
Abstract
Objective
Osteochondral allograft transplantation (OCA) is a well-established procedure for patients with symptomatic cartilage defects in the knee. Revision to OCA after prior failed cartilage repair has shown similar clinical outcomes as primary OCA; however, most of the failed procedures were arthroscopic procedures for smaller defects. There is no literature investigating the clinical outcomes after OCA for prior failed autologous chondrocyte implantation (ACI) for the treatment of large chondral defects of the knee. The purpose of this study was therefore to determine clinical outcomes of patients undergoing revision to OCA after prior failed ACI as compared with a matched cohort of patients undergoing OCA as a primary cartilage repair procedure (primary OCA).
Design
In this review of prospectively collected data, we analyzed data from 26 patients with at least 2 years follow-up. Thirteen patients who underwent revision to OCA after prior failed ACI by a single surgeon were compared with a matched group of patients who underwent primary OCA. The patients were matched per age, gender, body mass index, and defect size. Patient-reported outcomes, reoperations, and survival rates were compared between groups.
Results
There were no significant differences in patient-reported clinical outcome scores between the groups at final follow-up. Moreover, there was no significant difference in reoperation rates and survival rates between the groups.
Conclusion
The present study demonstrates that revision to OCA is a viable treatment option with favorable functional outcomes and similar reoperation and survival rate as primary OCA even for revision of large chondral defects previously treated with ACI.
Keywords
Introduction
Cartilage damage can lead to persistent symptoms including swelling, pain, loss of function, and may ultimately progress to symptomatic degeneration of the joint. 1 Articular cartilage has limited inherent capacity for spontaneous healing after injury; thus, symptomatic, full-thickness articular cartilage defects are difficult to manage especially in the young, high-demand patient population. 2 To delay or avoid a prosthetic arthroplasty, multiple treatment options are available to restore the injured cartilage depending on patient and lesion characteristics including drilling, abrasion arthroplasty, microfracture, osteochondral autograft transplantation (OAT), osteochondral allograft transplantation (OCA), and autologous chondrocyte implantation (ACI).2,3 Although choosing the proper cartilage restoration procedure is influenced by numerous factors, either marrow stimulation technique or OAT are preferred procedures for small chondral lesions.3-5 In contrast, large full-thickness chondral and osteochondral defects are frequently treated with ACI and OCA resulting in high patient satisfaction rates and significantly improved functional outcomes.3,6-11 Despite low failure rates over a long-term follow-up, especially young patients are at risk for revision surgery.3,5-11 In this situation, choosing the appropriate subsequent surgical intervention is challenging and not clearly determined. Surgeons may either perform a repeat cartilage restoration procedure or total knee arthroplasty.12-16
OCA is a well-established single-step procedure with the ability to restore bone stock and transplant viable chondrocytes within mature hyaline cartilage.15,17,18 Outcomes after OCA for the revision of prior failed non-OCA cartilage repair for smaller defects are similar to primary OCA, while outcomes of revision of a prior failed OCA are worse.10,14-16,18-20 Outcomes of OCA after prior failed ACI remain unclear. Since OCA and ACI are indicated for the same defect size, determining the clinical outcomes of revision to OCA after prior failed ACI is necessary to better define an overall treatment algorithm.
The purpose of this study was to assess the clinical outcomes of patients undergoing revision to OCA after prior failed ACI as compared with a matched cohort of patients undergoing OCA as a primary cartilage repair procedure (primary OCA). We hypothesized that revision to OCA would provide comparable clinical outcomes to those after primary OCA.
Methods
Patient Cohort
Our institutional review board approved this study (2018P000693/PHS), and written informed consent was obtained from all patients at the time they were entered into the database. In this review of prospectively collected data, 112 patients underwent OCA transplantation between September 2012 and February 2016. All procedures were performed by a single surgeon. Of the identified patients, 15 underwent OCA after failed prior ACI procedure. Two patients were lost during the follow-up period. Thus, 13 patients with a minimum of 2 years follow-up were included in this study.
The indications for treatment of cartilage defects with OCA were one or more full-thickness chondral or osteochondral defects of the knee with symptoms matching the defect location. Surgery was indicated in patients who were resistant to nonoperative therapies. Patients were evaluated through a physical examination, radiography, magnetic resonance imaging (MRI), and arthroscopic surgery before treatment with OCA was considered. Contraindications to treatment included inflammatory joint disease, unresolved or recent septic arthritis, metabolic or crystal disorders, or deficient soft tissue coverage. Tibiofemoral malalignment >3° from the neutral mechanical axis into the involved compartment was corrected with concomitant osteotomy. Patellofemoral maltracking was addressed with anteromedialization tibia tubercle osteotomy (TTO) 21 to centralize patellar tracking, and proximal soft tissue balancing (lateral release/lengthening, vastus medialis obliquus advancement, MPFL reconstruction) as necessary to centralize the extensor mechanism.
