
Abstract
Objective
To evaluate the effect of fear of reinjury on return to sport (RTS), return to work (RTW), and clinical outcomes following autologous chondrocyte implantation (ACI).
Design
A retrospective review of patients who underwent ACI with a minimum of 2 years in clinical follow-up was conducted. Patient-reported outcomes collected included the Visual Analog Scale (VAS) and Knee Injury and Osteoarthritis Outcome Score (KOOS). Kinesiophobia and pain catastrophizing was assessed using the Tampa Scale of Kinesiophobia-11 (TSK-11) and Pain Catastrophizing Scale (PCS), respectively. Patients were surveyed on their RTS and RTW status.
Results
Fifty-seven patients (50.9% female) were included in our analysis. Twenty-two (38.6%) patients did not RTS. Of the 35 patients (61.4%) who returned, nearly half (48.6%) returned at a lower level of play. TSK-11 (P = 0.003), PCS (P = 0.001), and VAS pain scores (P < 0.001) were significantly greater in patients that did not RTS than in those who returned. All KOOS subscores analyzed were significantly lower (P < 0.001) in patients that did not RTS than in those who returned at the same level or higher. Of the 44 (77.2%) patients previously employed, 97.7% returned to work. Increasing TSK-11 scores were associated with lower odds of returning to sport (P = 0.003).
Conclusion
Fear of reinjury decreases the likelihood that patients will return to sport after ACI. Patients that do not return to sport report significantly greater levels of fear of reinjury and pain catastrophizing and lower clinical knee outcomes. Nearly all patients were able to return to work after surgery.
Level of Evidence
IV case series.
Keywords
Introduction
Articular cartilage defects (ACDs) are increasingly common injuries in recreational to high-level professional athletes that often lead to pain and dysfunction.1-4 Autologous chondrocyte implantation (ACI) and its third-generation iteration matrix-associated autologous chondrocyte implantation (MACI) are restorative techniques that have been increasingly utilized to address these cartilage lesions, restore preinjury function, and get patients back to their desired level of work and sport.5,6 Prior studies have identified duration of knee symptoms, lesion characteristics, and preinjury level of competitiveness as nonmodifiable predictors of postoperative clinical outcomes.2,7-9 However, the effects of kinesiophobia, defined as reluctance to resume physical activity due to the fear of reinjury and pain catastrophizing, is not well studied in this cohort. 10
Kinesiophobia has garnered notable attention in the return to sport (RTS) literature particularly in patients with anterior cruciate ligament (ACL) injuries.9,11-14 A systematic review by Ardern et al. 13 described fear of reinjury as the most commonly reported reason for individuals changing or terminating postoperative sports participation after ACL reconstruction surgery. Similarly, Paterno et al. 15 reported that patients with heightened fear were 4 times more likely to report lower levels of activity, decreased functional performance, and increased risk of ipsilateral ACL reinjury postoperatively.
Thoma et al.10 provided initial evidence supporting the association of higher levels of kinesiophobia and pain catastrophizing with poor patient-reported outcomes in patients with ACDs. These effects may also be reflected in a patient’s disposition to RTS or return to work (RTW) although this has not been directly investigated. In patients with ACDs, the expected rate of RTS is high (89% and 86% RTS for ACI and MACI, respectively). 16 However, of the patients returning to sport, only 76% and 71% of ACI and MACI patients, respectively, returned to their preinjury sport level. Thus, it has been postulated that kinesiophobia and psychological factors may, in part, account for this discrepancy. 17 As many as 10%-39% of individuals have no recollection of a specific knee injury upon initial presentation for an ACD.18,19 Given the indolent nature of initial injury and poor regenerative capacity of articular cartilage, these initially asymptomatic lesions progress, leading to delayed presentation and ultimately chronic pain, a known contributor to kinesiophobia. 20
The high prevalence of articular cartilage injuries, discrepancies between levels of RTS, and predisposition for developing maladaptive behaviors due to chronic pain necessitate a better understanding of how kinesiophobia affects this population. The goal of this investigation is to evaluate the effect of fear of reinjury on RTS, RTW, and clinical outcomes following ACI.
Methods
Study Design
All study activities were commenced after approval by the institutional review board (i19-01430). A retrospective review of a prospectively collected database of patients who underwent an ACI or MACI procedure between August 1, 2010, and July 31, 2020, at a single urban academic medical center was performed. Demographic data, medical history, surgical information, and clinical outcomes measures were abstracted from the database. Data with respect to lesion characteristics including size, location, and grade (Outerbridge classification) were collected. Patients were included if they (1) underwent a unilateral ACI or MACI, (2) were under 50 years of age at the time of surgery, and (3) had at least 2 years of follow-up. Patients were excluded if they presented for a graft revision procedure or underwent a bilateral knee surgery.
Return to Sport and Return to Work
Subjects were surveyed and asked to indicate the level and type of sport played prior to their articular cartilage injury and whether they returned to play. If they returned, follow-up questions were administered to assess the physical and psychological barriers they faced (Suppl. Appendix A).
In addition, subjects were queried about their preinjury and postoperative employment status, specifying the degree of physical labor involved, to assess their RTW status.
