
Abstract
Anatomic anterior cruciate ligament (ACL) reconstruction is common procedure performed by orthopedic surgeons, particularly in association with sports-related injuries. Whereas traditional reconstruction techniques used a single bundle graft that was typically placed in a non-anatomic position, a renewed interest in anatomy has facilitated the popularization of anatomic reconstruction techniques. Recently, a focus has been placed on individualizing ACL surgery based on each patient’s native anatomical characteristics (e.g., insertion site size, notch size, and shape), thereby dictating the ultimate procedure of choice. As subjective outcome measurements have demonstrated varying outcomes with respect to single- versus double-bundle ACL reconstruction, investigators have turned to more objective techniques, such as in vivo kinematics, as a means of evaluating joint motion and cartilage contact mechanics. Further investigation in this area may yield important information with regard to the potential progression to osteoarthritis after ACL reconstruction, including factors affecting or preventing it.
Introduction
Anterior cruciate ligament (ACL) reconstruction is an operation performed frequently by orthopedic surgeons throughout the world. In fact, it is estimated that more than 200,000 ACL reconstructions are performed each year in the United States alone. 1 Traditionally, the single-bundle reconstruction technique has been the treatment method of choice in ACL surgery. However, traditional reconstruction techniques often failed to place the graft in an anatomic position. 2 Although these conventional reconstruction methods appear to, at least in the short term, improve knee stability, more recent studies have demonstrated continued symptoms of instability and a low rate of return to pre-injury sporting levels at long-term follow-up.3,4 Furthermore, alterations in knee joint kinematics following these conventional procedures potentially place the knee at an increased risk for developing osteoarthritis in the long term. 5
In this regard, a large, retrospective cohort study by Li et al. 6 demonstrated a 39% radiographic incidence of knee osteoarthritis in 249 patients at a mean 7.86 years after surgery. In this cohort, length of follow-up, body mass index, grade II or greater medial chondrosis, and prior medial menisectomy were determined to be the most optimal predictors of osteoarthritis. In a separate study, Oiestad et al. 7 reported an incidence of radiographic osteoarthritis in 62% of patients with an isolated ACL tear in a 10- to 15-year prospective follow-up. However, 32% of patients reported symptomatic osteoarthritis of the knee. 7
Recently, double-bundle ACL reconstruction has been proposed as a means of restoring the 2-bundle anatomy of the native ACL. A renewed interest in the native anatomy of the ACL has facilitated a movement toward anatomic reconstruction of the ACL. Anatomic ACL reconstruction can be defined as the functional restoration of the ACL to its native dimensions, collagen orientation and insertion sites. 8
The purpose of this review article is to discuss current concepts and future perspective in anatomic ACL reconstruction, including individualized surgery and objective outcome measurement using in vivo kinematics.
Anatomy and Function of the ACL
The ACL consists of 2 functional bundles, namely the anteromedial (AM) and posterolateral (PL) bundles, each named for their respective insertion site locations on the tibia. The bundles become evident during development of the fetus and are differentiable throughout life. 9 A septum of connective tissue divides the AM and PL bundles, which provides a blood supply to the ligament and allows the bundles to work synergistically throughout motion.10,11 Functionally, the AM bundle attains peak tension between 45° and 60° of flexion but remains tight throughout the knee range of motion. By comparison, the PL bundle is tight in extension and loosens with flexion, thereby allowing rotation to occur. Thus, the AM and PL bundles facilitate both anteroposterior and rotational stability of the knee, which depends on knee flexion angle. 12
Knowledge of the anatomy of the ACL and its surrounding anatomical structures is fundamental for understanding the principles of and performing an anatomical reconstruction. In this regard, bony landmarks such as the lateral intercondylar ridge (or “resident’s ridge”) and the lateral bifurcate ridge provide an important roadmap for the anatomical placement of the femoral tunnel(s) on the lateral wall of the intercondylar notch.13-15 Specifically, the intercondylar ridge denotes the most anterior border of the native ACL insertion site, whereas the bifurcate ridge runs perpendicular and posterior to the intercondylar ridge, dividing the insertion sites for the AM and PL bundles. Bony landmarks prove particularly useful in more chronic cases where the ACL remnant may have dissolved over time. The lateral bifurcate ridge can be identified in approximately 80% of cases. 16
Single- and Double-Bundle ACL Reconstruction
To date, numerous studies have demonstrated the clinical and biomechanical benefits of both anatomic single-bundle and anatomic double-bundle ACL reconstruction.17-19 Cadaver studies and subsequent clinical studies have shown mixed results when comparing anatomic single-bundle with anatomic double-bundle ACL reconstruction techniques. Some research groups have reported superior knee stability after using the double-bundle procedure,18,20,21 whereas other studies showed little or no difference between anatomic double-bundle and anatomic single-bundle ACL reconstruction.19,22-24
A recent review in the Cochrane Database analyzing randomized and quasi-randomized controlled trials of single- versus double-bundle ACL reconstruction concluded that the available evidence was insufficient to determine whether one technique was superior to the other in adults. 25 Furthermore, although there were no statistically significant differences between techniques using subjective outcome scores, double-bundle reconstruction appeared to be superior using objective measurements of knee laxity, as well as lower rates of ACL re-rupture and further meniscal injury.
One recent prospective study by Hussein et al. 24 (level of evidence II) investigated outcomes between anatomic single- and double-bundle techniques when surgery was individualized based on the size of the patients’ native ACL. With 101 patients (32 single-bundle, 69 double-bundle) at a mean follow-up of 30 months postoperatively (range = 26-34 months), the investigators found no differences in the Lysholm score, subjective International Knee Documentation Committee (IKDC) score, KT-1000 anteroposterior laxity measurements, and pivot shift examination.
