
Abstract
Clinical Relevance
In recent years, an increased posterior tibial slope has been identified as a nonmodifiable risk factor for anterior cruciate ligament (ACL) injury and increased failure rates after ACL reconstruction (ACLR). To date, the literature consists of clinical case series on slope reducing high tibial osteotomies and reports promising clinical results. However, higher case numbers are still lacking. The goal of the present series of anterior-closed-wedge high tibial osteotomies (ACW-HTO) was to analyze patient-reported outcome measures (PROMs) at a minimum of 2 years. It was hypothesized that an ACW-HTO with secondary ACLR after failed ACL surgery improves clinical outcome as compared with the pre-osteotomy state or can even give sufficient stability to avoid the need for revision ACLR.
Material and methods
One hundred consecutive cases with an ACW-HTO operated between February 2019 and December 2022 were included in 2 surgical centers (57 cases radiographic/51 cases with PROMs Sozialstiftung Bamberg and 43 cases radiographic/35 cases with PROMs Sporthopaedicum Berlin, Germany). The pre-injury (before first injury), the preoperative (before ACW-HTO), and the final postoperative conditions were documented using PROMs.
Results
The mean follow-up was 36 months (SD ±11, range 24-82), the follow-up rate for the PROMs was 85%. The mean preoperative slope of 14.6° (SD ±2.4°; range 11°-28°), measured according to the method of Dejour and Bonnin, was corrected to a mean of 6.8° (SD ±2.0°; range 0°-12°), P < 0.0001. No relevant complications were noted and no recurrent ACL graft failure was reported within the full follow-up period. Twenty-one patients had not received a revision ACLR after ACW-HTO at final follow-up due to sufficient stability. Prior to the first ACL injury, the mean Tegner activity scale was 7.3 points (SD ±1.7; 3-10) and mean Lysholm score revealed 98 points (SD ±4; range 79-100). Prior to ACW-HTO Tegner Scale was significantly reduced to 3.3 points (SD ±1.8; range 0-9) (P < 0.0001) and Lysholm score revealed 57 points (SD ±28; range 14-94) (P < 0.0001) as compared with the pre-injury level. At final follow-up, mean Tegner activity scale changed to 4.8 points (SD ±1.9; range 0-9), which significantly improved as compared with the pre-osteotomy stage (P < 0.0001). Of 85 patients, 18 achieved their pre-injury Tegner activity level, 2 even reached a level higher than the preoperative level. So the return to pre-injury activity level is 21%. The Lysholm score significantly improved to 83 points. (SD ±18; range 24-100) (P < 0.0001) as compared with the pre-osteotomy stage.
Conclusion
The present case series presents the largest published series after ACW-HTO and secondary ACLR. Clinical and radiographic results underline that this procedure is safe and significantly increases the patient’s ability to participate in light sports and activities of daily living due to an improved stability. An important fact is that 21% of patients after ACW-HTO have not needed a revision ACLR due to an improvement of stability after the osteotomy.
Keywords
Introduction
Corrective osteotomies of the proximal tibia in the sagittal plane played a subordinate role in knee surgery for many decades. Indications were mostly seen in cases presenting a genu recurvatum1 -4 or a fixed flexion deformity of the knee joint. The view changed abruptly as clinical studies presented by the Pinczewski group in 2013 and 2018,5,6 which showed that there is an increased risk of anterior cruciate ligament (ACL) graft failure if the posterior tibial slope (PTS) exceeds 12°. They further showed that in a population of young and active patients only 22% of initial ACL reconstruction (ACLR) survived at 20 years if the PTS exceeds 12°. 5
Earlier, clinical studies showed already an increased rate of ACL injuries in the presence of a steep PTS.7 -10 Furthermore, especially in the situation of multiple revision ACLR, it was found that the risk for further ACL injury exhibited 11.6-fold if the PTS exceeds 12°. 11 These findings led some authors to suggest a deflexion osteotomy to overcome this problem in the revision situation.12,13
Due to the strong impact of an elevated PTS, more and more case series about anterior-closed-wedge high tibial osteotomies (ACW-HTO) are available today.14 -18 However, larger case series with focus on postoperative activity and patient satisfaction are missing. Thus, the goal of the present study is to evaluate the clinical outcome of a larger cohort of ACW-HTO with respect to patient satisfaction, complications, early re-rupture rate, and the amount of slope reduction in a 2-center series. More specifically, it was hypothesized that a staged ACW-HTO with secondary revision ACLR improves knee function, as determined by the Tegner activity scale and Lysholm score, compared with the pre-osteotomy stage. Further on it was suggested that ACW-HTO gives sufficient stability in some cases even without a revision ACLR.