Outcome Measures
Psychological assessment of kinesiophobia was conducted using the shortened Tampa Kinesiophobia Scale 11 (TSK-11) and the Pain Catastrophizing Scale (PCS). The TSK-11 is a validated psychometric tool used to measure self-reported disability and pain-related activity-avoidance behavior.20,21 The PCS is comprised of three subscales analyzing psychological patterns of rumination, magnification, and helplessness, which may contribute to catastrophic thinking. 22 Higher scores in both these psychometric tools suggest elevated levels of kinesiophobia and pain catastrophizing. Patient satisfaction and pain were assessed using a Visual Analog Scale (VAS). Patient-reported clinical outcome measures included the Knee Injury and Osteoarthritis Outcome Score (KOOS) subscales of Pain, other Symptoms, Function in Sport and Recreation, and knee-related Quality of Life (QOL).23,24
Statistical Analysis
Independent samples t-tests were used to compare the difference in continuous variables. The Shapiro-Wilk test was used to assess continuous variables for normality. Analyses of variance were performed to compare the differences between the three RTS categories, with Tukey post hoc analysis to elucidate the differences between each category for normally distributed variables. The Kruskal-Wallis test was used for nonparametric variables with the Dwass-Steel-Critchlow-Fligner test for multiple comparisons analysis. Chi-squared analysis was performed to compare categorical and binomial variables between sex categories. Statistical significance for all analyses was set at P < 0.05 and odds ratios (ORs) were calculated with a 95% confidence interval. Averages are reported as mean ± standard deviation unless otherwise stated. All statistical analyses were performed using R Statistical Software (version 4.2.1; R Foundation for Statistical Computing, Vienna, Austria).
Results
Patient and Defect Characteristics
Flow of patient acquisition is displayed in Figure 1 . The final cohort consisted of 57 patients; 29 (50.9%) female and 28 (49.1%) male patients. The mean age of participants was 29.11 ± 9.25 years, and the mean body mass index (BMI) was 25.66 ± 6.05 kg/m2. Further descriptive demographic data are summarized in Table 1 .
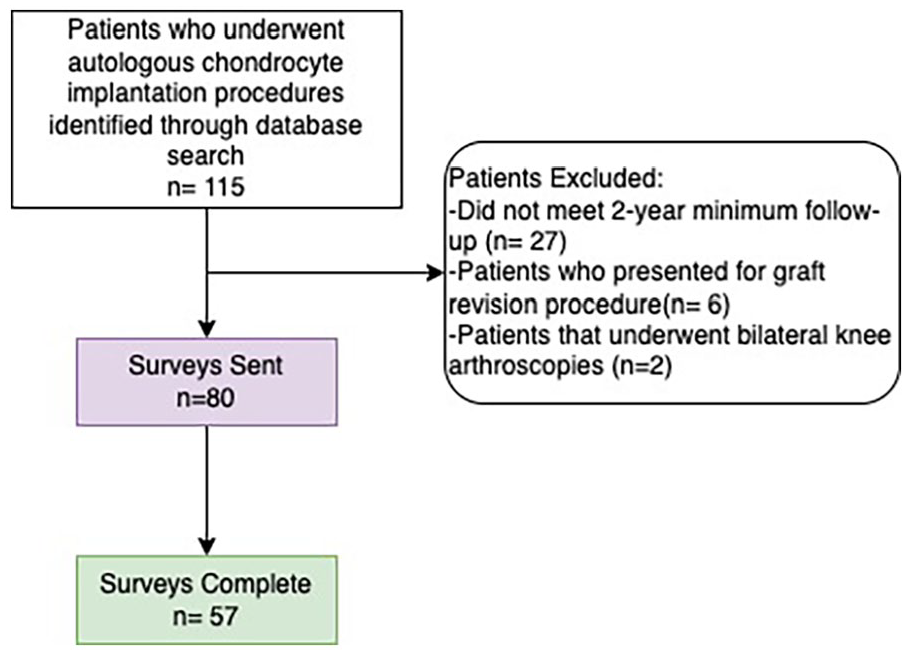
Flow of patient acquisition.
Patient Demographics and Presurgical Sport Level By Return to Sport Status.
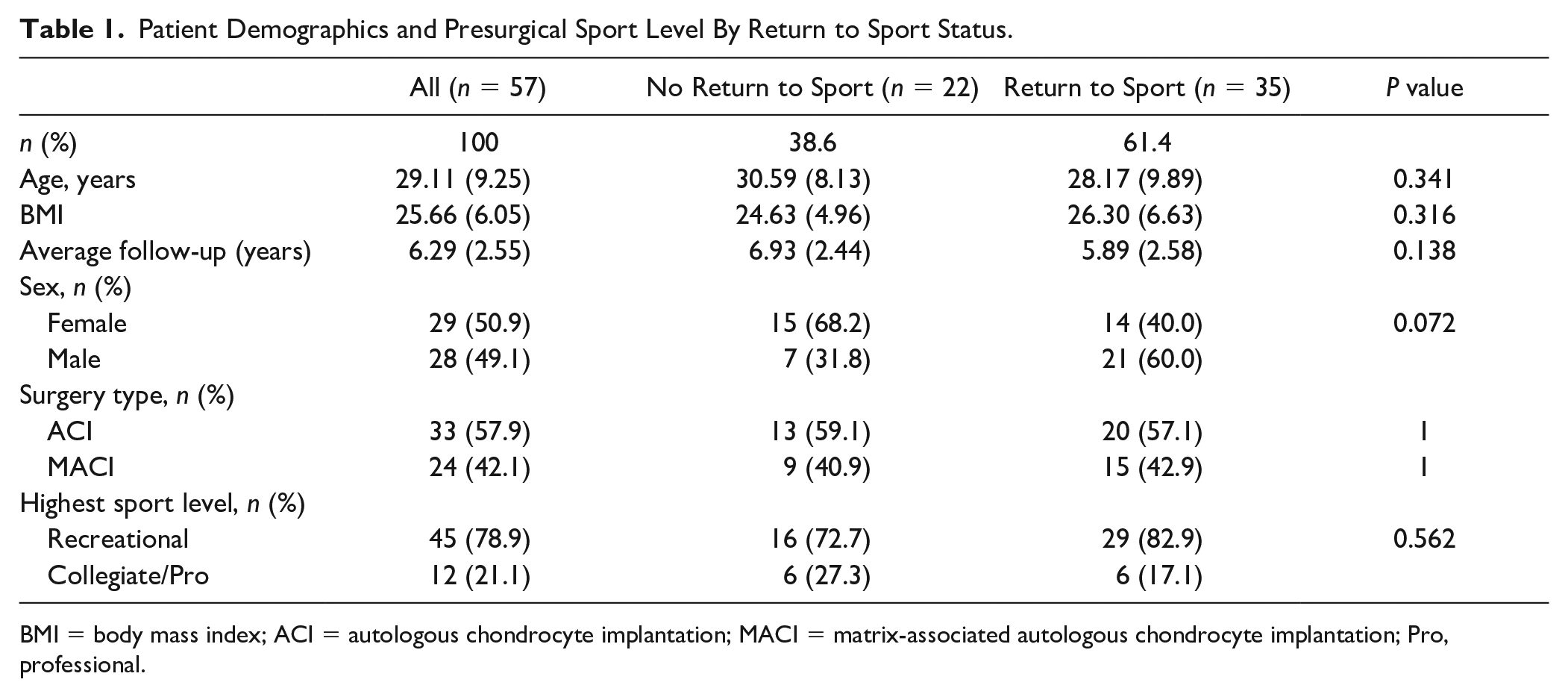
BMI = body mass index; ACI = autologous chondrocyte implantation; MACI = matrix-associated autologous chondrocyte implantation; Pro, professional.
