
Abstract
Olfactory neuroblastoma (esthesioneuroblastoma) is a rare malignant tumor of neuroectodermal origin. With only about 1,000 cases reported, there are no clear guidelines regarding management of this disease. Intracranial extension and orbital involvement have been shown to be independent risk factors associated with poorer outcomes. We hereby report a case of a 46-year old male presented with an 8-month history of progressive nasal obstruction and intermittent right-sided epistaxis associated with anosmia and increased pressure sensation in and around the right eye. Further evaluation revealed a large enhancing heterogeneous cystic and solid mass in the right nasal cavity measuring 5.0×5.3×4.6 cm with extension superiorly into the anterior cranial fossa and frontal lobes, ethmoid and sphenoid sinuses. A biopsy of this mass confirmed high grade olfactory neuroblastoma. Because of the intra-cranial extension, a decision was made to start neoadjuvant chemotherapy with cisplatin and etoposide. The patient had very good response to this treatment on a repeat imaging study and went on to have resection of this mass. Post-operatively, he received radiation therapy to the tumor bed and 2 more cycles of chemotherapy. He has been followed now for more than 8 months with no evidence of disease recurrence.
Introduction
Olfactory neuroblastoma (esthesioneuro-blastoma) is a rare malignant tumor of neuroectodermal origin. It is thought to arise from the olfactory epithelium that lines the superior third of the nasal septum, cribriform plate, and superior turbinates. Since Berger and Luc's initial report in 1924, approximately 1,000 cases have been reported with 5-year survival rate in the order of 60–70%. 1 The most common symptoms at the time of presentation are nasal obstruction (52%), epistaxis (42%), exophthalmos (19%), and headache (19%). 2 The age distribution of patients is unimodal with the majority of patients presenting at diagnosis in the 4th and 5th decades of life yet presentation in patients under 30 years of age is not uncommon. 3
There is no universally accepted staging system for olfactory neuroblastoma. Kadish et al were the first to propose a staging system based on a series of 17 patients. 4 Patients were classified into 3 stages: stage A, tumor confined to nasal cavity; stage B, tumor extends to one or more of the paranasal sinuses; and stage C, where the tumor extends beyond the nasal cavity and paranasal sinuses. Morita et al modified the Kadish staging system by re-classifying patients with lymph node or distant metastases as stage D. 5
The two most important factors influencing prognosis in patients with olfactory neuroblastoma are extent of disease at diagnosis and histologic grade.6,7 Survival rates have been reported to correlate with S-100 protein immunoreactivity and a low Ki-67 labeling index (<10%). 8 Intracranial extension and orbital involvement have been shown to be independent risk factors associated with poorer outcomes. 9 Lymph node status and age are also considered useful predictors of outcome. 3
A study of 311 patients based on Surveillance, Epidemiology and End Results (SEER) database showed that disease-specific survival at 10 years correlated with modified Kadish staging (83%, 49%, 39%, and 13% for stages A, B, C, and D, respectively). 3 There are no reported randomized trials to guide treatment in patients with olfactory neuroblastoma. The combination of surgery and adjuvant radiotherapy is the most widely used approach in patients with locally advanced disease.9,10 A review of 390 cases (1990–2000) showed that surgery plus radiation resulted in a five-year survival rate of 65%, compared with 48% with surgery alone. 6
Chemotherapy has been advocated, either in the adjuvant or neoadjuvant setting, in varying protocols.11–13 The capacity of induction chemotherapy to convert a previously unresectable presentation to one that is capable of complete surgical extirpation has been reported. 11 The following is a case report that is emblematic of successful multimodality management in a patient with locally advanced olfactory neuroblastoma with intracranial spread.
Case Report
A 46-year old male presented with an 8-month history of progressive nasal obstruction and intermittent right-sided epistaxis. He had experienced several weeks of anosmia and increased pressure sensation in and around the right eye with decreased visual acuity and diplopia on rightward gaze. His general health was without significant comorbidities. He was a nonsmoker and worked as an aircraft painter.
On examination, nasal endoscopy revealed a bulging mass arising from a region superior to the middle turbinate on the right side. An MRI of the sinuses showed a large enhancing heterogeneous cystic and solid mass in the right nasal cavity measuring 5.0×5.3×4.6 cm with extension superiorly into the anterior cranial fossa and frontal lobes, ethmoid and sphenoid sinuses with compression and erosion of the medial wall of the right maxillary sinus (Figure 1). A PET/CT scan showed intense radiotracer uptake in the large soft tissue mass that in the posterosuperior nasal cavity with Standard Uptake Value (SUV) of 35 without evidence of regional or distant spread. A biopsy of the mass revealed a high-grade olfactory neuroblastoma with extensive tumor necrosis, apoptosis with Ki67 staining of greater than 60%.
