
Abstract
Objective
To synthesize available evidence on the impact of concomitant focal cartilage lesions and their surgical treatment on clinical outcomes in the setting of anterior cruciate ligament (ACL)-reconstruction at short (6-36 months) and midterm (3-8 years) follow-up.
Design
Original level 1 or 2 studies comparing any patient-reported or objective outcomes in ACL-reconstructed patients (1) with and without concomitant focal cartilage lesion(s) or (2) after any type of cartilage surgical treatment were considered for inclusion. Systematic searches were conducted in MEDLINE via Ovid, Cochrane Library, EMBASE via OvidSP, and Web of Science.
Results
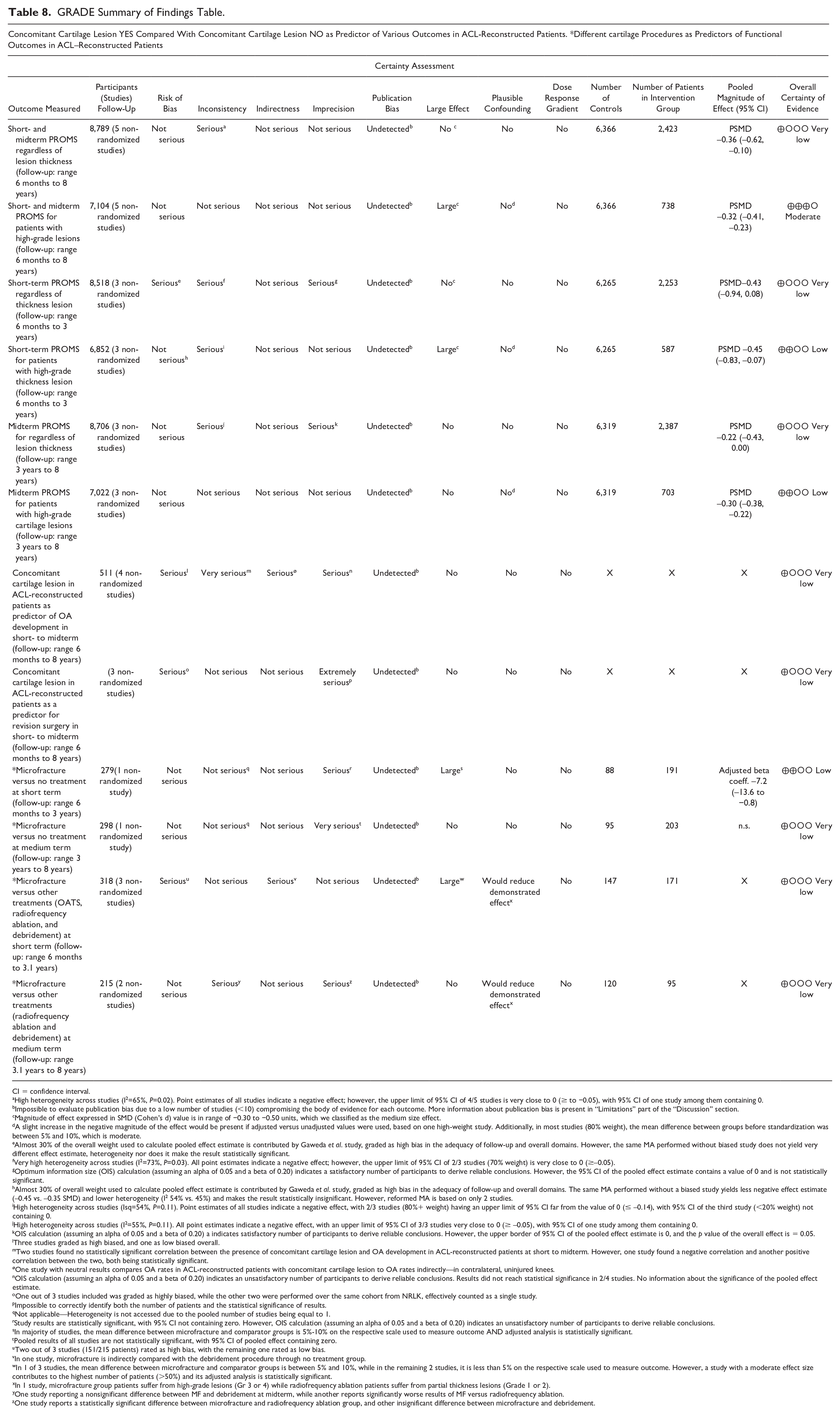
In meta-analysis performed across 6 studies (n=8,789 patients), we discovered with very low certainty, the correlation of concomitant any-thickness cartilage lesions and worse Patient-Reported Outcome Measure scores (PROMS) at cumulative short to mid, (pooled standardized mean difference (psmd) = −0.36; 95% confidence interval (CI) –0.62 to −0.10), short (psmd = −0.43; 95% CI = −0.94 to 0.08), and midterm (psmd = −0.22; 95% CI –0.43 to 0.00). Full-thickness lesions predicted worse PROMS with moderate certainty at cumulative short-midterm (psmd = −0.32; 95% CI = −0.41 to −0.23) and low certainty at both short (psmd = −0.45; 95% CI –0.83 to −0.07) and midterm (psmd = −0.30; 95% CI –0.38 to −0.22). In 4 studies for each outcome, mixed results were reported on osteoarthritis (OA) and reoperation rates.
Conclusions
As the main finding, concomitant full-thickness cartilage lesions in ACL-reconstructed patients are a predictor of worse PROMS in the cumulative short to midterm. Correlations of any-thickness lesions or different cartilage treatments with short- or midterm PROMS, OA, or reoperation rates were either with very low certainty, unmeasured, or with mixed results.
Introduction
The anterior cruciate ligament (ACL) is a functionally important component of a healthy knee joint. Due to high functional demands, acute tears of the ACL are common, especially in young, athletic individuals. The reported incidence ranges up to 68.8 cases per 100,000 person-years worldwide.1-4 ACL rupture is characterized in the short term by pain, instability, and reduced range of motion due to effusion5,6 and in the long term by potential premature emergence and accelerated progression of osteoarthritic changes.7-9 Concomitant focal cartilage lesions are an important predictor of functional outcomes after ACL reconstruction,10,11 detected in 19%-36% of all patients undergoing ACL reconstruction.12-14 Although cartilage lesions contribute to knee osteoarthritis (OA) development in the long term,15,16 their influence on Patient-Reported Outcome Measure Scores (PROMs) is still not well understood.17-20
Between 2017 and 2021, 4 systematic reviews (SRs) were published21-24 on PROMs or objective outcomes at short- to midterm follow-up after ACL reconstruction in patients with cartilage lesion(s). The majority of the existing SRs on this topic did not restrict themselves to studies with higher levels of evidence, or the Grading of Recommendation, Assessment, Development, and Evaluation (GRADE) Working Group’s guidelines for grading the quality of evidence.21,22 Notably, none of the relevant published SRs performed quantitative synthesis of results in a meta-analysis. Consequently, neither the prognostic value nor the optimal treatment of cartilage lesions in ACL-reconstructed patients is well established.
