
Abstract
Introduction:
Multiple trials demonstrated that adding Bevacizumab to the standard neoadjuvant chemotherapy in HER-2 negative breast cancer increases pathological complete response. We conducted this meta-analysis to evaluate that effect on survival.
Methods:
We performed a systematic search for randomized trials measuring the effect of adding either neoadjuvant or adjuvant Bevacizumab to the standard chemotherapy on disease-free and overall survival in breast cancer surgical candidates. The Mantel-Haenszel method and random effect model were used to analyze the data. A total of 7 randomized controlled trials were included in the analysis with a mean follow-up of 45 months.
Results:
No statistically significant difference in overall survival was found after adding Bevacizumab to the standard chemotherapy in the overall study population, HR=0.9, 95% CI (90.72–1.13), estrogen/ progesterone positive subgroup, HR=0.99, 95% CI (0.72–1.35), or in triple negative breast cancer, HR=0.88, 95% CI (0.77–1.01). However, there was a small but significant improvement in disease-free survival in triple negative breast cancer with a HR of 0.88, 95% CI (0.78–0.98), but not in estrogen/ progesterone receptor positive tumors, HR=1.01, 95% CI (0.81–1.26).
Conclusions:
The addition of Bevacizumab along with the standard chemotherapy would not improve overall survival in breast cancer surgical candidates, however, due to a small but significant improvement on disease-free survival in triple negative breast cancer, that would not eliminate the possibility of a certain subgroup of the latter who might benefit from adding Bevacizumab.
Introduction
Breast cancer is the second leading cause of cancer-related death in women. Multimodality treatments in the form of chemotherapy, radiation, and surgical resection lead to improvement in overall survival (OS). A wide variety of chemotherapeutic agents have achieved a drastic tumor response when being used in the neoadjuvant setting. 1 This applies especially for HER-2–positive breast cancer, in which up to 60% of the tumors respond to neoadjuvant chemotherapy (NAC).2,3
Response to NAC, measured by pathologic complete response (pCR) at the time of surgical resection, is correlated with event-free survival (EFS) and OS. 1 In the Collaborative Trials in Neoadjuvant Breast Cancer (CTNeoBC) consortium’s analysis, which included 12 trials with 11 955 patients, subjects with pCR in both the breast and axilla (ypT0 ypN0 or ypT0/IS ypN0) had statistically significant improvement in EFS and disease-free survival (DFS) compared with those who did not. 1 This association was strongest among triple-negative and hormonal receptor–negative, HER-2–positive patients with breast cancer and high-grade hormonal receptor–positive tumors. 1 This association was significant when the analysis was done at the individual data level but not at the trial level. 1
The American Society of Clinical Oncology (ASCO) and College of American Pathologists (CAP) define breast cancers that have less than 1% expression of estrogen and progesterone receptor (ER and PR) and either 0 or +1 HER-2 receptor expressions in immunohistochemistry (IHC) or an absence of HER-2 amplification in fluorescent in situ hybridization if IHC was +2 as triple-negative breast cancer (TNBC). 4 Advanced cancer grade, aggressive histological subtypes, mutations at the tumor suppressor genes, such as P53, and BRACA genes with the lack of targeted therapy make TNBC have the worst prognosis among all types of breast cancer.5,6 However, NAC offers a survival advantage in rapidly proliferating HER-2–positive and TNBC subjects who achieved pCR, as Cortazar et al 1 proposed.
