
Abstract
Objective. The aim of this work was to study the short- and mid-term effectiveness and safety of high-density autologous chondrocyte implantation (HD-ACI) in the first 50 patients with knee cartilage damage treated in our unit. Design. Fifty consecutive patients with cartilage lesions (Outerbridge grade III-IV) in the knee treated with HD-ACI were included in this study. Chondrocytes were isolated from a nonbearing cartilage area biopsy and were cultured until 40 to 50 million cells were obtained. Five million chondrocytes per cm2 of a porcine collagen type I/III membrane were implanted covering the defect. Procedure effectiveness was assessed by evaluating pain, swelling, and range of mobility (flexion and extension) at 6-, 12-, and 24-month follow-up. The International Knee Documentation Committee (IKDC) subjective evaluation form was used to evaluate symptoms and functions of the knee. Results. The percentage of patients with pain and swelling decreased progressively in the following visits, with differences being statistically significant (P < 0.001 and P = 0.040, respectively). IKDC scores improved progressively throughout the 24-month follow-up (P < 0.001). Thus, the mean IKDC score improvement was 26.3 points (95% confidence interval [CI] = 18.2-34.4 points) at 12 months and 31.0 points (95% CI = 22.9-39 points) at 24 months. No significant differences were found when performing extension (P = 0.112). Flexion significantly improved by 25.1° at 24-month follow-up (P = 0.013). Conclusions. HD-ACI is a safe and effective technique for the treatment of cartilage defects, improving clinical and subjective perception of knee functionality. These preliminary results encourage future studies comparing this technique with traditional ACI.
Introduction
Articular cartilage has a poor capacity for self-repair after a lesion due to its characteristics: It is an aneural, avascular, and alymphatic tissue. It is a special connective tissue, which is located in long bones, covering the articular surfaces of their ends. Great efforts have been made for many years in order to find an effective treatment for repairing cartilage defects due to their relatively high prevalence.1,2 In this sense, different procedures for cartilage repair have been developed. 3 There are some methods, which are also called “marrow stimulating” techniques, like abrasion, 4 drilling, 5 or microfractures 6 that are based on the stimulation of the mesenchymal stem cells (MSCs) from the underlying bone marrow. All of them result in the formation of a blood clot, which contains MSC that are implicated in the cartilage repair. However, these methods lead to the synthesis of a type-I collagen-rich fibrocartilaginous tissue unable to restore the functional characteristics of the original articular cartilage: hyaline cartilage with a type II collagen high content. 3 Other technique called mosaicplasty, is based on the transplantation of an osteochondral fragment from autologous or allogenic origin and is mainly recommended for cartilage lesions of less than 1 cm2. 7
The functions of a highly specialized tissue like hyaline cartilage could hardly be restored or even mimicked by another tissue like fibrocartilage. In the past decades, cell-based therapies have been developed in order to address this issue. Nowadays, autologous chondrocyte implantation (ACI) is the only cell therapy able to generate hyaline cartilage or hyaline-like cartilage. 8 It was first described in 1994 9 and many data about the long-term clinical benefits of this technique have been published.10,11 The original ACI technique was carried out with 20 million cultured chondrocytes suspended in liquid medium, which were then were implanted on the defect (independently of its size) under a periosteum flap. 9 Despite its good results, a high morbidity is associated to this technique due to the hypertrophy of the graft sometimes leading to a rescue surgery.12,13 This technique evolved into a new one called MACI (matrix-induced autologous chondrocyte implantation) consisting of the use of a porcine-derived type collagen I/III membrane as a carrier to deliver the chondrocytes to the cartilage lesion.14,15 In this technique, a 4 × 5 cm membrane is seeded with 20 million chondrocytes (1 million cells per cm2). Subsequently, the membrane is cut to fit the defect size and shape and fixed to the adjacent bone using both suture and fibrin-based glue. With the previous traditional ACI, all the cells obtained after the culture were implanted but with MACI only a part of the cultured chondrocytes are used for the implant and the remaining are discarded.
We hypothesized that maybe an increase in the cell density could improve the defect fill. For this reason, we started working on a new approach consisting in the use of the same membrane used in MACI but with high-density chondrocytes. In this sense, the ovine model was used to compare the histological and molecular features of the repaired tissue after MACI (1 million cells per cm2) or high-density autologous chondrocyte implantation (HD-ACI) (5 million cells per cm2). 16 Although repaired tissue in both cases was quite similar to the control (normal cartilage), the tissue synthetized after the HD-ACI was histologically more similar to the control than the tissue synthetized after MACI treatment. Moreover, the amount of type II collagen and aggrecan was closer to the control after HD-ACI rather than after MACI treatment. 16
We designed the procedure to treat the patient’s lesions with HD-ACI as follows: during the second surgery, the lesion surface area is measured and the membrane is cut according to the shape and size of the lesion. The chondrocytes are seeded onto the membrane to achieve 5 million cells per cm2 density and the membrane with the chondrocytes is attached to the defect. Since 2010 we have been treating patients with cartilage defects in the knee following this method and we have planned to study the short and mid-term effectiveness and safety of the HD-ACI in the first 50 patients who fulfilled the inclusion/exclusion criteria described in the next section.
