
Abstract
Objective:
The goals of this study are to address several questions, the answers to which are key to the understanding and eventually to the prevention of this frequent source of morbidity. These questions include the following: (1) What is the natural history of anterior cruciate ligament (ACL) deficiency? (2) How important is the status of the meniscus at the time of reconstruction? (3) Does ACL reconstruction prevent the development of osteoarthritis in the long term? (4) Can we predict which patients will develop osteoarthritis? (5) What can be done?
Design:
This study addresses the key questions above through the long-term follow-up of a cohort of patients treated with ACL reconstruction by Professor Henri Dejour in Lyon, France, supplemented with a review of the relevant literature.
Results:
The prevalence of osteoarthritis in ACL-deficient knees is about 40% after 15 years and close to 90% after 25 to 35 years. It remains unclear whether reconstruction of the ACL significantly reduces this risk. The status of the meniscus at the time of ACL reconstruction is a strong predictor of the risk of osteoarthritis: Patients who undergo total meniscectomy are at 2- to 10-fold increased risk of developing osteoarthritis relative to those with intact menisci. Patients showing early evidence of arthritis at short- to medium-term follow-up are at high risk for progression over subsequent years. Numerous emerging techniques may provide tools to more effectively prevent and treat osteoarthritis following ACL injury in the future.
Conclusion:
Osteoarthritis following ACL injury continues to be a major problem requiring further research.
Introduction
Injury to the anterior cruciate ligament (ACL) frequently results in symptomatic knee instability that significantly limits knee function. Modern surgical and rehabilitation techniques are often able to restore knee stability and allow return to high function; however, a major long-term concern remains the high risk of subsequent development of premature osteoarthritis in this young, active patient population. 1
The goals of this study are to address several questions, the answers to which are key to the understanding and eventually to the prevention of this frequent source of morbidity. These questions include the following: (1) What is the natural history of ACL deficiency? (2) How important is the status of the meniscus at the time of reconstruction? (3) Does ACL reconstruction prevent the development of osteoarthritis in the long term? (4) Can we predict which patients will develop osteoarthritis? (5) What can be done?
Methods
This study addresses the key questions above through the long-term follow-up of a cohort of patients treated with ACL reconstruction by Professor Henri Dejour in Lyon, France, 2 supplemented with a thorough review of the relevant literature.
The case series consists of a consecutive series of 410 patients treated by Professor Dejour for chronic ALC deficiency between 1978 and 1983. These patients have been followed up at various time points over the years and the data presented here include outcomes of 100 of the original 410 patients (24.4%) at 11 years, 3 17 years, 4 and 23 years 2 postoperation. The ACL reconstructions were performed using an intra-articular bone-patellar tendon-bone technique modified from that described by Clancy et al. 5 supplemented by an extra-articular reconstruction modified from the method of Lemaire. 6
Literature review was then undertaken to identify other studies of ACL deficient and reconstructed knees with long-term follow-up to supplement the data from the Lyon series. Of specific interest were series reporting outcomes based on meniscus status at the time of ACL reconstruction as well as series comparing operative and nonoperative treatment of ACL injuries.
Results
What Is the Natural History of ACL Deficiency?
Review of the literature identified several medium- and long-term studies that demonstrate high rates of osteoarthritis in chronically ACL-deficient knee. At 15 years of follow-up, the prevalence of osteoarthritis is this population has been reported to be about 40% in several series.7,8 Longer term follow-up demonstrates the prevalence of osteoarthritis to increase to near 90% by 25 to 35 years, with up to 50% of patients undergoing total knee arthroplasty in some series.9,10
Interestingly, meniscal status does not appear to be the major predictor of long-term outcome in this population. A similar proportion of patients with a normal meniscus8,9 and a subtotal meniscectomy at the time of ACL injury7,10 developed osteoarthritis. The influence of meniscal loss on the time course of osteoarthritis development as well as symptoms and activity level in these populations remains unclear.
How Important Is the Status of the Meniscus at the Time of Reconstruction?
