
Abstract
Objective
Despite an increased interest in treatment options for cartilage lesions of the knee, the relationship between lesion characteristics and the symptoms they elicit is not well understood. We evaluated the relationship between lesion characteristics and the patient-reported outcome measures (PROMs) and compared this with symptoms reported by patients scheduled for knee ligament reconstruction and knee arthroplasty.
Design
Preoperative data, including Lysholm score and The Knee Injury and Osteoarthritis Outcome Score (KOOS), in 90 consecutive patients scheduled for surgery for symptomatic isolated cartilage lesions were prospectively collected.
Result
The patients had a mean age of 33.2 years. There were 62 (69%) males. There was no statistically significant difference in PROMs between patients with cartilage lesions smaller or larger than 2 cm2, except for the KOOS subscale symptoms, with patients with smaller lesions reporting higher scores, 62.8 (95% confidence interval [CI] 58.3-67.3) vs. 51.9 (95% CI 45.5-58.4), P = 0.005. There was a small correlation between lesion size and Lysholm score. However, when adjusted for age, sex, body mass index, and lesion localization, this effect was not statistically significant. The International Cartilage Regeneration & Joint Preservation Society grade did not affect preoperative PROMs. Cartilage patients reported worse preoperative symptoms than patients scheduled for knee ligament reconstruction, and approaching the symptoms reported by patients scheduled for knee arthroplasty.
Conclusion
The size, depth, and location of cartilage lesions have little impact on the symptoms experienced by the patients. Cartilage patients have comparable symptoms to patients scheduled for knee arthroplasty.
Introduction
Focal cartilage lesions of the knee remain a challenging condition for patients as well as orthopedic surgeons. However, the relationship between the cartilage lesions and symptoms is not fully understood. Some studies have found a lack of clear relationship between intraarticular knee pathology and patient-reported symptoms,1,2 while others have reported that such a relationship exists.3,4
The etiology of a focal cartilage lesion may be trauma, osteochondritis dissecans or osteonecrosis. Some lesions give no or little symptoms, 4 whereas other lesions lead to disabling pain and loss of function in daily activities. Symptoms may be related to size, depth, or location of the lesion. Symptoms may also be affected by other factors, such as sex, body mass index (BMI), activity level, and age. Further understanding of the impact on lesion size and symptoms is important to advance our understanding of this difficult injury. Despite the fact that the lesion size influences the choice of management,5,6 there is little data in the literature on the effect of lesion size and location on function and patient-reported symptoms. Although attempts have been made to outline this previously, 7 the current manuscript delineate a more complete outline of this particular knee injury in comparison to other common knee conditions subjected to surgery.
In the present study, we look closer at patients scheduled for surgery of a focal cartilage lesion in a symptomatic knee. The aims of this study were to investigate how lesion size, location, or depth relate to the patient’s preoperative symptoms and if factors such as age, sex, BMI, or activity level are related to the preoperative symptoms experienced by the patients. We also wanted to investigate how these symptoms correlate to symptoms from other knee conditions such as anterior cruciate ligament (ACL) injuries, recurrent patella dislocations, and osteoarthritis.
Method
Patients
The inclusion criteria were men and women aged 18 and 50 years scheduled for surgery due to an isolated focal cartilage lesion of the femoral condyle or the trochlea diagnosed on magnetic resonance imagining (MRI), without malalignment of the lower extremities, no previous cartilage surgery, a ligamentous stable knee, and no radiographic evidence of osteoarthritis ( Table 1 ).
Inclusion and Exclusion Criteria.
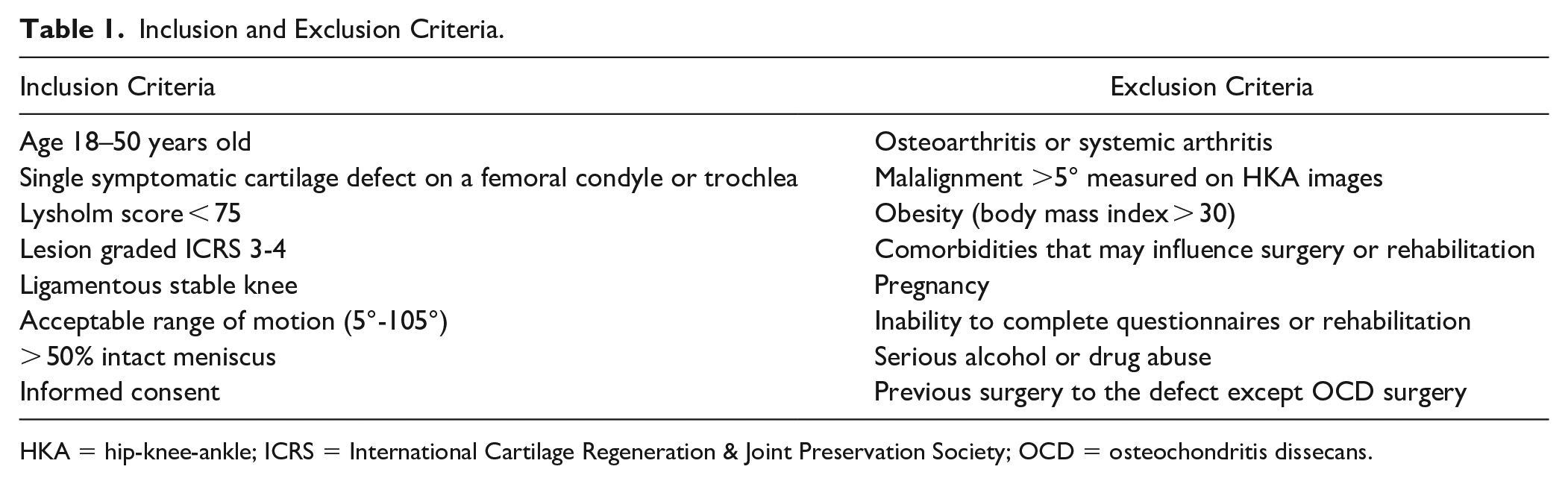
HKA = hip-knee-ankle; ICRS = International Cartilage Regeneration & Joint Preservation Society; OCD = osteochondritis dissecans.
