
Abstract
Testicular neoplasms occur in more than 90% of cases, due to primary testicular germ cell tumors. Other entities are non germ cell tumors of the testis, testicular manifestation of lymphomas or metastases. International and interdisciplinary co-operation has led to the development of urological guidelines and to good therapeutic success for testicular neoplasms. The gold standard for treatment of a testicular neoplasm is the radical orchiectomy. However, for individual cases with suspected lymphoma, a treatment decision differing from the guidelines may be reasonable. We present the case of a 38-year-old man with testicular manifestation of a transformed mycosis fungoides, which is the most common form of cutaneous T-cell lymphoma.
Introduction
Mycosis fungoides belongs to the group of primary cutaneous T cell lymphomas, according to WHO classification. It is defined as a non-Hodgkin's lymphoma of the skin without proof of extracutaneous manifestation at time of diagnosis. Mycosis fungoides accounts for 0.5% of all malignant lymphomas and for 44% of all cutaneous lymphomas, 1 and has an incidence of 0.5/100.000/year. 2 It occurs predominantly in men of middle and higher age. 3 Mycosis fungoides develops slowly from a premycoside stadium with an uncharacteristic skin pattern over the plaque stadium with extensive infiltrating foci to a tumor stadium with fungus formed ulcerating foci. In the plaque and tumor stadium, the probability of extracutaneous manifestation increases. The common indolent course of mycosis fungoides with a good prognosis deteriorates upon detection of transformation to a large cell T cell lymphoma. When a transformation is diagnosed, the median survival time is only 22 months. 4 The most common reason for death is immunosuppression due to lack of functional T helper cells. 5 For therapy of mycosis fungoides, a stadium adapted, conservative therapy is recommended. 6 In the early stages, the predominant therapy includes the use of topical steroids and light therapy. In the later stages, a combination of local and systemic therapies are favored. 7 Chemotherapy is indicated in patients with lymph node and organ manifestation (stadium IV). 8
Germ cell tumors (seminomas and non-seminonas) are the most common testicular tumors, representing 85-90%, followed by testicular non-germ cell tumors in 5% of cases, and testicular lymphomas in 5% of the patients. 9 Testicular lymphomas are mainly due to secondary involvement by non-Hodgkin's lymphoma of B-cell lineage. 10 Less than 1% of testicular neoplasms are metastases from tumors of the gastrointestinal tract, bone marrow, lung, or prostate. 11 The gold standard in treatment of testicular neoplasms is radical orchiectomy or, in very selected cases, testis sparing surgery. 12
Case Report
A 38-year-old patient presented to the urologic clinic with a growing scrotal mass that had developed over two weeks. Past medical history was relevant for a cutaneous T cell lymphoma (mycosis fungoides and lymphomatoid papulosis type C), initially treated nine years ago with light therapy (Balneo PUVA therapy) and steroid externals. Slow growing, partly ulcerating skin tumors had occurred three months prior to urologic presentation (Figure 1). Dermatologists performed a diagnostic excision of the skin tumors, and a CT scan for staging revealed, in addition to the skin tumors, the presence of a suspect testicular mass of the left side (Figure 2). The patient had no fever, night sweats, or weight loss, were noted and the ECOG performance status was 0. The histopathologic result of skin excision was not present at the time of presentation in the urology clinic.

Large-scale weeping and partly exulcerating tumor nodes with erythema at the back of the patient.