Material and Methods
This prospective cohort study was performed on 50 consecutive patients with cartilage lesions in the knee treated with HD-ACI. All the patients signed an informed consent and the study was approved by the Education and Research Committee of the hospital. To be included in this study, patients must have: Outerbridge grade III-IV cartilage lesion in the knee (femoral condyles, trochlea, tibial plateau, or patella), diagnosed by an imaging test (X-ray, magnetic resonance, or arthroresonance), 1 to 4 lesions of at least 1 cm2 in size and age ranging from 18 to 55 years. Exclusion criteria from the study were: arthrosis, specular lesions (femoral condyle and tibial plateau from the same side), misalignment of the limb (more than 10° varus or valgus), meniscal lesions, allergy to penicillin and/or streptomycin, hypersensitivity to bovine-derived products, active infection, tumoral pathology, and systemic diseases such as rheumatoid arthritis or other autoimmune diseases with articular involvement. We included the first 50 patients fulfilling the inclusion/exclusion criteria who had had 2 years of follow-up, so a sample of convenience was used to perform this study.
After diagnosing the chondral lesion(s), a cartilage biopsy from a nonbearing area (medial condyle) was taken, placed in Dulbecco’s modified Eagle medium (DMEM; Lonza Group Ltd., Basel, Switzerland) and immediately processed in a sterile GMP (Good Manufacturing Practice) certified room, approved by the Spanish Health Authorities. Chondrocytes were isolated after digestion with 1 mg/ml collagenase A (Roche Diagnostics GmbH, Mannheim, Germany) at 37°C overnight. The cells were cultured in DMEM supplemented with 10% of autologous serum,
Our technique consists in implanting high-density chondrocytes in a resorbable porcine collagen type I/III membrane (Chondro-Gide, Geistlich Biomaterials, Wolhusen, Switzerland) in a second surgery. During this surgery, each chondral defect was debrided and measured to cut the membrane according to their size and shape. Cells resuspended in DMEM were seeded onto the membrane at a rate of 5 million cells per cm2 of lesion. After 10 minutes, and once the cells had been adsorbed onto the membrane, the membrane was sutured to the adjacent bone and sealed to the injury using Tissucol (Baxter, Madrid, Spain). To avoid any variability in the technique, all surgical procedures were performed by the same surgeon.
Effectiveness of the treatment was assessed by evaluating the pain, the presence of swelling, and the range of mobility (flexion and extension) at 6-, 12-, and 24-month follow-up. To detect any improvement or deterioration in symptoms and functions, the International Knee Documentation Committee (IKDC) subjective evaluation form was used in the basal visit, at 12 and 24 months.
The statistical analysis was carried out using the IBM SPSS Statistics version 22.0.0. software. Quantitative variables were expressed as the mean or the median as central tendency measure. Dispersion of these variables was expressed as the standard deviation, the range, or the 95% confidence interval (CI) of the mean. Normality of quantitative variables was checked with the Kolmogorov-Smirnoff test. Means were compared using the Mann-Whitney U test (nonparametric) or the Student t test (normal distributed variables). Comparison of IKDC score at different moments in time was performed using the Friedman’s nonparametric test for related samples. Pairwise comparisons were performed using the Wilcoxon signed-rank test for related samples. No sample size calculation was performed since the study was performed with the first 50 patients fulfilling the inclusion/exclusion criteria. Instead, post hoc power estimation was carried out using the G*Power 3.1.9.2 software. 18 Categorical variables were expressed with the absolute frequency and the percentage. The evolution of these variables along the follow-up period was studied using cross-tabs, whose statistical significance was determined using Pearson’s χ2 test. All hypothesis contrasts were bilateral and a P value <0.05 was considered as statistically significant.