A case-control study was conducted with a group of 13 patients who underwent primary OCA. These patients were matched individually according to age, gender, body mass index (BMI) and defect size. Patient demographics are summarized in Table 1 . The closest existing match was used for age, BMI, and defect size, but a deviation of 5 years for age, 4.0 kg/m2 for BMI, and 10 mm for defect size was accepted. The groups were matched by an independent reviewer who was blinded to the clinical outcomes of each patient. ACI failure was defined as failure of the graft of more than 25% as judged on postoperative MRI or second-look arthroscopy, repeat cartilage repair, additional surgical MST (marrow stimulation technique) treatment violating the subchondral bone of the treated defect, or prosthetic replacement. The number and type of subsequent surgeries after the OCA transplantation were assessed. The survival rate was assessed using the Kaplan-Meier method, with failure after OCA as outcome endpoint. Patients were evaluated utilizing the Knee injury and Osteoarthritis Outcome Score (KOOS) Pain, KOOS Symptom, KOOS ADL, KOOS Sport/Rec, KOOS QOL, Lysholm, and IKDC.
Patients’ Demographics Comparison between Case and Matched Control Groups.
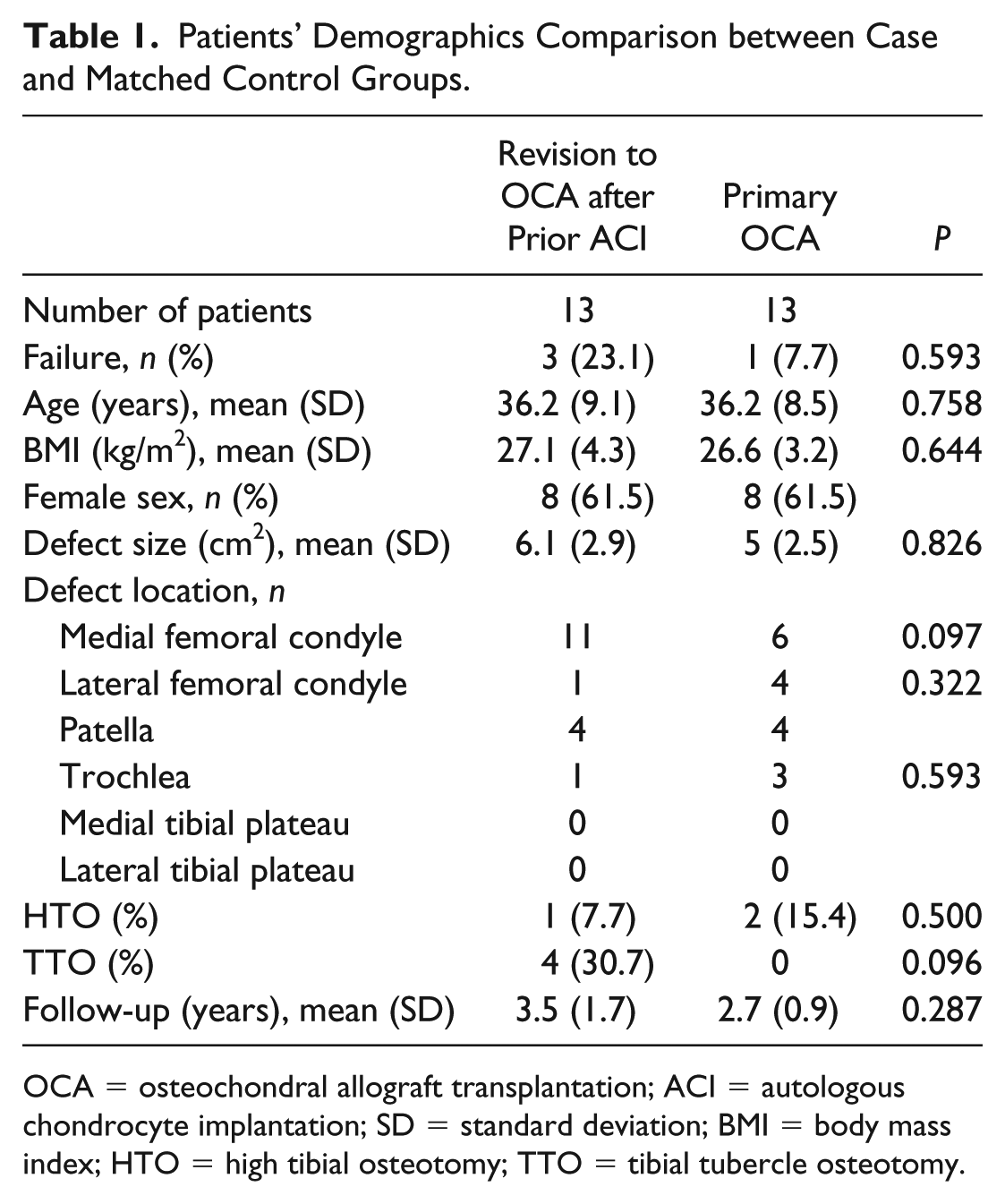
OCA = osteochondral allograft transplantation; ACI = autologous chondrocyte implantation; SD = standard deviation; BMI = body mass index; HTO = high tibial osteotomy; TTO = tibial tubercle osteotomy.