Bevacizumab is a monoclonal antibody that inhibits the activity of vascular endothelial growth factors (VEGFs). 7 Different subtypes of VEGFs have been identified. Stimulation of endothelial cells through VEGF subtype A results in endothelial cell proliferation, the sprouting of new blood vessels, an increase in endothelial cell permeability, and destruction of the surrounding extracellular matrix. 7 Therefore, inhibition of VEGF-A would inhibit angiogenesis, which is the critical step in cancer metastasis. Moreover, bevacizumab enhances the delivery of other chemotherapeutic agents to the tumor cells through pruning and remodeling of the tumor blood vessels, 8 which would account for the major therapeutic benefit of bevacizumab when used in a variety of metastatic cancers along with other chemotherapeutic agents. After being Food and Drug Administration (FDA) approved for use in metastatic breast cancer, bevacizumab has lost its FDA approval in that setting due to the lack of survival benefit, despite having a significant effect in improving disease progression.8,9
Several trials have evaluated the effect of adding bevacizumab to NAC on pCR, OS, and DFS in patients with breast cancer. The emphasis was, in particular, on HER-2–negative breast cancer, which lacks targeted therapy. Despite the significant improvement in overall pCR after adding bevacizumab to NAC in these trials, this effect varies based on the tumor hormonal receptor expression. Furthermore, whether this improvement in pCR would be translated into improvement in DFS or OS is yet to be determined.
The risk of both local and distant recurrence in surgically resected breast cancer decreases substantially after 5 years of follow-up, which is particularly true for subjects with TNBC and HER-2–positive breast cancer.10,11 Although Cao et al 12 conducted a meta-analysis to evaluate the effect of neoadjuvant bevacizumab on pCR in patients with breast cancer, its effect on disease recurrence and OS was not assessed. Moreover, their analysis on pCR in TNBC population included only 2 trials (GeparQuinto and NSABP B-40). Therefore, we conducted this meta-analysis to evaluate the effect of adding bevacizumab in either a neoadjuvant or adjuvant setting in HER-2–negative breast cancer on DFS and OS in both the overall study population and subgroups based on subjects’ hormonal receptor expression as well as presenting its effect briefly on pCR in HER-2–negative breast cancer.
Methods
Search strategy
We use the PRISMA statement for reporting meta-analysis and systemic reviews as shown in Diagram 1. We have searched the studies published by June 30, 2017, through Cochrane library databases, PubMed, Clinicaltrial.gov, and Scopus databases from inception. We used the MeSH terms “neoadjuvant chemotherapy,” “Breast Cancer,” and “Bevacizumab” connected with the Boolean operator “AND” for Cochrane library database and PubMed. We used the following Boolean strategy (neoadjuvant chemotherapy), (Breast Cancer) AND (Bevacizumab) for search in Clinicaltrial.gov and Scopus. We reviewed all articles, excluding the articles that were not in English. Publication bias was not assessed due the small number of the studies analyzed.

