
Abstract
Objectives
The impact of anterior cruciate ligament (ACL) reconstruction on knee osteoarthritis (OA) is still unclear. The aim of the current meta-analysis was to compare surgical treatment versus nonoperative management of ACL tears to assess the impact of these approaches on knee OA development at a 5 and 10 years of follow-up.
Design
A meta-analysis was performed after a systematic literature search (May 2021) was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines. Both randomized and nonrandomized comparative studies with more than 5 years of follow-up were selected. Influence of the treatment was assessed in terms of knee OA development, subjective and objective clinical results, activity level, and risk of further surgeries. Risk of bias and quality of evidence were assessed following the Cochrane guidelines.
Results
Twelve studies matched the inclusion criteria, for a total of 1,004 patients. Level of evidence was rated low to very low. No difference was documented in terms of knee OA development, Tegner score, subjective International Knee Documentation Committee (IKDC), and Lysholm scores. A significant difference favoring the surgical treatment in comparison with a nonsurgical approach was observed in terms of objective IKDC score (P = 0.03) and risk of secondary meniscectomy (P < 0.0001). The level of evidence was considered very low for subjective IKDC, low for knee OA development, objective IKDC, number of secondary meniscectomies, and Lysholm score, and moderate for post-op Tegner score.
Conclusions
The meta-analysis did not support an advantage of ACL reconstruction in terms of OA prevention in comparison with a nonoperative treatment. Moreover, no differences were reported for subjective results and activity level at 5 and 10 years of follow-up. On the contrary, patients who underwent surgical treatment of their ACL tear presented important clinical findings in terms of better objective knee function and a lower rate of secondary meniscectomies when compared with conservatively managed patents.
Keywords
Introduction
Anterior cruciate ligament (ACL) tears are common injuries among young and active individuals involved in sport activities that imply contact, deceleration, twisting, cutting, and jumping. Approximately 200,000 ACL tears occur every year in the United States with an increasing number of ACL reconstructions (from 32.4 patients per 100,000 person/year in the early 1990s to 43.5 patients per 100,000 person/year in the 2010s).1-5 Laxity due to ACL injury causes reduced knee function and abnormal changes at different levels in terms of joint homeostasis, with lower activity levels and poorer quality of life.6,7 While the consequences of the detrimental biomechanical changes are well recognized, more debated remains their management, with both surgical and conservative treatments being proposed to date. 8
Restoring knee anatomy and biomechanics through surgery can minimize sheer and torsional forces on menisci and cartilage surface, legitimating a safer return to previous levels of activity.9,10 On the contrary, there is also evidence that injured patients could cope well with ACL deficiency and thus they may undergo a conservative approach, which could lead to enough functional stability and no secondary injuries, as well as to the desired level of pivoting and cutting activities.11-16 While the clinical benefit of surgery versus conservative treatment is still debated, even more controversial is the possibility to limit joint degeneration by reconstructing the ACL, with conflicting results regarding the most effective approach to prevent knee osteoarthritis (OA).17,18
The aim of the present meta-analysis was to quantitatively synthesize the best literature evidence on this topic, including only studies directly comparing surgical treatment versus nonoperative management of an ACL tear, with a clear radiological knee OA evaluation and at least 5 years of follow-up. The hypothesis was that surgical treatment could provide lower rates of knee OA, while ensuring better knee function and higher activity levels compared with the conservative management of ACL tears.
Materials and Methods
Search Strategy and Article Selection
A systematic literature search was performed on May 10, 2021, using PubMed, Web of Science, Cochrane library, Scopus literature, and gray literature databases using the following string: (ACL injury OR ACL tear OR ACL rupture) AND (ACL reconstruction OR ACL surgery OR non-operative OR conservative OR non-reconstructive) AND (osteoarthritis OR OA). All duplicates were removed and then all records were assessed for eligibility by title and abstract, with full-text reading evaluation when needed. Inclusion/exclusion criteria are reported in Table 1. The Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines were used. The article selection process was independently performed by 2 authors (M.C., D.P.) with disagreement solved by consensus or by the intervention of a third author (L.D.). 19
Inclusion and Exclusion Criteria for Study Selection.