Magnetic resonance imaging of the head at patient presentation, before receiving the neoadjuvant chemotherapy.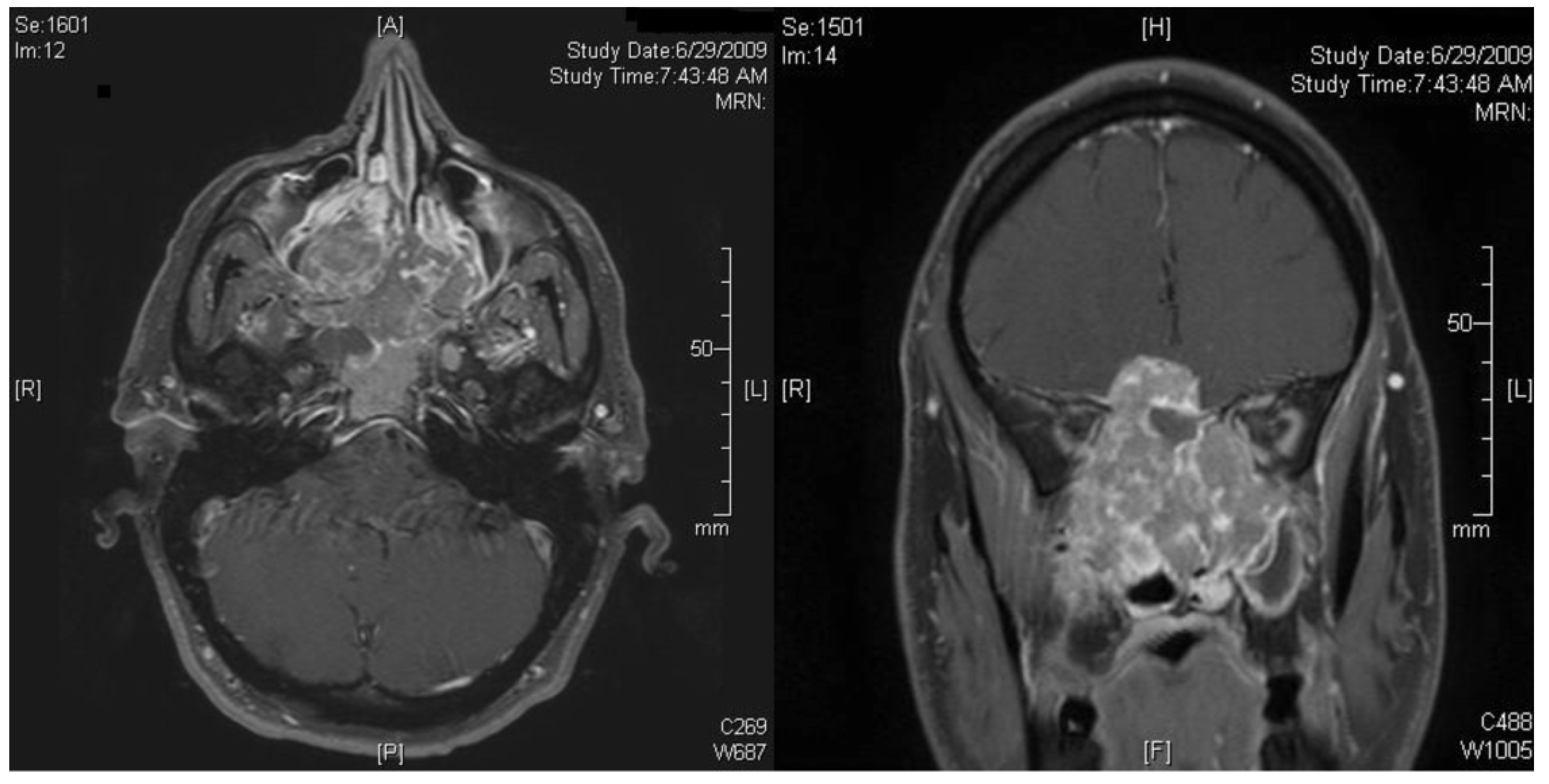
Immunohistochemical staining confirmed the tumor was positive for CAM5.2, neuron-specific enolase, synaptophysin, pankeratin and S-100 and negative for chromogranin A, TTF-1, CD99 and lymphoid and hematopoietic factors. The tumor was considered to be a Hyam's grade IV tumor, Kadish stage C.
Neoadjuvant therapy was considered because of the intracranial spread of tumor that would necessitate resection a considerable portion of the frontal lobe of the brain in a attempting to obtain negative margins at the time of surgery. Neoadjuvant chemotherapy was initiated with two cycles (cisplatin 75 mg/m2 on day 1 and etoposide 100 mg/m2 on days 1, 2, and 3, cycles repeated every 21 days). During this phase treatment, the patient's persistent headache, periorbital pressure and diplopia all resolved. Post-induction MRI demonstrated a major interval decrease in the size of the mass with resolution of the previous noted imaging-based evidence of intracranial extension (Figure 2).