Computed tomography scan showing a testicular neoplasm on the left side.
Inspection revealed an enlarged left hemiscrotum and, upon palpation, an induration without tenderness. B mode ultrasound showed an inhomogeneous tumor of the testis of 45×25 mm, presenting with central and peripheral hyperperfusion by Doppler ultrasound. The right testis and epididymis were normal by physical examination and ultrasound. Blood analysis showed normal results for AFP, β-HCG, and LDH.
A radical inguinal orchiectomy of the left side was performed. There were no intraoperative or postoperative complications and the patient was discharged two days after surgery. Histological examination showed an infiltration of the testis and epididymis by a CD30-positive T cell lymphoma (Figure 3). Considering the patient's medical history, the diagnosis of a transformed mycosis fungoides with a testicular metastasis as an extracutaneous manifestation in tumor stadium with organ manifestation (T3 N0 M1 according to Stadium IV A) was made.
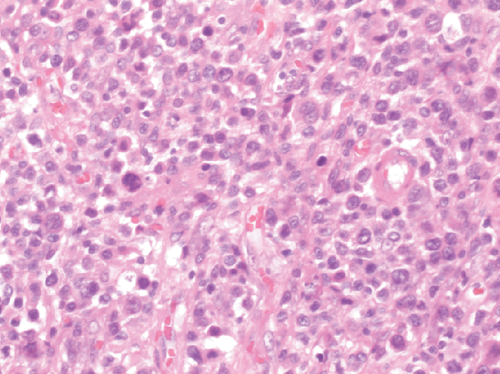
Testicular parenchyma with a dense pleomorphic infiltration of cells (Haematoxylin and Eosin, 40×).
The macroscopic specimen was 60×40×40 mm in size, containing a 50 mm soft beige brown tumor with necrosis and hemorrhage. Histological examination showed a dense pleomorphic infiltration of lymphoid blastic cells with round, partly cerebriform nuclei, which had diffusely infiltrated the testis and the epididymis. Immunohistochemical examination revealed a strong expression of CD30 in neo-plastic cells and a proliferation activity (Ki-67) of 90%. Immunohistochemical staining with antibodies to PALP, CD 117, and cytokeratin showed negative results. Finally, the diagnosis of a testicular infiltration by a CD30-positive T-cell lymphoma was made (Figure 4). Considering the clinical presentation, the histological results were in agreement with a transformed mycosis fungoides.

Immunohistochemical proof of CD30+ cells (CD30 stain, 10×).
The interdisciplinary tumor board decided on a palliative monotherapy with pegylated liposomal doxorubicin. Follow-up after six months showed a good response with regression of the cutaneous tumors.
Discussion
In our patient, mycosis fungoides was present for nine years, beginning with a mild course in the premycoside stadium. At urologic presentation, a scrotal mass was detected by palpation and ultrasound. Due to suspected primarily malignant testicular cancer or manifestation of the mycosis fungoides as a differential diagnosis, radical orchiectomy was performed. Transformed mycosis fungoides was diagnosed by histopathology and a mono-chemotherapy was started.
Because of the good response to chemotherapy with regressive cutaneous manifestation, alternative treatment options for the testicular neoplasm can be discussed retrospectively. One option would be to take an intraoperative frozen section. If the tumor would have been smaller than 2 cm. easily resectable and had been clearly diagnosed as a lymphoma, tumor enucleation might have been discussed as an option, as it is common in non-germinal tumors with no appearance of malignancy in frozen sections. 13 Another indication for organ sparing surgery is the presence of a synchronous or metachronous contralateral testicular tumor or a single testis. 14 For organ sparing surgery, preoperative leydig cell function and serum testosterone levels should be normal and the tumor should invade less than 30% of the volume of the testis. 15 Another option would be to take a scrotal biopsy for confirmation of the diagnosis. The advantage of morbidity reduction should be weighed against the oncologic risk of metastatic spread in the case of a primary testicular tumor. Although testicular biopsy is currently almost exclusively used during a testicular sperm extraction, it still remains a diagnostic option in selected patients. 16 In our patient, differential diagnosis included progression of mycosis fungoides, testicular cancer, or concurrent second lymphoma, which has been shown in patients with mycosis fungoides. 17 Thus, a complete histopathologic and immunohistological evaluation would be recommended. On the other hand, in our patient, mycosis fungoides in tumor stadium would probably maintain the illness determining the prognosis, irrespective of the biopsy result. According to our knowledge (Medline search on September, 2013, search terms: testis and mycosis fungoides), testicular manifestation of transformed mycosis fungoides has not been previously reported. There is one case report of non-transformed mycosis fungoides involving the testis and maxillary sinuses. 18
Conclusions
This case report demonstrates the importance of detailed history and interdisciplinary oncologic management. Retrospectively, the orchiectomy that was performed neither influenced the prognosis nor the therapy strategy for the patient. Therefore, a management differing from urological guidelines can be discussed by choosing alternative diagnostic or therapeutic strategies in well selected patients.
Footnotes
Acknowledgements
The authors are grateful for the support received from the Department of Pathology, Klinikum Siloah Hannover, Germany.