tpCR: Absence of the invasive disease in the breast and lymph nodes in the overall study population. tPCR indicates pathologic complete response.
The eligibility criteria for our meta-analysis included the following. (1) Randomized controlled trials comparing subjects who received bevacizumab and chemotherapy vs chemotherapy alone in either a neoadjuvant or adjuvant setting with curative intent (nonmetastatic breast cancer). (2) HER-2 negative status as per ASCO/CAP definition. (3) Full published articles in a peer-reviewed journal as well as abstracts presented at oncology conferences. (4) Studies with one of the following available as their primary or secondary outcomes: pCR, ²²EFS, DFS, and OS.
Exclusion criteria included the following: (1) nonrandomized trials and (2) using bevacizumab in metastatic breast cancer. A total of 7 randomized clinical trials met our inclusion criteria and were included in our meta-analysis. These trials are Artemis,13,14 Geparquinto,15–17 NSABP B-40, 18 Beatrice, 19 CALGB (40603),20,21 SWOG S0800, 22 and Eastern Cooperative Group E5103. 23
Statistical analysis
All outcomes were calculated using RevMan, version 5.3, for Windows (Cochrane Collaboration, Oxford, UK). The pooled hazard ratio was calculated using a random effect model to overcome the heterogeneity of the included studies. Results were reported with 95% confidence interval (CI), with a P value of <.05 considered significant. Cochran’s Q-statistic was used to calculate statistical heterogeneity and the I2 statistic was used to measure the statistical heterogeneity between trials. Statistical heterogeneity was considered to be significant when the associated P value was below .1.
Outcomes of interest
(1) Total pCR (tpCR) (defined as the absence of invasive disease in the breast and lymph nodes [ypT0/IS ypN0]), (2) pCR (defined as the absence of invasive disease in the breast only [ypT0/IS ypN0/+]), (3) disease- or invasive DFS, and (4) OS. We also subanalyzed each of the previous outcomes according to the hormonal receptor status based on the data available in the included trials.
Characteristics of the Included Studies
The NSABP B-40, Artemis, GeparQuinto, and SWOG S0800 trials evaluated the effect of neoadjuvant bevacizumab on HR+, HR−/HER-2− tumors. However, 10 cycles of adjuvant bevacizumab were added in the NSABP B-40 trial. While 6 cycles of neoadjuvant bevacizumab were used in the NSABP B-40, GeparQuinto, and SWOG S0800 trials, only 4 cycles were used in the Artemis trial. These trials reported pCR as their primary outcome. Overall survival and DFS were reported as their secondary outcomes after a mean follow-up of 4 years.
Different definitions of pCR were reported in these trials. In our meta-analysis, the term pCR was defined as the absence of invasive disease in the breast irrespective of the lymph nodes (yT0/IS, N0/+), whereas tpCR was defined as the absence of invasive disease in both the breast and lymph nodes (yT0/IS, N0) with carcinoma in situ being allowed in both definitions.
Taking the above-mentioned definitions for pCR and tpCR into consideration, the NSABP B-40 trial has data for pCR but not for tpCR. However, the Artemis trial has data for both pCR and tpCR for the overall study population and their hormonal receptor subgroups. As in the Artemis trial, GeparQuinto has data for both pCR and tpCR for the overall study population and for TNBC. However, for ER/PR+ tumors, GeparQuinto has data only for tpCR which is defined as the absence of both invasive and noninvasive residuals in the breast and invasive disease in the lymph nodes (ypT0 ypN0).
CALGB (40603) evaluated the effect of 9 cycles of neoadjuvant bevacizumab on pCR and tpCR as defined in our meta-analysis in HR−/HER-2− tumors. However, 1 year of adjuvant bevacizumab was given in the Beatrice trial, which reported its effect on invasive DFS, DFS, and OS after a mean follow-up of 4.7 years.
As for pCR, different cutoffs were used to define ER/PR+ tumors in these trials. GeparQuinto defined ER/PR+ breast cancers as those that had expression of 10% or more of either one of these receptors, whereas the cutoff of 1% was used in the NSABP B-40, Eastern Cooperative Oncology Group E5103, and SWOG S0800 trials. The Artemis trial divided breast cancer into 3 categories based on their ER/PR Allred score. Tumors with a 0-2/8 Allred score were labeled as ER/PR−, an Allred score of 3-5/8 as weakly positive hormonal receptor tumors, and an Allred score of 6-8/8 as strongly positive hormonal receptor tumors. An Allred score of more than 3 was considered to be hormonal receptor positive in our meta-analysis as per the ASCO/CAP definition. 3
The CALGB (40603) and Beatrice trials included TNBC only. Tumors with ER/PR expression of less than 10% were included in the former, whereas tumors with an Allred score of 3/8 and less were included in the latter.
SWOG S0800 and Beatrice were phase 2 randomized controlled trials, and all other studies were phase 3.
Characteristics of each study are summarized in Table 1.
Characteristics of the included studies.