Identification of the short- and midterm clinical outcomes after ACL reconstruction in patients with and without cartilage lesions was determined as the primary study objective. Identification of the preferred surgical approach for treating cartilage lesions at the time of ACL reconstruction was determined as a secondary study objective.
Methods
This SR and meta-analysis was performed following a predefined protocol complying with recommendations from the Cochrane Musculoskeletal Group, 25 and designed following the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA-P) guidelines. 26
Inclusion and Exclusion Criteria
Original level 1 or 2 studies 27 reporting outcomes after ACL reconstruction in patients with cartilage lesions, comparing either different surgical treatments, or to patients without cartilage lesions were included. All studies had to be published in full-text in English or Norwegian after 1945.
All comparisons had to be made either at a specific follow-up point or as changes from baseline within a timeframe of 6-36 months (short term) or 3-8 years (medium term) after ACL reconstruction.
Studies reporting any type of patient-reported or objective outcome measures were considered eligible. Studies reporting on rates of return to sport, adverse events, complications and harms of intervention, reoperations, or failures of intervention were also considered eligible for inclusion.
Laboratory, cadaver, and biomechanical studies or those reporting primarily on patients with concomitant OA, bone bruises, chondromalacia, ACL revision surgery, or partial ACL tears at baseline were excluded.
Literature Search Strategy
We collected data primarily from the following medical databases: MEDLINE via Ovid, Cochrane Library, EMBASE via OvidSP, and Web of Science. The search strategy was developed by the review team, in collaboration with a medical librarian (S.T.K.) with expertise in SR searches. A detailed draft of the final search strategy in the MEDLINE via Ovid electronic database on 09.03.2023. is displayed in Table 1 .
Literature Search Strategy in Medline via Ovid Electronic Database.
Database(s):
Secondary data were collected after a manual search on the topic in 3 of the most frequently cited journals, 28 in relevant on-going or recently completed trials 29 and snowball search of references within included studies and excluded relevant SRs found during the primary search.
Screening across Inclusion Criteria
References obtained from the primary literature search were imported into the DistillerSR® software, 30 where they were screened for eligibility across the predefined inclusion and exclusion criteria. Duplicate references were identified and removed. The remaining references underwent title, abstract, and full-text screening. References consistent with the inclusion criteria on every screening level proceeded to the data extraction stage. Relevant information was extracted using one of two customized, pre-designed extraction forms comprising 147 and 91 questions, respectively, in either a multiple-choice or an open-ended form. The assessment on each level was performed independently by two members of the research team. Conflicts were resolved through discussion or involvement of other members of the research team.
Data Items
The following data items were extracted from each study eligible for qualitative or quantitative analysis: general information, study characteristics, participant characteristics, characteristics of comparator or intervention group, follow-up times, and primary and secondary outcome measures.
Risk of Bias and Quality of Evidence Assessment
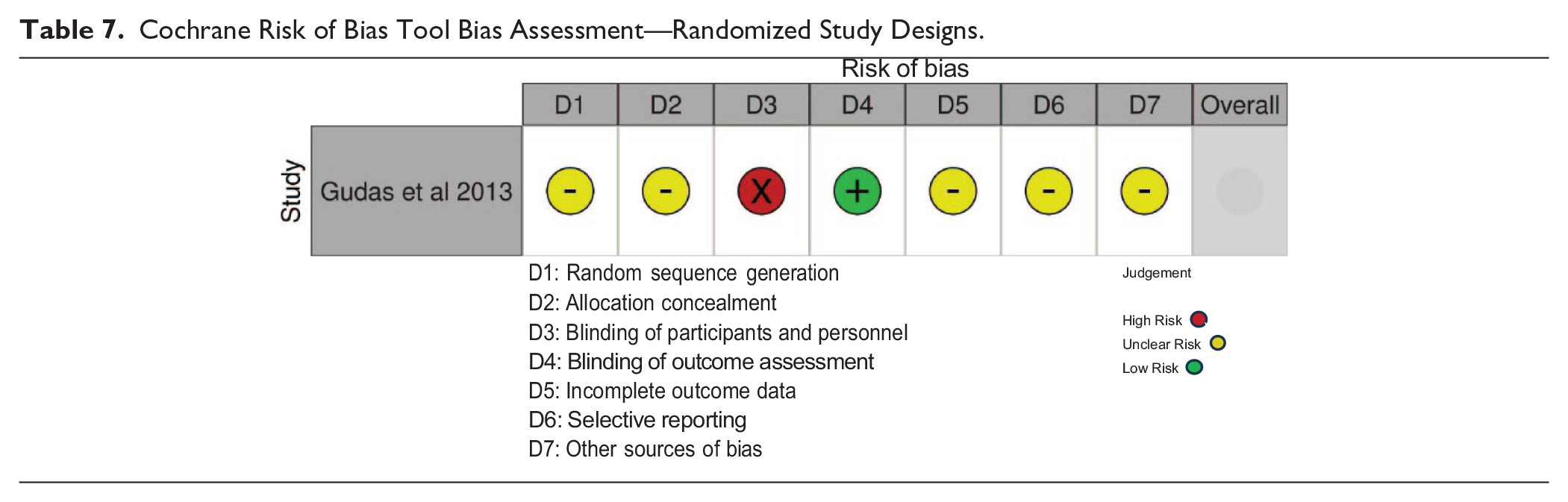
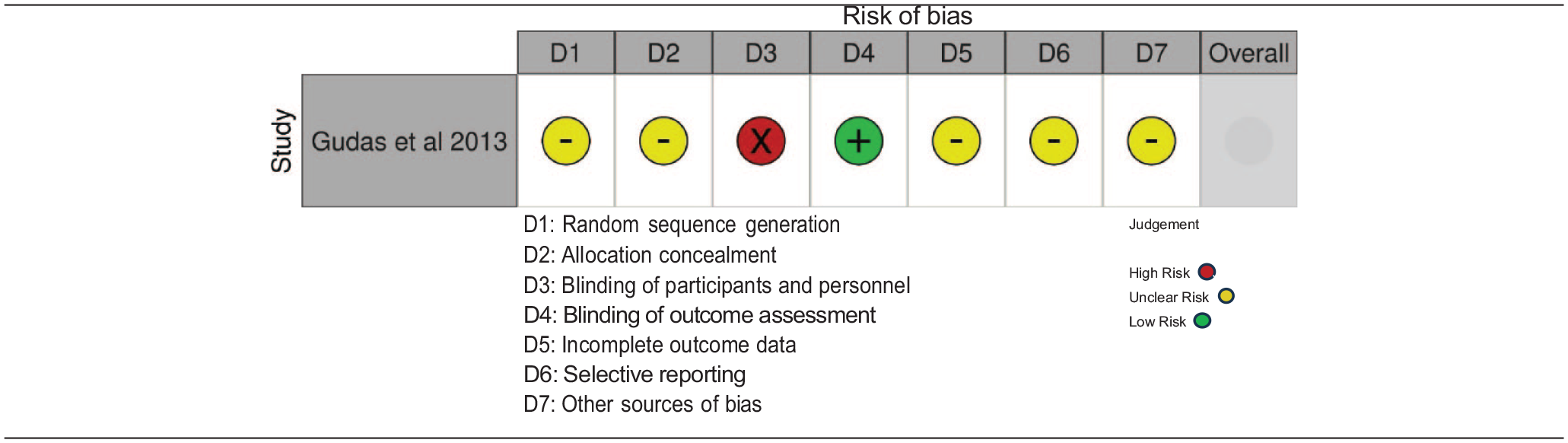
We evaluated the included randomized studies with the Cochrane Collaboration tool for assessing the risk of bias.25,31 The tool consists of multiple subdomains each graded with high, low, or unclear risk of bias after further qualitative elaboration.