The Concept of Individualized Surgery
There is variation between individuals in the size and shape of the ACL. 26 Therefore, anatomic reconstruction of the ACL should take into account the differences between the anatomical characteristics of each patient in order to potentially restore native ligament function. In this regard, Karlsson et al. 27 suggested that the morphology of the knee and native ACL should direct the type of procedure (single-bundle or double-bundle), graft type, and tunnel size ( Figs. 1 and 2 ). Anatomic features that can be objectively evaluated preoperatively and intraoperatively include the ACL tibial and femoral insertion site size, inclination angle, and length, as well as the femoral intercondylar notch size. The following sections summarize several simple measurement techniques, providing a means by which ACL reconstruction can be evaluated quantitatively and on an individualized basis.
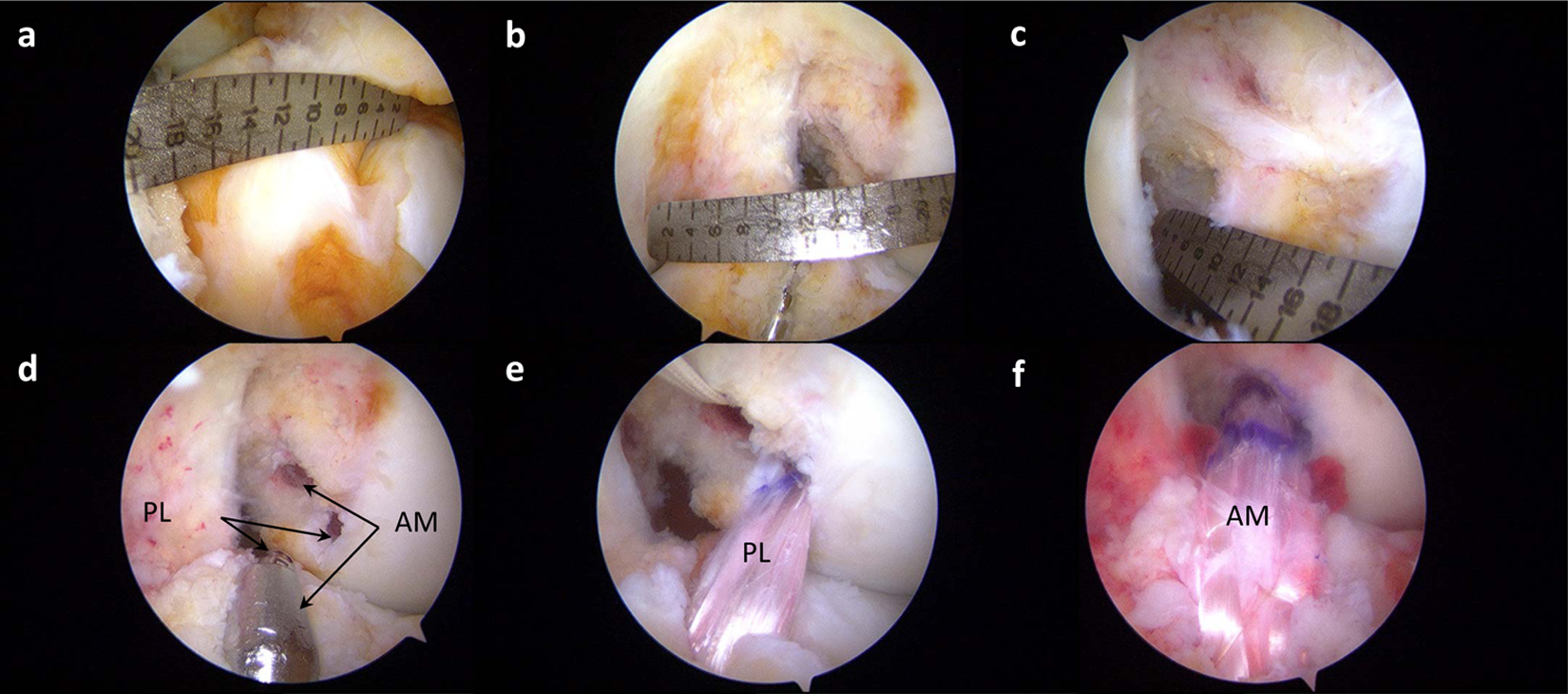
Anatomic double-bundle reconstruction with hamstring autograft in the left knee. (
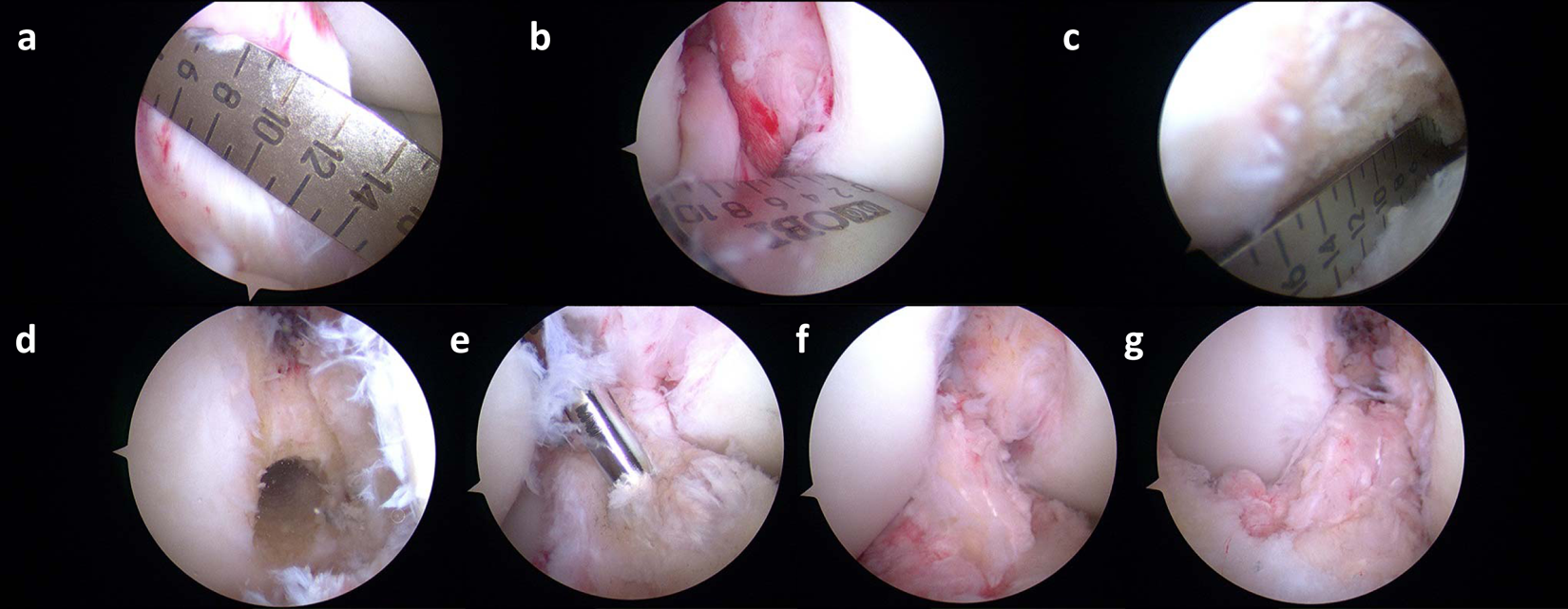
Anatomic single-bundle reconstruction with quadriceps tendon autograft in the right knee. (
ACL Insertion Site Size and Percentage Reconstructed Area
The size of the femoral and tibial insertion sites of the ACL are variable. 26 Using an arthroscopic ruler, Kopf et al. 26 measured the femoral and tibial insertion sites of 137 patients undergoing primary anatomical ACL reconstruction. The authors found that the tibial insertion site length was between 16 and 18 mm in 66.4% of patients and the femoral insertion site length was between 16 and 18 mm in 64.3% of patients. In another study measuring intraoperative insertion site size, Hussein et al. 24 determined that the femoral insertion site length ranged from 11 to 20 mm and the tibial insertion site length ranged from 9 to 20 mm.
