
Abstract
Objective
To determine (1) if bone bruise characteristics seen on magnetic resonance imaging are associated with patient-reported outcomes prior to and following anterior cruciate ligament reconstruction and (2) if the combined presence of bone bruises with articular cartilage pathology results in inferior 2- or 6-year outcomes.
Design
Bone bruise volume and severity were measured on 81 patients’ preoperative magnetic resonance imaging in the medial and lateral femoral condyle (MFC, LFC) and medial and lateral tibial plateau (MTP, LTP) using the Costa-Paz classification and a modified version of Roemer and Bohndorf’s technique. The relationships between bone bruise volume and severity with Knee Injury and Osteoarthritis Outcome Score (KOOS) and International Knee Documentation Committee (IKDC) scores were assessed, and pre- and postoperative KOOS and IKDC scores were compared between those with bone bruises either with or without combined local articular cartilage pathology.
Results
All 81 patients had a bone bruise in at least 1 region and 70 (86%) had bone bruises in ≥2 regions. LTP bruises were the most common (76/81, 94%), followed by the LFC (66, 81%), MTP (46, 57%), and MFC (20, 25%). Neither bone bruise volume nor severity was associated with inferior postoperative outcomes. The subset of 17 patients with bone bruises and combined articular cartilage pathology were 3.4 times more likely to be symptomatic at 6-year follow-up than those without articular cartilage pathology (P = 0.04).
Conclusions
The volume and severity of preoperative bone bruises alone were not associated with 2- or 6-year outcomes; however, bone bruises combined with local articular cartilage pathology appear to be more symptomatic after ACL reconstruction.
Keywords
Introduction
Despite overall favorable outcomes reported after anterior cruciate ligament (ACL) reconstruction, there is a high percentage of young adults with established posttraumatic osteoarthritis (PTOA) of the knee 10 to 20 years after ACL injury. This percentage has been estimated to be between 40% and 50%, with early, irreversible radiographic changes presenting as early as 2 to 5 years after the initial injury. 1 In one study, the long-term outcome following ACL reconstruction indicated that greater than 75% of affected athletes experienced significant daily symptoms and 42% had radiographically documented symptomatic OA; the average age of symptomatic patients in this study was 32 for females and 38 for males (thus between 12 and 14 years after their athletic career finished). 1 The importance of this is highlighted by the fact that ACL injuries in patients under 18 years of age are dramatically rising. 2
Damage to articular cartilage is a known accelerator of OA, and while the majority of patients who suffer an ACL tear will have significant subchondral bone edema (suggesting injury to the overlying cartilage), they often will not present with macroscopic cartilage damage at the time of ACL reconstruction. Subchondral bone edema, which has been interchangeably termed a “bone marrow lesion” or “bone bruise,” is the result of a violent contusion of the femur onto the tibia during the mechanism leading to an ACL injury. It has been suggested that the resulting bone bruises may be associated with the development of articular changes. Adachi et al. 3 and Costa-Paz et al. 4 reported that patients with areas of a severe (Grade 3) bone bruise developed cartilage lesions, confirmed by magnetic resonance imaging (MRI), as early as 1 year after injury. Similarly, Potter et al. 5 suggested that the incidence and volume of a bone bruise at the time of surgery was associated with cartilage lesions in affected and unaffected areas at 2, 5, and 7 years postinjury. 5 Specifically, the authors reported that the region with the greatest risk of cartilage loss was the lateral femoral condyle, with a 50-fold increase in the risk of cartilage loss 5 to 7 years after ACL injury. However, long-term follow-up studies looking at the mere incidence of bone bruises have not shown a direct correlation of bone bruising to the development of PTOA.6-10
While there is some disagreement in the literature as to the association between the presence of bone bruises and the development of PTOA, the presence of preoperative bone bruises has not been found to be associated with inferior patient-reported outcomes 2 years after ACL reconstruction. 11 Given that the location and severity of bone bruises are highly variable between patients, it remains unclear if the volume or severity of these lesions may in fact be a predictor of worse clinical outcomes. It also remains unclear if patients with bone bruises and combined articular changes are at greater risk of persistent pain and/or reduced function. The purposes of this study were then to determine (1) if preoperative bone bruise volume and severity correlate with patient-reported outcomes either prior to or following ACL reconstruction and (2) if the combined presence of bone bruises with articular cartilage pathology at the time of surgery results in either inferior patient-reported outcomes or a greater prevalence of symptomatic knees during the first 6 years after ACL reconstruction when compared with patients with only isolated bone bruises.