There were a total of 72 high-grade lesions in 57 knees. Most lesions were in the patella (n = 39, 54.2%), followed by trochlea (n = 18, 25%), medial femoral condyle (MFC) (n = 9, 12.5%), and lateral femoral condyle (n = 6, 8.3%). Forty-four (77.1%) patients had 1 defect, 12 (21.1%) had 2 defects, and 1 (1.8%) had 4 defects. The mean lesion size at implantation was 3.4 cm2.
Concomitant Procedures
In this cohort, 35 (61.4%) patients underwent a concomitant tibial tubercle osteotomy (TTO), 7 (12.3%) underwent medial patellofemoral ligament reconstruction, 5 (8.8%) underwent lateral release, 3 (5.3%) underwent a chondroplasty, 1 (1.8%) underwent a meniscal allograft transplant, and 1 (1.8%) underwent a meniscectomy.
Return to Sport and Clinical Outcomes
Of all, 61.4% of patients reported returning to sport after surgery. No differences in RTS rates were found between procedure types (MACI vs. ACI) and preinjury level of sport activity (recreational vs. collegiate/professional) ( Table 1 ).
When stratifying patients into those that returned to sport and those that did not, there were significant differences in VAS pain and satisfaction, all KOOS subscores, TSK-11, and PCS, which are reported in
Table 2
. Patients who returned to sport had significantly higher average KOOS scores across all subscores (symptom: 82.00 vs. 63.73, pain: 91.98 vs. 74.12, sports: 75.86 vs. 41.36, QOL: 70.18 vs. 34.38, P < 0.001). Both the mean TSK-11 (26.59 ± 3.81 vs. 22.00 ± 6.16, P = 0.003) and PCS (9.41 ± 9.42 vs. 2.83 ± 4.53, P = 0.001) scores were significantly higher in patients who did not return to sport. The number, size, and location of cartilage lesions, as well as the quantity and type of concomitant procedures, were nonsignificantly different between groups (
Table 2