Methods
Data Collection
All patients who underwent ACW-HTO between 2019 and 2022 in 1 of the 2 centers (51 cases Sozialstiftung Bamberg and 34 cases Sporthopaedicum Berlin, Germany) were recorded. After ACW-HTO, most patients underwent implant removal and revision ACLR. In 2 cases, ACW-HTO and ACR revision reconstruction were done single-staged. Two years after ACW-HTO was defined as an endpoint for the present evaluation.
Inclusion criteria were as follows:
Completed preoperative knee function questionnaire;
Completed postoperative knee function questionnaire;
Available preoperative and postoperative radiographs for radiological evaluation even if final questionnaire is not available.
Exclusion criteria were as follows:
Additional correction in the coronal plane;
Post-traumatic corrections;
Additional major ligament injuries such as posterolateral corner or posterior cruciate ligament involvement;
Missing final questionnaire.
Demographic data such as age at ACW-HTO, gender, affected side, and number of previous ACLRs were recorded. The Tegner activity scale 19 and the Lysholm score 20 were selected as patient-reported outcome measures (PROMs), as the reliability of the scores in ACL insufficiency has been proven also in the German version.21,22 Both were assessed at 3 time points:
Prior to first ACL injury (retrospective history: best state ever).
Prior to ACW-HTO.
Two years after the osteotomy.
Range of motion was measured in increments of 5° using a conventional goniometer. Types of additional ligament stabilizations, such as an anterolateral tenodesis at final ACLR, were recorded.
Statistical analysis
The data are presented as mean values (standard deviation [SD] and range); a data plot was used to test whether the data was parametric or nonparametric. Statistical analysis was conducted using the Wilcoxon test and Spearman correlation in the PSPP software (GNU operating system).
Radiographic assessment
In all cases presenting an ACL injury, long lateral radiographs are taken in the participating centers. Poor quality images were excluded or repeated. Exclusion criteria were a short tibial shaft (less then 15 cm), femoral condyle overlapping >5 mm, and a poor differentiation between medial and lateral tibial plateau. The PTS was measured as the angle between the proximal anatomical axis and medial tibial plateau according to the technique of Dejour and Bonnin
23
(

Long lateral image of the knee joint, the slope is measured using the Dejour method (14°) (left). Planning of the anterior closed-wedge osteotomy (right), a correction angle of 8° would lead to a postoperative slope of 6°.
Indication and Surgical Procedure
The indications for the use of an ACW-HTO include the following:
Number of previous ACLR (none vs one vs multiple);
Degree of PTS (≥12°);
Grade of anterior laxity;
No severe additional malalignment in the coronal plane;
Grade of degeneration (osteoarthritis, cartilage damage, meniscus loss);
Involvement of peripheral structures.
Two different surgical procedures were used, an infratuberosity osteotomy (ITO) as described by Hees and Petersen
24
and a supratuberosity approach (STO) as described elsewhere.4,13,15 In both techniques, the hinge point is located close to the insertion site of the posterior cruciate ligament (

Positioning of 2 K-wires (left), the hinge point is in the area of the posterior cruciate ligament insertion site as shown on the fluoroscopy. The angle is measured as previously calculated in the planning (right).

Postoperative state after internal fixation in the lateral view
After surgery, full weightbearing was restricted for 4 to 6 weeks with no limited range of motion. After sufficient bone healing, monitored by conventional x-rays and/or computed tomography, patients were scheduled for implant removal and final ACLR and, if needed, for an additional LET (lateral extra-articular tenodesis).
No funding was received for this publication. The ethics committee of the Friedrich Alexander University Erlangen approved this study (Approval RIB Number 24-455-B) and every patient gave informed consent.