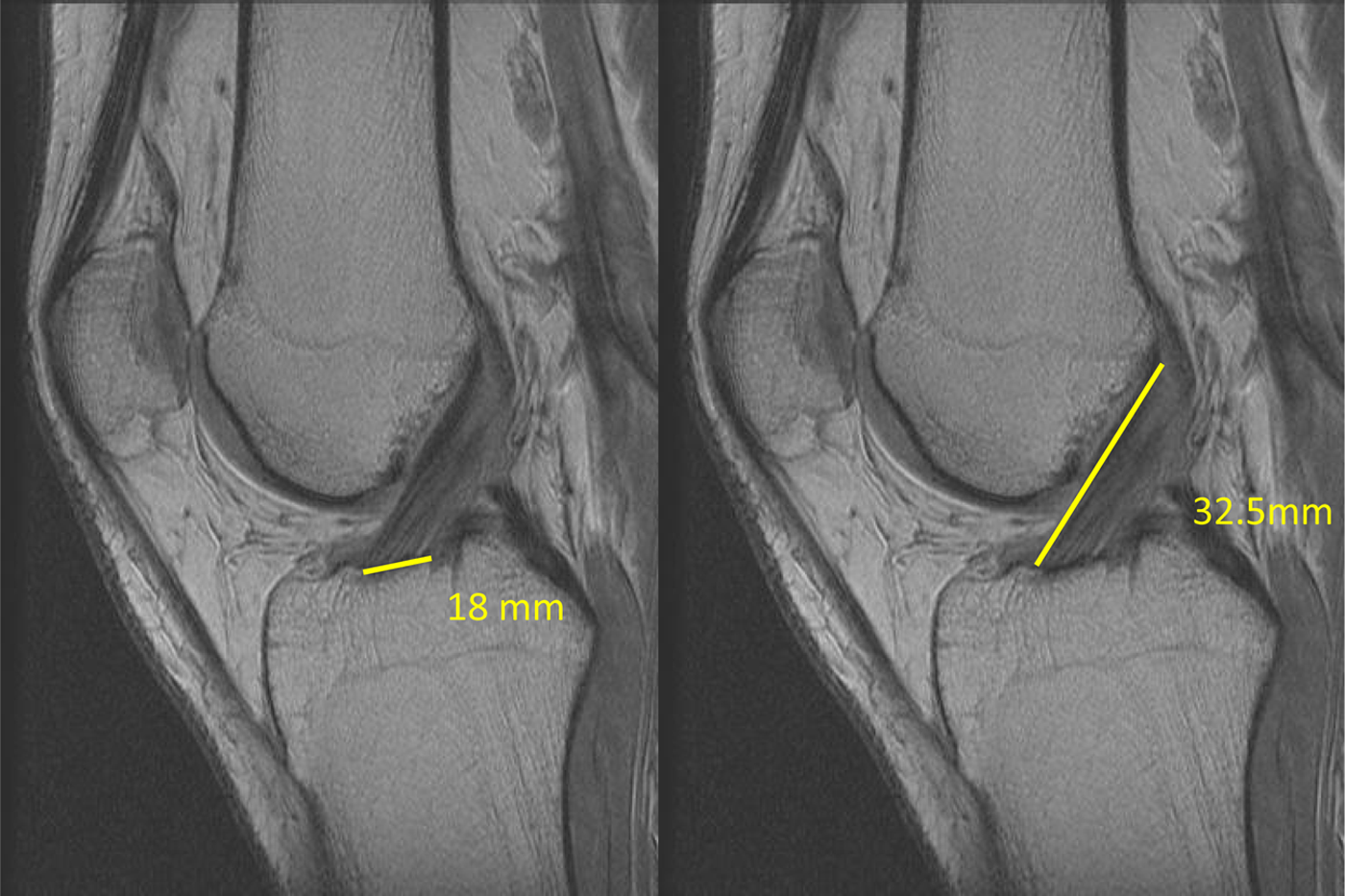
A method for preoperative measurement of the ACL tibial insertion site using MRI has been described ( Fig. 3a ). 28 Briefly, a sagittal proton density image that best demonstrates the ACL tibial insertion site is chosen, and the distance between the most anterior and posterior fibers of the ACL attachment is measured. Measuring the ACL insertion site preoperatively can provide guidance for the indication of single- or double-bundle ACL reconstruction. Tibial insertion sites 18 mm or greater may require double-bundle reconstruction, as a single graft may not adequately restore the native insertion site. In contrast, an insertion site less than 14 mm may not allow for 2 tunnels to be drilled. 8 Insertion sites between 14 and 18 mm can often be reconstructed using either a single- or a double-bundle technique; technique choice in these cases is the subject of considerable research (including an ongoing clinical trial at our institution).
