectomy with en bloc excision of the residual 10 × 5 cm inguino-scrotal mass and overlying skin was performed 6 weeks post NACT (Figure 2(c) and (d)). Due to the dramatic reduction in tumour size, primary closure was able to be achieved. Final pathological staging found ypT1aNXM0S0 with 80% necrotic non-viable seminoma and 20% mature teratoma (18 mm in maximum dimension and confined to the testis; including cartilage, glands, and keratin). Surgical margins were clear. Follow-up is ongoing with three monthly tumour markers and 6-monthly CT imaging. He remains disease free at 12 months.
Written patient consent was obtained and approval to publish this case was acquired from Barwon Health Institutional Review Board (Project ID: QA/119,277).
Narrative review
Method
Tumour markers all reported in standardised units with normal limits defined as: AFP <10 ng/mL, β-hCG <5 mIU/mL, LDH <1.5X Normal U/I NR = Not reported. Management: N-No Treatment, B–Biopsy, S–Surgery, C-Chemotherapy, R-Radiotherapy. Pathology: NSGCT- Non Seminomatous GCT, SGCT-Seminomatous GCT, EC- Embryonal Carcinoma, YS- Yolk sac tumour, 1A historical term usually indicating mixed EC and teratoma, 2 Reported as pure SGCT, although elevated AFP implies mixed disease.

Results
The median age at presentation was 36 years (range 18–61). Two men (out of 20) had a history of childhood orchidopexy for cryptorchidism7,8. Three others had a history of scrotal orchidectomy prior to developing an ipsilateral recurrent fungating scrotal mass (all NSGCT)9,11. The median time from patient noticing an abnormality to seeking medical assistance was 6 months (range 4–14 months), although the delay was not clearly reported in 10 cases. At presentation three men had a febrile illness, four had severe anaemia (4.6–7.1 g/dL), two reported significant weight loss and one had urinary retention. 20% (4) of the men died from complications of advanced disease during initial admission.
65% (13) of the cases were NSGCT, 20% (4) were SGCT, 10% (2) were mixed (SGCT and NSGCT) and one was anaplastic seminoma. Five men had pure embryonal carcinoma (EC) making it the most common histological subtype, with a further three men having teratocarcinoma; a historical term typically indicating mixed EC and teratoma.
20% (4) had localised (T4, stage I) disease at presentation, of which the majority (3) were SGCT. In comparison, 35% (7) of cases had metastatic (stage III) disease at presentation, all of which were NSGCT except for 1 anaplastic seminoma.
Ten cases underwent upfront surgery (Table 1). Seven of these had partial scrotectomy and wide local excision (WLE) for an ulcerated GCT mass confined to the scrotum. Positive margins occurred in 1 case. The three alternative cases had more extensive masses involving perineum, abdominal wall, inguinal canal or retroperitoneum. As such, more radical surgery was performed, including colostomy diversion and rotational flap closure in one case and penectomy with perineal urethrostomy in another. The third case was an incomplete resection.
In comparison, six cases underwent neoadjuvant chemotherapy (Table 1). Five of these had locally advanced disease extending beyond the scrotum, into the abdominal wall, inguinal canal or retroperitoneum. One died 5 days after the first cycle of chemotherapy from presumed complications of intracranial metastases. The other five all achieved either a complete response or significant downsizing of the primary tumour with closure of the fungating ulcer. All five underwent radical orchidectomy with WLE of any residual mass, with a flap or plastics assistance required in two cases for primary wound closure. There were no reported positive margins.
Due to significant comorbidity, one other case was referred for radiotherapy as primary treatment of the fungating mass.
Discussion
These 20 case reports suggest that fungating disease is the extreme local natural history of neglected testicular GCTs. Reasons for late presentation include poor health literacy, limited access to health care and psychological barriers (including fear, embarrassment and shame). 25 Such scrotal masses can be the result of either SGCT or NSGCT (especially EC), however NSGCT appears to carry a higher risk of concurrent metastatic disease. Choriocarcinoma was only evident in 1 case as a minor component of mixed NSGCT. This is consistent with the natural history of choriocarcinoma, an aggressive form of NSGCT which often presents with disseminated disease and typically a small or “burned out” testicular primary: not a fungating mass.
Whilst orchidectomy typically precedes chemotherapy in the management of GCT (except where there is widely disseminated metastases), such convention may not always be appropriate for extensive T4 disease. Our reported case of a fixed and fungating inguino-scrotal mass (with initial biopsy and tumour markers suggestive of SGCT) had an absence of nodal or metastatic spread. Nonetheless, upfront WLE carried a high risk of positive surgical margins and difficult reconstruction due to a sizeable soft tissue defect. Any wound healing issues would have also further delayed systemic therapy.
Along with four other case reports, we demonstrated that neoadjuvant chemotherapy can markedly reduce tumour bulk, consequently improving resectability and minimising morbidity.
Whilst chemotherapy may theoretically increase the sepsis risk of a fungating wound, 26 this was not demonstrated in these cases. In fact, the ulcerated component of the fungating masses all resolved with chemotherapy treatment, affirming that many GCTs are highly sensitive to platinum based chemotherapy. 27 For the few large invasive masses that proceed straight to extirpative surgery (sometimes out of concern regarding infection), outcomes were often less satisfactory, with less organ preservation (e.g. penectomy), poorer cosmesis and positive margins.
Due to limited data, prognosis and long-term outcomes remain uncertain for this rare cohort of men with fungating testicular GCT.
Conclusion
Fungating scrotal GCTs are a rare presentation. The sequencing of treatments (surgery and chemotherapy) may be influenced by factors such as the extent of local disease, metastatic burden, patients functional status and the presence of infection. Our case nonetheless underscores the utility NACT can have in the management of such complex presentations, and the importance of multidisciplinary discussion. By reviewing comparable reports, a pattern emerged of NACT dramatically reducing tumour volume, thus having a transformative role in achieving resectability and optimising subsequent surgical success.
Footnotes
Ethics approval
Ethical approval to report this case was obtained from Barwon Health Research and Ethics Committee (Project ID: QA/119,277).
Informed to consent
Written informed consent from the patient was obtained to use their de-identified information and clinical photographs in this published article.
Author Contribution
PP designed the research project. DG and PP performed the literature search and review of the articles. DG wrote the first draft of the manuscript. All authors contributed to revisions and approval of the final draft.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analysed during this study are included in this published article.