Methods
Patients
Patients with primary ACL injuries enrolled over a 2-year period from a single site (N = 121) that had consented to be a part of an institutional review board–approved prospective longitudinal cohort were evaluated for inclusion into the current study. Patients were included in the current analysis if they had a complete ACL tear, no collateral or posterior cruciate ligament injury, a preoperative MRI meeting basic standard requirements (T2 or PD sequences in the coronal and sagittal plane and a slice thickness ≤5 mm), underwent a primary ACL reconstruction, with both 2- and 6- year follow-up. Out of the original 121 patients in the overall cohort, 81 patients were identified that met the study criteria.
Patient-Reported Outcome Measures
Patients completed Knee Injury and Osteoarthritis Outcome Score (KOOS) and International Knee Documentation Committee (IKDC) questionnaires prior to and at 2 and 6 years following ACL reconstruction. We employed the operational definition of a symptomatic knee based on the 5 KOOS subcomponents first developed by Englund et al. 12 A knee was considered symptomatic if at least 50% of the responses to the questions used to calculate the KOOS Knee-related Quality of Life (KRQOL) subscale were less than the best possible response and the KOOS KRQOL subcomponent score was ≤87.5, provided that similar criteria were met for at least 2 of the remaining 4 KOOS subcomponents (at least 50% of each subscale responses were less than the best possible response with subcomponent scores below the following thresholds: Pain ≤86.1, Symptoms ≤85.7, Activities of Daily Living (ADL) ≤86.8, Sports and Recreation (Sport) ≤85.0. 12
Intraoperative Data
Surgeons completed a custom questionnaire documenting history of injury and previous surgeries, general exam findings under anesthesia, intra-articular injuries to meniscus and cartilage, and surgical technique. Knee exam findings were documented according to the updated 1999 IKDC guidelines. Articular cartilage injuries were classified according to the modified Outerbridge classification. 13 Consistent with Potter et al., Outerbridge grades ≥2 were considered to be representative of clinically meaningful changes to the articular cartilage. 5
Bone Bruise Severity and Volume
A minimum of sagittal and coronal sections imaged according to a T1 and a T2 weighted or proton density (PD) protocol as well as axial sections were required to be included in the current study. All MRI exams were uploaded to the site’s picture archiving and communication system (PACS) and subsequently de-identified using the Mac-based OsiriX software (Pixmeo, Bernex, Switzerland) as well as a custom PERL script to remove other identifiers in additional DICOM tag fields. No standardized sequences were utilized. All MRI scans were reviewed, and slice thickness and orientation were documented. MRIs were considered to be adequate for evaluation if they included T2 or PD sequences in the coronal and sagittal plane and a slice thickness of no more than 5 mm.
Bone bruises were graded on each patient’s MRI according to the criteria established by Costa-Paz et al. 4 The Costa-Paz 4 system has the advantage of being a clinical system to grade bone bruise severity that can readily be applied to MRI images without the need for complex DICOM data set evaluations. We analyzed all MRI scans for the Cost-Paz severity according to the authors’ initial description of the scale. The Costa-Paz scale ranges from Type 1 to 3. Diffuse signal with change of medullary component, often reticular and distant from the articular surface, was considered a Type 1 lesion. A Type 2 lesion was defined as localized signal bordering the articular surface. More severe, Type 3 lesions were defined as disruption or depression of the normal contour of the cortical surface, often associated with an articular lesion. 4
The volume of each bone bruise was also measured from the patient’s preoperative MRI. Bone bruise volumes were measured from the T2 or PD weighted coronal images in a modification of Roemer and Bohndorf’s technique. 14 To calculate bone bruise volume, the border of each bone bruise was manually traced within the PACS software on each individual coronal slice in which the bone bruise was visible. The resulting area for the slice was then multiplied by the slice thickness to create the bone bruise volume for that individual slice. This process was repeated for all slices in which the bone bruise was visible, and the volume of the bone bruise was then represented as the sum of the slice volumes. We are aware that this constitutes a rough estimate of the true volume of the bone bruise; however, our intention was to provide an easily clinically applicable approach that can be performed in the office on any MRI without the need of specialty software. Bone bruise volume was measured on each MRI in the medial and lateral femoral condyle (MFC, LFC) and medial and lateral tibial plateau (MTP, LTP), and the total bone bruise volume was the sum of the volumes of bruises present in any of the 4 boney regions.