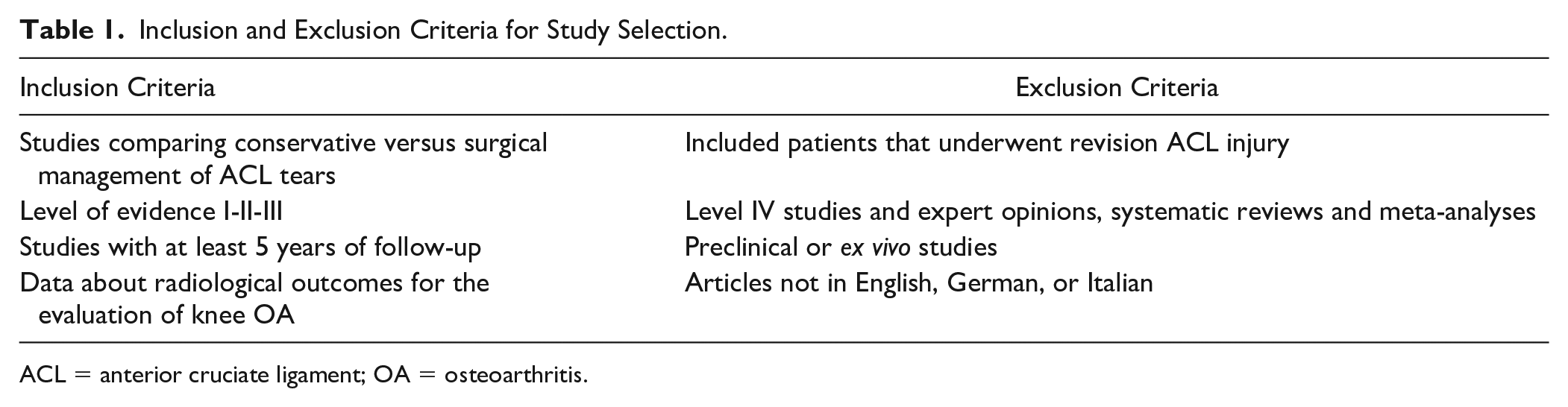
ACL = anterior cruciate ligament; OA = osteoarthritis.
Data Extraction, Synthesis, and Measurement of Outcomes
Relevant data from the included articles were independently extracted by 2 authors from the full-text version or supplementary data (M.C., L.D.), using a previously extraction form according to Cochrane’s guidelines. Nonoperative approach was defined as all the treatment options not involving a surgical reconstruction, that is, physiotherapy, functional training, wait and see, bracing, and so on. Information on study methodology concerned level of evidence, study design, inclusion/exclusion criteria, graft source, time from injury to intervention, other associated surgical treatments, post-surgical rehabilitation, and follow-up length. Patients’ characteristics and clinical outcomes of treatments were also collected: number of patients included and assessed at follow-up, patients’ sex, age, body mass index (BMI), and cause of injuries, previous surgical treatment on the index knee, associated lesions, pre-surgical and post-surgical clinical scores (objective International Knee Documentation Committee [IKDC], subjective IKDC, Lysholm, Tegner, Knee injury and Osteoarthritis Outcome Score [KOOS]), rate of re-tears, rate of complications, knee stability, secondary meniscectomies, and radiological results (IKDC, Kellgren and Lawrence, Fairbank, Ahlbäck, and joint space narrowing Osteoarthritis Research Society International – OARSI – scoring systems). To normalize data from the different radiological scores, the equivalence table reported in the article by Kohn et al. 20 and a cutoff higher than second grade on Kellgren and Lawrence, Ahlbäck and OARSI scoring system, and C grade on Fairbank and IKDC scoring systems were set to identify clinically significant OA according to previous literature.21-24 As such, OA was considered as a dichotomous outcome.
Assessment of Risk of Bias and Quality of Evidence
The risk of bias was assessed using the revised tool for Risk of Bias in randomized trials (RoB 2.0) and in nonrandomized trials (ROBINS-I) approved by the Cochrane collaboration group.25,26
Randomized studies were considered as “low risk” of bias if a low risk of bias was scored in all domains of the analysis; it was rated as “some concerns” if a score of “some concerns” was obtained in at least one domain of the analysis. In the end, randomized studies were judged as “high risk” if the study was judged to be at high risk of bias in at least one domain of the analysis or it had risen some concerns for multiple domains.
Nonrandomized studies were rated as at a low risk of bias if data were reasonably complete, proportions, and reasons for missing participants were similar across intervention groups, the analysis addressed missing data, and is likely to have removed any risk of bias. A study was judged as moderate risk of bias if there were deviations from usual practice, but their impact on the outcome is expected to be slight and proportions of and reasons for missing participants differ slightly across intervention groups. In the end a study was rated at a high risk of bias if methods of outcome assessment were not comparable across intervention groups and there were important co-interventions not balanced across intervention groups, or there were deviations from the intended interventions (in terms of implementation and/or adherence) that were likely to impact on the outcome.
The overall quality of evidence for each outcome was graded according to the Grading of Recommendations Assessment, Development and Evaluation (GRADE) guidelines. 27 An outcome was deemed to have a very low level of evidence if the true effect was probably markedly different from the estimated effect. A low level of evidence was marked when that the true effect is similar to the estimated effect. Similarly, a moderate and high level of evidence was assigned when the true effect of intervention was deemed very close or almost the same of the true effect.