Abbreviations: ER, estrogen receptor; LNs, lymph nodes; pCR, pathologic complete response; PR, progesterone receptor.
E: epirubicin, C: cyclophosphamide, D: docetaxel.
T: docetaxel, A: doxorubicin, C: cyclophosphamide, X: capecitabine, G: gemcitabine.
T: docetaxel, E: epirubicin, C: cyclophosphamide, F: 5-fluorouracil.
wP-AC: once-weekly paclitaxel, A: doxorubicin, C: cyclophosphamide.
dd AC: dense dose doxorubicin and cyclophosphamide (60 mg/m2 and 600 mg/m2, respectively).
Results
Total pCR
A pooled analysis from 3 trials (Artemis, GeparQuinto, and SWOG S0800) with a sample size of 2917 resulted in a statistically significant effect of bevacizumab on tpCR for the overall study population (hormonal receptor–positive and negative and HER-2–negative breast cancers) with an HR of 1.37, 95% CI (1.10-1.71), as shown in Figure 1.

tpCR: Absence of the invasive disease in the breast and lymph nodes in the overall study population. tPCR indicates pathologic complete response.
The effect of bevacizumab on tpCR was marked in TNBC. The analysis of the Artemis, GeparQuinto, CALGB (40603), and SWOG S0800 trials, with a sample size of 1404 patients, revealed an HR of 1.61, 95% CI (1.27-2.05), in favor of the bevacizumab arm, as shown in Figure 2. However, the effect of bevacizumab on tpCR in ER/PR+ tumors was not statistically significant, as shown in Figure 3.

tpCR (TNBC): Absence of invasive disease in the breast and lymph nodes in triple-negative breast cancer. tPCR indicates pathologic complete response.
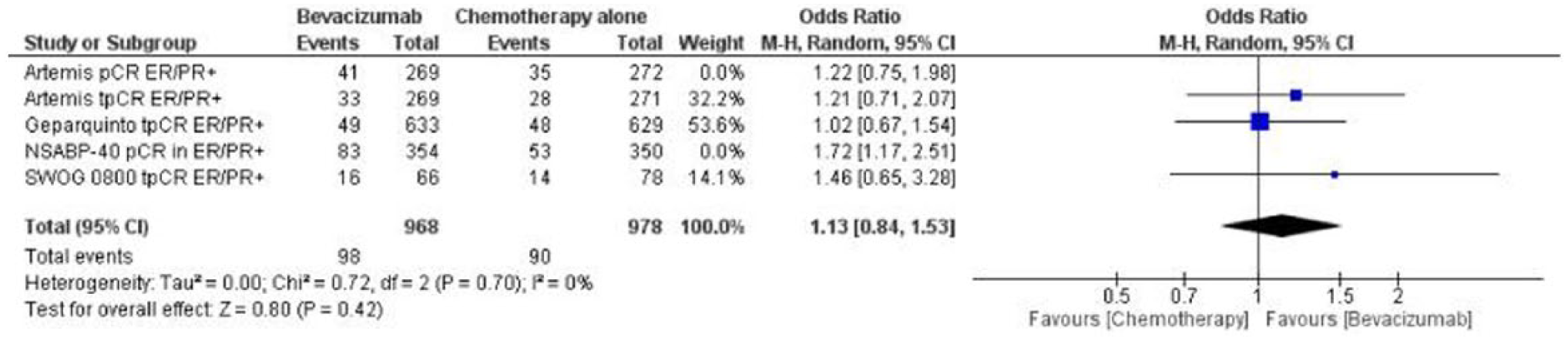
tpCR (ER/PR+): Absence of invasive disease in the breast and lymph nodes in ER/PR+ breast cancer. ER indicates estrogen receptor; PR, progesterone receptor; tPCR, total pathologic complete response.
Pathologic complete response
The pooled analysis of the 3 trials, Artemis, GeparQuinto, and NSABP-40, with a sample size of 3887 patients, resulted in a statistically significant effect on pCR in favor of the bevacizumab arm with an HR of 1.31, 95% CI (1.13-1.52), as shown in Figure 4.

pCR: Absence of invasive disease in the breast only in the overall study population. pCR indicates pathologic complete response.
The effect of bevacizumab on pCR was statistically significant in both TNBC and ER/PR+ breast cancer with an HR of 1.48, 95% CI (1.23-1.78) and HR of 1.50, 95% CI (1.08-2.08), respectively, as shown in Figures 5 and 6.