). Although there was no significant difference in the dichotomous question assessing quality-of-life improvement postoperatively, individuals who did not return to sport reported significantly lower improvement in symptoms, pain, and sport activity (
Outcomes Scores, Concomitant Procedures, and Lesion Location by Return-to-Sport Status.
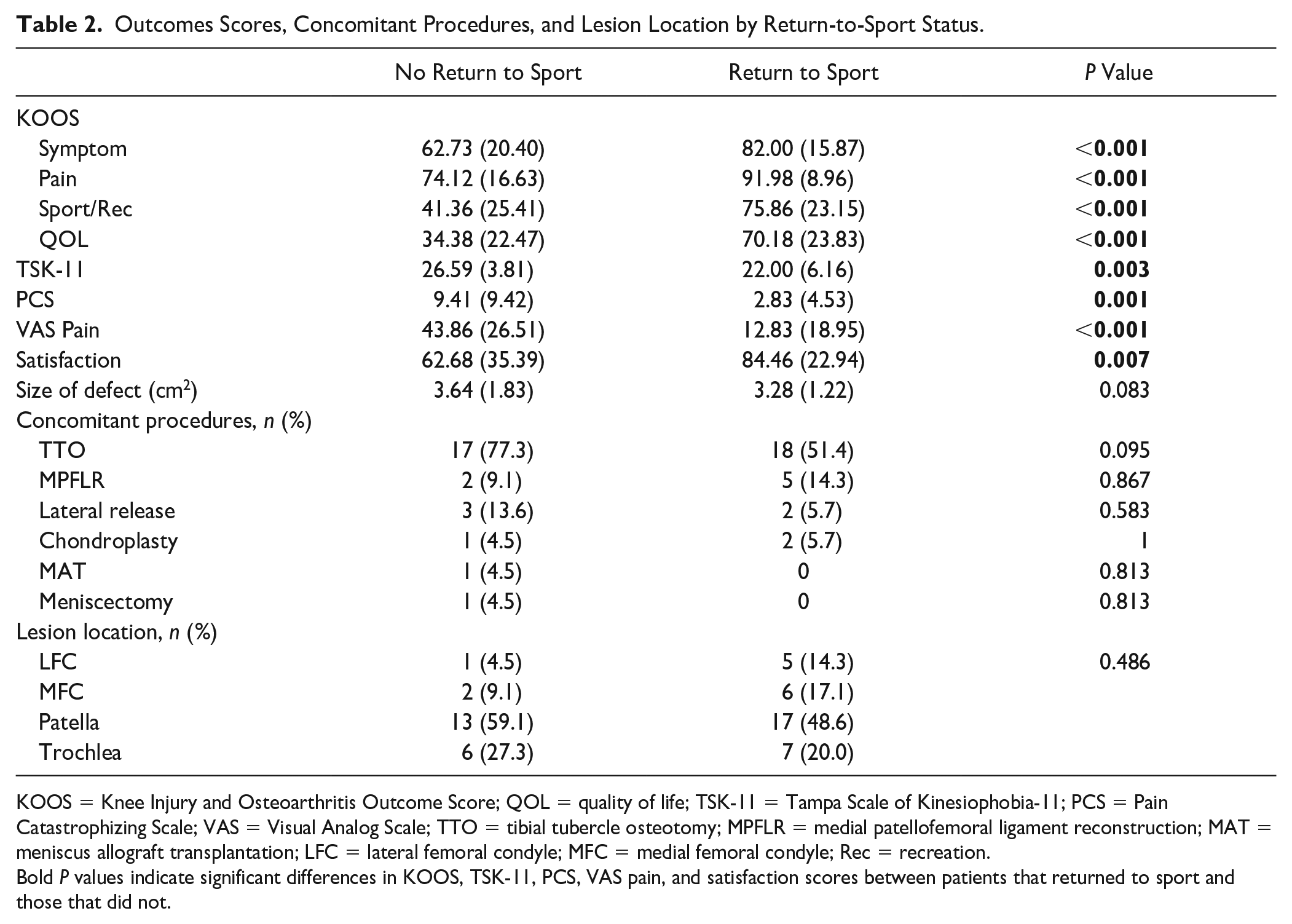
KOOS = Knee Injury and Osteoarthritis Outcome Score; QOL = quality of life; TSK-11 = Tampa Scale of Kinesiophobia-11; PCS = Pain Catastrophizing Scale; VAS = Visual Analog Scale; TTO = tibial tubercle osteotomy; MPFLR = medial patellofemoral ligament reconstruction; MAT = meniscus allograft transplantation; LFC = lateral femoral condyle; MFC = medial femoral condyle; Rec = recreation.
Bold P values indicate significant differences in KOOS, TSK-11, PCS, VAS pain, and satisfaction scores between patients that returned to sport and those that did not.
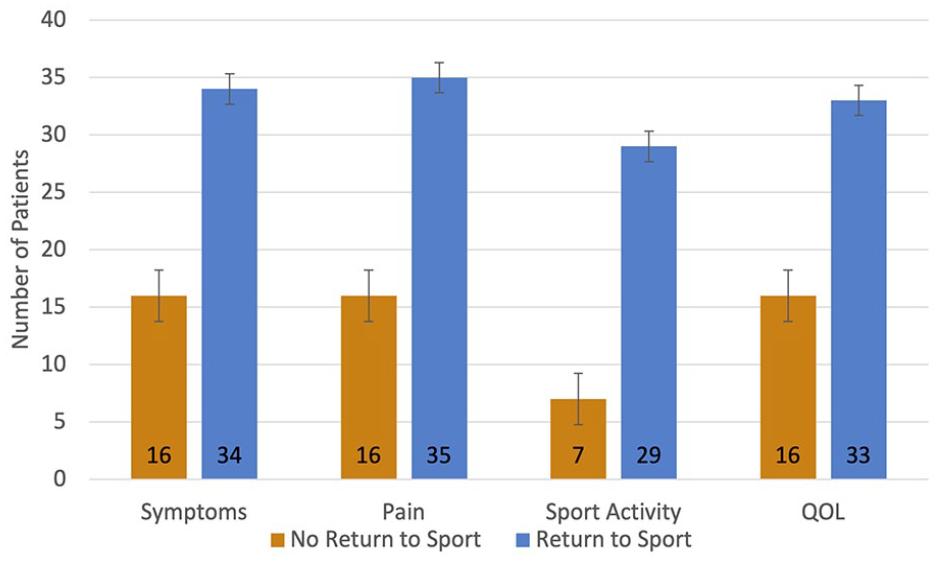
Number of patients that reported improvement in outcomes among patients that returned to sport and those that did not. QOL = quality of life. P values for inter-group comparisons: Symptoms (p=0.02), pain (p=0.005), sport activity (<0.001), QOL (0.059).
A subanalysis of individuals who returned to sport was performed. There was no difference in age, sex, or BMI between patients who returned to sport at a level lower than preinjury participation compared to those who returned at the same level or higher. Patient-reported outcomes also did not differ significantly between these groups, except for KOOS-QOL scores which were significantly higher in those that retuned to sport at the same or higher level than patients that retuned to sport at a lower level. Further demographic information and preinjury athletic activity are summarized in Table 3 .
Subgroup Analysis of Outcomes Based on Return-to-Sport Level.