Statistical Analysis
To investigate the effect of treatment on all outcomes, different analyses were conducted. Using RevMan software 5.3, the differences between surgical and conservative management of ACL injury in terms of knee OA, subjective and objective IKDC, Tegner activity level, Lysholm score, and need of a secondary meniscectomy were assessed through the Mantel-Hanszel test and expressed as risk ratios for dichotomous variables (RR = risk ratio surgical/conservative), and through the inverse variance method and expressed as mean differences for continuous variables (MD = mean difference surgical-conservative). Heterogeneity was tested using Cochran’s Q statistic and I2 metric and was considered significant when I2 > 25%. A fixed-effect model was preferred in the absence of significant heterogeneity; when the I2 was above the cutoff of 25%, a random effect model was used. Due to the high clinical heterogeneity of the included studies (heterogeneous rehabilitation protocols, different activity levels, etc.), a sensitivity statistical analysis was performed, applying the random effect model for all the considered outcomes. A P value of 0.05 was set as level of significance. When data from the same study population were available at different follow-ups or in different studies, the longest-term follow-up was selected. This choice was made in light of the nature of OA evolution, as it is a condition which often requires many years to be clinically evident. As such, a sensitivity analysis was performed including only studies with a follow-up longer than 10 years. A sensitivity analysis excluding all confounding factors (i.e., age, meniscal injuries.) was considered; however, single patient data were not available. As such, a pair match analysis to normalize confounders could not be performed.
When mean and standard deviations were not available from the full-text articles, they were estimated from median range and sample size using the formula proposed by Hozo et al. 28 or following the Cochrane guidelines, and sensitivity analyses excluding these studies were performed.
Results
Article Selection and Patients’ Characteristics
The PRISMA flowchart of the article’s selection process is presented in Figure 1. Out of 2,424 identified studies, 12 were included in the quantitative synthesis (3 randomized controlled trials [RCTs] and 9 non-randomized comparative studies). To evaluate OA rates, 4 studies used the Kellgren and Lawrence score, 4 opted for the IKDC radiological score, 2 opted for the OARSI joint space narrowing scoring system, 1 study used the Fairbank score, and 1 used the Ahlbäck score. The mean follow-up was 11 years ranging from 5 to 24 years. Ten studies opted for a bone patellar tendon bone (BPTP) graft; in one article, both BPTP and hamstring grafts were included, and one article did not specify the graft used. Subjective IKDC was reported in 5 studies, objective IKDC was assessed in 7 articles, Lysholm was reported in 9 studies, and Tegner activity level was analyzed in 9 studies. Secondary meniscectomies were reported in 5 studies.
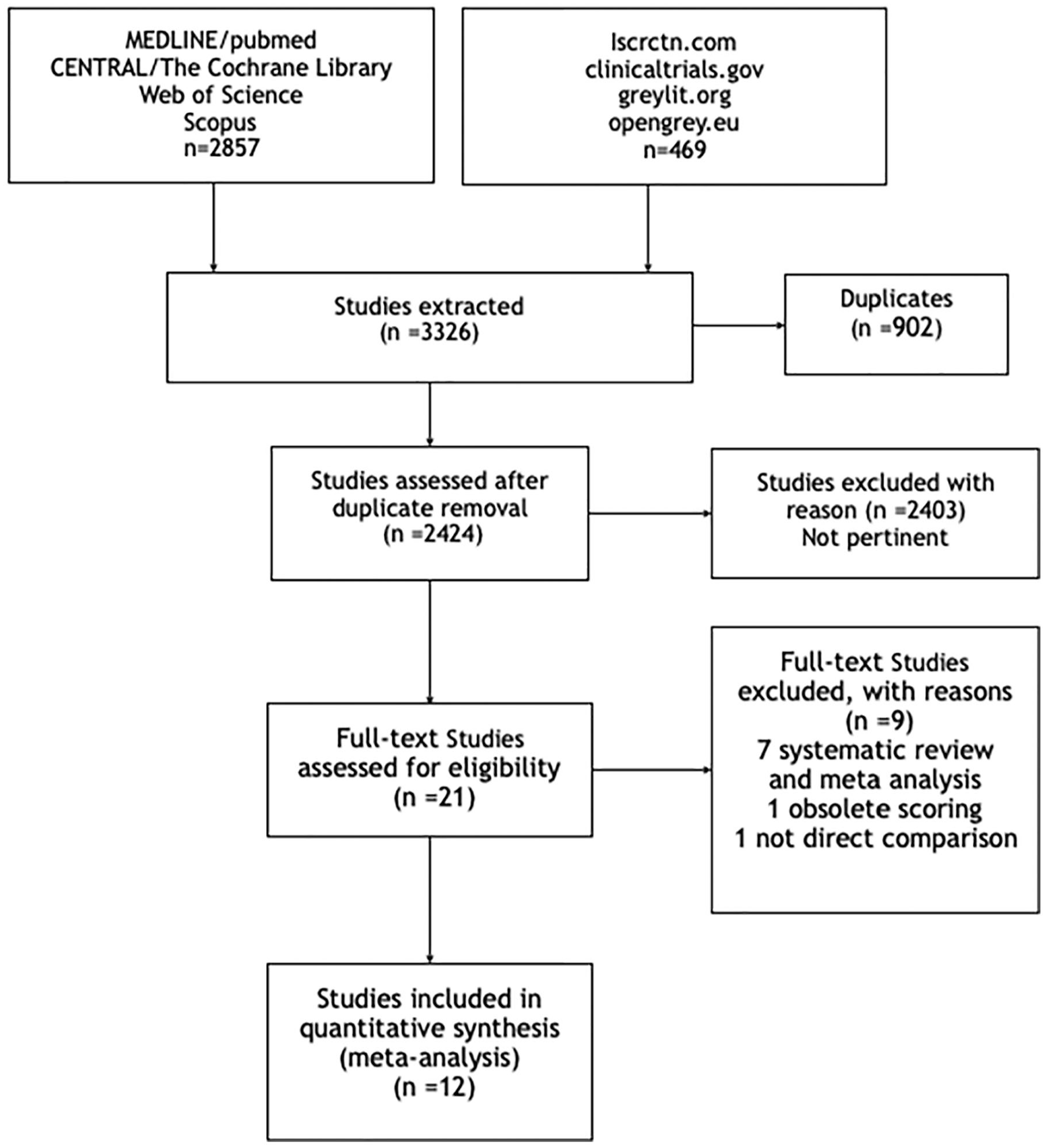
PRISMA flowchart of the article selection process. PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-analysis.