pCR (ER/PR–positive tumor): Absence of invasive disease in the breast only in ER/PR positive, HER-2–negative breast cancer. ER indicates estrogen receptor; pCR, pathologic complete response; PR, progesterone receptor.

pCR (TNBC): Absence of invasive disease in the breast only in triple-negative breast cancer. pCR indicates pathologic complete response.
Disease-free survival
The effect of bevacizumab on DFS in the overall study population (ER/PR+, ER/PR−, and HER-2–negative breast cancer) was evaluated in the GeparQuinto, NSABP B-40, Artemis, E5103, and SWOG S0800 trials. The pooled analysis of these trials included 7117 patients with a mean follow-up of 45.5 months. The results revealed no statistically significant difference in DFS between bevacizumab-treated and non–bevacizumab-treated groups with an HR of 0.95, 95% CI (0.82-1.09), as shown in Figure 7.

DFS overall: Disease-free survival in the overall study population.
Subanalysis for the effect of bevacizumab on DFS in ER/PR-positive tumors also did not reveal a significant difference with an HR of 1.01, 95% CI (0.81-1.26), as shown in Figure 8. Due to high heterogeneity of the included trials, sensitivity analysis was done by eliminating one trial at a time. The heterogeneity became insignificant after eliminating NSABP B-40 trial from the analysis and the result remains insignificant for this subgroup as shown in Figure 9.

DFS in ER/PR+/HER-2–negative breast cancer: Disease-free survival in ER/PR+, HER-2–negative breast cancer. ER indicates estrogen receptor; PR, progesterone receptor.

DFS in ER/PR+ HER-2–negative tumors, after excluding NSABP B-40 trial from the analysis. DFS indicates disease-free survival; ER, estrogen receptor; PR, progesterone receptor.
In addition to the beforementioned trials, the Beatrice and CALGB (40603) trials were included in the subanalysis for the effect of bevacizumab on DFS in TNBC. The analysis included 7491 patients with a mean follow-up of 46 months. The result was statistically significant in favor of the bevacizumab arm with an HR of 0.88, 95% CI (0.78-0.98), as shown in Figure 10.

DFS (TNBC): Disease-free survival in triple-negative breast cancer.
Overall survival
The OS after using bevacizumab in the overall study population was evaluated in the Artemis, GeparQuinto, NSABP B-40, E5103, and SWOG S0800 trials. The analysis included 7119 subjects. After a mean follow-up of 45.5 months, no statistically significant difference in OS was found between the bevacizumab-treated and non–bevacizumab-treated arms with an HR of 0.90, 95% CI (0.72-1.13), as shown in Figure 11.

OS: Overall survival in the overall study population.
Similar trials were used in the subanalysis for the effect of bevacizumab on OS in ER/PR+ tumors. A total of 5657 patients were included in the pooled analysis with a mean follow-up time of 45.5 months. No significant effect was found in the bevacizumab group in terms of OS with an HR of 0.99, 95% CI (0.72-1.35), as shown in Figure 12. Due to high heterogeneity of the included trials, sensitivity analysis was done by eliminating one trial at a time. The heterogeneity became insignificant after eliminating NSABP B-40 trial from the analysis and the result remains insignificant for this subgroup as shown in Figure 13.

OS in ER/PR+ HER-2–negative tumors: Overall survival in ER/PR+, HER-2–negative breast cancer. ER indicates estrogen receptor; PR, progesterone receptor.

OS in ER/PR+ HER-2–negative tumors, after excluding NSABP B-40 trial from the analysis. ER indicates estrogen receptor; PR, progesterone receptor.
Beatrice and CALGB (40603) were added to the previous trials in the subanalysis on OS in TNBC. The pooled results were not statistically significant with an HR of 0.88, 95% CI (0.77-1.01), as shown in Figure 14.