Statistical Analyses
Statistical analyses were specific to each of the study’s intended purposes. First, the relationships between bone bruise volume and both pre- and postoperative KOOS and IKDC scores were assessed by calculating Pearson product moment correlation coefficients. Historically, correlation coefficients between 0.3 and 0.49 have been considered “moderate,” with those greater than 0.5 considered “large.” 15 For the current study, we then considered potentially clinically meaningful correlations to be those greater than 0.5. Additionally, KOOS subscales and IKDC scores were compared between groups of patients with Type 1, 2, and 3 bone bruises defined using the Costa-Paz criteria to determine the role of bone bruise severity on pre- and postoperative patient-reported outcomes. For this analysis, separate 3 × 3 (group × time) repeated-measures analyses of variance (ANOVA) were used to individually compare each of the 5 KOOS subscales and IKDC scores between groups with varying degrees of bone bruise severity.
Second, to determine if bone bruises with coexisting articular pathology were associated with increased symptoms either prior to or following surgery, pre- and postoperative KOOS and IKDC scores were compared between patients with isolated bone bruises (ISOLATED) and patients with bone bruises with combined Outerbridge grade 2 or greater articular pathology at the time of surgery (COMBINED) using 2 × 3 repeated-measures ANOVA. This process was used for each of the 5 KOOS subscales as well as the IKDC score. The prevalence and risk of symptomatic knees at 6-year follow-up was also compared between the ISOLATED and COMBINED groups using Fisher exact tests and odds ratios, respectively. We also compared the volume of bone bruises between those with and without coexisting articular cartilage pathology using an independent t-test, and the prevalences of medial and lateral meniscal tears were compared between groups using χ2 tests. For all analyses, an α level of P < 0.05 was considered statistically significant, and all analyses were performed with SPSS Statistics 22 (IBM, Armonk, NJ), with the exception of odds ratio calculations, which were performed with MedCalc version 16.1 (MedCalc Software, Ostend, Belgium).
Results
Bone bruises were common, with all 81 (100%) having a bone bruise in at least 1 region and 70 (86%) having bone bruises in ≥2 regions. LTP bruises were the most common (76/81, 94%), followed by the LFC (66, 81%), MTP (46, 57%), and MFC (20, 25%). The prevalence of observed combinations of bone bruises is displayed in Table 1 . There were no clinically meaningful correlations between the total volume of bone bruises or bone bruise volumes of each individual region with any of the 5 KOOS subcomponents or IKDC scores either prior to surgery or 2 or 6 years following ACL reconstruction (r < 0.5 for all comparisons).
Prevalence of Observed Bone Bruise Patterns.
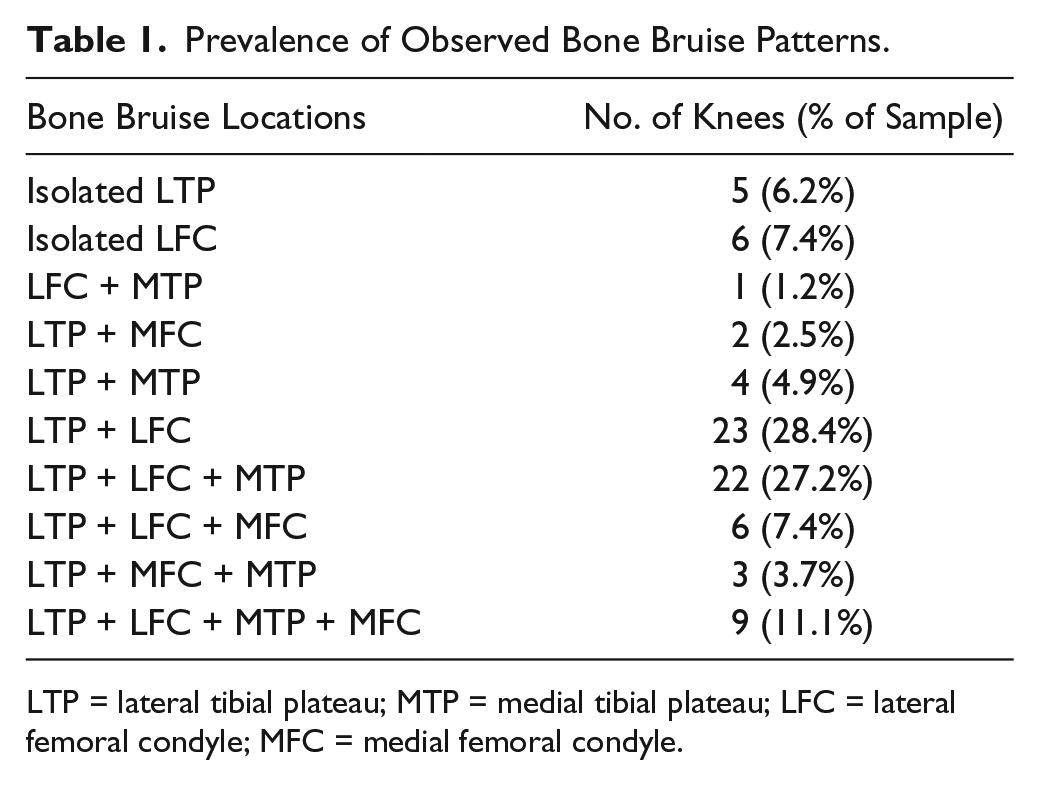
LTP = lateral tibial plateau; MTP = medial tibial plateau; LFC = lateral femoral condyle; MFC = medial femoral condyle.