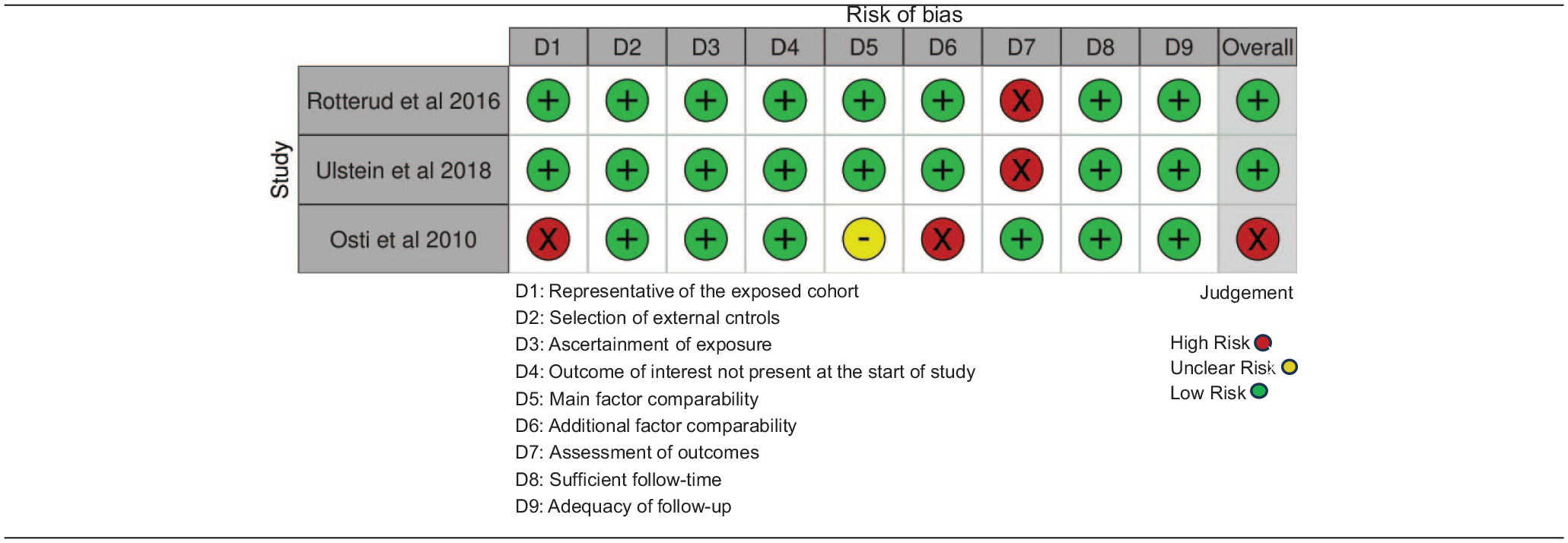
Bias in non-randomized studies was evaluated using the Newcastle Ottawa Scale (NOS). 32 The scale comprises 3 main domains: selection, comparability, and outcome, further divided into 2-4 separately graded subdomains. The overall score is determined as good, fair, or poor based on the section sub-scores. 32 In the adequacy of the follow-up subdomain of NOS, the threshold for low risk of bias grading was set to a minimum of 80% of the baseline population followed up, or if more than 20% was missing, a detailed reporting of characteristics of those patients.
Two reviewers conducted the bias assessment phase, with disagreements resolved through discussion, or involvement of a third reviewer. Graphic representations of the assessments were created using the RevMan 5.4 software 33 for randomized studies, or the robvis tool 34 for non-randomized studies.
The quality of the results was assessed through the application of the GRADE approach 35 and presented the results in a table format, using the GRADEpro GDT software. 36
Summary Measures and Planned Methods of Analysis
Statistical analysis
Meta-analysis was performed with the RevMan 5.4 software, 33 pooling compatible studies reporting PROMs as continuous variables. The data were presented as pooled standardized mean differences (psmd) with 95% confidence intervals (CIs). Within-scale differences were handled by standardizing reported mean differences.
A random effects model with inverse variance weighted average was used. Heterogeneity between studies was examined with the I2 statistic, describing the ratio of variance in the true effects to the total observed variance. 37 When multiple interventional groups were present,38-40 single interventional groups were created by pooling patient data and calculating combined means and standard deviations (SDs) for every intervention group.
When multiple studies reported results from the same cohort, only one study using a single outcome measure in a designated timeframe was used. The process was performed according to the criteria and recommendations of the Cochrane Handbook for Systematic Review of Interventions. 25
Inter-rater agreement of bias assessment was analyzed with the Kappa score and was interpreted on a range from no agreement to almost perfect agreement according to recommended guidelines. 41
Results
Study Selection
Our main search identified 2411 studies, and manual search another 8. Among the 120 initially relevant studies, 21 were included in the SR, while 6 were used for meta-analyses. The complete selection procedure, with detailed reasons for exclusion, is presented in
The PRISMA flow diagram represents the search and selection procedure applied during the literature review.
Study Characteristics
All 21 studies were published in English. Among them were 15 “registry based” or “prognostic (prospective) cohort” studies39,40,42-54; 2 “interventional non-randomized”55,56; 1 “interventional randomized”
57
; 1 “prospective (observational) comparative”
58
; 1 “exploratory”
59
; and 1 “natural history”
38
study. A complete overview of the study characteristics is presented in
Study and Patient Characteristics.
Study and Patient Characteristics.
Primary Outcomes
Of 21 included studies, 14 compared PROMs in patients with and without cartilage lesions, from 6 months to 8 years after ACL reconstruction.38-40,42,43,45-47,51,53,55-57,59 A total of 14,311 individuals (46.9% females, 9-69 years old at baseline) were enrolled, with 9,123 reported lesions. Most studies reported cartilage lesions independently of grade39,43,46,47 while others only reported full-thickness (at least Grade 3 or higher) lesions 59 according to Outerbridge38,55 or International Cartilage Repair Society classification (ICRS).56,57 One prognostic study 42 reported Outerbridge Grade 2 or higher lesions, but not Grade 1 lesions. Cartilage lesions treatment varied between studies: from surgically untreated38,39,43,57 to microfracture,43,55,57 chondroplasty (debridement),43,57 abrasion arthroplasty, 43 mosaicplasty, 43 drilling, 55 and Osteochondral Autologous Transplantation Surgery (OATS).56,57
Quantitative Analysis of Primary Outcomes
Six studies with 8,789 patients (38% with CFCLs) were eligible for quantitative analysis. We obtained data from a range of different outcome assessment systems.
Cumulative short- and medium-term follow-up
As our primary objective: In the cumulative short- to midterm, regardless of grading, cartilage lesions were associated with worse PROMS (

Cumulative short- to medium-term PROMs.