Ninety consecutive patients scheduled for cartilage surgery due to symptomatic lesions of the femoral condyle or trochlea were included in the study (
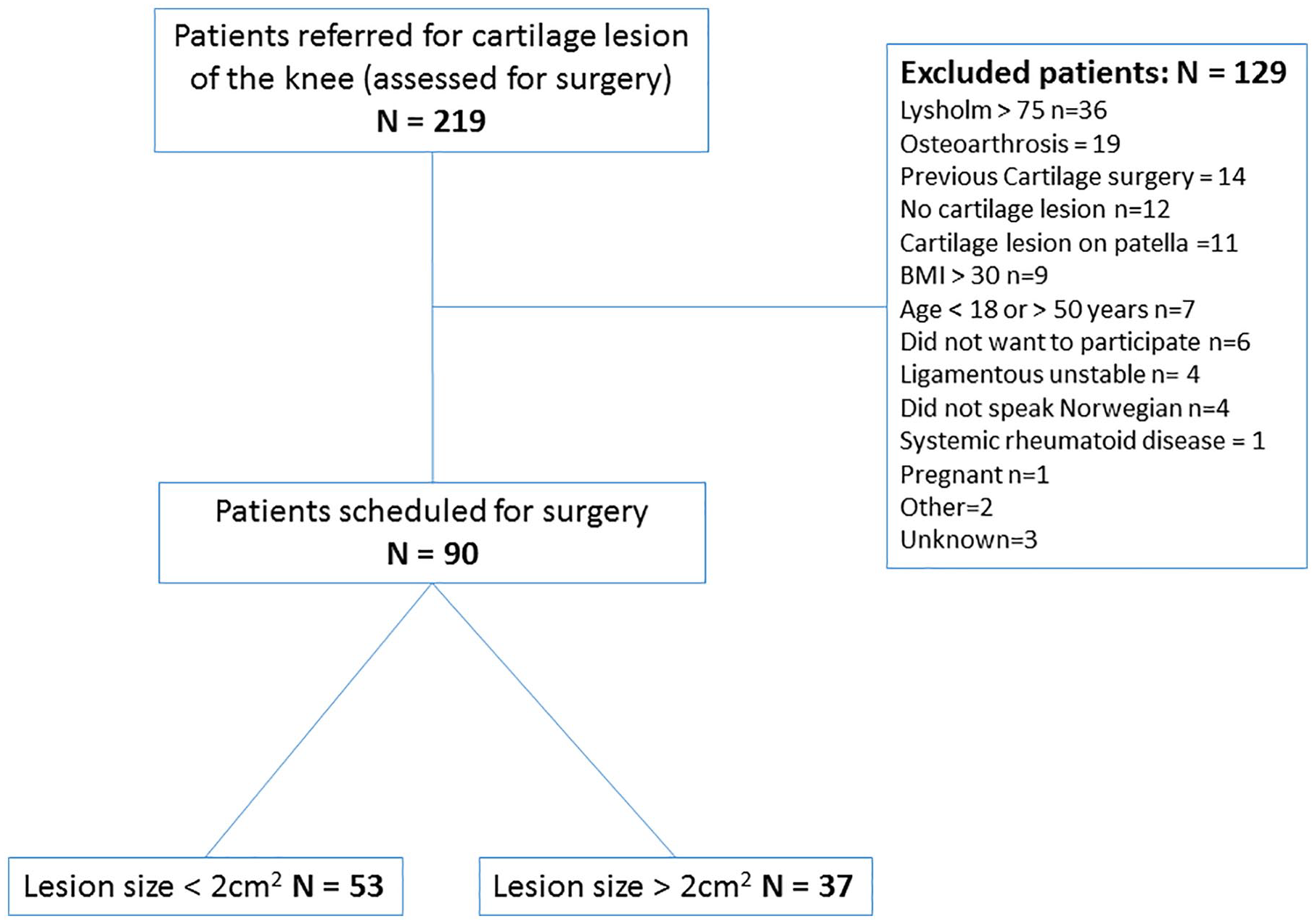
Flowchart of included patients.