Measurement of the tibial insertion site (
One goal of anatomic ACL reconstruction is to restore the native ACL insertion site as closely as possible. Siebold and Schuhmacher 29 therefore developed a “Modified Insertion Site Table” to determine the percentage of insertion site that would be restored using varying drill diameters and drill guide angles. Using this table, the authors determined that tibial insertion sites 16 mm or less would adequately be restored using a single-bundle technique, whereas insertion sites 18 mm or greater would require a double-bundle technique to sufficiently restore the ACL insertion site. The elliptical shape of the ACL insertion site, however, limits the drill diameter to the smallest dimension of the ACL. Therefore, in our institution, we aim to restore 60% and 80% of the native insertion site. By understanding and objectifying the anatomy of each patient and individualizing the surgery, a sufficient restoration of ACL insertion site may be achieved. 24
ACL Length
The length of the ACL plays an important role in choice of graft for the reconstruction. Similar to measuring the tibial insertion site on MRI, a sagittal proton density sequence best showing the ACL is chosen, and the distance between midpoint of the tibial insertion site and the femoral insertion site is measured ( Fig. 3b ). 28 Graft length within the bony tunnel has been reported to be correlated to the strength of the tendon–bone tunnel complex in animal models. 30 Therefore, preoperatively measuring the intra-articular size of the native ACL may allow for understanding the total length of graft needed to allow for adequate tunnel healing.
Femoral Intercondylar Notch
The size, shape, and orientation of the femoral intercondylar notch varies, which also should affect the indication for ACL reconstruction technique. The shape of the intercondylar notch has been described as “A,” “W,” or “U” shaped. 31 Wolters et al. 32 measured the intercondylar notch size of 82 patients undergoing ACL reconstruction and found a large range of height and width. The height of the notch ranged from 14 to 28 mm and the width at the base of the notch ranged from 10 to 21 mm. The relevance of measuring the notch size is that a smaller notch size may cause technical complications when attempting a double-bundle procedure or result in a subsequent loss of flexion/extension and potentially graft failure. This can also result from non-anatomic placement of the tibial tunnel anteriorly or the femoral tunnel superiorly and posteriorly. 33 Furthermore, a smaller notch can increase the risk of ACL re-injury.34,35
Femoral intercondylar notch size should be measured intraoperatively to determine whether a single- or double-bundle technique is warranted. To decrease the risk of possible graft failure, the surgeon must take care not to overfill the notch and place the graft anatomically. Wang et al. 36 advise that a notch size less than 12 mm in width should be an indication for use of a single-bundle ACL reconstruction technique. Based on objective intraoperative assessment of anatomy by measuring, ACL reconstruction can be customized to each individual patient.
Postoperative Assessment of Graft Tunnel Position
To postoperatively assess femoral tunnel placement, radiographs can be analyzed for femoral tunnel angle. Measurement of the femoral tunnel angle on a posterior–anterior 45° flexion weightbearing radiograph is a simple analysis of femoral tunnel placement ( Fig. 4 ). This technique for measurement has been described previously by Illingworth et al. 37 The authors reported that femoral tunnel angles of greater than 32.7° are indicative of anatomic position of the tunnel. In contrast, femoral tunnel angles of less than 32.7° may not be anatomical. Using these methods, surgeons can postoperatively assess the location of the femoral tunnels and the correlation between graft and native ACL orientation.
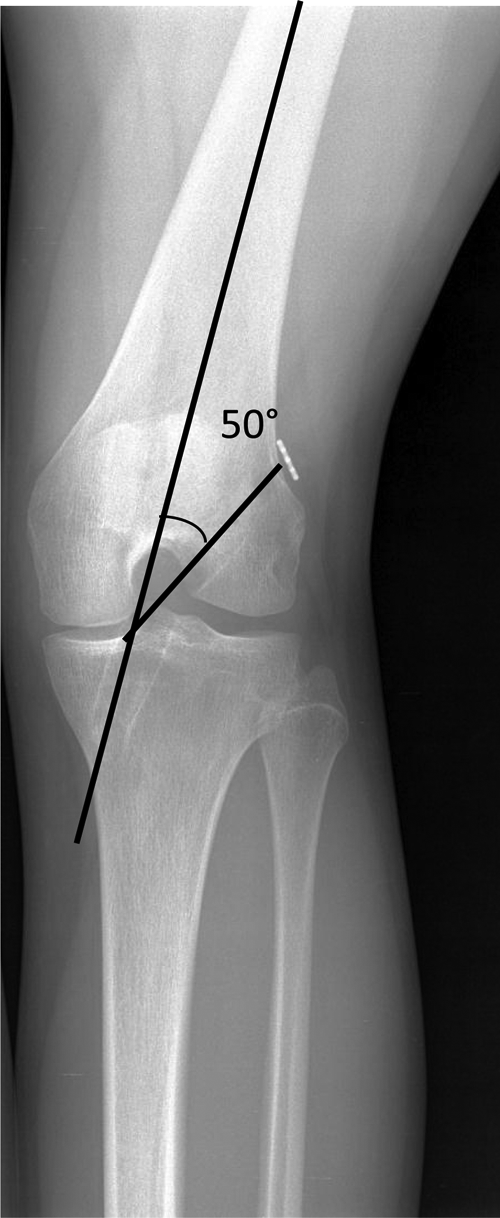
Determination of femoral tunnel angle on posterior–anterior 45° flexion weightbearing radiograph.