Cumulative short- to medium-term PROMs (full-thickness cartilage lesions only).
Short-term follow-up (6-36 months)
Concerning short-term follow-up,39,55,56 there is some evidence associating cartilage lesions with worse PROMS, but with high heterogeneity, and no statistical significance (

Short-term PROMs.

Short-term PROMs (full-thickness cartilage lesions only).
Medium-term follow-up (3-8 years)
At midterm follow-up,38,40,59 cartilage lesions predicted worse PROMs regardless of grading (

Medium-term PROMs.

Medium-term PROMs (full-thickness cartilage lesions only).
Qualitative Description
Primary Outcomes (PROMs)
For the remaining 8 studies42,43,45-47,51,53,57 investigating PROMS that could not be included into the quantitative analyses, a detailed narrative summary of results was performed.
Three studies43,45,51 were performed on the Multicenter Orthopedic Outcomes Network (MOON) cohort. Jones et al. 45 with 1,308 patients found a significant negative impact of medial femoral condyle (MFC), lateral femoral condyle (LFC), and medial tibial plateau (MTP) full-thickness (Grade 3 or 4) cartilage lesions on 6-year IKDC scores. Full-thickness cartilage lesions in the MFC, trochlea, and MTP had a significant negative impact on the 6-year KOOS pain scores. Grade 2 MFC lesions predicted higher KOOS pain scores than Grade 1 lesions in these compartments. MFC, LFC, and MTP high-grade lesions were significant negative predictors of 6-year KOOS Qol score. Cox et al. 43 also found a significant negative impact of high-grade lesions of LFC and MTP on KOOS symptoms score, trochlear lesions on KOOS ADL score, and MTP high-grade lesions on KOOS sport/rec and IKDC scores. As in Jones et al. 45 a significant negative effect of Grade 4 MFC lesions on the Marx activity score at 6-year follow-up was observed, which contradicts the findings in Dunn et al. 51 (393 patients), where no significant associations between location and the grading of cartilage lesions and the 2-year Marx scores were reported.
Spindler et al. 42 found a significant negative correlation (p < 0.001) between the presence of MTP chondromalacia and 5-year KOOS pain score, while other PROMs were not significantly affected by location or degree of cartilage lesion.
One prospective cohort study 47 across 201 subjects reported the degree of patient satisfaction at a mean follow-up of 35.9 months. No statistically significant associations were found between the primary outcome scores and cartilage lesions, regardless of grading.
In a study by Barenius et al. 53 cartilage lesions at the time of ACL reconstruction were significantly associated with a decreased likelihood (RR=0.80, OR=0.76) of functional recovery at 2-year mean follow-up.
In a study by Gudas et al. 57 containing 136 patients at baseline, with a mean follow-up of 3 years, 34 patients with isolated ACL reconstruction reported significantly better IKDC subjective scores compared with the groups of patients with concomitant full-thickness cartilage lesions treated with either microfracture, debridement, or OATS. A significant difference was also observed in the median Tegner scores, favoring the isolated ACL reconstruction group over both microfracture and debridement groups.
Finally, in a study by McAllister et al. 46 of 55 patients followed for a mean of 3.6 years, patellofemoral and MFC cartilage lesions were predictors of both lower physical function and physical assessment domain scores of SF-36 test, with MFC cartilage lesions also predicting inferior bodily pain assessment scores. Moreover, the grading of cartilage lesions was associated with the negative effect size of the outcome.
Secondary Outcomes
Seven studies38,44,45,48-50,56 examined the effect of cartilage lesions on objective outcome measures other than PROMs, in ACL-reconstructed patients at short- to midterm follow-up.
Post-operative OA assessment
Four studies38,45,49,50 across 511 patients, performed radiographic OA assessments. Two studies found no significant correlation between cartilage lesions and radiographic signs of OA, that is, MFC and LFC cartilage lesions were not associated with worse 6-year IKDC radiographic scores, 38 and MFC cartilage lesions were not related to narrowing of the medial compartment joint space in a nested cohort of 262 patients from the MOON cohort at 2-3-year follow-up. 45 A prognostic study by Keays et al., 49 on 56 patients with 6-year follow-up, determined increased grading of full-thickness cartilage lesions with subchondral bone involvement to be a significant risk factor for both patellofemoral and tibiofemoral OA development. However, Ulstein et al. 50 reached the opposite conclusions after following 41 patients for a median of 8.2 years; in the OA assessment, using the Kellgren Lawrence scale, Grade 2 or higher OA was significantly more frequent in patients without a cartilage lesion with those with (21/22 vs. 12/19).
Reoperation rates
Four studies examined reoperation rates.44,48,50,56 Since two of them44,50 used the same Norwegian Knee Ligament Registry (NKLR) subcohort, and the third, and largest one 48 did not report the number of patients at follow-up, the total number of patients is hard to estimate. In Gaweda et al. 56 only 2 reoperations were reported after 6 months among 32 patients without cartilage lesions, compared with none among 21 patients with cartilage lesions. In another short-term (mean 2.1 years) follow-up study by Røtterud et al. 44 the reported reoperation rates were low and similar in the two groups: 6/50 (12%) without cartilage lesions, and 5/30 (17%) with. At long term (mean 8.4 years) in the same cohort, the reoperation rates remained balanced but increased to 22% and 24%. 50 In a large cohort of 13,102 patients, those who received a hamstring tendon (HT) autograft were significantly less likely to receive revision ACL-surgery within 2 years when cartilage lesions were present. 48 In contrast, more patients who received bone-patellar tendon-bone (BPTB) autograft underwent ACL revision surgery if a cartilage lesion was present at index surgery, but the difference was not statistically significant.
Comparison of surgical treatments
Outcome measures from 4 studies with altogether 518 patients treated with different surgical approaches were reported.52,54,57,58; 147 patients received microfracture,52,54,57,58 112 surgical debridement,52,54,57; 34 OATS, 57 ; 25 radiofrequency ablation 58 and the rest no surgical treament.52,54,58 In the short term (2.1 years), microfracture significantly predicted worse KOOS scores (KOOS Sport/rec and KOOS QoL) compared with no treatment, while differences between debridement and no treatment on all KOOS subscales were not significant. 52 In the medium term (5.1 years), KOOS subscale scores did not significantly differ between microfracture, debridement, or no treatment in the same subcohort of Swedish and Norwegian KLR 2005-2008 cohort. 54 One prospective comparative study 58 reported no difference in PROMs in patients treated with microfracture (n= 25), compared with radiofrequency ablation (n= 25) at 2-year follow-up, while mean Tegner scores favored radiofrequency ablation group at 5-year follow-up. A randomized study 57 reported no difference between the mean subjective IKDC scores and the median Tegner scores for patients treated with debridement (n=34) and microfracture (n=34) at 3-year follow-up, with both treatment groups reporting significantly worse scores compared with OATS (n=34).