Magnetic resonance imaging of the head after receiving the neoadjuvant chemotherapy, showing considerable decrease in the size of the tumor.
The patient went on to have an endoscopic assisted craniofacial resection with resection of dural, septectomy, and bilateral medial maxillectomies and anterior/posterior ethmoidectomies. The patient was reconstructed with a vascularized pericranial flap. At the time of surgery all gross tumor was removed with margins assessed by intraoperative frozen section assessment. The frontal lobe of brain demonstrated no evidence of viable tumor present, allowing for a more conservative resection in this region. Final histopathological results of the specimen showed the tumor to be 1.2×0.6 cm in diameter with margins were free of tumor. Postoperatively, the patient healed well without evidence cerebrospinal leak and concurrent adjuvant chemoradiation was initiated. The patient received 54 Gy of radiation to the tumor bed in 27 fractions. The patient was to receive 2 cycles of cisplatin and etoposide protocol concurrent with radiation therapy however because of symptoms of nausea and extreme fatigue associated with treatment, the second cycle of chemotherapy was withheld. The patient has been followed clinically and with repeated imaging for more than 8 months and has demonstrated no evidence of disease local recurrence (Figure 3).
Magnetic resonance imaging of the head after surgical resection, showing no evidence of residual tumor.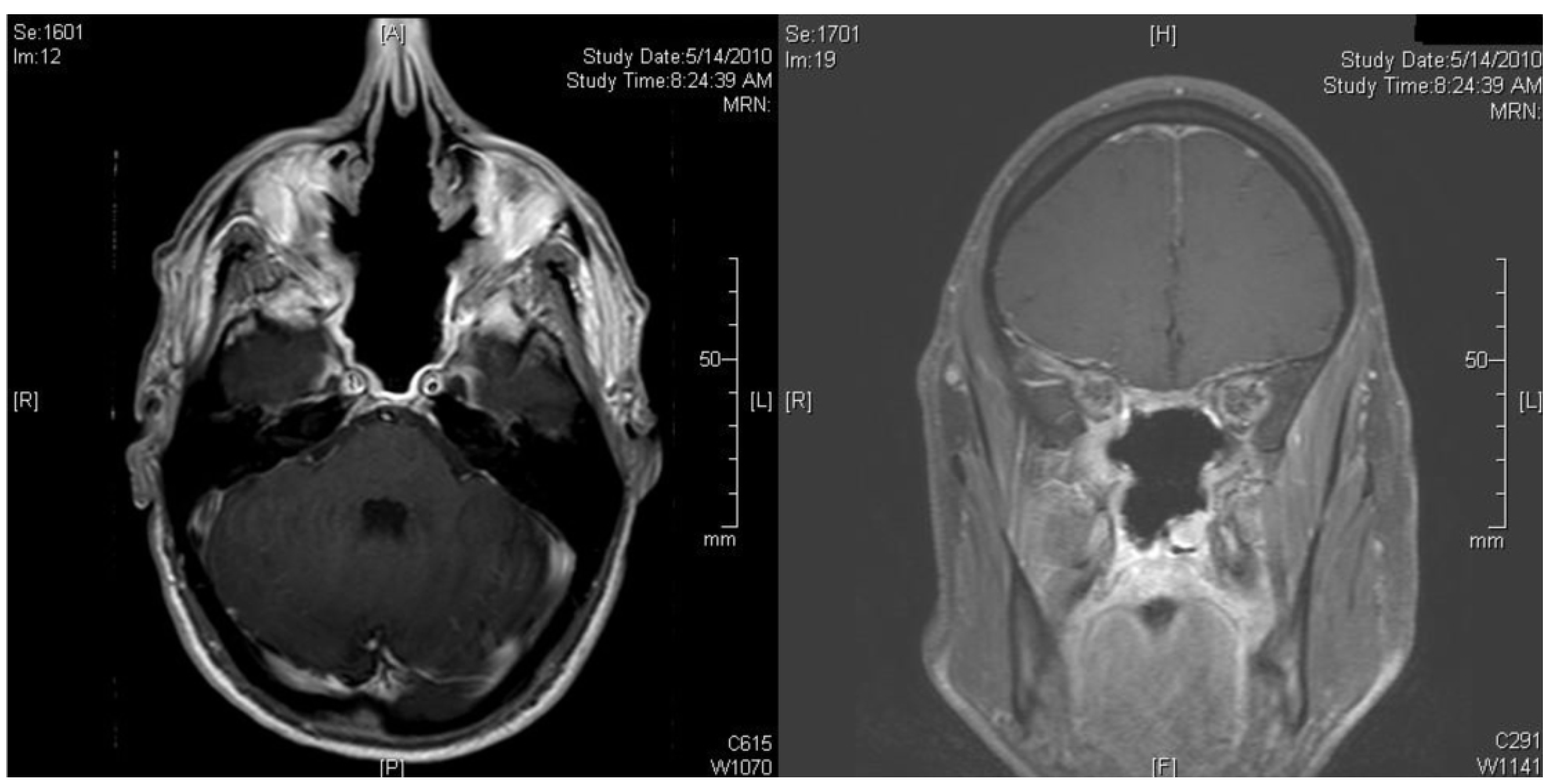
Discussion
The optimal treatment modality for olfactory neuroblastoma continues to be debated because of limited cohort size and treatment inconsistencies previously reported in the medical literature. Earlier staged lesions (Kadish A & B) have typically been described as being treated with a monomodality regimen such as surgery or radiation. Radical surgical resection has been shown to result in improved 5-year survival rates (76.2% vs. 14.3%) when compared to radiation alone when monomodality therapy is performed. 2 Tumor grade, low versus high, has been used to direct the indication for adjuvant therapy after surgical resection. Radiation therapy has been advocated for low-grade lesions with close margins, residual and recurrent disease and in all patients with high-grade tumors. 5
Kadish stage C patients have typically been advocated to receive combination therapy such as surgery with adjuvant radiation therapy. The use of combined modality treatment with surgery, radiotherapy and chemotherapy in various combinations has been increasingly adopted over the last two decades.7,14,15 The use of neoadjuvant chemotherapy for Kadish stage C disease has been reported in retrospective cohort studies. 16 Various chemotherapeutic combination regimens have been used involving alkylating agents and anthracylines with significant toxicities.13,16 Response to chemotherapy may be dependent upon the Hyam's grading of the original tumor. McElroy et al. noted that high-grade olfactory neuroblastoma was sensitive to cisplatin-based chemotherapy. 7