Demographics and Patient Characteristics in 90 Patients with Full Thickness Isolated Cartilage Lesions of the Knee Scheduled for Surgery.
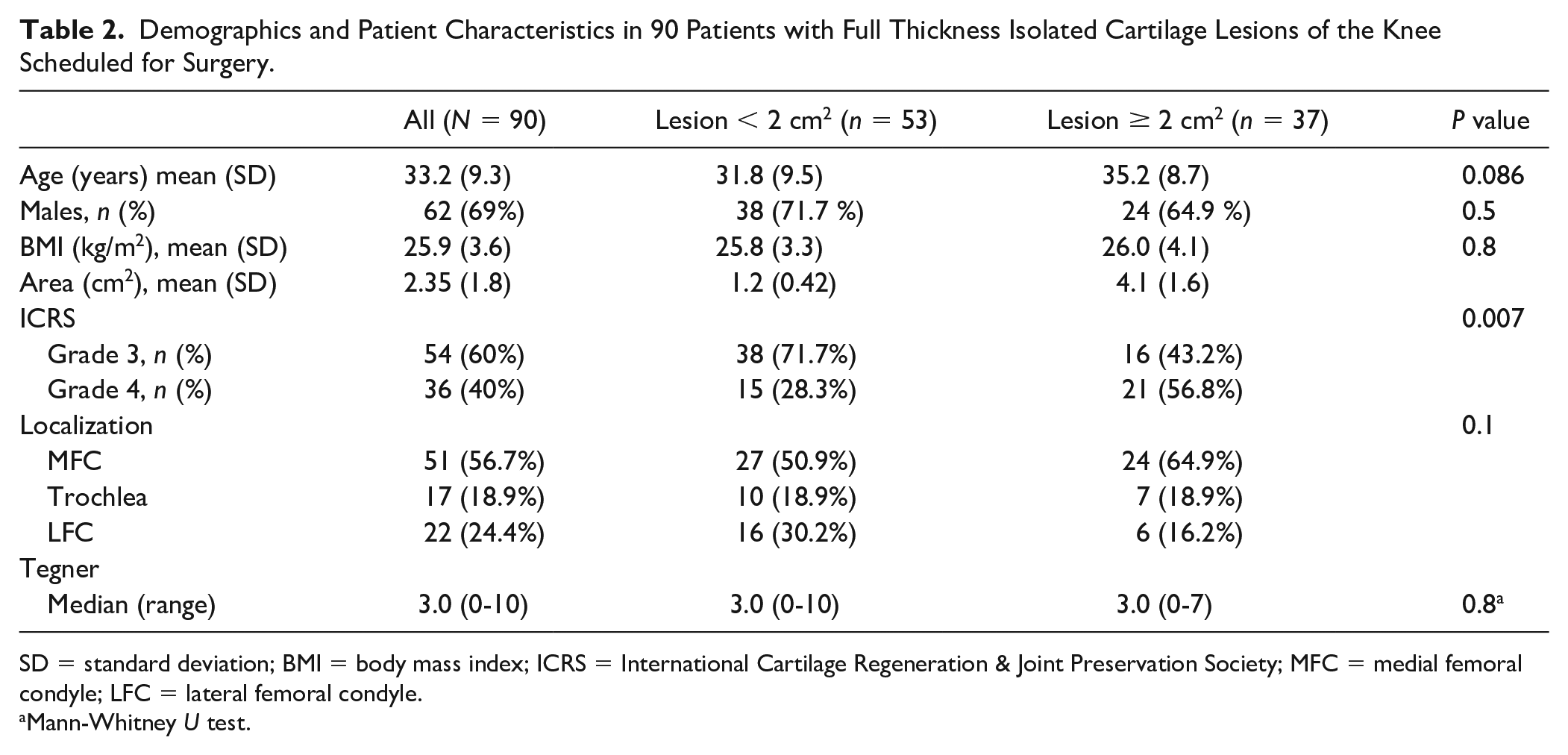
SD = standard deviation; BMI = body mass index; ICRS = International Cartilage Regeneration & Joint Preservation Society; MFC = medial femoral condyle; LFC = lateral femoral condyle.
Mann-Whitney U test.