Risk of bias within studies
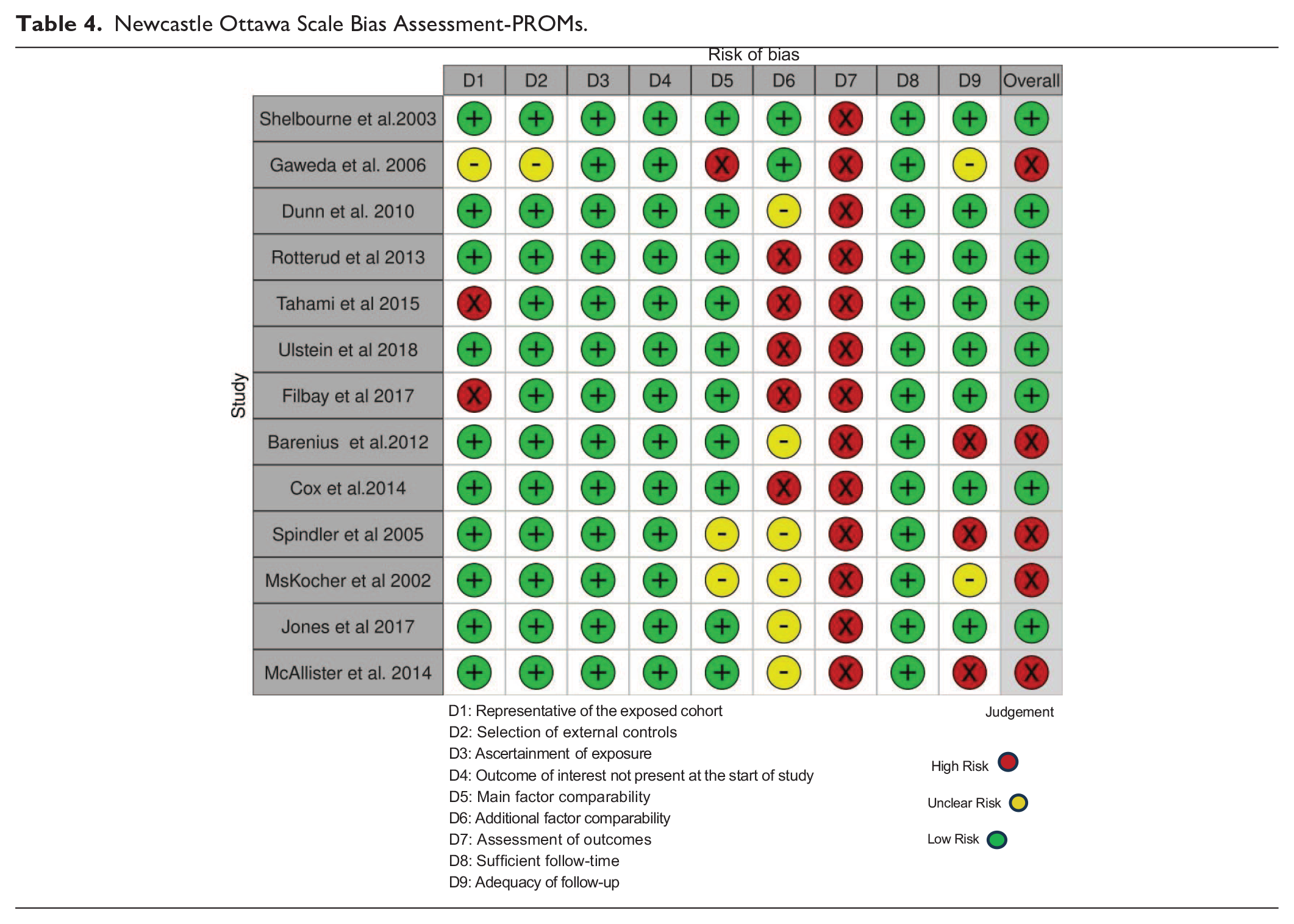
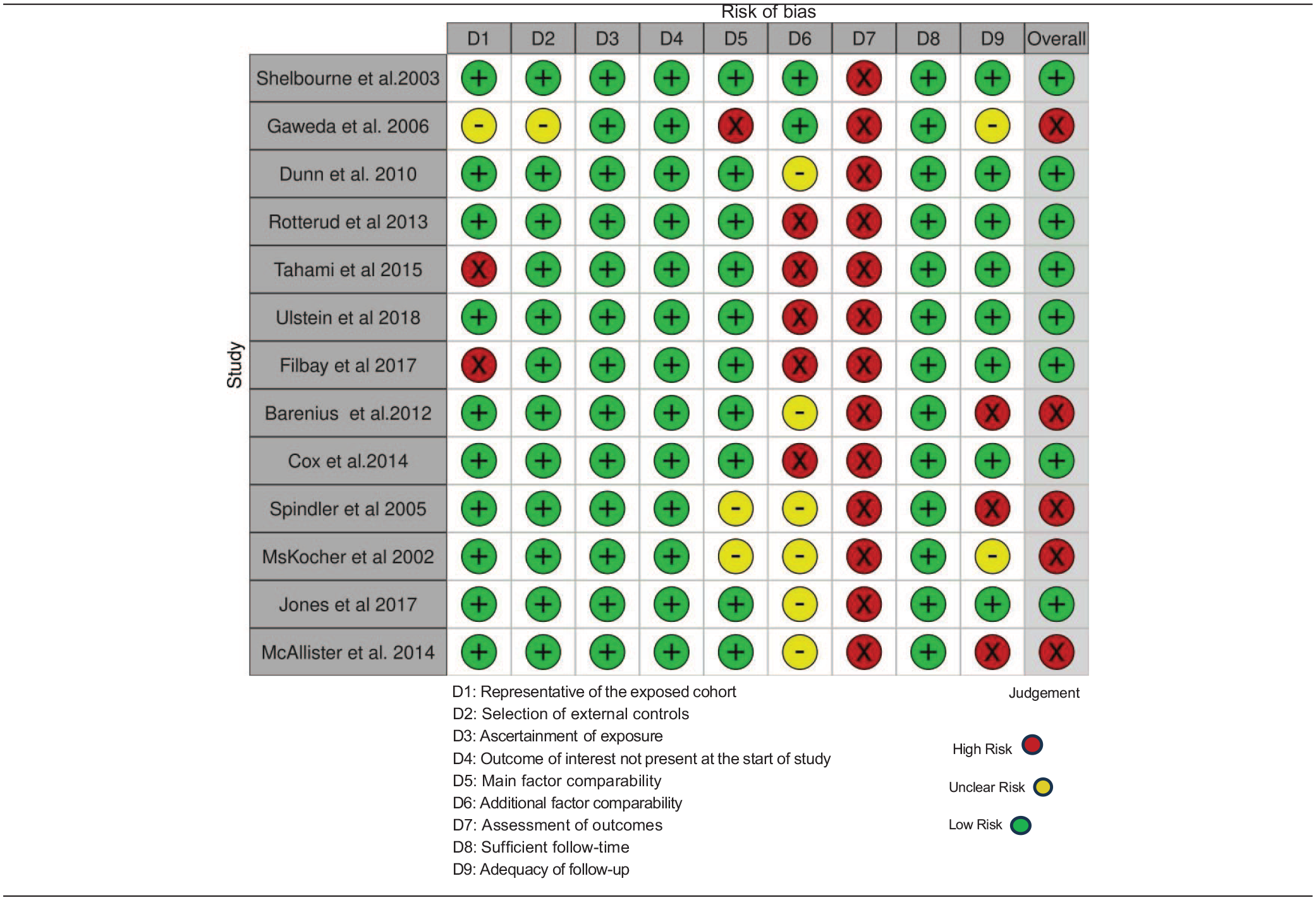
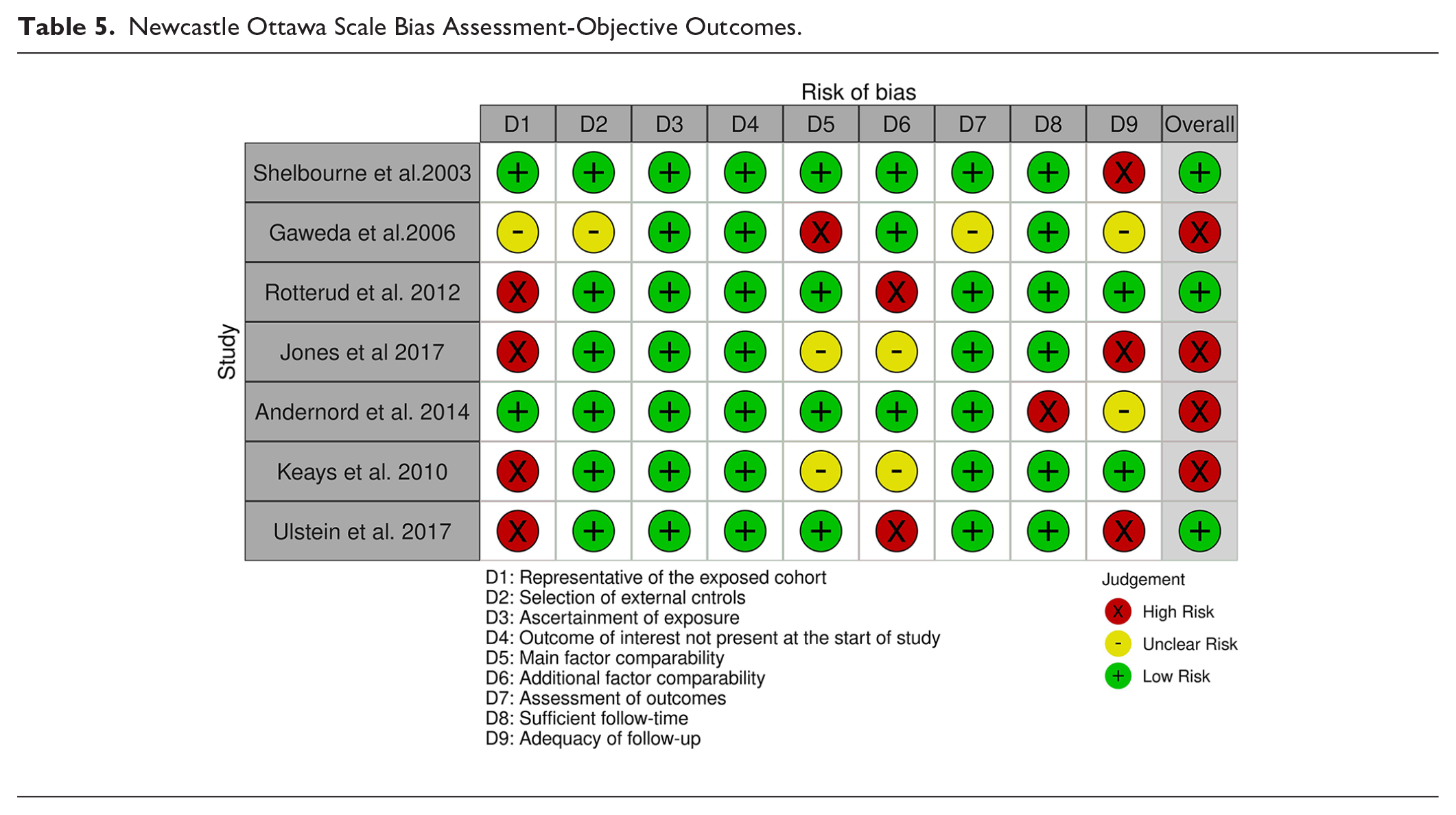
All included studies except Gudas et al. 57 were non-randomized in design, and assessed for bias using the NOS. Of 13 studies reporting PROMS, 8 were graded as low38,39,40,43,45,51,55,59 and 5 as high risk of bias,42,46,47,53,56 the most common reasons being the usage of subjective outcome assessments (all studies), low rate of follow-up42,46,53 and underreporting of adjustment factors other than age and gender.39,40,42,43,45-47,51,53,55,59 (Table 4). In 7 studies examining secondary outcomes, 4 were rated as high45,48,49,56 and 3 as low risk of bias (Table 5).38,44,50