Overall, 1,004 patients were included in this meta-analysis, 547 in the surgical group, and 457 in the conservative group. The male/female ratio was 2:3, and the overall mean age at the time of injury was 30 years (range: 18-56 years). No significant differences in baseline characteristics of the patients were found between the 2 treatment approaches in all included studies. Further details on studies and patients are reported in Table 2.
Characteristics of the Included Studies and Patients.
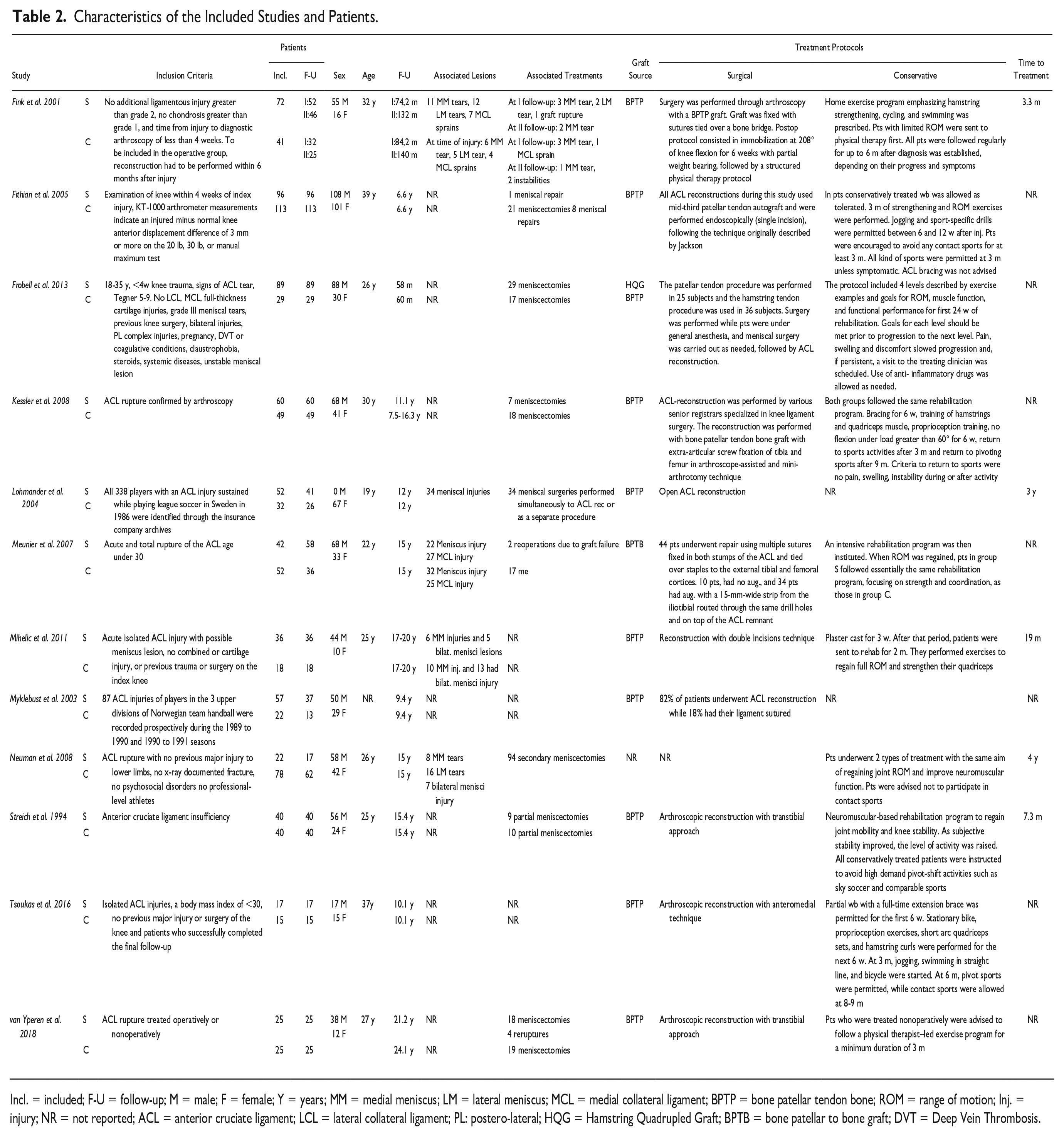
Incl. = included; F-U = follow-up; M = male; F = female; Y = years; MM = medial meniscus; LM = lateral meniscus; MCL = medial collateral ligament; BPTP = bone patellar tendon bone; ROM = range of motion; Inj. = injury; NR = not reported; ACL = anterior cruciate ligament; LCL = lateral collateral ligament; PL: postero-lateral; HQG = Hamstring Quadrupled Graft; BPTB = bone patellar to bone graft; DVT = Deep Vein Thrombosis.