Results
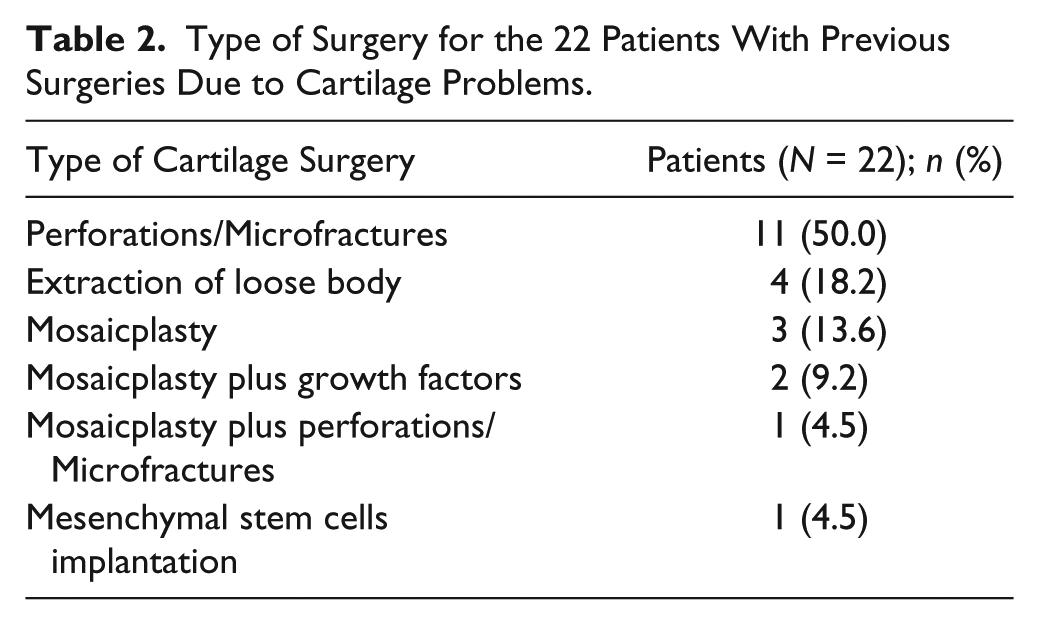
The demographic characteristics of the 50 patients included in the present study are depicted in Table 1 . The median age of the patients was 35 years (range 18-49 years) and the most frequent diagnosis was chondral lesion. As shown in Table 1 , most patients had 1 previous surgery. In 22 (44%) of the 36 patients with previous surgeries, these surgeries were due to cartilage problems, being bone marrow stimulation techniques (perforation/microfractures) the most frequent previous cartilage surgery performed: 11 of the 22 (50%) patients with one previous cartilage surgery and 1 patient underwent this technique as well as mosaicplasty ( Table 2 ). The number of lesions and the mean sizes are shown in Table 3 . Thirty-four patients