Newcastle Ottawa Scale Bias Assessment-PROMs.
Newcastle Ottawa Scale Bias Assessment-Objective Outcomes.

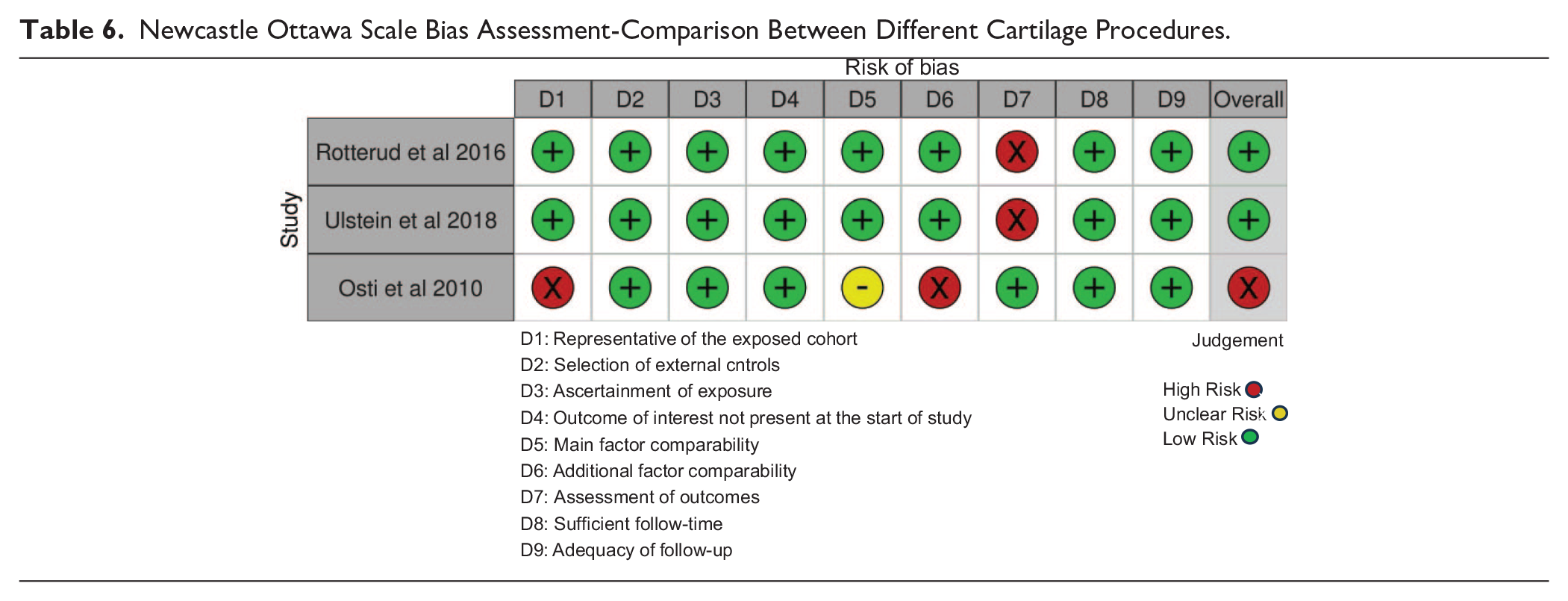
In 2 out of 3 studies comparing different cartilage procedures, the risk of bias was graded as low52,54 and in 1 it was rated as high 58 due to the inability to adjust for size and depth of the cartilage lesions (Table 6). Gudas et al. 57 study was graded according to the Cochrane risk-of-bias tool for randomized trials, 26 faring poorly in the sections of sequence generation, allocation concealment, blinding of participants and personnel and selective outcome reporting, due to lack of information provided in the study ( Table 7 ).