The Costa-Paz grading system was used to define bone bruise severity in 80 of the 81 patients. Of the 80, 45 (56%) were defined as Type 1, 29 (36%) as Type 2, and 6 (8%) as Type 3. KOOS Symptom (P = 0.80), Pain (P = 0.37), ADL (P = 0.62), Sports (P = 0.91), and Knee-related Quality of Life subscales (P = 0.68), as well as IKDC (P = 0.69) did not differ either prior to, 2 years, or 6 years after ACL reconstruction based on bone bruise severity defined using the Costa-Paz grading system.
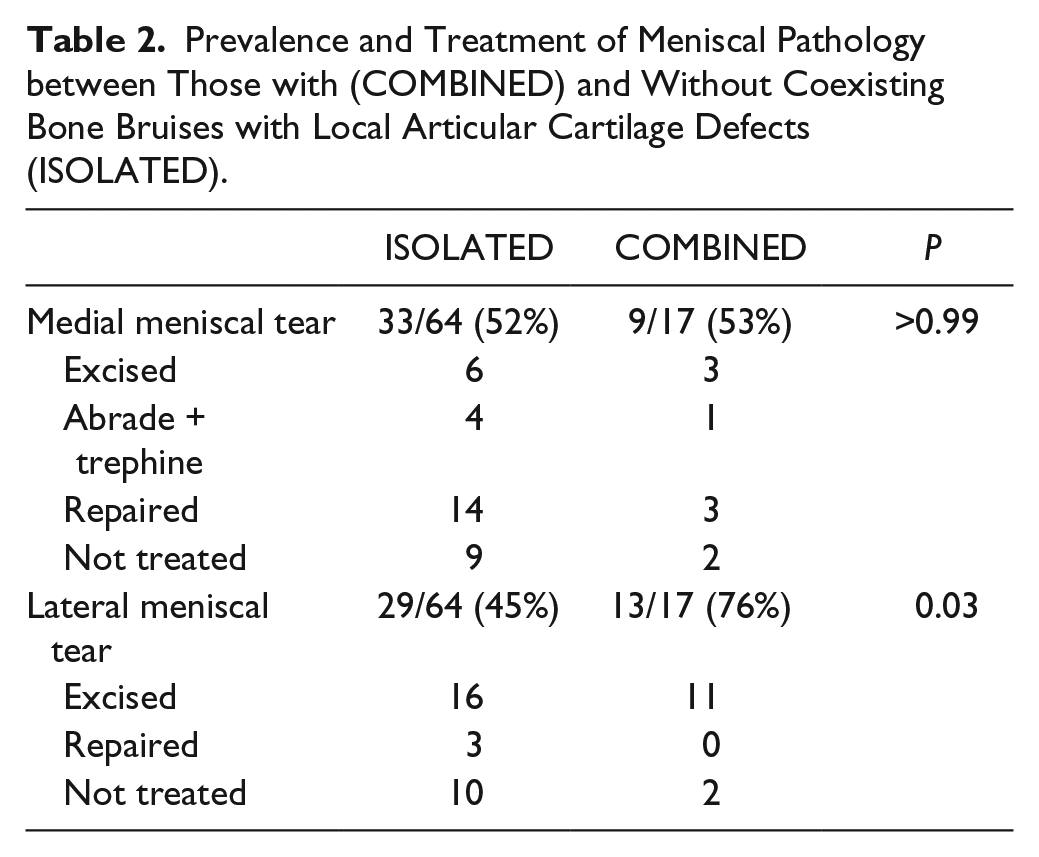
There was a subset of 17 patients with lateral bone bruises and combined articular cartilage pathology at the time of surgery, and this subset was significantly older (ISOLATED = 26.1 ± 12.3 years vs. COMBINED = 33.9 ± 10.7 years, P = 0.02) with significantly greater body mass index at the time of surgery (ISOLATED = 24.3 ± 3.7 kg/m2 vs. COMBINED = 27.8 ± 4.4 kg/m2, P = 0.006). Lateral bone bruise volumes were significantly larger in those patients with combined articular cartilage pathology (ISOLATED = 36.4 ± 43.2 mm3 vs. COMBINED = 61.0 ± 44.2 mm3, P = 0.03). The 2 groups did not differ in