In contrast, meniscus status appears to be a very strong predictor of subsequent development of osteoarthritis in patients who undergo ACL reconstruction. Review of the literature reveals numerous comparative studies with 4- to 12-year follow-up comparing prevalence of osteoarthritis in ACL-reconstructed patients who underwent partial meniscectomy with normal menisci versus those with normal menisci. These studies demonstrate 2- to 10-fold increased risk of osteoarthritis following partial meniscectomy ( Table 1 ).11-16 A recent systematic review that included only prospective studies with minimum 5-year follow-up demonstrated similar findings. 17
Radiographic Signs of Osteoarthritis in Patients with Normal Menisci and Those with Partial Meniscectomy at Surgery.
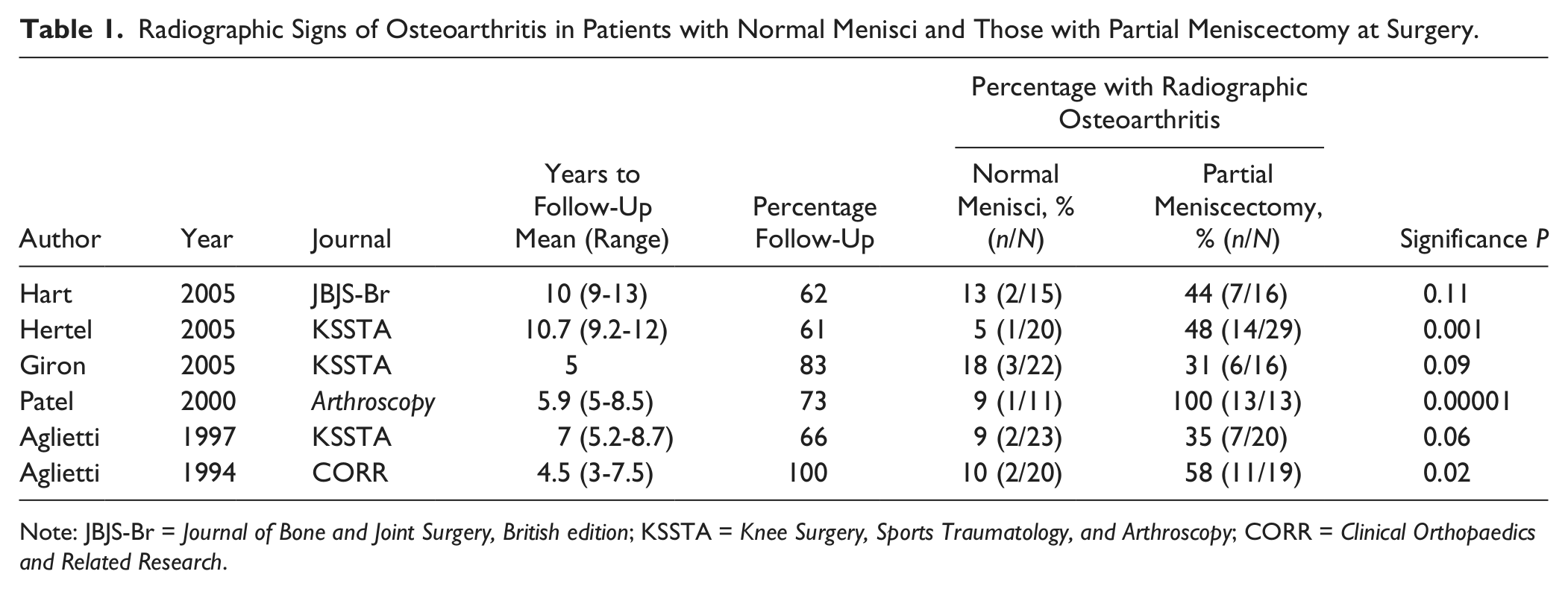
Note: JBJS-Br = Journal of Bone and Joint Surgery, British edition; KSSTA = Knee Surgery, Sports Traumatology, and Arthroscopy; CORR = Clinical Orthopaedics and Related Research.
At longer term follow-up, the series of patients reconstructed by Professor Dejour in Lyon demonstrates similar findings at 24.5 years’ follow-up. 2 Patients were twice as likely to develop IKDC (International Knee Documentation Committee) grade C or D osteoarthritis if they underwent partial meniscectomy at the time of ACL reconstruction. Articular cartilage lesions noted at the time of ACL reconstruction also appear to be significant predictors of future development of osteoarthritis. In this same series, the presence of medial compartment cartilage defects at reconstruction was associated with a 5-fold increased risk of osteoarthritis at final follow-up.