Newcastle Ottawa Scale Bias Assessment-Comparison Between Different Cartilage Procedures.
Cochrane Risk of Bias Tool Bias Assessment—Randomized Study Designs.
The degree of inter-rater agreement was strong (Kappa=0.843) and moderate (Kappa=0.719) for studies reporting primary and secondary outcomes, respectively.
Discussion
Primary outcomes
The most important finding of the present study, estimated with moderate uncertainty on the available level 1 and 2 evidence data, was that high-grade cartilage lesions in ACL-reconstructed patients are associated with worse cumulative short- to midterm PROMS. Our estimates from a similar analysis, performed separately for short- and midterm follow-up data, were of high uncertainty. Additionally, we concluded with a very high degree of uncertainty, that cartilage lesions in ACL-reconstructed patients are associated with worse short-, mid-, and cumulative short- to midterm PROMS, regardless of lesion depth (Table 8).
GRADE Summary of Findings Table.
CI = confidence interval.
High heterogeneity across studies (I2=65%, P=0.02). Point estimates of all studies indicate a negative effect; however, the upper limit of 95% CI of 4/5 studies is very close to 0 (≥ to −0.05), with 95% CI of one study among them containing 0.
Impossible to evaluate publication bias due to a low number of studies (<10) compromising the body of evidence for each outcome. More information about publication bias is present in “Limitations” part of the “Discussion” section.
Magnitude of effect expressed in SMD (Cohen’s d) value is in range of −0.30 to −0.50 units, which we classified as the medium size effect.
A slight increase in the negative magnitude of the effect would be present if adjusted versus unadjusted values were used, based on one high-weight study. Additionally, in most studies (80% weight), the mean difference between groups before standardization was between 5% and 10%, which is moderate.
Almost 30% of the overall weight used to calculate pooled effect estimate is contributed by Gaweda et al. study, graded as high bias in the adequacy of follow-up and overall domains. However, the same MA performed without biased study does not yield very different effect estimate, heterogeneity nor does it make the result statistically significant.
Very high heterogeneity across studies (I2=73%, P=0.03). All point estimates indicate a negative effect; however, the upper limit of 95% CI of 2/3 studies (70% weight) is very close to 0 (≥–0.05).
Optimum information size (OIS) calculation (assuming an alpha of 0.05 and a beta of 0.20) indicates a satisfactory number of participants to derive reliable conclusions. However, the 95% CI of the pooled effect estimate contains a value of 0 and is not statistically significant.
Almost 30% of overall weight used to calculate pooled effect estimate is contributed by Gaweda et al. study, graded as high bias in the adequacy of follow-up and overall domains. The same MA performed without a biased study yields less negative effect estimate (–0.45 vs. –0.35 SMD) and lower heterogeneity (I2 54% vs. 45%) and makes the result statistically insignificant. However, reformed MA is based on only 2 studies.
High heterogeneity across studies (Isq=54%, P=0.11). Point estimates of all studies indicate a negative effect, with 2/3 studies (80%+ weight) having an upper limit of 95% CI far from the value of 0 (≤ –0.14), with 95% CI of the third study (<20% weight) not containing 0.
High heterogeneity across studies (I2=55%, P=0.11). All point estimates indicate a negative effect, with an upper limit of 95% CI of 3/3 studies very close to 0 (≥ –0.05), with 95% CI of one study among them containing 0.
OIS calculation (assuming an alpha of 0.05 and a beta of 0.20) a indicates satisfactory number of participants to derive reliable conclusions. However, the upper border of 95% CI of the pooled effect estimate is 0, and the p value of the overall effect is = 0.05.
Three studies graded as high biased, and one as low biased overall.
Two studies found no statistically significant correlation between the presence of concomitant cartilage lesion and OA development in ACL-reconstructed patients at short to midterm. However, one study found a negative correlation and another positive correlation between the two, both being statistically significant.
One study with neutral results compares OA rates in ACL-reconstructed patients with concomitant cartilage lesion to OA rates indirectly—in contralateral, uninjured knees.
OIS calculation (assuming an alpha of 0.05 and a beta of 0.20) indicates an unsatisfactory number of participants to derive reliable conclusions. Results did not reach statistical significance in 2/4 studies. No information about the significance of the pooled effect estimate.
One out of 3 studies included was graded as highly biased, while the other two were performed over the same cohort from NRLK, effectively counted as a single study.
Impossible to correctly identify both the number of patients and the statistical significance of results.
Not applicable—Heterogeneity is not accessed due to the pooled number of studies being equal to 1.
Study results are statistically significant, with 95% CI not containing zero. However, OIS calculation (assuming an alpha of 0.05 and a beta of 0.20) indicates an unsatisfactory number of participants to derive reliable conclusions.
In majority of studies, the mean difference between microfracture and comparator groups is 5%-10% on the respective scale used to measure outcome AND adjusted analysis is statistically significant.
Pooled results of all studies are not statistically significant, with 95% CI of pooled effect containing zero.
Two out of 3 studies (151/215 patients) rated as high bias, with the remaining one rated as low bias.
In one study, microfracture is indirectly compared with the debridement procedure through no treatment group.
In 1 of 3 studies, the mean difference between microfracture and comparator groups is between 5% and 10%, while in the remaining 2 studies, it is less than 5% on the respective scale used to measure outcome. However, a study with a moderate effect size contributes to the highest number of patients (>50%) and its adjusted analysis is statistically significant.
In 1 study, microfracture group patients suffer from high-grade lesions (Gr 3 or 4) while radiofrequency ablation patients suffer from partial thickness lesions (Grade 1 or 2).
One study reporting a nonsignificant difference between MF and debridement at midterm, while another reports significantly worse results of MF versus radiofrequency ablation.
One study reports a statistically significant difference between microfracture and radiofrequency ablation group, and other insignificant difference between microfracture and debridement.