the prevalence of medial meniscal pathology; however, lateral meniscus tears were significantly more common in the COMBINED group (P = 0.03; Table 2 ). Regardless of group, as previously reported, all KOOS subcomponents and IKDC scores significantly increased from preoperative data collection to 2 years, and these gains were maintained at 6 years (P < 0.001; Table 3 ). The group with bone bruises and combined articular cartilage pathology had significantly lower KOOS Pain and ADL subcomponent scores both prior to and following surgery ( Table 3 , Fig. 1 ).
Prevalence and Treatment of Meniscal Pathology between Those with (COMBINED) and Without Coexisting Bone Bruises with Local Articular Cartilage Defects (ISOLATED).
Pre- and Postoperative KOOS Subscales and IKDC Scores for Those with Isolated Bone Bruises and Those with Bone Bruises Combined with Articular Changes.
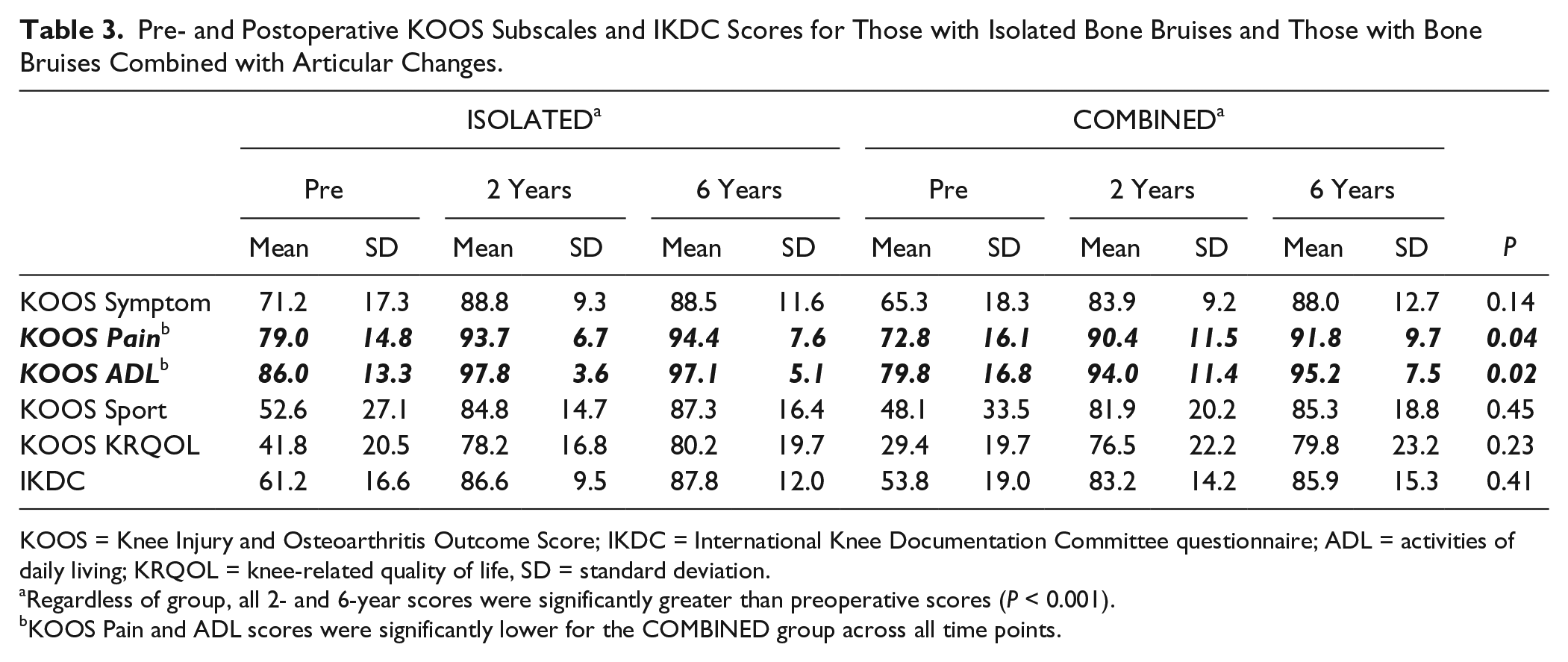
KOOS = Knee Injury and Osteoarthritis Outcome Score; IKDC = International Knee Documentation Committee questionnaire; ADL = activities of daily living; KRQOL = knee-related quality of life, SD = standard deviation.