OS TNBC: Overall survival in triple-negative breast cancer.
Interestingly, the GeparQuinto and Artemis trials revealed more DFS events in the bevacizumab-treated group when taking into account only the subjects who achieved pCR, as shown in Figure 15.

DFS in patients who achieved pCR. DFS indicates disease-free survival; pCR, pathologic complete response.
Discussion
As noted earlier, the meta-analysis of Cortazar et al 1 revealed significant improvement in DFS and OS in patients with breast cancer who achieved pCR at the individual level. The insignificant association between pCR and survival at the trial level was likely due to the heterogeneity of breast cancer subgroups who were included in each trial. 1 Bevacizumab is a monoclonal antibody which targets VEGF receptors and it has been used in a wide variety of malignancies, such as colorectal cancer, non–small-cell lung cancer, glioblastoma multiforme, renal cell carcinoma, and many others. 6 Enhancing the delivery of other chemotherapy to the tumor tissue and preventing new blood vessel formation are the major mechanisms by which it inhibits tumor growth, invasion, and metastasis.6,7
GeparQuinto,15–17 Artemis,13,14 and CALGB (40603)20,21 used bevacizumab as an NAC in breast cancer surgical candidates. These trials revealed a statistically significant effect on pCR in the bevacizumab-treated group compared with the control group in both the overall study population and in TNBC but not in ER/PR+ tumors. For tpCR, Artemis13,14 and GeparQuinto15–17 revealed a statistically significant effect in favor of the bevacizumab arm in TNBC only. Furthermore, SWOG S080022 results showed that bevacizumab had a statistically significant effect on tpCR in the overall study population and in TNBC but not in ER/PR–positive tumors. However, the NSABP B-40 trial 18 showed that bevacizumab had a statistically significant effect on pCR in the overall study population and in ER/PR+ tumors but not in TNBC (the effect on tpCR was not studied).
In our meta-analysis, only pCR, not tpCR, was significant in ER/PR+ breast cancer when treated with bevacizumab. Of note, this analysis included only 2 trials (Artemis and NSABP B-40) as GeparQuinto does not have data on pCR in this subgroup. However, both pCR and tpCR were significant in TNBC when it was treated with bevacizumab compared with the standard chemotherapy with an odds ratio of 1.48 and 1.61, respectively. Our meta-analysis in TNBC showed that 452 subjects in the bevacizumab arm achieved pCR compared with 384 subjects in the standard chemotherapy arm, and 325 achieved tpCR in the bevacizumab arm compared with 256 in the standard chemotherapy arm. This result yields an absolute risk reduction of 11.2% and 9.6%, respectively, with a corresponding number need to treat 10.4 and 8.7, respectively.
Despite the fact that bevacizumab-treated groups had significant results in terms of pCR, this was not translated into improvement in OS either in the overall study population or in the subgroups based on their HR expression after a mean follow-up of 45.5 months, as shown in our meta-analysis.
However, our meta-analysis revealed that bevacizumab had a statistically significant effect on DFS in TNBC only and after a mean follow-up of 46 months with an HR of 0.88, 95% CI (0.78-0.98). However, this result should be interpreted with caution because analysis of DFS for both the Artemis and GeparQuinto trials revealed a statistically significant worse DFS in the subjects who achieved pCR in the bevacizumab arm when compared with those who achieved pCR with the standard chemotherapy alone, as shown in Figure 15. Moreover, if we take into consideration the number of DFS events for TNBC in the Artemis, Beatrice, NSABP B-40, CALGB (40603), and SWOG S0800 trials (which had data for DFS events in TNBC) in the bevacizumab arm compared with that in the standard chemotherapy arm, as shown in Table 2, it yields an absolute risk difference of 1.6% in favor of the bevacizumab arm with a number needed to treat of 63. Therefore, a sizable number of patients who achieved pCR in TNBC using bevacizumab had DFS events and we would need to treat many TNBC subjects using bevacizumab to translate this improvement in pCR into a disease-free and even OS benefit.
Disease-free survival events in TNBC.