Our conclusions are supported by the SR performed by Pedersen et al., 23 which reported a correlation between cartilage lesions and worse PROMS at 2-10 years follow-up after ACL reconstruction in 31,556 subjects across 4 studies. Hamrin Senorski et al. 24 also concluded that the absence of a cartilage lesion at the time of ACL reconstruction significantly increased the odds of reporting an 80th percentile result in the KOOS 4 score at 2-year follow-up. Cartilage lesion’s thickness was associated with worse KOOS scores, suggesting a relationship between the lesion thickness and PROMs. However, the similarity to Pedersen et al. is not surprising, considering the substantial overlap of study cohorts in both reviews.
Results were mixed in Magnussen et al. 22 While Hanypsiak et al. 18 and Lebel et al. 19 reported no significant differences in subjective IKDC scores, Shelbourne and Gray 60 identified articular cartilage lesion as a predictor of lower Cincinnati and subjective IKDC scores in ACL-reconstructed patients. However, the minimum follow-up time for all studies in Magnussen et al. was 10 years, and one of them 18 involved patients with bone bruising at baseline.
In Fillardo et al., 21 of 27 included studies, 21 indicated worse short- to midterm subjective, objective, or radiological outcomes if a cartilage lesion was present.
Conflicting results were reported in 2 NLKR cohort studies40,50: where the smaller study 50 (n=74) found no association between full-thickness cartilage lesions and KOOS subscale scores at 5-9 year follow-up, in contrast to the larger study 40 (n=6,785). This may result from the inter-study patient characteristics, with the first 50 using stricter inclusion criteria than the second. 40 A younger population with higher baseline PROMs implies a more physically active cohort, plausibly with higher self-motivation and increased rehabilitation adherence.61-63 Another reason might be shorter injury to surgery interval between cohorts.64,65
Large prospective cohort studies by Rotterud 39 and Ulstein 40 received high relative weight in the meta-analysis models. However, considering their methodological rigor, sample size, and low bias risk, we concluded that omitting those studies would be ill-advised.
For two studies39,40 included in the meta-analysis, pooled crude mean KOOS QoL scores were used instead of adjusted beta coefficients, due to the intervention group structure. Adjusted and unadjusted beta coefficients were similar for partial thickness and indicated the same conclusions in the full-thickness group, which was considered during the GRADE evaluation. Consequently, we conclude that representative results are reported here.
The main limitation of the current meta-analysis is the heterogeneity in PROMs pooled across the included studies, due to limitations of the evidence base. 66 However, all included PROMS examined similar general components of knee function, with the only exception being KOOS. Therefore, only KOOS Qol subscale scores were considered as best fit for analysis.67,68 Consequently, the presented analyses reflect knee function in a broader sense across multiple evaluation systems, making it difficult to give specific practical recommendations to patients with different activity levels and knee function demands. 68
Meta-analysis comparing PROMs between patients with partial and full-thickness lesions was not performed, due to limited available evidence. However, due to frequent issues with misclassification, it is questionable whether studies focused solely on ACL-reconstructed patients with partial thickness lesions should be encouraged at all.69-73
A high number of studies did not report concomitant cartilage treatments,39,42,46,47,59 suggesting the interpretation that most lesions were untreated.
Secondary Outcomes
We observed, with a very high degree of uncertainty, an association between cartilage lesions and both OA development and reoperation rates, in the cumulative short- and midterm (Table 8).
Conflicting results across studies may stem from the inclusion criteria, especially in regard to baseline meniscal status as a known OA predictor in the long term.74,75 All 3 studies38,45,50 that did not observe a correlation between cartilage lesions and OA development also excluded patients with meniscal lesions, unlike one study 49 that reached the opposite conclusion. In Grassi et al., 76 both cartilage lesions and meniscal lesions were identified as independent predictors of OA development in ACL-reconstructed patients. The minimum follow-up was 20 years: since the time from surgery is critical in the pathophysiological process of OA development, we consider their study design to be more appropriate than short-term evaluations.
Optimal surgical cartilage lesion treatment
From the available short-term data, with high uncertainty, we observed an association between the microfracture procedure and worse PROMs compared with no treatment, and no association at midterm, with the limitation that both results used the same cohort of patients. The microfracture procedure was also associated with worse PROMs compared with OATS at short term, and radiofrequency ablation at midterm (Table 8).
One study 58 compared PROMS in 25 ACL-reconstructed patients with full-thickness cartilage lesions treated with microfracture to 25 ACL-reconstructed patients with partial thickness cartilage lesions treated with radiofrequency ablation, attributing the differences solely to the surgical procedure, without adjusting for lesion depth as a confounder.
Another limitation was the lack of level 1 or 2 studies examining outcomes in ACL- reconstructed patients treated with novel cartilage reparation procedures (matrix-induced autologous chondrocyte implantation [MACI], scaffold- based procedures, etc.). 77
The exact number of lesions is potentially underestimated due to: reporting only the single, highest grade lesion per patient,38,39,48,55,59 grouping lesions together into compartmental chondrosis,42,43,46,47 and unclear terminology concerning the articular cartilage injury (chondromalacia, chondrosis and focal lesions used interchangeably).43,45-47,49,51
Due to the small number of available studies, publication bias was not evaluated with funnel plots: some factors present suggest an increased risk of publication bias 78 (only 1 randomized control trial [RCT], mostly observational cohort studies) or a decreased risk (large studies with rigorous methodology, no evidence of premature stopping, not a new research topic, no industry-sponsored studies).
Most studies could have described the covariate adjustment in regression analyses more precisely. There is no reasoning presented as to why certain factors are considered confounders, with no distinction between confounders, colliders, and mediators, which would be necessary for precise causal interpretations. Directed acyclic graphs (DAGs) were not created, increasing the risk of bias and preventing repeated analysis in further studies.79-82
The results from our study might facilitate realistic expectations following ACL reconstruction in patients with concomitant cartilage lesions, both for patients and surgeons. Finally, based on the limited body of evidence, avoiding microfracture procedures for the treatment of cartilage lesions might be advisory, considering no proven benefit compared with other, less invasive procedures.
Conclusions
In conclusion, high-grade cartilage lesions in ACL reconstruction result in predictably worse PROMS in the short to midterm, while the same might be true regardless of the grading of the cartilage lesions. It is uncertain whether the presence of a cartilage lesion in ACL-reconstructed patients leads to knee joint OA within the relatively short time to follow-up in this SR (up to 8 years), with factors such as meniscal status potentially being decisive. Due to the scarcity of high-quality evidence, further pragmatic (RCT) studies are necessary to enable conclusions about the optimal treatment of cartilage lesions in ACL-reconstructed patients.
Footnotes
Acknowledgements and Funding
Skjalg Tønnessen Kalvik—UiO senior medical librarian contributed to the process of conducting an initial medical database search and removal of duplicates. The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The University of Oslo provided help from the librarian in the process of conducting an initial medical database search and removal of duplicates. Funders did not influence the selection of study design, analysis, interpretation of data, manuscript writing, or the publication process. They are not responsible for the content, conclusions, and recommendations given in this systematic review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This meta-analysis synthesizes data from previously published studies, all of which obtained ethical approval, and involves no new data collection or direct interaction with human or animal participants.