Furthermore, measuring the inclination angle on MRI allows for comparison of graft positioning of the reconstructed ACL with respect to the native ACL. Illingworth et al. 37 described the technique for measurement of the ACL inclination angle using MRI ( Fig. 5 ). The native, intact ACL inclination angle is between 43° and 57°. Therefore, an anatomical reconstruction of the ACL should be similar to the native ACL inclination angle.
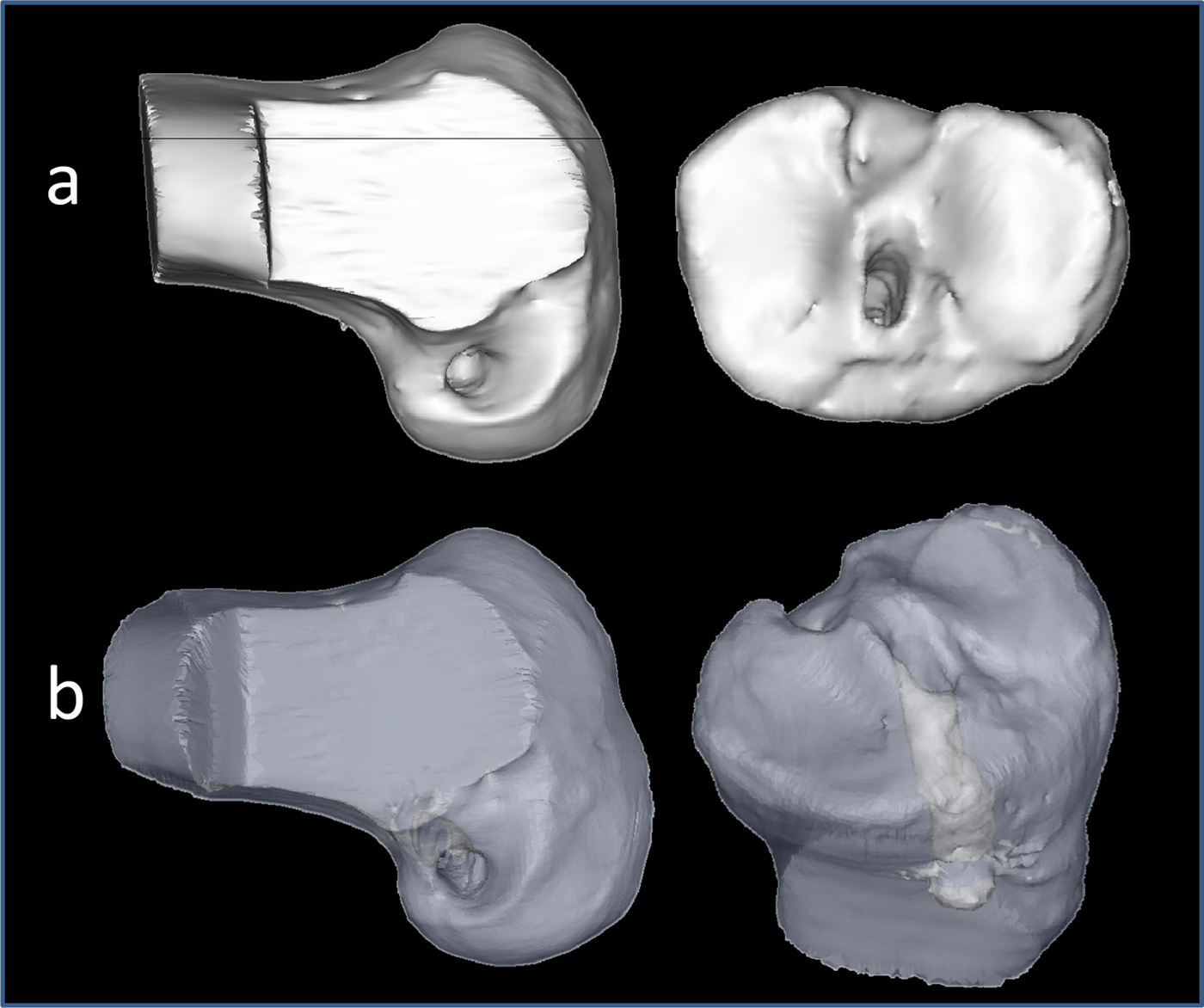
Three-dimensional computed tomography scan evaluation after anatomic single-bundle reconstruction with a quadriceps tendon autograft in the left knee. (a) Evaluation of tunnel aperture placement. (b) Evaluation of tunnel trajectory.
Three-dimensional computed tomography scan is presently recognized as the imaging method most accurate for evaluating tunnel placement on both the femur and tibia ( Figs. 6 and 7 ).38-40 Three-dimensional computed tomography scans are useful to obtain in the event that a revision procedure is required in the future, such that an evaluation of tunnel location and trajectory can be performed.