Outcomes of Surgical versus Conservative ACL Reconstruction
In the surgical versus conservative analysis, no significant differences were found in terms of development rates of knee OA (12 studies, RR = 0.93, P = 0.19, confidence interval [CI]: 0.86-1.31; Figure 2). These results were confirmed by the sensitivity analysis including only studies with a follow-up longer than 10 years (8 studies, RR = 1.14, P = 0.49, CI: 0.74-1.28).
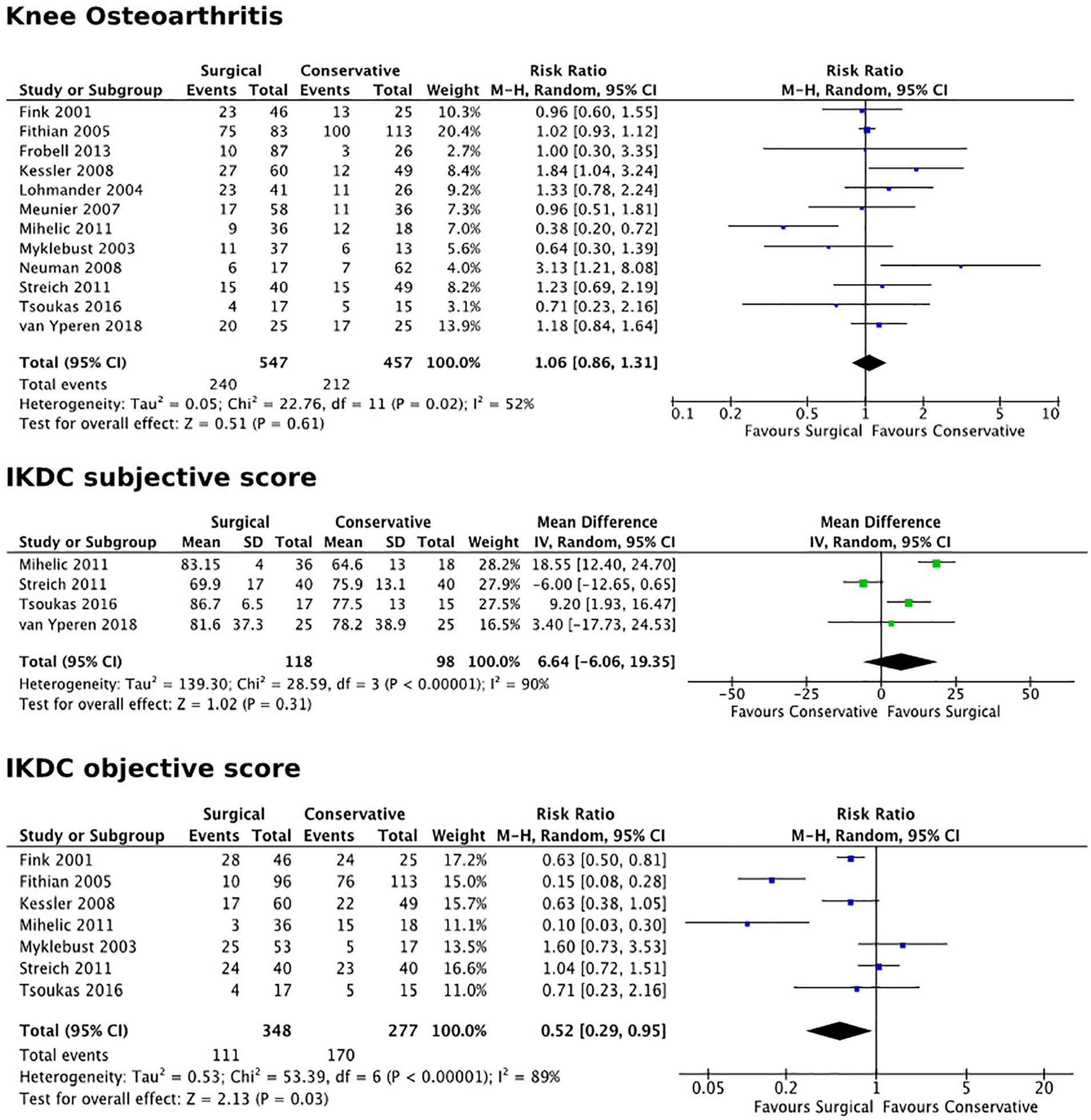
Forest plots for knee osteoarthritis rates and IKDC subjective and objective evaluation forms. IKDC = International Knee Documentation Committee; CI = confidence interval.