Does ACL Reconstruction Prevent the Development of Osteoarthritis in the Long Term?
Perhaps the most important question regarding the long-term outcomes of ACL injury is whether ACL reconstruction alters the natural history in regards to the development of osteoarthritis. Several comparative studies have attempted to answer this question with 11- to 20-year follow-up after ACL injury ( Table 2 ). Mihelic et al. 18 compared the prevalence of osteoarthritis in an ACL-reconstructed group and ACL-deficient group 17 to 20 years after ACL injury. They noted significantly less IKDC grade C or D osteoarthritis in the reconstructed group (28%) relative to the ACL-deficient group (67%). In a similar study, Streich et al. 19 looked at the prevalence of osteoarthritis at 15 years post-ACL injury and noted equal osteoarthritis prevalence (38%) in both reconstructed and ACL-deficient groups. Further confusing matters, a study by Kessler et al. 20 actually noted a higher prevalence of osteoarthritis (45%) in the reconstructed group than in the ACL deficient group (28%) 11 years after ACL injury. Clearly, more research is necessary to clarify these findings.
Radiographic Signs of Osteoarthritis in Patients Treated with ACL Reconstruction versus Nonoperative Management.
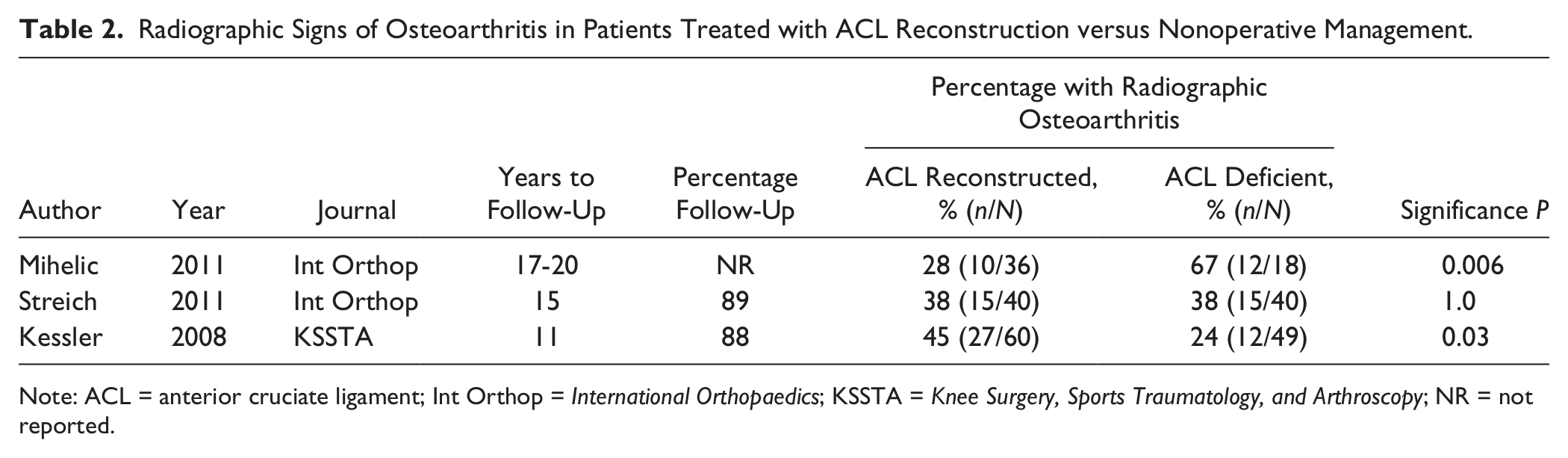
Note: ACL = anterior cruciate ligament; Int Orthop = International Orthopaedics; KSSTA = Knee Surgery, Sports Traumatology, and Arthroscopy; NR = not reported.