Patient-Reported Outcome Measures
The patients completed the following validated patient-reported outcome scores prior to surgery:
Lysholm score
Lysholm score is a knee-specific outcome score containing 8 domains: limp, locking, pain, stairclimbing, use of support, instability, swelling, and squatting. 8 The Lysholm score quantifies the knee function on a scale from 0 to 100 (best) and has been recommended as an outcome measure in knee cartilage injuries. 9
The Knee Injury and Osteoarthritis Outcome Score (KOOS)
The KOOS score is a widely used questionnaire, which assesses 5 patient-reported domains: pain, symptoms, activity of daily living, sport and recreational function, and knee-related quality of life. A score from 0 to 100 (best) is calculated for each subscale which are independently used in all outcome comparisons, as recommended by Roos et al. 10
Visual analog scale (VAS) score
A VAS for pain was used, where 0 represents no pain and 10 represents the worst pain imaginable. VAS was provided for sitting and standing separately.
The patient-reported outcomes were compared with the symptoms reported by patients scheduled for ACL reconstruction reported to the Norwegian Knee Ligament Register, 11 patients scheduled for medial patellofemoral ligament (MPFL) reconstruction due to patella instability, 12 and patients scheduled for knee arthroplasty reported to the Norwegian arthroplasty registry. 13
Statistics
Continuous variables are presented as mean, median, 95% confidence interval (CI), range, and standard deviation (SD), while categorical data are presented in frequencies. Nonparametric variables were compared using the Mann-Whitney U test, while normally distributed variables were compared using Student t test. Categorical data were compared using the chi-squared test. Linear regression analysis was performed with adjustment for age, gender, and body mass index (BMI). A P value of <0.05 was considered significant. The analysis was performed using the Statistical Package for Social Sciences (SPSS) version 25 (IBM Corp, Armonk, NY, USA).
Results
There was no statistically significant difference in patient-reported symptoms at the time of inclusion between patients with cartilage lesions smaller or larger than 2 cm2, except for the KOOS subscale symptoms, with patients with smaller lesions reporting higher scores, 62.8 (58.3-67.3) vs. 51.9 (45.5-58.4), P = 0.005,
Table 3
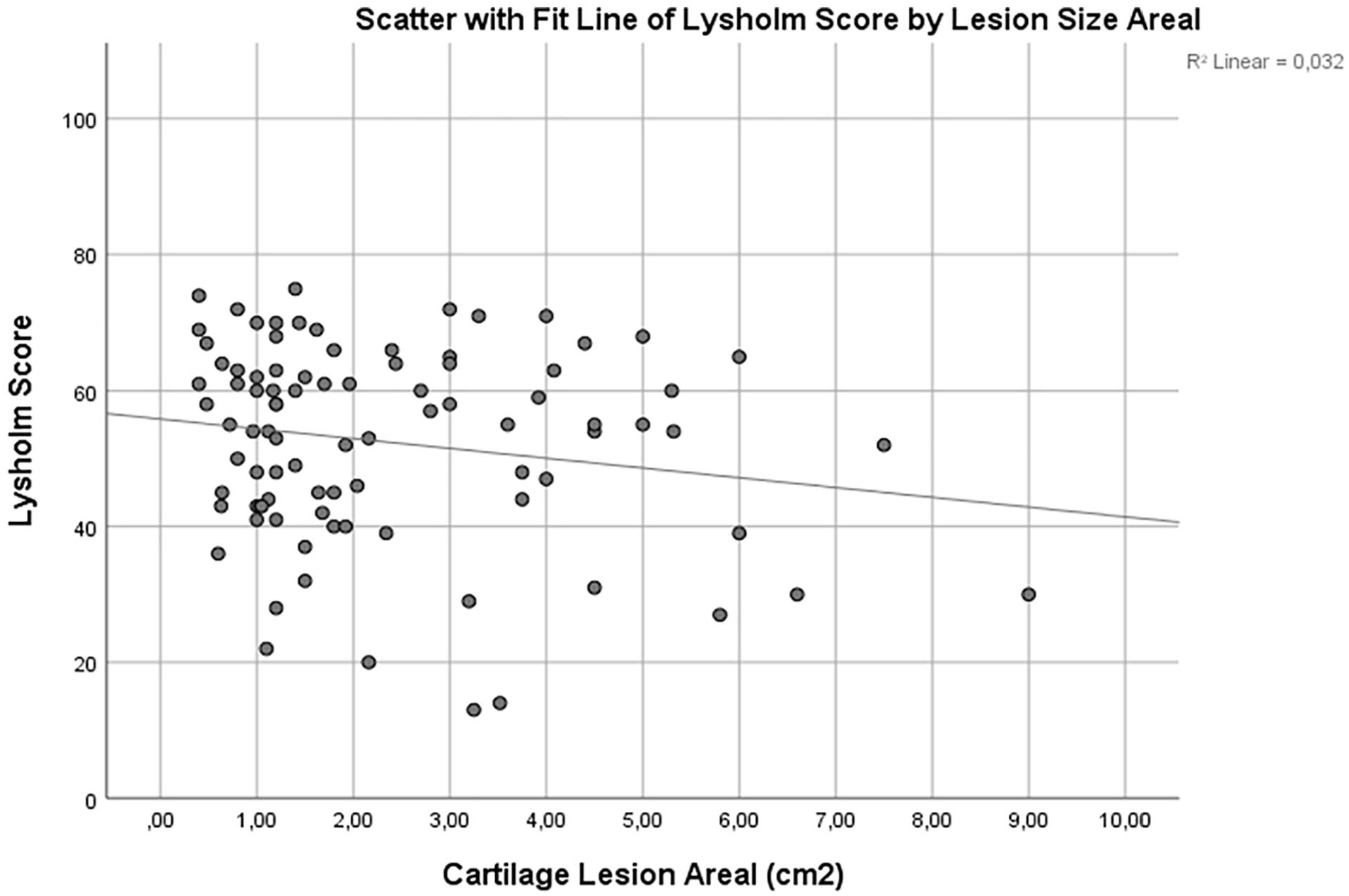
. There was a small correlation between lesion size and Lysholm score, with patients with larger lesions reporting slightly lower Lysholm scores (
Preoperative Patient-Reported Outcome Measures in 90 Patients Scheduled for Surgery due to Symptomatic Isolated Cartilage Lesions of the Femur.