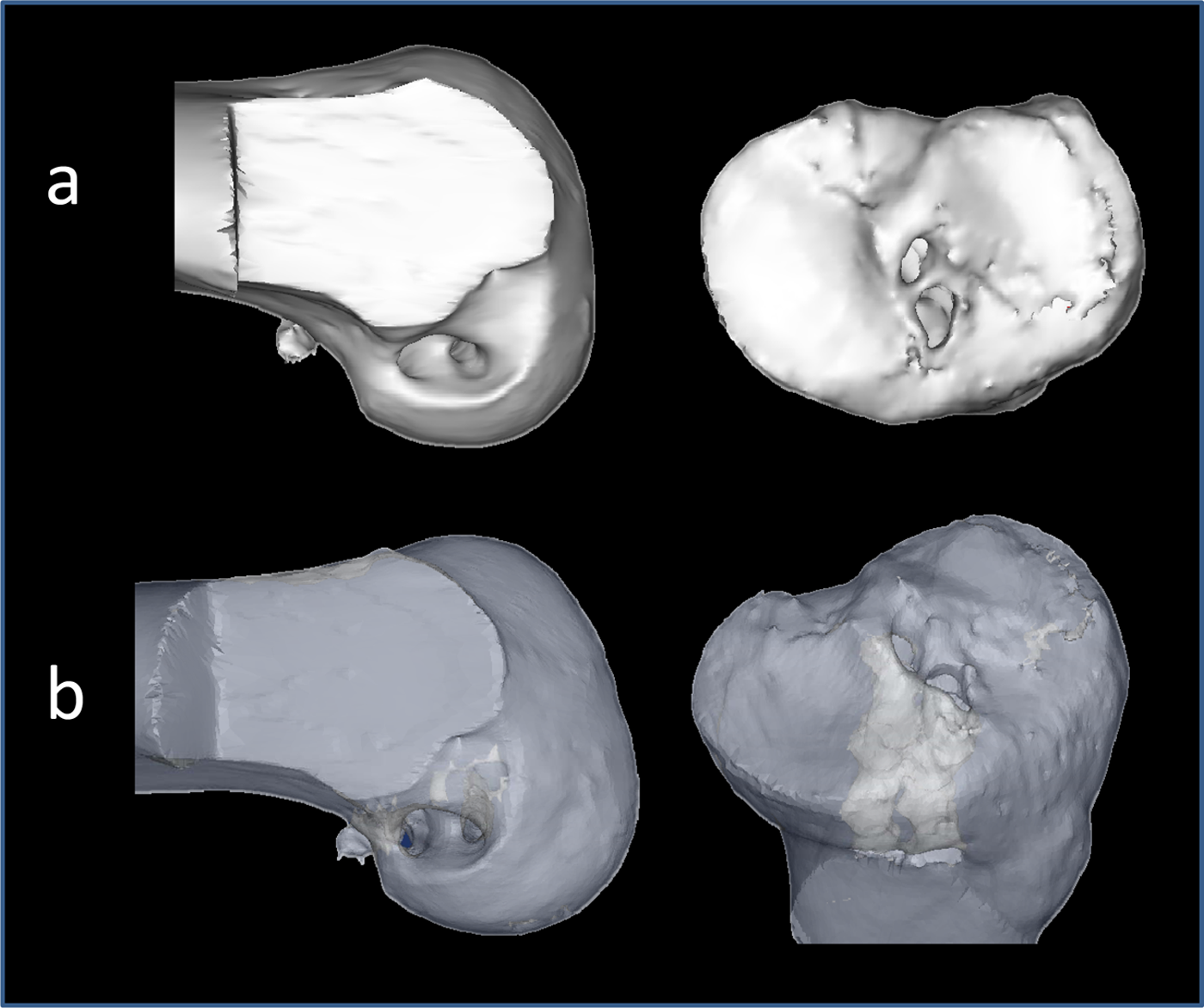
Three-dimensional computed tomography scan after anatomic double-bundle reconstruction with hamstring autograft in the left knee. (a) Evaluation of tunnel aperture placement. (b) Evaluation of tunnel trajectory.
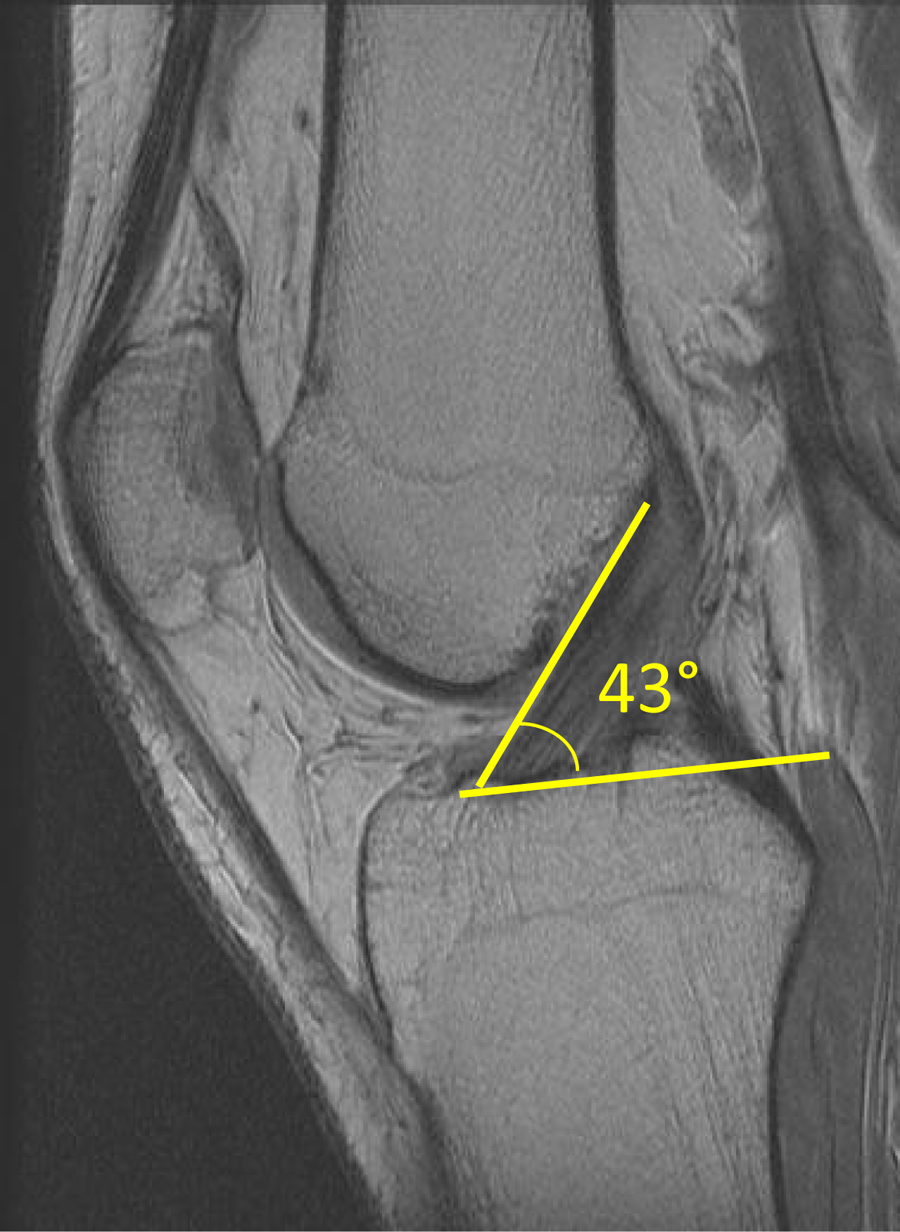
Measurement of the tibial insertion site inclination angle of the anterior cruciate ligament on magnetic resonance imaging.