Results
Demographic Data
One hundred consecutive cases with an ACW-HTO operated between February 2019 and December 2022 were included in 2 surgical centers (51 cases Sozialstiftung Bamberg and 35 cases Sporthopaedicum Berlin, Germany). Demographic data are given in
Demographic Data for the Included Cases.

Note. No significant difference in gender distribution or side distribution appeared (P < 0.0001)
For the sample size calculation, the 85 patients included in the follow-up are taken as the population. This results in a number of at least 70 patients needed to have a confidence level of 95% that the real value is within ±5% of the measured value.
No cases had to be excluded because of poor imaging quality of the radiographs.
Indication for Slope Surgery
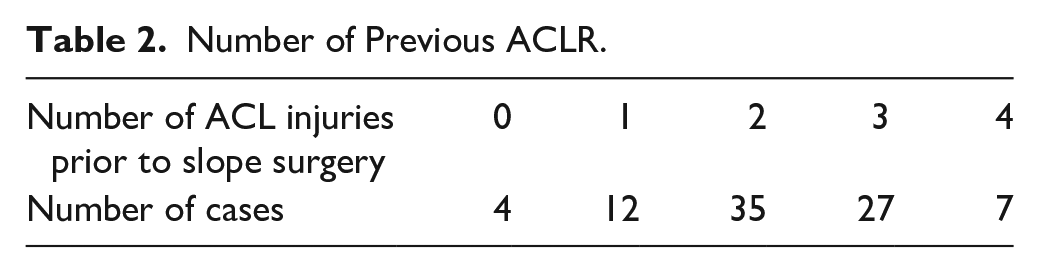
In 81 cases, an ACL graft insufficiency combined with an outlier TS was the primary indication to perform the osteotomy. The remaining 4 cases which underwent ACW-HTO presented ACL insufficiency due to mucoid degeneration of the ACL or ACL insufficiency combined with a fixed flexion contracture (
Number of Previous ACLR.
Slope Values
The mean PTS measured 14.6° (SD ±2.4°; range 11°-28°) and was significantly reduced to 6.8° (SD ±2.0°; range 0°-12°) (P < 0.001) (see
Slope Values.


Boxplot for preoperative and postoperative slope values (P < 0.0001).
Subsequent surgeries
At follow-up, 78 cases had already undergone implant removal, 7 had not. At that time, 64 cases had already undergone cruciate ligament revision reconstruction, 21 cases had not. The revision ACLR was performed on average 9 (3-25) months after the osteotomy. In 10 of these remaining cases, patients refused further ACLR due to an improved stability. In 8 cases, the cruciate ligament was in continuity in the arthroscopy before ACW-HTO and was not replaced (4 times primary ACL, 4 times after revision). In 2 cases, the patients were not satisfied with the course of treatment and refused further revision ACLR. In only 1 case, the revision ACLR surgery could not be performed due to personal time constraints of the patient.
In 33 of those patients who had undergone revision ACLR, an additional anterolateral tenodesis was performed; 31 cases did not undergo additional stabilization (see

Flowchart on follow-up procedures after ACW-HTO (ACLR = ACL revision reconstruction).
Complications
There were no cases of delayed bone healing, postoperative hematoma, vessel or nerve injury, infection, or deep vein thrombosis seen in this cohort during their postoperative follow-up.
PROMs
Lysholm score was as shown in
Lysholm Score and Tegner Score Results (Pre-injury Score, Pre-osteotomy Score and Postoperative Follow-up Score 2 Years After Surgery).


Boxplot of Lysholm score data.
The minimum clinically important difference (MCID) was determined using a determination-based method25,26 to evaluate whether the statistical significant difference also means a clinical improvement. After the following procedure was reported to be reliable, 27 we used the 0.5 SD of the observed change in PROMs as an approximate value for the MCID.
The observed improvement of the Lysholm score from prior to the osteotomy to after the osteotomy was 28 points (SD ±21; range −37 to 85). Therefore, the MCID for the Lysholm score was 10.5 points which means a clear clinical improvement.
On the Tegner activity scale, at the pre-injury level was 7.3 points (SD ±1.7; 3-10) (

Boxplot of the Tegner activity scale data.