Regardless of group, all 2- and 6-year scores were significantly greater than preoperative scores (P < 0.001).
KOOS Pain and ADL scores were significantly lower for the COMBINED group across all time points.
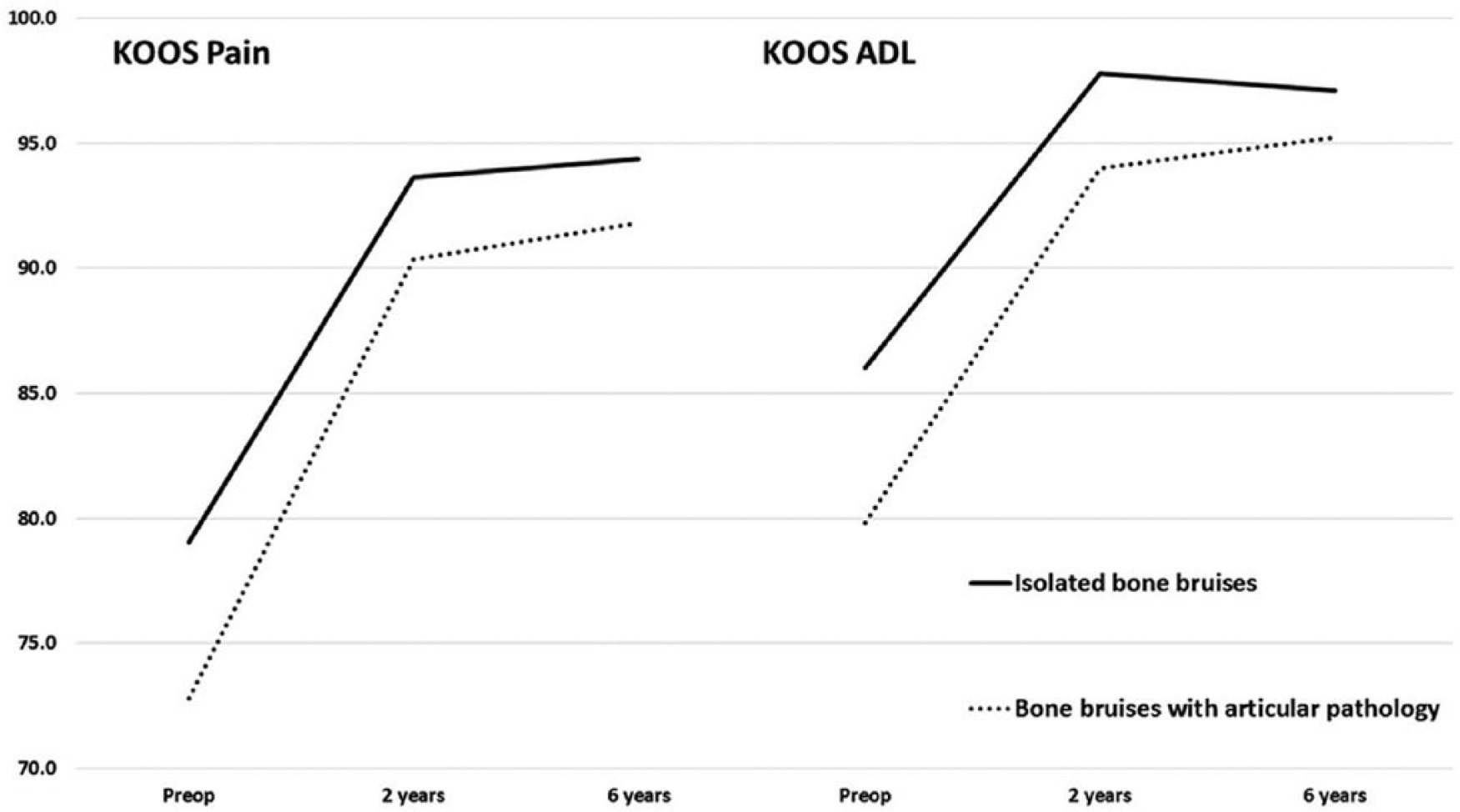
Both prior to and following ACL reconstruction, patients with bone bruises and combined articular cartilage pathology demonstrated significantly lower Knee Injury and Osteoarthritis Outcome Score (KOOS) Pain (P = 0.04) and Activities of Daily Living (ADL; P = 0.02) scored compared to those with isolated bone bruises.