had only 1 lesion (68%), 12 patients had 2 lesions (24%), 3 of them had 3 lesions (6%) and 1 patient had 4 lesions (2%) ( Table 3 ). In most patients, cell implantation was carried out by open surgery ( Fig. 1A ) and the elapsed time between biopsy collection and chondrocyte implantation was 6.43 weeks (range 6-35 weeks) ( Fig. 1B ).
Demographic Characteristics of Patients Included in the Study (N = 50).
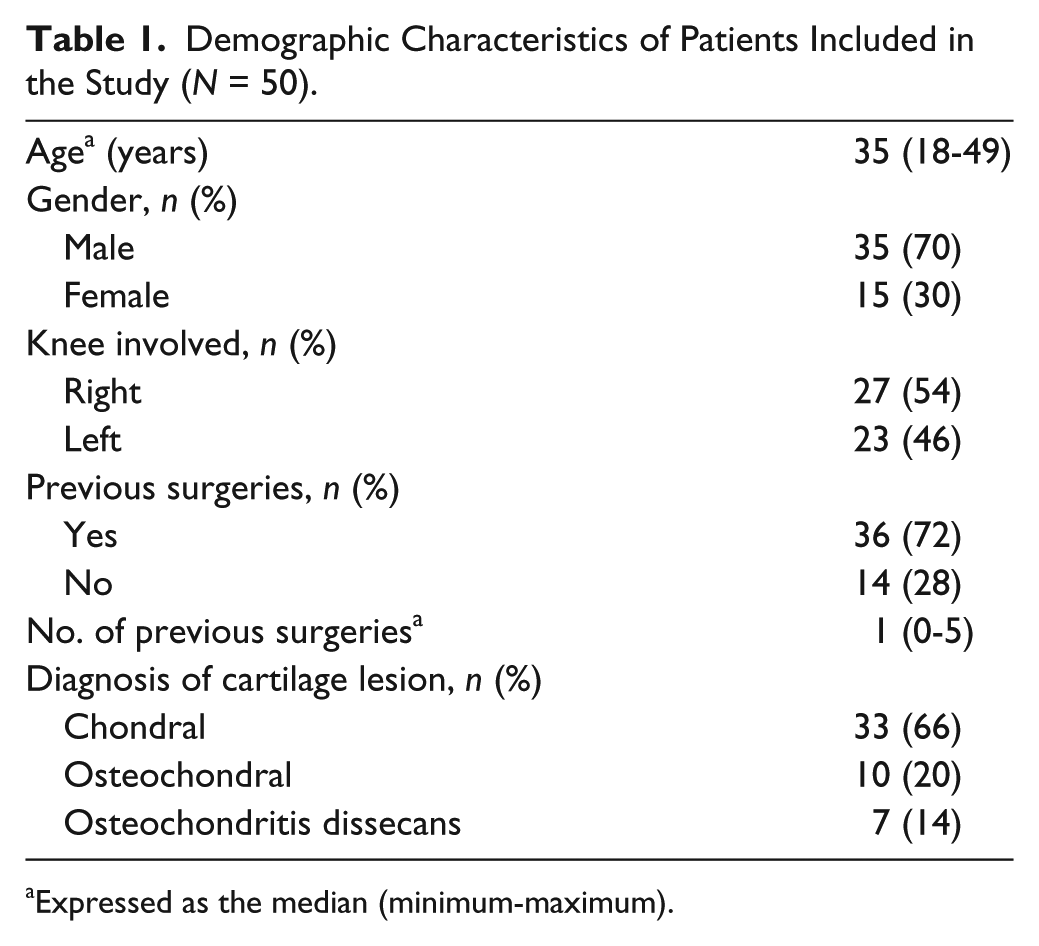
Expressed as the median (minimum-maximum).
Type of Surgery for the 22 Patients With Previous Surgeries Due to Cartilage Problems.
Location and Size of the Chondral Lesions in the Patients Included in the Study.
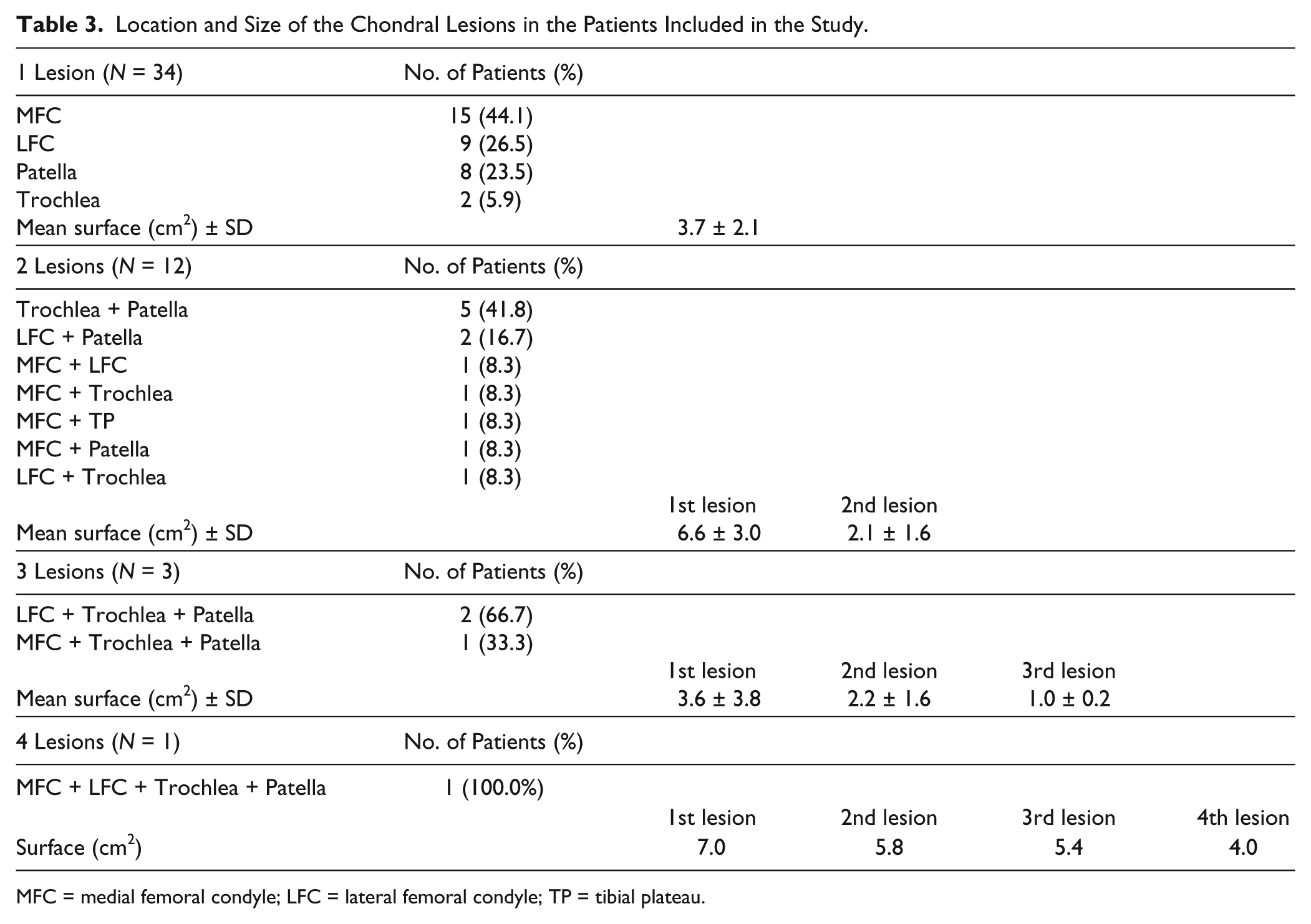
MFC = medial femoral condyle; LFC = lateral femoral condyle; TP = tibial plateau.