Fitzek et al.examined the use of neoadujvant chemotherapy for olfactory neuroblastoma and neuroendocrine carcinoma in 19 patients with Kadish stage B [4] and C [15] disease. 12 In this study patients received two cycles of cisplatin (33 mg/m2/d) and etoposide (100 mg/m2/d) and were re-assessed with repeat imaging. A significant response, of greater than >50% reduction in tumor dimensions, (partial or complete) was seen in 13 patients. If less than a partial response was noted, surgical resection prior to radiotherapy was recommended. Postoperatively, the patients underwent radiation via high-dose proton-photon beam radiotherapy to 69.2 cobalt-Gray equivalents. Alternatively, if the patient experienced a significant response to induction chemotherapy went directly to radiotherapy followed by 2 additional cycles of chemotherapy. For persistent disease after radiation in this group, salvage surgery was offered. With a median follow up of 45 months, 15 of the 19 patients were alive and free of disease. There were 2 local recurrences and the 5-year local control rate and overall survival were 88% and 74% respectively. Our patient's induction treatment parallels this study's approach, however the significant response to initial chemotherapy was used to aid surgical management of what was previously unresectable tumor. 12
Polin et al. advocate preoperative chemoradiation noting that it results in a reduced tumor burden and thus increases the likelihood of complete resection and long-term disease-free progression. 17 In the University of Virginia protocol, 34 patients with advanced disease were initially treated with two cycles of cyclophosphamide (300–650 mg/m2) and vincristine (1–2 mg), followed by 50 Gy of radiation therapy prior to definitive surgical resection. Two-thirds of patients showed a significant response in tumor burden with neoadjuvant treatment and these patients experienced a lower rate of disease-related mortality when compared to nonresponders. 17 Disease free survivals of 86.5% at 5 years and 82.6% at 15 years have been reported with this protocol. 16 These survival rates are significantly higher than those cited for surgery followed by adjuvant radiation (65% at 5 years) cited by Dulguerov et al. in their meta-analysis. 6 Kim et al. reported on their use of neodjuvant etoposide (75 mg/m2), cisplatin (20 mg/m2), and ifosfamide (1000 mg/m2) for olfactory neuroblastoma. In their study they reported objective responses in 9 of 11 patients (2 complete, 7 partial) with the most common significant toxicity being grade 3/4 neutropenia (37%). 18
Conclusions
Neoadjuvant chemotherapy consisting of etoposide and cisplatin is a potentially effective therapeutic option in the treatment of locally advanced esthesioneuroblastoma prior to surgical resection. Due to the rarity of this tumor larger, multi-institutional studies will be necessary to validate the efficacy of this treatment in comparison to current protocols using chemotherapy exclusively in the adjuvant setting.