No statistically significant differences were also found in terms of subjective IKDC score (4 studies, MD = 6.6, P = 0.31, CI: −6.06 to 19.35; Figure 2), Lysholm score (8 studies, MD = 5.6, P = 0.14, CI: −1.77 to 12.93), and Tegner activity level (9 studies, MD = 0.1 P = 0.69, CI: −0.64 to 0.65; Figure 3) at final follow-up. Objective evaluation in terms of abnormal/severely abnormal IKDC objective score was found statistically significant (7 studies, RR = 0.52, P = 0.03, CI: 0.29-0.95; Figure 2) in favor of the surgical treatment in comparison with the nonsurgical treatment. A higher number of patients (66 out of 226 assessed) in the conservative group required secondary arthroscopic meniscectomy, whereas only 29 of the 249 included in the surgical group went through this procedure during follow-up (5 studies, RR = 0.42, P < 0.0001, CI: 0.27-0.63; Figure 3).
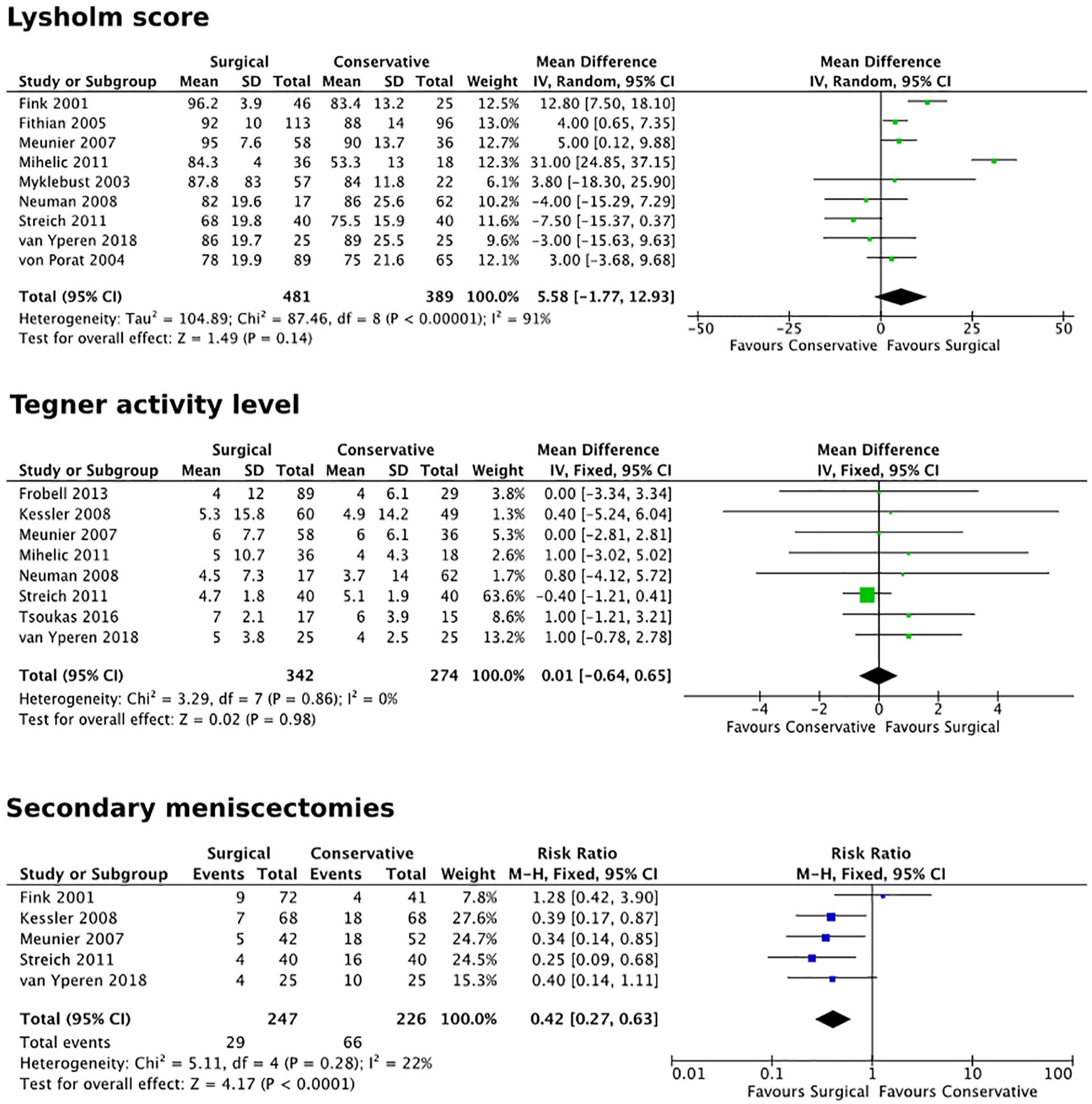
Forest plots for Lysholm and Tegner scores and risk of secondary meniscectomies. CI = confidence interval.