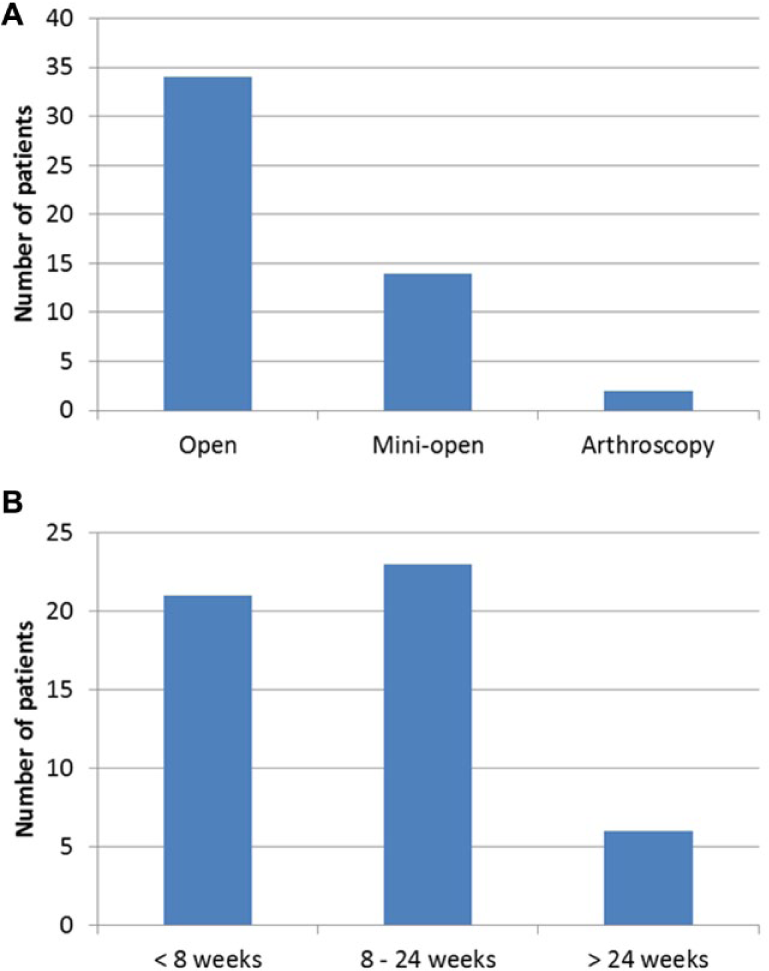
Frequencies of surgical procedures of chondrocyte implantation (
Evolution of pain, swelling, and mobility (flexion and extension) from the basal visit to 6, 12, and 24 months was studied. Results are collected in Table 4 . At the basal visit, all patients suffered pain and the percentage of patients with pain significantly decreased in following visits: 50 patients (100%) at the basal visit, 18 (36%) at 6 months, 17 (34%) at 12 months and 11 patients (22%) at 24 months (P < 0.001; Pearson χ2 test) ( Table 4 ). The percentage of patients with swelling significantly decreased from the basal visit compared with the 6-month follow-up and remained stable until the 24-month follow-up: 8 patients (16%) in the baseline and 2 patients (4%) at 6-, 12-, and 24-month follow-up (P = 0.040; Pearson χ2 test) ( Table 4 ). With respect to mobility, no statistical significant differences were found in extension ( Table 4 ). Nevertheless, all patients showed complete extension at the 24-month follow-up (P = 0.112; Pearson χ2 test). In the case of flexion, statistically significant differences were found in the follow-up period, improving by 23.1° from the basal visit (P = 0.013; Pearson χ2 test).