However, postoperative activity remained 2.5 points lower on average compared with the best function as recalled by the patient prior to their injury. There was a statistically significant difference between pre-injury and the postoperative values (P < 0.0001). Furthermore, there was statistical significance between the pre-osteotomy and the post-osteotomy stated (P < 0.0001) and the MCID calculation also showed a clear clinical improvement.
Of 85 patients, 18 achieved their pre-injury Tegner activity level, 2 even reached a level higher than the preoperative level. So the return to pre-injury activity level is 21%.
In the more detailed analysis of the PROMs, it was investigated whether there was a difference between the patients with isolated ACW-HTO and the group with ACW-HTO and revision ACLR. In group 1, the Lysholm score was 59 before osteotomy, and 84 at the follow-up time, an improvement of 25 points. In group 2, Lysholm was 54 before osteotomy, 81 at the follow-up time, a difference of 27 points. There is therefore no significant difference (P < 0.0001) due to the additional treatment with revision ACLR.
There was also no significant difference (P < 0.0001) in the Tegner score (ACW-HTO plus revision ACLR before osteotomy 3.4, at follow-up 5.0, difference 1.6 points. ACW-HTO without revision ACLR 3.0 before osteotomy, 4.4 at the time of follow-up, difference 1.4 points).
It was also investigated whether the PROMs in patients with ACW-HTO and revision ACLR differed depending on whether or not a LET was performed. Interestingly, there was no difference at all here: the patient with LET changed from 54 to 80 points in the Lysholm score (difference 26 points), without LET from 62 to 88 points (difference also 26 points). The change in the Tegner score with LET was from 2.8 to 4.4 points (difference 1.6) and without LET from 3.8 to 5.4 points (difference also 1.6 points). So the LET did not lead to any change in the PROMs. But this was not randomly assigned; it was only an observation and indication to LET was a subjective case-based decision.
Ninety-one percent of the cases answered “yes” to the question if they would undergo the surgery again.
The range of motion was documented in 57 of 85 patients preoperatively and in 48 of 85 patients postoperatively. It changed only minimally, on average from preoperatively 1° - 2° - 130° to postoperatively 2° - 0° - 129°. The changes were not significant. No case showed relevant restrictions of movement or relevant hyperextension.
No re-rupture of the revision ACLR was reported within the follow-up period.
Discussion
The goal of the present investigation was to study if an ACW-HTO improves the activity level and the subjective satisfaction in cases with failed ACLR in the presence of an outlier PTS. The present investigation clearly demonstrates that there is a significant improvement in Lysholm score and Tegner activity scale after surgery as compared with the pre-osteotomy stage.
It was shown that the patients had a very high activity level before the first ACL injury (average Tegner score 7.3) and showed a significantly lower activity level (Tegner score 3.3) directly before the ACW-HTO. More importantly, however, it was shown that ACW-HTO significantly increased the activity level again (Tegner score 4.8), an activity level between leisure and competitive sport, even if the initial level could not be completely reached.
The minimal change in extension postoperatively after ACW-HTO is also important information. Many publications warn that extension osteotomy is associated with a high degree of hyperextensibility of the knee joint. However, this has not yet been substantiated with high case numbers. In this group, it can now be shown for the first time that the change in bony geometry is not reflected one-to-one in postoperative mobility.
Furthermore, it was shown that not a single re-rupture of the revision ACL was seen.
This finding is in line with previous reports14,28 -31
Mabrouk et al. 17 reported on 64 cases in a 2-year follow-up. All patients received revision ACLR and ACW-HTO. Three cases of ACL re-rupture were reported, and one-third of all patients showed an nonsymptomtic genu recurvatum. About half of all patients could return to impact sports.
Thus, we can conclude that an ACW-HTO in the presence of an outlier TS improves functional outcome. However, the pre-injury level could not be reached after the ACW-HTO with or without a secondary revision ACLR. This might be attributable to the fact that in most cases presented here, a long history with multiple previous surgeries is present. It is apparent that these multiple surgeries combined with multiple injuries create a certain field damage to the knee joint current surgical techniques seem unable to fully address.
Declined revision ACLR, when offered, shows the ACW-HTO had improved their functional stability sufficiently. However, it should be taken into consideration that a certain fatigue after a long history of injuries and surgeries might explain a willingness to accept lower functional outcome and a lower level of satisfaction rather than face the prospect of further ACW-HTO surgery.