Objective Outcomes of Surgical Techniques
In Vivo Kinematics
Non-Anatomic ACL Reconstruction
Traditional ACL reconstruction procedures are performed using a single-bundle graft, without attempting to recreate the native double-bundle ACL anatomy. Single-bundle, non-anatomic procedures may eliminate anterior/posterior laxity but fail to restore rotational stability.18,41
Numerous in vivo kinematic studies, using various loading conditions, have confirmed that these non-anatomic procedures fail to restore normal dynamic knee function ( Fig. 8 ). Georgoulis et al. 42 examined ACL-deficient individuals before and after non-anatomic bone–patellar tendon–bone ACL reconstruction during walking using video-motion analysis. The ACL-deficient patients demonstrated greater tibial internal rotation; however, it approached normal levels after ACL reconstruction. In a subsequent investigation performing higher demand activities, such as stair descent and pivoting, tibial rotation was significantly larger in the ACL reconstructed knees compared to the contralateral ACL-intact legs. 43
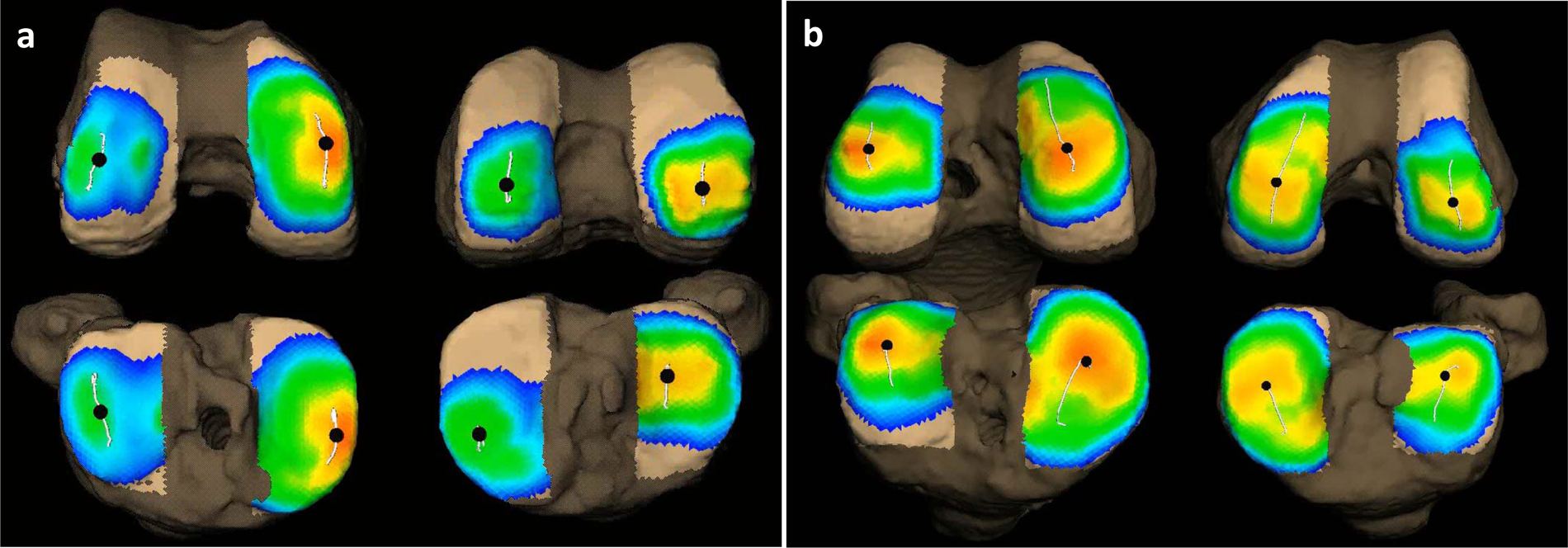
Two patients that underwent primary unilateral anterior cruciate ligament (ACL) reconstruction. Patient “
Skin motion artifacts may affect recorded measurements during kinematic investigations. Therefore, in vivo knee kinematics after ACL reconstruction has also been investigated using radiographic techniques, thus eliminating skin motion artifacts. Brandsson et al., 44 using continuous radiostereometric analysis, found that tibial rotation and anteroposterior translation were not restored by non-anatomic ACL reconstruction with bone–patellar tendon–bone autografts in 9 unilateral ACL patients at 1 year after surgery. Logan et al. 45 used open-access MRI to show that ACL reconstruction reduced sagittal laxity to within normal limits. ACL reconstruction did not, however, restore normal tibiofemoral kinematics during static weightbearing. 45 Papannagari et al. 46 studied ACL reconstructed knees using a dual-orthogonal fluoroscopic system and reported that although anterior laxity was restored, according to KT-1000 arthrometer testing, ACL reconstruction did not restore normal knee kinematics under weightbearing conditions.
Studies of more physically demanding tests require specialized high-speed radiographic imaging systems. Evidence of persisting rotational instability following ACL reconstruction was provided by Tashman et al.5,47 using a 250 frame/s dynamic stereo x-ray system to evaluate in vivo kinematics of the knee during downhill running for patients who underwent traditional, non-anatomic single-bundle reconstruction. Traditional single-bundle ACL reconstruction restored normal anteroposterior translation, but the reconstructed knees were more externally rotated and more adducted relative to the contralateral, uninjured knees. These rotational changes were associated with shifts in the areas of joint contact and a reduction in medial-compartment joint space under dynamic loading. There is substantial and growing evidence from in vivo knee kinematics studies that non-anatomic single-bundle ACL reconstruction fails to restore pre-injury knee function under functional loading conditions.