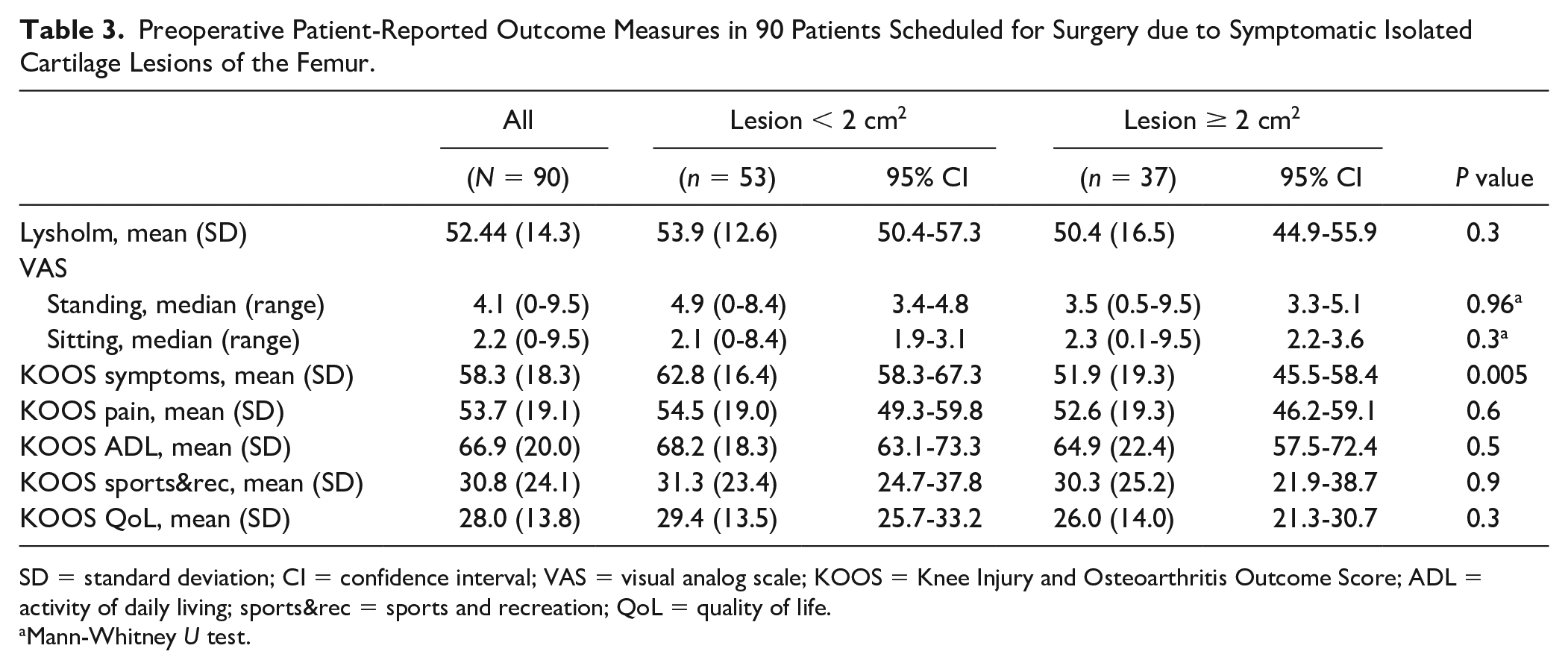
SD = standard deviation; CI = confidence interval; VAS = visual analog scale; KOOS = Knee Injury and Osteoarthritis Outcome Score; ADL = activity of daily living; sports&rec = sports and recreation; QoL = quality of life.
Mann-Whitney U test.