Evolution of Pain, Swelling, and Mobility from the Basal Visit Until 24-Month Follow-up.
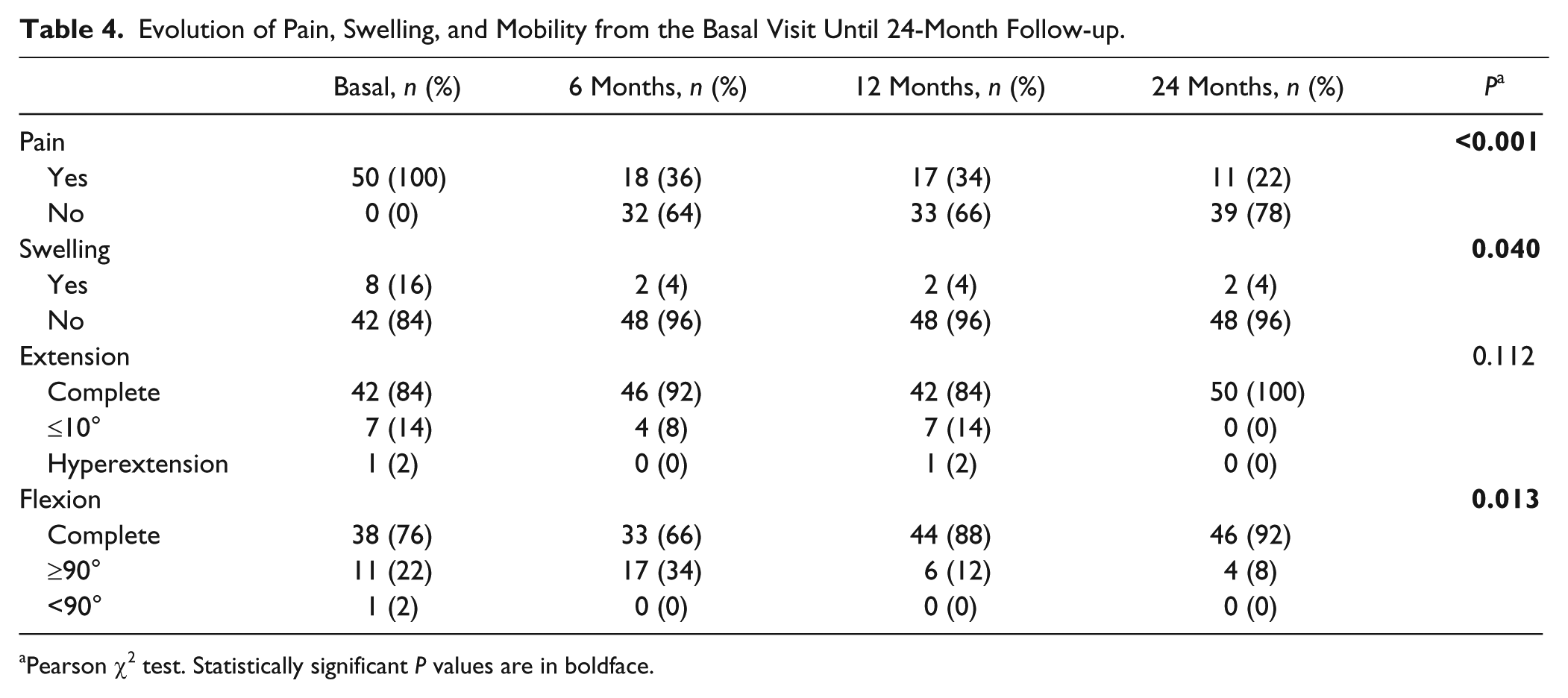
Pearson χ2 test. Statistically significant P values are in boldface.
Knee symptoms and functions, measured using the IKDC questionnaire, showed a significant improvement when basal, 12-month, and 24-month follow-up visits were compared (P < 0.001; Friedman’s test for related samples) ( Fig. 2 ). The estimated post hoc power for this comparison was 94%. In all pairwise comparisons the estimated post hoc power was 95%. Thus, as shown in Figure 2 , the IKDC basal score was 38.6 points (95% CI = 32.9-44.3 points) and increased to 65.2 (95% CI = 58.6-71.8 points) at 12 months and to 69.6 (95% CI = 63.0-76.1 points). All pairwise comparisons were also statistically significant, indicating that IKDC scores improved progressively from the basal visit until 24-month follow-up (P < 0.001 in all pairwise comparisons; Wilcoxon signed-rank tests). Thus, the mean IKDC score improvement from the basal visit was 26.3 points (95% CI = 18.2-34.4 points) at 12 months and 31.0 points (95% CI = 22.9-39 points) at 24 months.