Risk of Bias and Quality of Evidence
The risk of bias was rated moderate (“some concerns”) in the 3 RCTs: the main source of bias was the lack of blinding of the assessor, which could influence the evaluation of the outcome. Moreover, the possibility to undergo surgery given to the patients of the conservative group in 2 of the RCTs included29,30 may have directed the patients with a worst outcome outside the conservative group. In the nonrandomized comparative trials, the risk of bias should be considered high. The main problem was the presence of confounders that cannot be controlled: among all, the level of activity after intervention may be different in the 2 groups and this could seriously affect results at long-term follow-up.
The level of evidence was considered very low for subjective IKDC, low for knee OA development, objective IKDC, number of secondary meniscectomies, and Lysholm score, and moderate for post-op Tegner score. The risk of bias of the included studies was considered to have influenced the results of all outcomes. Statistical heterogeneity was above the cutoff of I2 = 25% in the results of 4 out of 7 outcomes: this may be due to the heterogeneity in the characteristics of the included patients and in the rehabilitation protocols. Finally, the low number of patients included caused further downgrading of the level of evidence for “imprecision” for subjective IKDC and number of meniscectomies. Details of risk of bias assessments are listed in Figures 4 and 5.

Risk of Bias of Included Randomized Controlled Trial.
Risk of Bias of Included Nonrandomized Controlled Trial.
Discussion
The main finding of this meta-analysis is that there is no evidence supporting that ACL reconstruction prevents knee OA. Moreover, similar results were obtained in terms of subjective outcomes and activity level versus the nonoperative approach. On the contrary, the objective knee evaluation was in favor of surgery, which also reduced the need for secondary meniscectomies.
Patients who withstand an ACL rupture are at a higher risk of developing knee OA than the general population (prevalence 24.5%-51.2%). 31 The detrimental effects on joint biomechanics have been well-demonstrated by several studies, both ex vivo and in patients.32,33 Residual chronic instability can result in a bigger risk of cartilage damage and, consequently, higher rates of knee OA, due to the higher stress endured by the joint for the lack of one of the knee’s main static stabilizers. From this perspective, surgery has been considered an effective option to reduce instability with the aim of preventing the development of secondary degeneration.34-38
However, the exact pathogenic mechanisms through which ACL injury influences the progression of joint degeneration are still not clear, as many factors, aside from joint instability, concur in the pathogenesis and progression of knee OA. 39 In this light, an ACL rupture must be considered as a lesion involving the whole joint rather than a mere ligament injury. Many other knee structures can be affected, which can also be responsible for the development of knee OA. 40
The frequent presence of associated lesions underlines an important aspect: the impact of the acute trauma on all knee structures.39,41,42 To this regard, bone bruise has a high prevalence (up to 55.2% in the most recent papers) among ACL injured individuals, and its persistence has been correlated to a more severe degenerative progression of the entire joint. 42 Recent evidence also suggested possible effects on the long-term clinical outcome.41,42 The altered subchondral bone signal can be the expression of a worse joint derangement.43,44 In fact, size and location of bone bruise correlate with the presence of meniscal lesions, which are one of the main risk factors for post-traumatic knee OA. 45 Other studies46-48 also showed a correlation with an increased rate of cartilage damage, another trigger for the development of knee OA. 49
Cartilage lesions are often described in correspondence to the index trauma at the BME (Bone Marrow Edema) level, with an estimate overall prevalence of 32% among patients undergoing primary ACL reconstruction. 50 The presence of cartilage lesions can negatively affect the outcome of ACL injuries. Many studies on large cohorts of patients, such as those from the Scandinavian national registry51-53 and the MOON cohort,54,55 pointed out how patients with cartilage defects benefit less from an ACL reconstruction, achieving significantly lower Patient-Reported Outcome Measure (PROM) scores at mid-term follow-up. Moreover, this joint derangement can go beyond the local damage to the articular surface. High-energy traumas can trigger an immune response in both chondrocytes and synoviocytes, which produce inflammatory mediators such as interleukins 1, 6, and 8 as well as tumor necrosis factor (TNF). 56 These molecules are able to induce proteoglycans degradation, collagen destruction, as well as chondrocytes necrosis. Recent evidence shows that prolonged activation of inflammatory pathways due to an ACL injury can alter joint homeostasis and OA biomarkers: fluid aggrecan, MMP-1, MMP-3, and ADAM12 were found increased, whereas the metalloprotease inhibitor TIMP-1 tended to decrease after ACL injury. 57 Thus, besides causing the first insult at the cartilage level, the index trauma can alter the joint homeostasis by triggering detrimental inflammatory and degenerative processes.