Preoperative Lysholm score stratified by lesion size in 90 patients scheduled for cartilage surgery of the knee.
Multivariate Linear Regression Analysis of the Effect on ICRS Grade 3 (Reference) or 4, Lesions Size (cm2), and Lesion Localizationon Lysholm Score in 90 Patients with an Isolated Cartilage Lesion of the Knee.
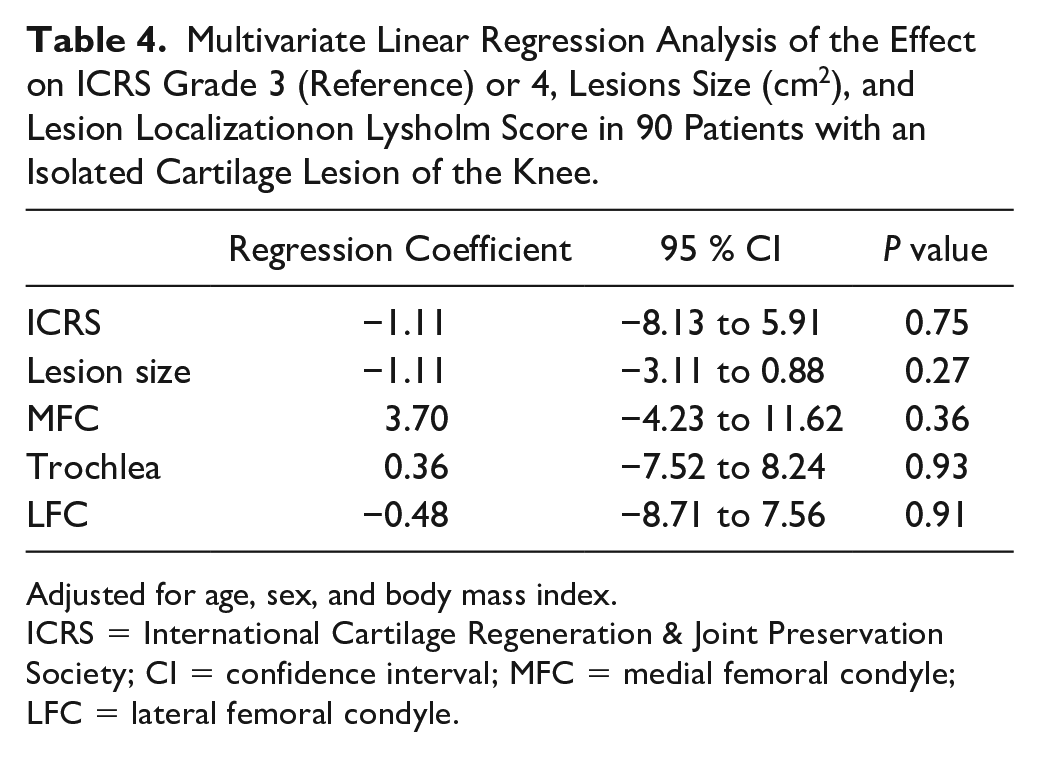
Adjusted for age, sex, and body mass index.
ICRS = International Cartilage Regeneration & Joint Preservation Society; CI = confidence interval; MFC = medial femoral condyle; LFC = lateral femoral condyle.
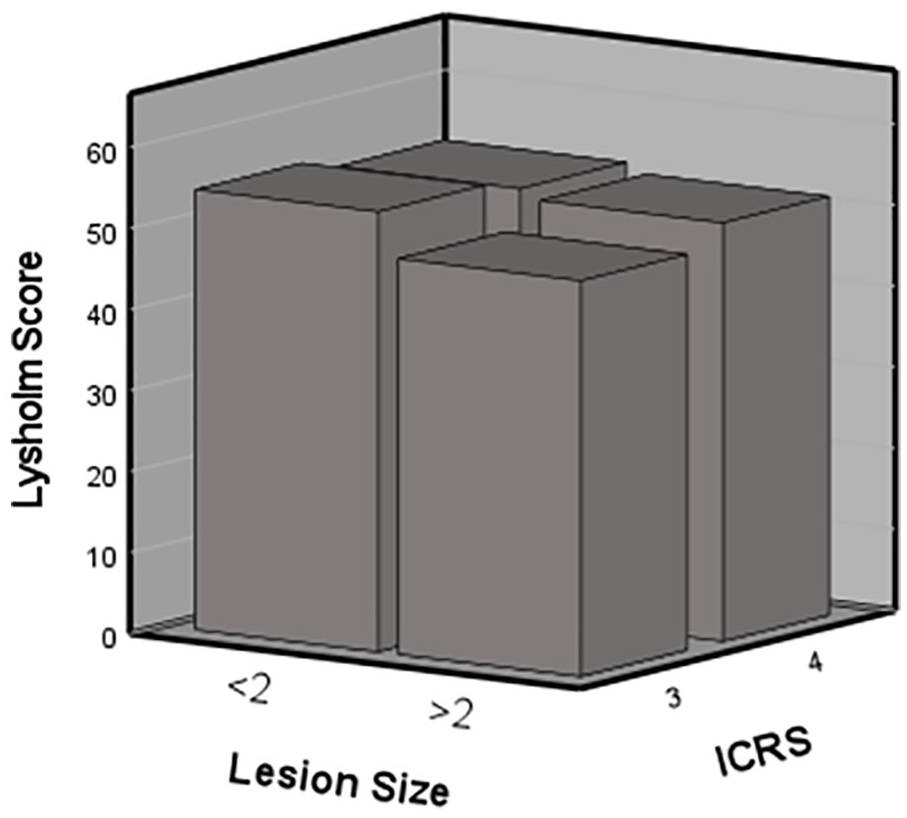
Preoperative Lysholm score according to International Cartilage Regeneration & Joint Preservation Society (ICRS) grade and lesions size smaller or larger than 2 cm2 in 90 patients scheduled for cartilage surgery of the knee.