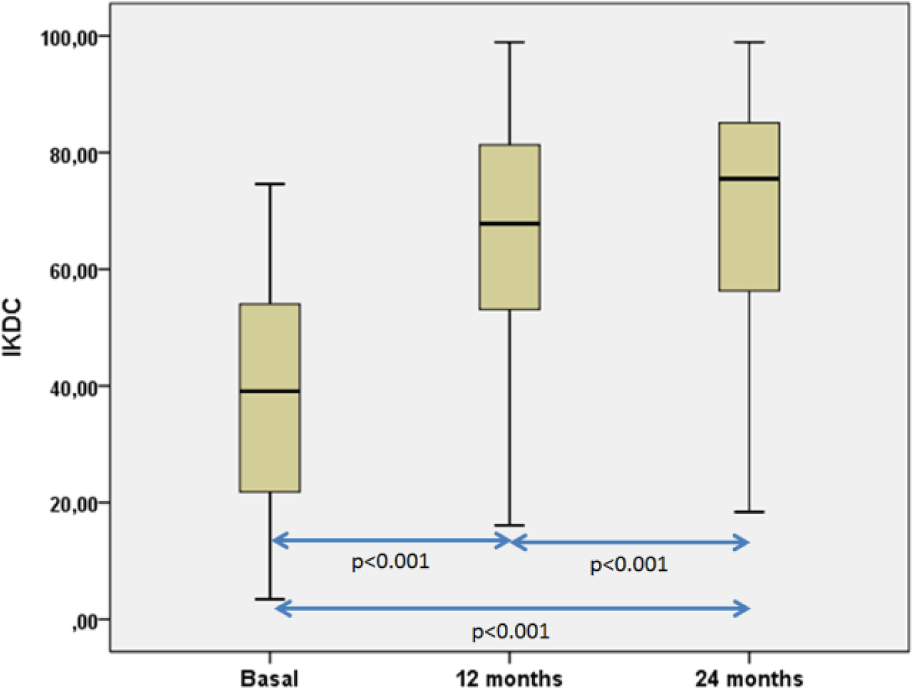
Boxplot representations of the evolution of International Knee Documentation Committee (IKDC) scores. We have found statistically significant differences when all IKDC were compared (P < 0.001; Friedman’s test for related samples). Pairwise comparisons were also statistically significant (P < 0.001 in all the pairwise comparisons; Wilcoxon signed-rank test).
In order to study the influence of having previous microfractures in the patients’ evolution, the mean IKDC score of both subgroups along the treatment was compared. No statistical differences in between patients with or without previous microfractures were found in the basal, 12-month, and 24-month visits (P = 0.497; Mann-Whitney U Test) ( Fig. 3 ). The estimated post hoc power for this comparison was 10.4%.
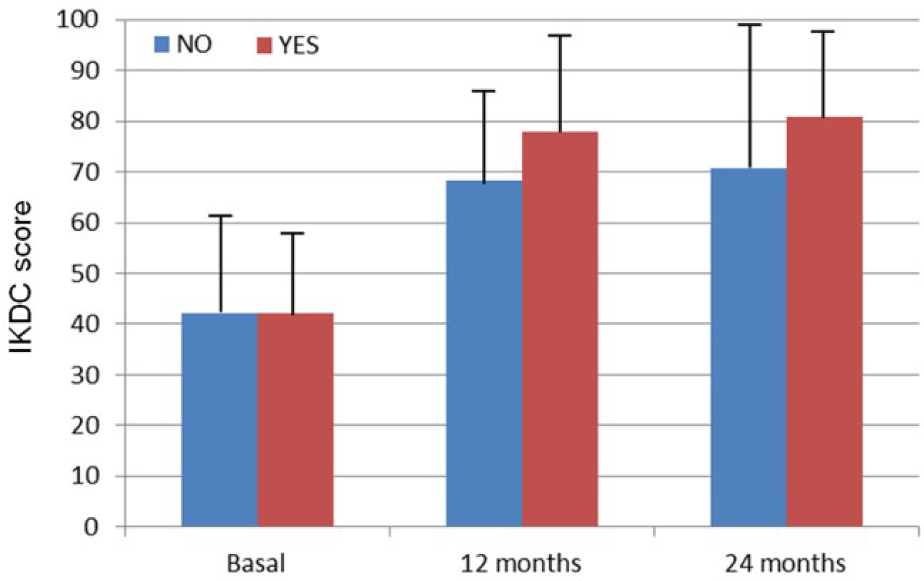
International Knee Documentation Committee (IKDC) scores in patients with or without previous microfractures in the basal, 12-month, and 24-month follow-up visits. No statistically significant differences were found between both groups in any visit (P > 0.05; Mann-Whitney U test).