Surgical Procedure
OCA was performed as described in detail previously.22,23 Briefly, after induction of anesthesia, concomitant procedures were performed before OCA if necessary. Mini-parapatellar arthrotomy was performed to visualize the cartilage defect. Any degenerated cartilage as well as fibrous tissue was debrided. The defect was then sized with a sizing guide and an identical sized reamer was used to ream to a depth of approximately 6 to 8 mm using constant cold irrigation. The donor condyle was prepared using the same sizing guide. After harvesting the allograft plug, it was trimmed to the previously measured depths using a sagittal saw. The allograft was then pulse lavaged to remove any remaining marrow elements to decrease immunogenicity. Finally, the graft was placed into the recipient site with manual pressure only, until it was flush circumferentially.
Postoperative Rehabilitation
Postoperative rehabilitation was also described previously. Briefly, protected weight-bearing with knee brace was applied for 4 to 6 weeks, followed by progression to full weight-bearing as tolerated. During this period, patients were permitted to begin unrestricted range of motion exercises, quadriceps sets, straight-leg raises, and patellar mobilization. A stationary bicycle was permitted at 4 weeks. Open chain exercises were not permitted in this first phase. Strengthening was added at the 6-week point and was increased over the next 2 to 3 months. Patients progressed to sport-specific activities by 4 to 6 months after surgery for isolated OCA and by 8 to 12 months for those undergoing concomitant procedures. 10
Statistical Analysis
SPSS (version 21.0; IBM Corp) was used to perform statistical analyses. Demographic results are reported as mean and standard deviation. Descriptive statistics were performed with chi-square or Fisher exact testing, and Mann-Whitney U testing. Survivorship of OCA was calculated utilizing the Kaplan-Meier method. The log rank test was performed to compare survivorship of primary and revision to OCA. Among patients’ intact graft at final follow-up, the Wilcoxon signed-rank test was used to compare differences in functional scores (obtained from KOOS, Lysholm, and IKDC) between the 2 time points (preoperatively and final follow-up). Mann-Whitney U tests were used to compare the improvement in scores between OCA after failed ACI and primary OCA. All statistical tests were 2-tailed. A P value of 0.05 was used to determine statistical significance.
Results
Baseline demographics showed no significant differences between groups ( Table 1 ). In the revision to OCA group, 12 patients (92.3%) underwent at least one prior procedure before ACI (excluding the cartilage biopsy) ( Table 2 ). The time to failure after ACI averaged 3.3 ± 1.7 years. Mean follow-up period was 3.2 ± 1.5 years (revision to OCA: 3.5 ± 1.7; primary OCA: 2.7 ± 0.9). The reason for failure after ACI was defined based on the intraoperative findings: 7 patients failed through delamination, 5 patients due to biological failure to form adequate cartilaginous repair tissue, and 1 patient due to progression of disease.
Type and Frequency of Previous Surgeries before ACI in the Revision to OCA Group.