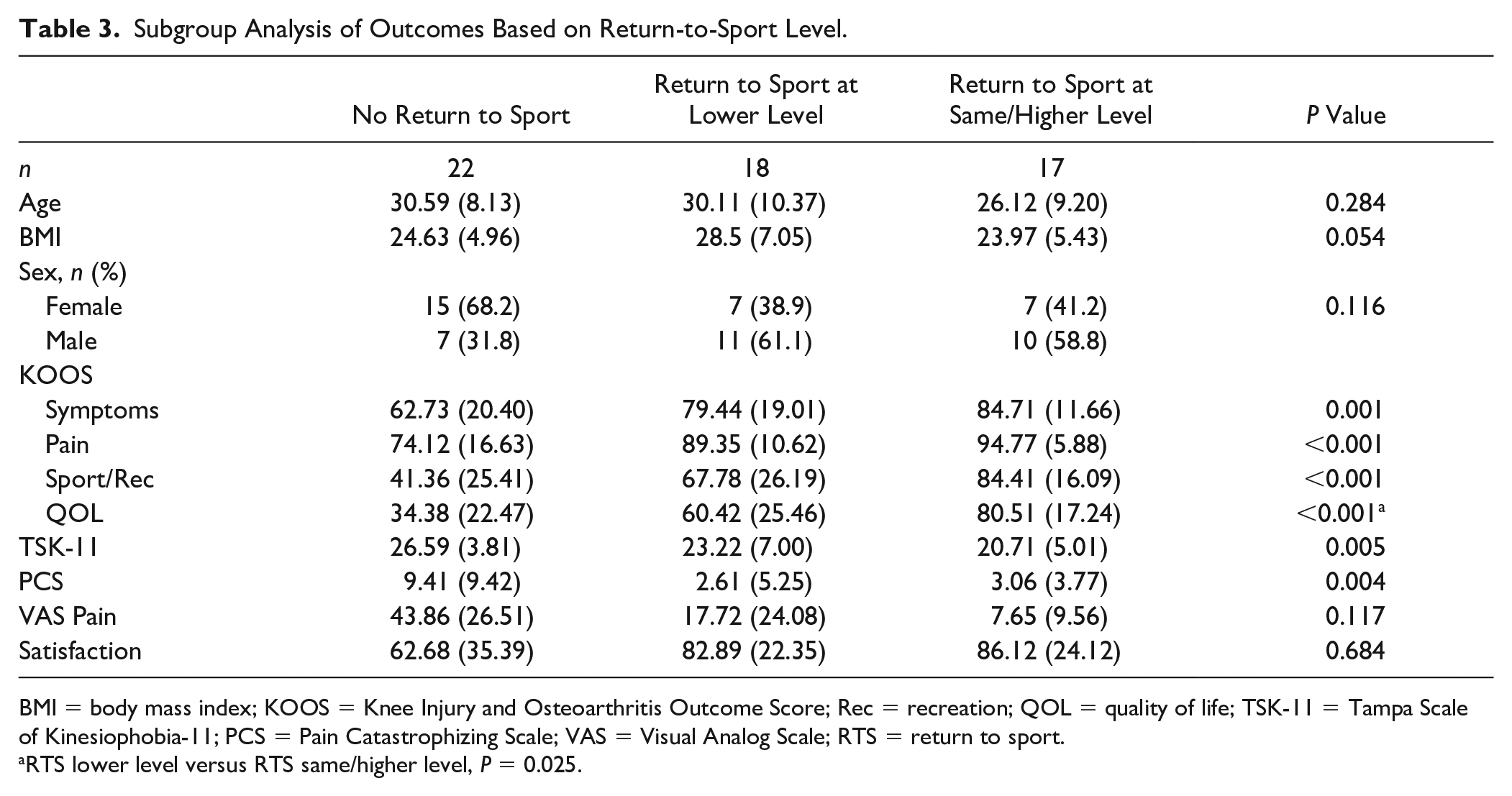
BMI = body mass index; KOOS = Knee Injury and Osteoarthritis Outcome Score; Rec = recreation; QOL = quality of life; TSK-11 = Tampa Scale of Kinesiophobia-11; PCS = Pain Catastrophizing Scale; VAS = Visual Analog Scale; RTS = return to sport.
RTS lower level versus RTS same/higher level, P = 0.025.
Although each stepwise decrease in sport level was accompanied with increased average levels of kinesiophobia, fear of reinjury was only significantly higher in the group that did not return to sport than in those returning at the same level or greater (P = 0.003). Consistently, patients that did not return to sport had higher rates of pain catastrophizing than both patients that returned to sport at a lower level and those who returned at the same level or higher (P = 0.002, P = 0.024).
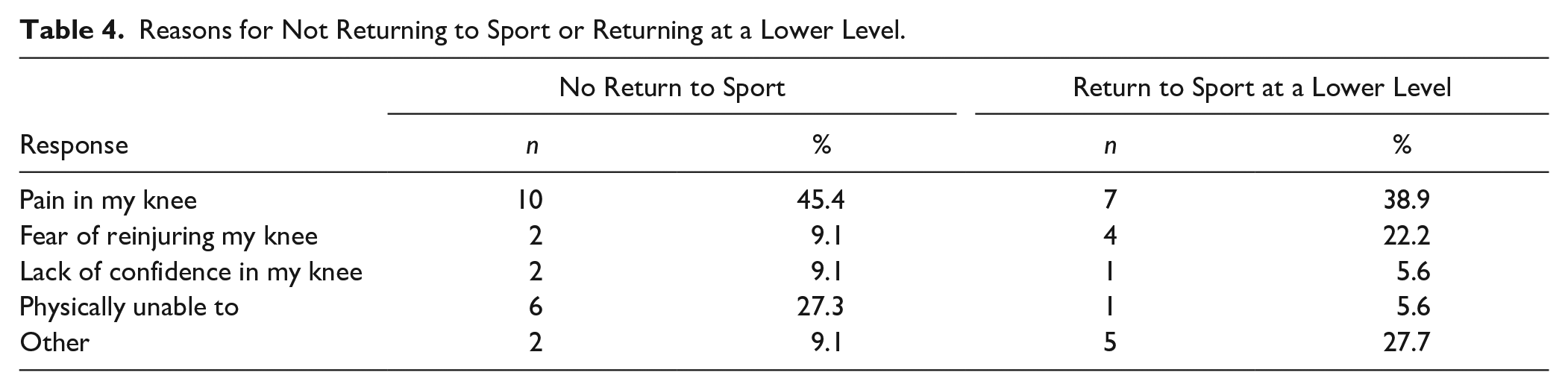
The most common reason reported for both not returning to sport and returning to sport at a lower level was pain in the knee at 45.5% and 38.9%, respectively ( Table 4 ). Fear of reinjury was stated as the primary reason for decreasing sport level in 22% of those returning at a lower level of play.