At this point, it needs to be discussed that an additional osteotomy within a long history of disease adds further field damage to the knee joint and prolongs the treatment time if performed staged. In this connection, it is to consider that 2 different points of view exist on the usage of an ACW-HTO as a treatment option. On one hand, one might consider that the osteotomy offers a protective tool against further ACL graft failure. 28 On the other hand, an ACW-HTO offers just a salvage procedure to cope with multiple ACL graft failures in the presence of an outlier slope. 32 This essential question, however, cannot be answered with the findings of the present report.
A major point of the current dispute is the degree of the PTS as an indicator to add an ACW-HTO in the primary situation, after the first graft failure, or in cases with multiple graft failures.
There is no doubt that a PTS exceeding 12° presents a hazard for ACL injury or ACL graft failure.33 -35 But could this value be used as a strict threshold to indicate an osteotomy?
Song et al. 16 published the only case series so far combining a primary ACLR with a slope reduction osteotomy. They included 18 patients with a steep slope (mean 18.5° [17°-20°]) and an anterior tibial translation (ATT) of more than 10 mm. All clinical scores showed a significant improvement at final follow-up, with significant reduction of the ATT and no re-rupture reported.
In a recent investigation, researchers found that up to 20% of non-ACL-injured patients presents a PTS equal or greater than 12°. 36 The difference between ACL-injured and noninjured cases got more prominent with an increasing TS. Duerr et al. 37 described an 18.7-fold increased risk of an additional ACL graft failure in the situation of revision ACLR if the PTS exceeds 14°. Gwinner et al. 11 reported in a larger series of revision ACLR a mean slope of only 9.8° in cases presenting a single graft failure. But in cases with multiple graft failures, the mean TS exceeded 12°, indicating that a slope of 12° does not necessarily needs correction of the PTS in the situation of first ACL graft failures. A moderately increased TS, such as 12°, could be used as an additional indicator for an ACW-HTO in combination of other factors, such as the degree of anterior laxity, age, and level of activity.
In relation to the current research, if is obvious that an outlier slope such as 12° is hazardous for a native ACL and a reconstructed ACL. However, on the other hand around, we still do not know whether an outlier TS necessarily leads to an ACL injury. In the study of Weiler et al. 36 on PTS mean values and outliers, 5.8% of non-ACL-injured cases present a slope equal or greater than 14°.
At this point, there are to discuss certain flaws of the present investigation.
First, it was not possible to follow all patients, but an Follow up rate of 85% is generally deemed acceptable. Second, at follow-up, only 64 cases underwent final implant removal and revision ACLR but were analyzed within the group of cases without (N = 21) final revision ACLR due to various reasons as mentioned above. If one takes into consideration that a revision ACLR might further improve final outcome, the subjective outcome data are not positively influenced by this flaw. Third, most cases were collected prospectively, but some were also collected retrospectively, which can play an important role of bias. So both groups were analyzed and no statistical difference in the PROMs between them was found. Next, we need to consider that there is a certain change of knowledge and a changed view on this new topic within the orthopedic community over the last few years. Thus, the follow-up time of up to 82 months does not reflect the current scientific stage, especially with respect to indication, surgical technique, target slope, and so on. One other point is that stability of the ACL and graft failure rates were not systematically evaluated and presented data on failures only are based on reported issues. Further on it is a heterogenic cohort with very different conditions (meniscus status, number of previous ACL procedures, etc.) and there is not a control group of re-revision ACLR to compare return to sport rates or any other data.
Conclusion
Over the last decade, the negative impact of a steep PTS on ACL injury and failure rates after ACLR has been well documented. Hereby, the use of a slope reducing osteotomy seems to be a promising tool to overcome these problems. This investigation was able to show that an ACW-HTO improves outcome in this specific cohort of patients, presenting an outlier PTS and ACL insufficiency, often combined with multiple previous surgeries. The level of sporting activities and activities of daily life can be significantly improved compared with presurgery level. However, in the majority patients, studied here, the pre-injury activity level could not be reached.
Footnotes
Ethical Considerations
An approval from the ethical board of the Friedrich Alexander University Erlangen was given at December 3, 2024. All patients gave their informal consent to be part of the study verbal or in written consent.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.