Unfortunately, longer term comparative studies evaluating osteoarthritis risk in similar ACL-injured populations treated with or without ACL reconstruction are nonexistent. One must therefore resort to comparing the results of case series of patients treated with and without surgery. Using this method, in case series of patients with normal menisci at the time of surgery, the prevalence of osteoarthritis appears to be higher 14 to 35 years later in patients who did not undergo ACL reconstruction (40% to 90%)8,9 relative to those who did undergo reconstruction in the Lyon series (35%). 2 Similar results are found when comparing case series of patients with abnormal menisci at the time of reconstruction. These case series demonstrate that patients treated nonoperatively exhibit a higher prevalence of osteoarthritis at 35 years postinjury (90%) 10 than those who underwent ACL reconstruction in both the Lyon data (42%) 2 as well as a study by Yamaguchi et al. 21 (50%). One must remember that such comparisons are subject to numerous sources of bias and represent low-level evidence. Clearly, comparative studies on this subject would be preferred.
Can We Predict Which Patients Will Develop Osteoarthritis?
Following ACL reconstruction, it would be ideal to be able to predict which patients are at highest risk for subsequent osteoarthritis development and then intervene in some way to minimize this risk. As noted above, the presence of additional intra-articular pathology (meniscal or articular cartilage injury) at the time of surgery does appear to increase the risk of subsequent development of osteoarthritis. The impact of other patient factors such as body mass index or activity level on this risk remains unclear. 17
Although our ability to predict at the time of injury or surgery which patients will develop osteoarthritis is limited, short- and medium-term follow-up data provide insight into a patient’s long-term prognosis. Data from the Lyon series indicate that patients with no evidence of degenerative change on plain films 11 years after surgery are at very low risk to develop osteoarthritis over the next 15 years.2,3 Similarly, if early evidence of degenerative change is visible on radiographs 11 years following surgery, the risk of significant progression of osteoarthritis over the next 15 years is quite high. While having this information at the time of reconstruction would be more useful, information on the patient’s status 10 years after surgery can be quite useful and informative to patients moving forward.
Discussion
What Can Be Done?
Strategies to reduce osteoarthritis risk begin at the time of the initial ACL reconstruction. Meniscal repair and preservation has been shown in several comparative studies to reduce subsequent risk of osteoarthritis at 4 to 7 years postoperative compared with partial meniscectomy.11,12,22,23 Operating earlier on ACL-deficient knees and preventing the occurrence of some medial meniscal tears that can develop with persistent instability nay also potentially maximize meniscus tissue.24-27
In spite of efforts to preserve meniscal tissue, subtotal meniscectomy is sometimes unavoidable. In these cases, one can consider other techniques to mitigate poor results. Meniscal allograft has long been felt to offer advantages in such patients, particularly in younger patients without significant degenerative disease. 28 Newer meniscal scaffold techniques can be used to address segmental meniscal defects or loss of the entire meniscus. 29 The goals of both procedures are to address both the abnormal joint loading and loss of stability associated with meniscal loss.
Similarly, when evidence of early degenerative change is noted at the time of ACL reconstruction, one can consider early intervention through either activity modification (limiting high-impact activities) or altering joint loading forces through concurrent high tibial osteotomy. Data regarding the results of ACL reconstruction in association with high tibial osteotomy are limited to case series. Several studies have demonstrated maintenance of pain relief and continued control of anterior tibial translation at 2- to 5-year follow-up.30-32 One case series with 12-year follow-up demonstrated progression of osteoarthritis by at least one grade in only 17% of the knees. 33
There is also great potential exhibited by new techniques that may aid in meniscal preservation, cartilage restoration, and joint protection. These include new meniscal scaffold technologies, 34 biologic agents that may prevent inflammatory processes leading to cartilage death, 35 and cartilage restoration and biologic joint resurfacing techniques. 36 Further research and longer follow-up are necessary to accurately evaluate the potential of such techniques.
Conclusions
The long-term risk of osteoarthritis in ACL-deficient knees is high. It remains unclear whether reconstruction of the ACL significantly reduces this risk. The status of the meniscus at the time of ACL reconstruction is a strong predictor of the risk of osteoarthritis. Patients showing early evidence of arthritis a short- to medium-term follow-up are at high risk for progression over subsequent years. Numerous emerging techniques may provide tools to more effectively prevent and treat osteoarthritis following ACL injury in the future.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study does not require institutional review board approval.