Furthermore, a significantly greater proportion of this group was defined as having symptomatic knees (7/17 [41%] vs. 11/64 [17%], P = 0.049) at 6-year follow-up and were 3.4 times more likely to have a symptomatic knee at 6 years than those without articular cartilage pathology (odds ratio = 3.4; 95% confidence interval = 1.1-10.8; P = 0.04).
Discussion
The purposes of this study were to determine (1) if preoperative bone bruise volume and severity correlate with patient-reported outcomes either prior to or following ACL reconstruction and (2) if the combined presence of bone bruises with articular cartilage pathology at the time of surgery results in either inferior patient-reported outcomes or a greater prevalence of symptomatic knees during the first 6 years after ACL reconstruction when compared to patients with only isolated bone bruises. In this study of a tightly controlled prospective cohort of patients undergoing primary ACL reconstruction, we found bone bruises to be present on preoperative MRI in 100% of patients suffering a complete ACL tear. The distribution of those bone bruises is not uniform, however. The majority of patients have bone bruises in the LTP (76/81, 94%) and LFC (66, 81%), whereas bone bruises occur on the MTP (46, 57%) and MFC (20, 25%) much less frequently. Surprisingly, neither the size of individual bone bruises nor total bone bruise volume or bone bruise severity were associated with reduced pre- or postoperative KOOS or IKDC scores.
On the contrary, the size of tibiofemoral bone marrow lesions in the OA knee have been related to patient-reported pain. 16 In tibiofemoral OA, the bone remodeling process becomes chronic—a process that may be worsened in knees with combined bone marrow edema and local articular changes. The articular cartilage, if interrupted, cannot shield the underlying bone from continued mechanical and hydrodynamic stress. This increases the force borne by and fluid shift through the lesion site, and creates a perpetuating cycle of bone remodeling and chronic pain.16-18 However, if this stress can be removed, bone bruises can resolve. For example, the majority of asymptomatic, uninjured distance and marathon runners demonstrate bone marrow edema, and even a small percentage were graded as having severe lesions.19-21 The presence and severity of bone marrow lesions in this healthy, active population did not correlate with pain or symptoms. There are obvious differences between the traditional OA patient and marathon runner; however, one rationale for the different pain response to bone marrow edema between the 2 groups is that the trauma to the subchondral bone is not constant in the runner. The bone can respond to the repetitive stress and adapt over time, breaking the cycle of remodeling whereas the knee with untreated tibiofemoral OA cannot.