Discussion
Here, we report the use of this treatment based on the 5-fold increase in cell density compared with the traditional MACI in 50 patients with cartilage defects in the knee. In order to be eligible for our treatment, patients could not be older than 55 years (our patients have a median age of 35 years) similar to the age of patients treated in other studies.3,19 In a relatively high number of our patients, chondrocyte implantation was not the first treatment option to treat their cartilage defects, so they were first treated with bone marrow stimulation techniques such as drilling or microfractures. These techniques together with others such as mosaicplasty are mainly recommended to treat cartilage defects smaller than 1 cm2 but ACI should be considered when the former techniques fail. 3 In fact, the defects of patients included in this study are focal lesions and had a mean size higher than 1 cm2. As a consequence, these became candidates to receive a chondrocyte implantation following our own criteria and those published by other authors.20,21 More than a half of our patients (34 out of 50) underwent an open surgery. This relatively high number of patients is related to the number of those having more than 1 lesion or to the location of the cartilage defects, which may limit the access by arthroscopy or mini-open surgery.
A mean IKDC score improvement of 26.6 points at 12 months and 31.0 at 24 months was observed in our patients, On the other hand, it has been published that the minimum clinically important difference in the IKDC is 16.7 point at 12 months. 22 This result means that the patients perceive a real clinical improvement 12 months after HD-ACI implantation. Our results about the mean IKDC improvement are in agreement with that found by other authors with ACI and MACI.23-26 In fact, Cvetanovich et al. 23 have recently reported a mean improvement of 29.7 points in adolescent patients treated with ACI, after a mean follow-up period of 4.6 years. Recently, a systematic review in patients treated with ACI at a mean follow-up period of 11.4 years has been published. 24 In this study, the authors report a slightly lower but significant improvement in the IKDC score of 16.5 points. 24 Similar results have been found by Kreuz et al. 25 in patients treated with MACI, obtaining an improvement of 25.0 points after a 48-month follow-up period. In another study performed in patients treated with MACI, Niethammer et al. 26 have reported a mean IKDC score improvement of 18.7 after 3-year follow-up.
Although our results are similar to those of other authors, a comparative study between MACI and HD-ACI should be carried out in order to address the extent to which a treatment is more efficient than the other. Since our results in the sheep animal model indicate that any novel tissue synthesized after HD-ACI was more similar to the healthy cartilage than to that obtained after low-density chondrocyte implantation as occurs with MACI. 16 A study including histological assessment of the novel tissue would be useful to address this question. However, the performance of such study will be difficult due to ethical reasons. Future studies comparing HD-ACI with ACI and MACI and cartilage fill and quality evaluation after HD-ACI implantation, including MRI and T2 mapping are currently ongoing.
A relatively high percentage of our patients (22%) had had microfractures prior to the HD-ACI implantation. It has been published that the risk of graft failure increased in patients with previous bone marrow stimulation techniques. 27 Surprisingly, no differences between patients with or without previous microfractures have been found in our patients. Moreover, the mean IKDC scores between both groups did not differ. This study was not designed to compare both groups and the lack of differences could be explained by a small sample size. In fact, post-hoc analysis showed that the power for this analysis was only 10.4%, suggesting that the number of patients were not enough to detect statistical differences between both groups. A study comparing patients with or without previous microfractures with a higher sample size will be performed in the future.
The pain, swelling, and the flexion of the operated limb improved from the basal to 24-month follow-up. Extension of the affected leg improved at 24 months although the result was not statistically significant. Taken as a whole, these results indicate that chondrocyte implantation improves the clinical outcome of patients with cartilage defects. Furthermore, these results are supported by the fact that the IKDC index increased progressively from the basal to 24-month follow-up, indicating that patient’s subjective perception on the functionality of their knees improved with treatment. Our results are in agreement with those published by other authors concerning the effectiveness of autologous chondrocyte implantation.28-30
Our study has some limitations. First of all, as stated above, neither a second-look sample nor an image study was performed to assess the quality of the novel tissue synthesized or the cartilage filling after the implantation. The inclusion of a group of patients treated with MACI would be useful to compare the effectiveness of our technique with others. Finally, it would be desirable to include patients with a more homogeneous clinical history. In spite of the limitations, our results demonstrate that HD-ACI is a safe and effective technique in the treatment of cartilage defects, improving clinical and subjective perception of knee functionality.
Footnotes
Acknowledgments and Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study has been supported by Fundación Dr. Pedro Guillén.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was obtained from the Education and Research Committee of the Clínica CEMTRO.
Informed Consent
Written informed consent was obtained from all subjects before the study.
Trial Registration
Not applicable.