Anatomic ACL Reconstruction
Subjective outcome measurements (e.g., patient reported outcomes, pivot shift) have varied between single- and double-bundle ACL reconstruction, with the double-bundle procedure demonstrating a superiority in some, whereas others have shown no difference.25,48-50 Meredick et al. 49 showed that double-bundle reconstruction does not result in clinically significant differences in the KT-1000 measurement and pivot shift test compared with single-bundle ACL reconstruction. Araki et al. 51 reported that there were no significant differences in manual Lachman and pivot shift test, knee extension with heel height difference, knee flexion, and extension muscle peak torques at 60°, one-legged hop, and Lysholm score between anatomic single- and double-bundle ACL reconstructions.
Objective measurements have therefore recently been developed to determine whether differences exist between anatomic single- and double-bundle ACL reconstruction for restoring dynamic knee function and stability. Several video-motion analysis studies have found no difference in knee kinematics and rotational stability between double-bundle and single-bundle ACL-reconstructed knees during gait, high-demand pivoting activities, or other dynamic movement tasks.51-55 However, because of limitations associated with surface marker-based registration techniques, small alterations in transverse- and coronal-plane rotations or shifts in tibiofemoral contact locations may not be detectable with these methods. Therefore, these studies cannot provide definitive answers with regard to superiority of either the single- or double-bundle reconstruction technique.
Radiographic studies of knee kinematics overcome the limitations of skin markers by directly tracking bone motion. Abebe et al., 56 using biplanar fluoroscopy and MRI, reported that anatomic femoral placement of the graft in single-bundle reconstruction resulted in kinematics that more closely replicated that of the intact knee versus a non-anatomic femoral placement. This study, however, evaluated knee function during a series of static positions, so the results may not reflect true dynamic joint behavior.
Hoshino et al. 57 retrospectively studied 17 patients who underwent ACL reconstruction by the single-bundle (n = 7) or double-bundle (n = 10) procedure. They used dynamic stereo x-ray to capture biplane radiographic images of the knee during downhill treadmill running. Tibial anterior translation, axial rotation, and joint sliding distance in the medial and lateral compartments were compared between reconstructed and contralateral knees in both single- and double-bundle groups. Reduced anterior tibial translation and increased knee rotation were observed in the reconstructed knees compared with the contralateral knees in both single- and double-bundle groups. The mean joint sliding distance on the medial compartment was larger in the reconstructed knees than in the contralateral knees for both the single-bundle group (9.5 ± 3.9 mm vs. 7.5 ± 4.3 mm) and the double-bundle group (11.1 ± 1.3 mm vs. 7.9 ± 3.8 mm). These results suggest that neither ACL reconstruction procedure fully restored normal knee kinematics or medial joint sliding. A larger, prospectively randomized study is currently underway to rigorously evaluate this hypothesis. 58
Contact Patterns
Although anatomic ACL reconstruction may closely restore the mechanical function of the ACL such as anteroposterior tibial translation or rotation, occult cartilage abnormalities seen following ACL injury persist.59,60 Stergiou et al. 61 proposed that shifts of joint loading to normally unloaded regions may lead to development of osteoarthritis in both ACL-deficient and reconstructed knees. Rotational instability after ACL injury remains even following ACL reconstruction; however, the effects of these abnormal knee kinematics on joint contact and the resulting implications for the development of knee osteoarthritis have yet to be fully characterized.43,62-64
In a study by Hoshino and Tashman 65 using the dynamic stereo x-ray system, the relationship between rotational knee kinematics and joint contact paths revealed that a greater tibial internal rotation is associated with a larger magnitude of sliding motion in the medial compartment. In a previous study by Tashman et al., ACL reconstructed knees were more externally rotated and adducted during the stance phase of running. Therefore, abnormal motions, as described in these studies, may contribute to long-term joint degeneration associated with ACL injury and reconstruction.
Van de Velde et al. 66 investigated the abnormal cartilage contact deformation related to ACL reconstruction using a dual fluoroscopic and MRI technique. They reported that ACL deficiency shifted the articular contact location to smaller regions of thinner cartilage and increased the cartilage contact deformation, which may provide insight in the relationship between altered biomechanics and cartilage degeneration. Furthermore, after ACL reconstruction, a shift in cartilage contact resulted in a considerable change in cartilage loading distribution within the knee joint. Hosseini et al., 67 using a similar system, demonstrated that contact biomechanics of the tibiofemoral cartilage after ACL reconstruction were similar to those measured in intact knees. However, at lower knee flexion angles, an abnormal posterior and lateral shift of cartilage contact location to smaller regions of thinner tibial cartilage resulted in an increase of the magnitude of cartilage contact deformation, similar to ACL deficient knees. They suggested that clinically recovered anterior knee stability might be insufficient to prevent postoperative cartilage degeneration due to the lack of restoration of in vivo cartilage contact biomechanics. Therefore, the goal of ACL reconstruction should not only be the short-term clinical recovery of knee function but also the restoration of cartilage contact biomechanics to potentially prevent or limit the development of osteoarthritis. Continued progression toward this goal will require critical evaluation of ACL surgery using objective outcome measurement tools.
Conclusion
Over the past 10 years, a renewed interest in the native anatomy of the ACL has facilitated the progression of reconstruction techniques from non-anatomic to more anatomic techniques. Furthermore, double-bundle ACL reconstruction has also become popular as a potential means of more closely restoring the native anatomy and function of the ACL. To date, numerous studies comparing single- and double-bundle reconstruction techniques have been performed, but there is little evidence to suggest a superiority of one technique over another. 25 More recent work has focused on individualizing ACL reconstruction based on each patient’s distinct anatomical characteristics such as native insertion site size, as well as notch size and shape. Finally, investigators have turned to objective outcome measurement tools, such as in vivo kinematics, to provide a precise assessment of knee joint motion and contact mechanics. Continued investigation in ACL surgery and factors affecting the potential progression to osteoarthritis in the long term is essential in furthering the understanding to prevent this possible risk in the future.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study does not require institutional review board approval.