We suspect that the lack of relationship between bone bruises and either pre- or postoperative outcomes for ACL patients is largely due to the location of the bone bruises, the acute mechanism of injury, and our standard perioperative rehabilitation protocols. The majority of bone bruises were located on the lateral side. In general, during either walking or running gait, lower forces are borne by the lateral compartment, which may then lessen the likelihood of lateral bone bruises that are persistent or progressive in nature. Second, bone bruises are the direct result of the contact between the tibia and femur occurring at the time of ACL injury. 22 Provided that this violent mechanism is not recreated the resultant bone bruise will resolve, and our standard perioperative care may provide ample opportunity for this to occur. Both prior to and following surgery, rehabilitation programs and restrictions on running and cutting during the early postoperative period protect against repetitive, high-impact events necessary for persistent bone marrow edema. Clinical studies have supported this concept, as all Type 1 and Type 2 lesions as well as the majority of Type 3 bone bruises resolved 2 years following ACL reconstruction. 4
It is therefore unlikely that the severity or volume of preoperative bone bruises alone will be an accurate predictor of the progression of radiographic osteoarthritis. All 81 patients in our series had a lateral bone bruise, whether isolated or in conjunction with bone bruises in other regions. With evidence that the majority of bone bruises resolve, 4 bone bruises are not associated with pain and/or patient-reported function at 2 or 6 years, and the fact that 100% of patients demonstrated a lateral bruise pattern, the presence of lateral bone bruises is simply not a sensitive enough measure to be used as a predictive tool. More likely is that an individual patient’s progression of PTOA is multifactorial (articular cartilage damage, condition of the menisci, residual laxity or over-constraint, self-imposed activity modification, etc.). The multifactorial nature of PTOA progression and the inability for neither preoperative MRI nor postoperative radiographic assessment to identify patients with early degenerative changes has created the need for innovative methods to identify patients that have not followed a normal recovery pattern, but are instead demonstrating accelerated cartilage changes and a more rapid progression of PTOA.23,24
While the isolated presence of a bone bruise does not appear to be an indicator of poor midterm outcomes, the combined presence of a bone bruise with local articular cartilage pathology may be associated with inferior pain and daily function. If there was one subset of ACL patients in which bone bruise presence, volume, or severity might be indicative of persistent pain and/or functional limitations, we would expect it to be those with combined bone bruises and articular cartilage pathology. We likened this subset of patients to be more similar to the OA knee as they were significantly older and heavier with significantly greater bone bruise volumes and macroscopic articular pathology. We initially hypothesized that mild to moderate articular changes would increase the force attenuated by the subchondral bone, thus increasing the likelihood of persistent bone marrow edema and, possibly, pain. This hypothesis was, in part, supported by the current results. This subset did demonstrate significant improvements in all KOOS subscales and IKDC scores over the course of the first 6 years after ACL reconstruction. While KOOS Pain and ADL scores were statistically lower in this subset of patients both prior to and following surgery, these group differences were small in magnitude and likely not clinically meaningful. Furthermore, patients with bone bruises and combined articular cartilage pathology were 3.4 times more likely to have a symptomatic knee at 6 years than those without articular changes.
A significantly greater proportion of patients with bone bruises and combined articular cartilage pathology had concurrent lateral meniscus pathology than those with bone bruises without articular cartilage pathology. In isolation, lateral meniscectomies have been demonstrated to increase the risk of OA progression.25,26 However, a clear relationship between lateral meniscectomy and OA progression when performed at the time of ACL reconstruction has not been established. Recently, a systematic review and data from a large prospective cohort indicated that medial meniscal injury and/or meniscectomy increased the risks of OA development and poor patient-reported outcomes, but that lateral meniscus injury/meniscectomy did not.27,28 As such, it remains unclear if there is a potential connection between the increased prevalence of lateral meniscus pathology and knee symptoms 6 years after ACL reconstruction for those with combined bone bruises and articular cartilage pathology.
This study was not without limitation. We used a fairly simple method to estimate bone bruise volume whereas a more technically demanding voxel analysis would have been more accurate. However, we wanted to maintain the clinical relevance of our findings by utilizing a measurement technique that can easily be performed in any clinical setting with standard clinical MRI scans. Second, even though this is a very well-controlled single-center cohort, the sample size of this study was not large enough to allow for a comprehensive regression analysis of our data. Finally, it is also possible that patient-reported outcomes at 2 or 6 years are not sensitive enough to indicate possible structural changes associated with the progression of PTOA. Further long-term analyses are necessary to determine if a meaningful relationship exists between bone bruise location, volume, and/or severity with patient-reported outcomes 10 years after ACL reconstruction, particularly in those with combined articular changes at the time of surgery.
In conclusion, neither the volume nor severity of preoperative bone bruises identified on MRI were individually associated with 2- or 6-year patient-reported outcomes. ACL reconstruction successfully improved patient-reported pain and function, although patients with combined local articular cartilage pathology demonstrated significantly greater bone bruises volumes and had increased pain and reduced ability to perform activities of daily living. This older, heavier subset of patients were significantly more likely to be symptomatic 6 years after ACL reconstruction.
Footnotes
Authors’ Note
The study was performed at the Vanderbilt Orthopedic Institute and the University of Kentucky.
Acknowledgments and Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by the National Football League Charities Medical Grants Program. In addition, research reported in this publication was supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases of the National Institutes of Health under Award Number 5K23AR060275. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was obtained from the Vanderbilt University Institutional Review Board (Protocol #111583).
Informed Consent
Written informed consent was obtained from all subjects before the study.