Reasons for Not Returning to Sport or Returning at a Lower Level.
Subgroup Analysis of Outcomes by Lesion Location and Concomitant TTO
Patient outcomes were compared based on lesion location (MFC vs. LFC vs. trochlea vs. patella) and concomitant TTO. KOOS scores did not differ significantly based on lesion location (P > 0.05). However, patients with MFC lesions reported higher KOOS symptom subscores than patients with trochlear lesions (86.9 vs. 65.0, P = 0.05), which neared statistical significance. In addition, no significant differences were found with regard to pain, satisfaction, TSK-11 or PCS scores, or RTS rates among patients based on lesion location (P > 0.05). Patients who underwent a TTO reported significantly lower RTS rates than non-TTO patients (50% vs. 87.5%, P = 0.03) and larger defect size (mean = 3.6 cm2 vs. 2.7 cm2, P = 0.02). Pain, satisfaction, and clinical outcomes were not significantly different among groups (P > 0.05). Notably, the distribution of TTO and non-TTO patients was also not significantly different when comparing patients who return to sport to those that do not (77.3% vs. 51.4%, P = 0.095).
Relationship between TSK-11/PCS and Outcomes
Increased TSK-11 scores were associated with lower odds of returning to sport. A logistic regression model controlling for age, sex, and BMI found that for every point increase in TSK-11 score, the odds of RTS decrease by a factor of 0.8 (95% CI OR [0.70-0.93], P = 0.003). TSK-11 was a significant predictor of KOOS subscores including KOOS-Symptom (β = 1.48), KOOS-sport (β = 2.81), KOOS-QOL (β = 3.50), and KOOS-pain (β = 1.57; P = 0.01, P = 0.03, P = 0.03, and P < 0.001, respectively). A subsequent bivariate analysis found a negative correlation between TSK-11 and all KOOS subscores, as well as between PCS and all KOOS subscores (
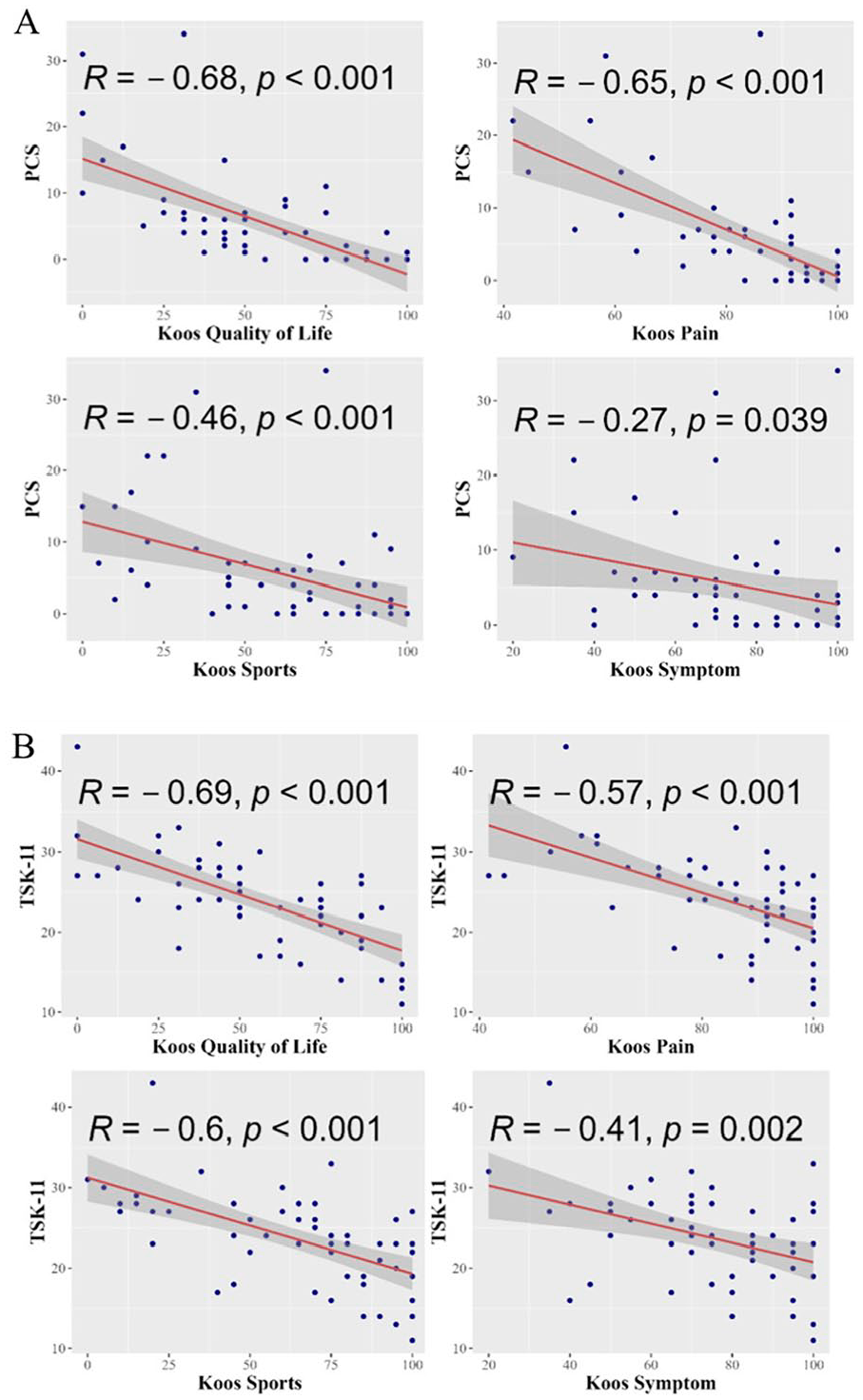
Scatter plots depicting correlations of fear of reinjury (TSK-11) and pain catastrophizing (PCS) with patient-reported outcomes. (
Return to Work
Prior to surgery, 44 (77.2%) patients were employed, and of those, the most common duties included desk and office work (56.8%). Prior to surgery, 18 (40.9%) patients took time off work, most commonly (44.4%) for >20 days. Of those who were employed before injury, 43 (97.7%) returned to work, with the majority ultimately returning at the same level of function (n = 34, 73.9%). Thirty-seven (84.1%) patients returned to modified work within 6 months of surgery and had significantly lower TSK-11 scores (23.32 vs. 29.20, P = 0.04) than patients who returned to work more than 6 months after the operation. Most patients (n = 36, 80%) returned to modified work within 3-4 months, and 82.6% (n = 38) resumed full work duty within 1 year.