Abbreviation: TNBC, triple-negative breast cancer.
Number needed to treat to prevent one disease-free survival event. NNT = 1/(0.205 − 0.189) = 63 subjects.
Many theories would explain the previous findings; bevacizumab enhances the delivery of other chemotherapeutic agents to the tumor milieu through pruning of the blood vessels, which would explain its effect on grossly large tumors. However, theoretically speaking, micro-metastasis and tumor stem cells serve as a nidus for later recurrence after resection of the primary tumor and it is unlikely to be eliminated by VEGF inhibitors. 13 Moreover, a lack of effect on cancer stem cells could stimulate these cells to develop cellular pathways to overcome VEGF inhibitors; this theory would explain the possible rebound phenomena which was observed when bevacizumab was given in the adjuvant setting along with oxaliplatin in colon cancer, in which worse OS was noted in the bevacizumab-treated group. 24 In contrast to the bevacizumab, improvement on EFS after adding trastuzumab to the NAC in HER-2–positive tumors was more pronounced in patients who had achieved pCR with an HR of 0.29. 25
As expected, more side effects were observed in the bevacizumab-treated groups in these trials, eg, in the NSABP B-40 trial, 16 patients who were treated with bevacizumab had more frequent hypertension, hand-foot syndrome, and mucositis. In the GeparQuinto trial, 13 the number of patients who had either a delay in their chemotherapy or dose reduction was higher in the bevacizumab group than in the standard chemotherapy group, 43.1% vs 35.6% and 20.8% vs 12.5%, respectively. Cao’s meta-analysis showed that bevacizumab-treated group had a statistically and clinically significant odds of having fatigue, hand-foot syndrome, surgical complications, thrombocytopenia, neutropenia, and neutropenic fever. Moreover, their analysis revealed that neoadjuvant bevacizumab did not have a significant effect on conservative breast cancer surgery. Nonetheless, these results would not exclude certain subgroups of patients with TNBC who might benefit from receiving bevacizumab as neoadjuvant treatment, such as those with a high VEGF serum level as shown in the Beatrice trial, in which subjects with serum VEGF of 133.6 pg/mL and more tended to have fewer invasive DFS events, although the result was not statistically significant.
Our meta-analysis has some limitations:
First, it is a retrospective pooled analysis at the trial level. Such analysis would not take into account the difference in patient’s characteristics among the included trials, such as the type of chemotherapy, number of cycles being used and percentage of patients who completed the preplanned chemotherapy, and sequence of and time interval between different chemotherapeutic regimens. In our analysis, we used a random effect model to overcome this heterogeneity. Although analysis of DFS and OS in ER/PR+ tumors yielded high heterogeneity, eliminating the NSABP B-40 trial from that analysis would bring the heterogeneity to a nonsignificant level without affecting the results.
Second, different cutoffs for the level of ER/PR receptors in the tumor burden or their intensity as per the Allred score were used in these trials, which further increases the heterogeneity of the included population.
Third, the possible presence of confounding factors which could increase pCR and thus survival in certain TNBC subgroups, such as degree of lymphocytic infiltration, T-cell signatures, and programmed cell death ligand level, was not assessed in these trials. 26
Conclusions
Although bevacizumab increased the pCR when used as a neoadjuvant or adjuvant chemotherapy in nonmetastatic breast cancer, no significant improvement in OS after a mean follow-up of 45 months was noted. However, the slight but significant increase in DFS in TNBC would not eliminate the possibility of certain TNBC subgroups who might benefit from the treatment. Future trials on certain subgroups of TNBC, such as those with high VEGF, might unveil these subgroups.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
YA: Conception of the idea, review all relevant articles, statistical analysis and writing the manuscript. ZH: Review all relevant articles and writing the manuscript. KK: Review and drafting the manuscript.