The cartilage patients reported worse preoperative symptoms compared with patients scheduled for ACL reconstruction or MPFL reconstruction, and approaching the symptoms reported by patients scheduled for total knee replacement (
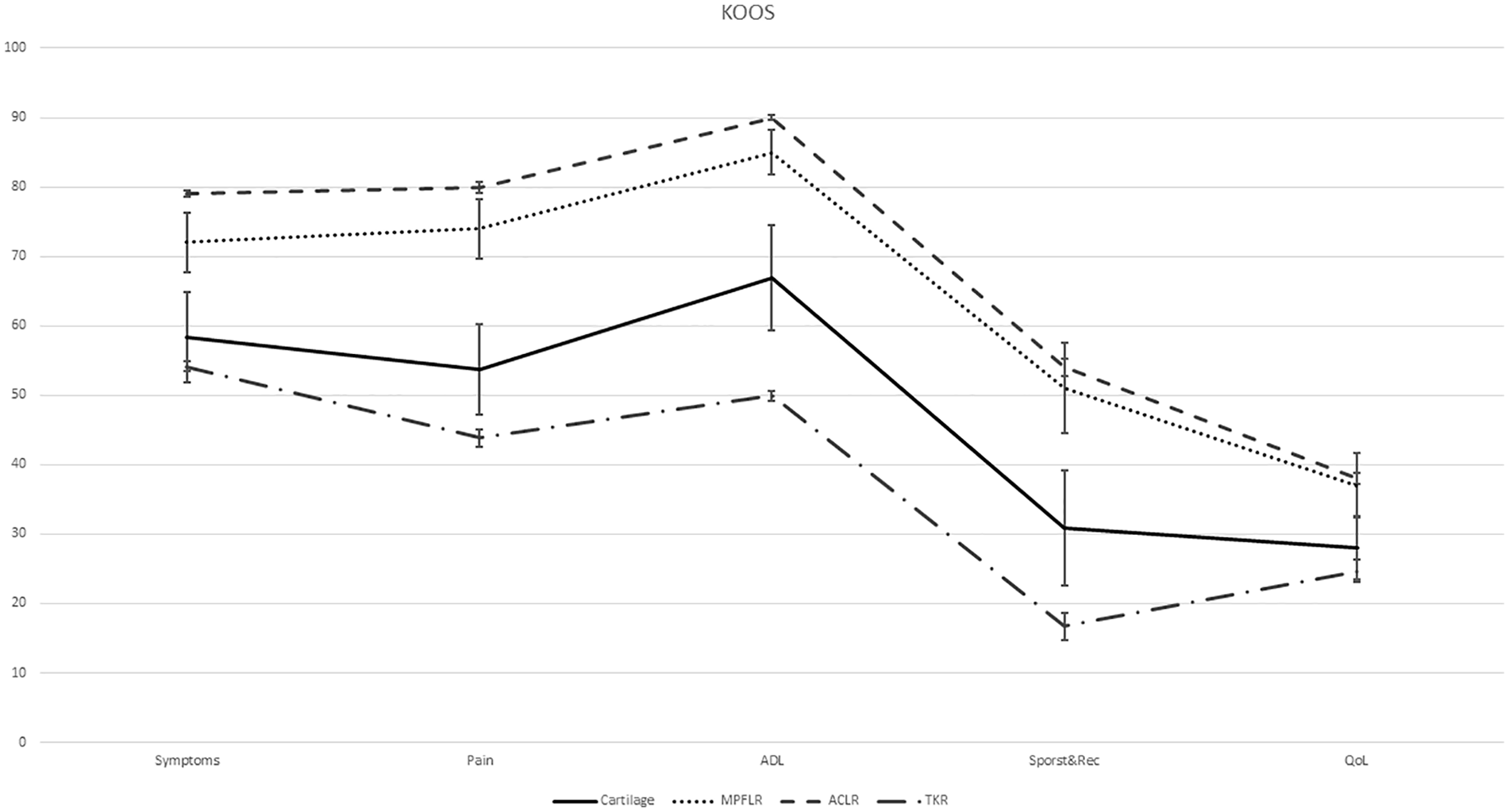
Preoperative Knee Injury and Osteoarthritis Outcome Score (KOOS) scores in patients scheduled for anterior cruciate ligament reconstruction (ACLR), medial patellofemoral ligament reconstruction (MPFLR), cartilage surgery and total knee replacement (TKR). Brackets represent 95% confidence intervals.