Discussion
The most important finding of this study is that patients who report elevated levels of kinesiophobia and pain catastrophizing do not return to preinjury level of sports participation and have worse clinical knee outcomes and pain intensity compared to patients who return to their preinjury level of sport. Higher levels of fear of movement and reinjury decrease the odds of returning to sport and were negatively correlated with functional knee measures. Despite this variation in return to preinjury level of sport, nearly all patients returned to work at full capacity. Collectively, these findings support that psychological factors have a significant impact on postoperative return to sport participation and clinical outcomes and minimal effect on RTW status following MACI or ACI surgery.
Our findings showed a modest decrease in RTS rate (61%) as compared to previous studies with a similar discrepancy between levels of sport participation.7,8,16 For example, a systematic review by Campbell et al. 16 found an overall 85% rate of RTS. However, the mean percentage difference between those that returned to sport overall (including at a lower level) and those that returned to their preinjury level was 11.5%, which is consistent with our study results (10%). Notably, all but one patient in this study that was employed prior to surgery returned to work, and at least 86% (n = 38) returned at the same level of work capacity or higher. Individuals in this study had a relatively quick RTW at a modified or full work capacity. This is in accordance with a recent systematic review that described a close to 100% rate of RTW after evaluating 277 patients that underwent ACI. 24 These findings may further be explained by the mainly sedentary work and absence of heavy labor involved in the job descriptions (nearly 60%) of the patients in this study. More physically demanding jobs may increase the time elapsed until complete RTW is resumed. 25
Patients that did not return to sport had significantly higher levels of pain-related fear of movement and reinjury, as indicated by their higher TSK-11. The negative association of both RTS and KOOS scores with TSK-11 scores supports that patient psyche may substantially deter patients from reaching their optimal physical performance. Consistent with these data, Thoma et al. 10 evaluated 35 patients undergoing articular cartilage restorative procedures (osteochondral allograft [OCA] and ACI) and reported higher fear of reinjury and pain catastrophizing in patients with ACDs than in a control group without knee pain. They similarly described negative associations between TSK-11 scores and 4 of 5 KOOS subscales. Moreover, upon comparing the TSK-11 and PCS scores of patients with ACDs to the average scores of populations affected by ACL injury, patellofemoral pain syndrome, osteoarthritis, and total knee arthroplasty, it was reported that the ACD patients exhibited comparable scores. Notably, the scores observed in the ACD group were among the highest, which reinforces the findings in our study. Our findings, in conjunction with the aforementioned evidence, offer additional support for the notion that fear of reinjury and pain catastrophizing can hinder patients from achieving their preinjury sports participation level.
Despite the paucity of data regarding psychological determinants of postoperative sport and function following ACDs, much can be drawn from published ACL-reconstruction data given many similarities between the two patient populations.9,11-14 Linkable concepts of behavioral decision-making may be explained by the fear avoidance model. This model identifies pain catastrophizing after injury as the impetus to the formation of a cyclical pattern of negative affect and thoughts. 26 The proposed paradigm is a sequential series of negative thoughts that begins with the inciting painful event, followed by aggrandization through pain catastrophizing actions which leads to pain-related fear, avoidance, hypervigilance, and eventually disuse, depression, and disability.
A systematic review by Trinh et al. 27 compared outcomes of 366 patients that underwent either an isolated ACI or a combined ACI and patellofemoral osteotomy. In their cohort, individuals with a concomitant osteotomy reported significantly higher improvements in multiple outcome scores. We did not observe a similar trend in our study, where outcomes did not differ significantly based on the presence of a co-occurring TTO. However, we observed a significantly lower RTS rate among patients that underwent a concomitant TTO (50% vs. 87.5%, P = 0.03). RTS status was not reported in the aforementioned study, which limits comparison. In this study, reported levels of pain and satisfaction after surgery were not significantly different between those that underwent TTOs and those that did not. In addition, the distribution of patients that underwent TTOs did not differ significantly when comparing patients by RTS status (return to sport vs. no return to sport), which suggests consideration of additional factors that may influence sport participation.
The most common physical reason cited for not returning to sport or returning to sport at a lower level was pain in the knee. Nielson et al. 28 similarly reported pain as a chief deterrent in 47% of patients after OCA transplantation. Additional published data evaluating specific reasons why individuals do not return to sport after cartilage defects are limited. Nonetheless, pain has been described as the principal reason for not returning to play after ACL surgery, as well as other orthopedic surgeries.29,30 In this study, the same individuals that did not return to sport also had significantly higher pain catastrophizing scores than those that did return. It is important to note that pain catastrophizing scores were also positively correlated with pain levels. For this reason, consideration of the degree to which reported pain levels can overrepresent actual or perceived pain in those with higher pain catastrophizing scores is paramount to accurately assess clinical outcomes.