Another key aspect that can influence knee OA progression is the meniscal status, as the incidence of degeneration after ACL rupture ranges from 16% for an isolated lesion to 50% when the injury involves a meniscal lesion. 58 A previous meta-analysis on 1,554 patients after an ACL reconstruction pointed out that OA prevalence was significantly higher in those undergoing meniscectomy, yielding a 3.5 higher odds of developing knee OA at long term. 59 Moreover, cartilage lesions associated with meniscal tears have been correlated with poorer subjective and objective results. 60 Secondary meniscectomies, especially of the medial meniscus, wielded a higher risk of post-traumatic knee OA also in conservatively treated patients. 61
The results of this meta-analysis confirmed previous literature36,62 showing a higher number of secondary meniscal procedures in patients treated conservatively. However, while the protection of the meniscal structure from ACL reconstruction was demonstrated, the impact of the lower number of secondary meniscectomies in terms of knee OA preventions is still controversial. A recent study of Lien-Iversen et al. suggested higher OA rates in surgically treated patients, although with some limitations due to the low number of included patients. 62 On the contrary, the paper of Øiestad et al. 63 pointed out that patients who returned to pivoting sport had lower rates of knee OA, although with a high risk of selection bias due to the retrospective nature of this study. This meta-analysis overcame some of the limitations of previous publications, including all published comparative studies on this topic. Data from the available literature showed a lower number of meniscectomies after ACL reconstruction, but still similar rates of OA at 5 and at 10 years of follow-up. The unexpected results in terms of lack of OA protection from surgical ACL reconstruction and joint biomechanics restoration might be explained from different perspectives.
A possible explanation of the finding that ACL surgery did not have an impact over OA development may be that, aside from 3 rather small RCTs,29,30,40 most of the literature relies on cohort studies where the choice of treatment was made according both to the surgeons’ opinion and the patients’ desires. Patients who chose a surgical treatment might have different expectations and desired level of activity, whereas individuals choosing a nonsurgical approach could have been advised on the importance of lowering their level of activity, avoiding activities which could be detrimental for their joints.13,64 Patients often opt for surgery aiming at a return to sport, which can entail remarkable stress on their knees. This higher level of stress could impact on the development of knee OA. However, this remains a mere speculation. While the sport activity level after surgery is a key aspect, it was unfortunately poorly documented by the available studies. Future research should monitor and properly report both return to sport and activity level of treated patients, as this factor may be crucial in concealing the potential benefits of surgery in terms of knee OA development.34,65
Another aspect should be considered while interpreting these findings. The current literature presents limitations which are inevitably reflected in this meta-analysis. The majority of the studies are nonrandomized trials with a serious risk of bias. Besides the high risk of selection bias with uncontrolled confounders, in 2 out of 3 included RCTs patients were given the possibility to undergo surgery in case of unsatisfactory results with the conservative treatment: this unavoidably has led to the exclusion from the conservative group of patients with the worst outcome. Moreover, current studies do not allow to properly handle statistically the data from cross-over patients and delayed surgeries. As a result, the documented level of evidence is low for the evaluation of the risk of OA development (primary outcome of the study) and in almost all the secondary outcomes. This hinders the possibility to draw definitive conclusions on this issue, and new high-level trials should shed light on this topic. 66 Furthermore, the use of different radiological scoring systems to evaluate OA may be an important source of heterogeneity and represents another weakness of this evaluation: the IKDC scoring system could overreport the severity of OA 67 and the Ahlbäck classification has a poor inter- and intraobserver agreement. 68 Finally, we analyzed papers with more than 5 years of follow-up and performed a sensitivity analysis at 10 years. Still, the latter was based on a lower number of patients, which warrants more research efforts toward documenting results at long term, when a difference in terms of OA development may be more likely detected. Nonetheless, despite these limitations, this meta-analysis, performed according to Cochrane guidelines, was able to quantitatively synthesize several aspects and to underline some interesting findings. ACL reconstruction is a common and effective procedure able to restore knee biomechanics; however, despite the better objective outcome and the protection from further meniscal lesions, there is no evidence of benefits in terms of OA development after surgical treatment of ACL tears.
In the end, this meta-analysis of the current literature did not support an advantage of ACL reconstruction in terms of OA prevention. Moreover, no differences were also reported for subjective results and activity level at mid/long-term follow-up. On the contrary, some clinically relevant findings have been underlined, both in terms of joint derangement and functional outcome. Patients who underwent a surgical treatment of their ACL tear presented better knee function and a lower rate of secondary meniscectomies in comparison with nonoperatively managed patents.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Cuzzolin, Dr. Deabate, Professor Filardo, and Dr. Previtali declare they have no conflict of interest. Professor Zaffagnini reports personal fees from I+ SRL, grants from Fidia Farmaceutici SPA, CartiHeal ltd, IGEA Clinical Biophysics, BIOMET, and Kensey Nash, outside the submitted work. In addition, Professor Zaffagnini has a Springer patent with royalties paid. Professor Candrian reports grants from Medacta International SA, Johnson & Johnson, Lima Corporate, Zimmer Biomet, and Oped AG, outside the submitted work.
Ethical Approval
This study was approved by our institutional review board.