Discussion
The main finding of this study is that the size of the cartilage lesions has little effect on the level of pain and function in patients scheduled for cartilage surgery of the knee. Location of the lesion in the knee also did not substantially affect the level of symptoms reported by the patient preoperatively. However, the pain and disability reported by patients with isolated cartilage lesions approach the values reported by patients scheduled for knee arthroplasty.
We could not demonstrate any substantial effect of the lesions size or ICRS grade on the level of pain reported at the time of surgery. Our results are supported by Solheim et al. who evaluated patient-reported symptoms in 570 patients with chondral or osteochondral lesions of the knee and found that size and location had little influence on patient-reported symptoms. 7 It is clear that the etiology of the pain and symptoms caused by the lesions is not well understood. It seems that even small lesions can give symptoms severe enough to warrant surgery. Cartilage itself is aneural and cartilage defects alone do not elicit pain. Cartilage lesions regardless of size may instigate the same response to the joint through synovitis, leading to similar degree of symptoms. This may also explain why symptoms of cartilage patients are different from those suffering ligament instability, and more similar to those reported by osteoarthritic patients. At the same time, up to 69% of asymptomatic individuals can have full thickness cartilage lesions diagnosed on MRI scans.1,2,14 It is therefore difficult to ascertain that it is indeed the cartilage lesion identified on the MRI that is causing the symptoms.
There is no consensus regarding what constitutes the best treatment for symptomatic cartilage lesions. There has been a great focus on various surgical methods to treat these lesions, but without understanding the basic pathophysiology of the condition, it is unlikely that an ideal surgical treatment will be found. Surgical treatment options include debridement, 15 microfracture, 16 mosaicplasty, 17 osteochondral allograft transplantation (OAT), 18 and cell-based therapies, such as autologous chondrocyte implantation (ACI). 19 Surgical treatment is often dictated by lesion size and location, and the patient’s age, general health, activity level, and symptoms. There is general agreement in the literature that microfracture is not effective in larger lesions, and a cutoff of 2 cm2 is often cited.5,6,20 ACI or OAT is commonly offered patients with larger lesions.6,18-20 The literature has an abundance of case series evaluating the effect of various type of cartilage surgeries, but there is a lack of high-level prospective trials with a true control group. It is reported that up to 75% of patients with a focal cartilage defect of the knee has good to excellent results following a regimen of conservative treatment.21,22 Future clinical studies need to include a conservative control group (non-operative or sham-surgery).23,24
Over a decade ago, Heir et al. compared 60 patients scheduled for surgery for an isolated cartilage lesion of the knee with 64 patients scheduled for total knee arthroplasty (TKA). They found that patients enrolled for cartilage surgery have score values on the KOOS quality of life subscale equal to patients scheduled for TKA. 25 Our study confirms this finding in a larger cohort of cartilage patients. We demonstrate that cartilage lesions of the knee is a severe condition with detrimental effect on pain and function. In fact, patients scheduled for cartilage surgery are closer in age to patients scheduled for ACL and MPFL reconstruction, but have KOOS scores approaching that of older patients scheduled for knee arthroplasty.
Limitations
Our study was conducted in a specialist center in one country and may have limited external validity. A Lysholm score below 75 was an inclusion criterion for this study. This introduces a selection bias that may influence our results. The patients in this study are patients scheduled for surgery—Whether the same findings apply to patients treated non-operatively cannot be answered by our study. As a majority of the patients had a lesion on the medial femoral condyle, it might be that other locations respond better to non-surgical treatment.
Conclusion
The size, depth, and location of cartilage lesions have little impact on the pain and symptoms experienced by the patients.
Footnotes
Authors’ Note
The work was conducted at Akershus University Hospital, Norway.
Acknowledgments and Funding
The authors thank Heidi Andreassen Hanvold, PT, for help in data management. They thank Tommy Frøseth Aae, Øystein Lian, Håvard Visnes, and Thomas Birkenes for including patients. The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by research grants awarded from the Research Council of Norway, Grant 243818.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics
This study was approved by the Regional Committee for Medical and Health Research Ethics, North-Norway (2015/2200 and 2015/2202). The study was conducted in accordance with the Declaration of Helsinki and conformed to the International Committee of Medical Journal Editors recommendations for protection of research participants. All included patients provided written informed consent.