To our knowledge, this is the first study to use psychometrics to evaluate the influence of kinesiophobia on the ability to return to preinjury sports participation after ACI and MACI. Our findings support a call for designing, implementing, and validating screening tools that help identify patients that may benefit from additional support throughout their rehabilitative course. Based on our data, the TSK-11 and PCS can successfully be used as part of this process. Nonetheless, the creation of a specific screening tool for cartilage injuries would be concordant with the use of the ACL-RSI to evaluate an athlete’s confidence, emotion, and risk appraisal when returning to sport after ACL injury. 31 An additional strength to this study is that it is one of few that details the primary reasons for patients not returning to sport. Recognizing these salient factors can potentiate targeted therapeutic interventions for future patients. For example, if patients that score high in measures of pain-related activity avoidance also tend to report fear of reinjury as their primary obstacle to returning to sport, installment of progressive graded exposure to athletic positions and movements during rehabilitation may prove beneficial. On the other hand, if patients that score high in pain catastrophizing also report pain as the primary reason for not returning to sport, implementation of cognitive behavioral therapy may improve thought restructuring and limit the execution of maladaptive behaviors. 32 Lastly, this study provides valuable information regarding rates of RTW, which is rarely reported in this population. This may improve managing expectations regarding expected work-related functional limitations, financial insecurities that may arise during the recovery period, and surgical planning.
We recognize that this study is not without limitations. First, there lies a possibility of inherent selection bias given the retrospective nature of this study. We achieved a 71% questionnaire response rate, which may not fully represent the outcomes of all eligible patients. This may influence our study results if patients self-selected to participate as a result of poor or superior postoperative outcomes. This can potentially bias our findings by skewing sample sizes and psychometric findings of patients that returned to sports and those that did not. Thus, a randomized controlled trial assessing psychosocial factors prospectively is preferred. In addition, information on time to return to work and the level at which patients returned was based on patient recollection, which can introduce recall bias. Although we used validated psychometric tools, we acknowledge that these may not fully assess the complexity of psychosocial components mediating clinical outcomes. Despite the validity of the questionnaires used for assessing outcomes, the strict structure of the answers may not fully allow patients to report their experiences. To mitigate this, we added an open text box at the end of the questionnaire where patients that desired to elaborate on their unique experience had the opportunity to do so.
The abilities to return to sport and work following injury have been described as important predictors of patient satisfaction. 33 Therefore, further studies evaluating the relationship between preoperative psychological measures and self-reported expected outcomes after surgery with RTS and clinical function in patients with ACDs are needed. Furthermore, prospective studies utilizing standardized screening tools to guide clinical intervention before surgery, during rehabilitation, and immediately before sport participation for patients with ACDs may be warranted to maximize the likelihood for complete return to sport.
In conclusion, this study highlights the role of kinesiophobia and pain catastrophizing in the formation of deleterious thought patterns that may hinder optimal mental confidence required before returning to preinjury sport. In addition to decreased rates of RTS, patients grappling with these psychological challenges also experience inferior clinical outcome scores. However, nearly all were able to return to full work duty.
Supplemental Material
sj-docx-1-car-10.1177_19476035231183256 – Supplemental material for Kinesiophobia and Pain Catastrophizing Leads to Decreased Return to Sport Following Autologous Chondrocyte Implantation but Does Not Affect Return to Work
Supplemental material, sj-docx-1-car-10.1177_19476035231183256 for Kinesiophobia and Pain Catastrophizing Leads to Decreased Return to Sport Following Autologous Chondrocyte Implantation but Does Not Affect Return to Work by Jairo Triana, Naina Rao, Michael Buldo-Licciardi, Ariana Lott, Nicole D. Rynecki, Jordan Eskenazi, Michael J. Alaia, Laith M. Jazrawi, Eric J. Strauss and Kirk A. Campbell in CARTILAGE
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JT, NR, MB-L, AL, NDR, and JE report no conflict of interest. MJA is a board or committee member in AAOS, editorial or governing board member in Arthroscopy, board or committee member in Arthroscopy Association of North America, a paid consultant for BodyCad, editorial or governing board member of the Journal of Cartilage and Joint Preservation, paid consultant for JRF Ortho and Mitek, receives research support from Orcosa, Inc, and publishing royalties, financial, or material support from Springer. LMJ receives research support from Arthrex, Inc, is an editorial or governing board member of Bulletin for the Hospital for Joint Diseases, editorial or governing board member of JBJS Reviews, receives research support from Mitek and Smith & Nephew, publishing royalties, financial, or material support from Wolters Kluwer Health—Lippincott Williams & Wilkins. EJS is a board or committee member of AAOS and American Orthopedic Association, paid consultant, paid presenter, or speaker for Arthrex, Inc, board or committee member of Arthroscopy Association of North America, has stock or stock options in Better PT, receives research support from Cartiheal, is in the editorial or governing board of Cartilage and Bulletin of the Hospital For Joint Diseases, receives research support from Fidia, is a paid consultant for Flexion Therapeutics, receives publishing royalties, financial, or material support from Jaypee Publishing, is a paid consultant for Joint Restoration Foundation, is a paid consultant, paid presenter, or speaker and receives research support from Organogenesis, is a paid consultant, paid presenter, or speaker for Smith & Nephew, receives publishing royalties, financial, or material support from Springer, is a paid consultant for Subchondral Solutions, and is a paid consultant, paid presenter, or speaker for Vericel. KAC is a board or committee member for AAOS and Arthroscopy Association of North America and receives research support from Stryker.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.