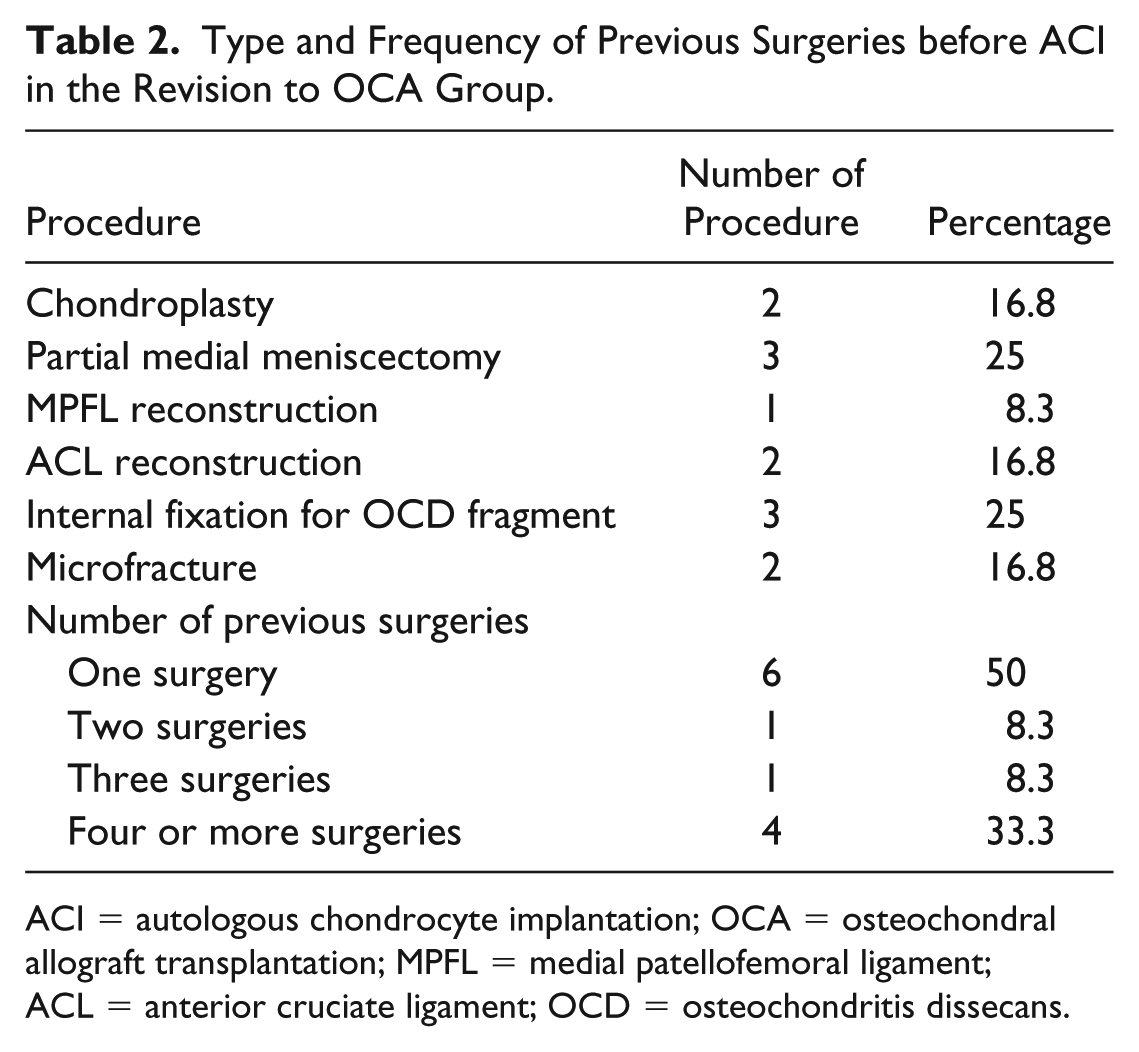
ACI = autologous chondrocyte implantation; OCA = osteochondral allograft transplantation; MPFL = medial patellofemoral ligament; ACL = anterior cruciate ligament; OCD = osteochondritis dissecans.
Preoperative KOOS Pain was significantly lower in the revision to OCA group (48.5 ± 15.6) than in the primary OCA group (61.6 ± 14.4) (P = 0.042). Postoperative functional scores showed no significant difference between both groups ( Fig. 2 ).
All patients in both groups demonstrated significant improvement in all functional scores after failed ACI revision to OCA (P < 0.05) ( Fig. 3 ).
Among patients who underwent revision to OCA, 5 patients (38.4%) had reoperations, including chondroplasty, lysis of adhesions, and removal of painful hardware, compared with 3 patients (23.1%) in the primary OCA group ( Table 3 ). In all these cases, the OCA graft was intact. There was no significant difference in either reoperation rate (P = 0.673) or mean time to reoperation between the groups (revision to OCA: 1.8 ± 1.9 years; primary OCA: 0.7 ± 0.4 years; P = 0.157). No difference was seen regarding failure rates between both groups with 3 patients (23.1%) in the revision to OCA group and 1 patient (7.7%) in the primary OCA group (P = 0.593) ( Table 3 ). OCA graft survival rate was 86.7% at 5 years (95% confidence interval = 49.4-95.7) among patients who underwent revision to OCA compared with 91.4% at 5 years (95% confidence interval = 56.6-98.9) among patients who underwent primary OCA. Survivorship distributions were not statistically different between both groups (P = 0.515) ( Fig. 1 ).
Reoperations Performed During the Follow-up Period.
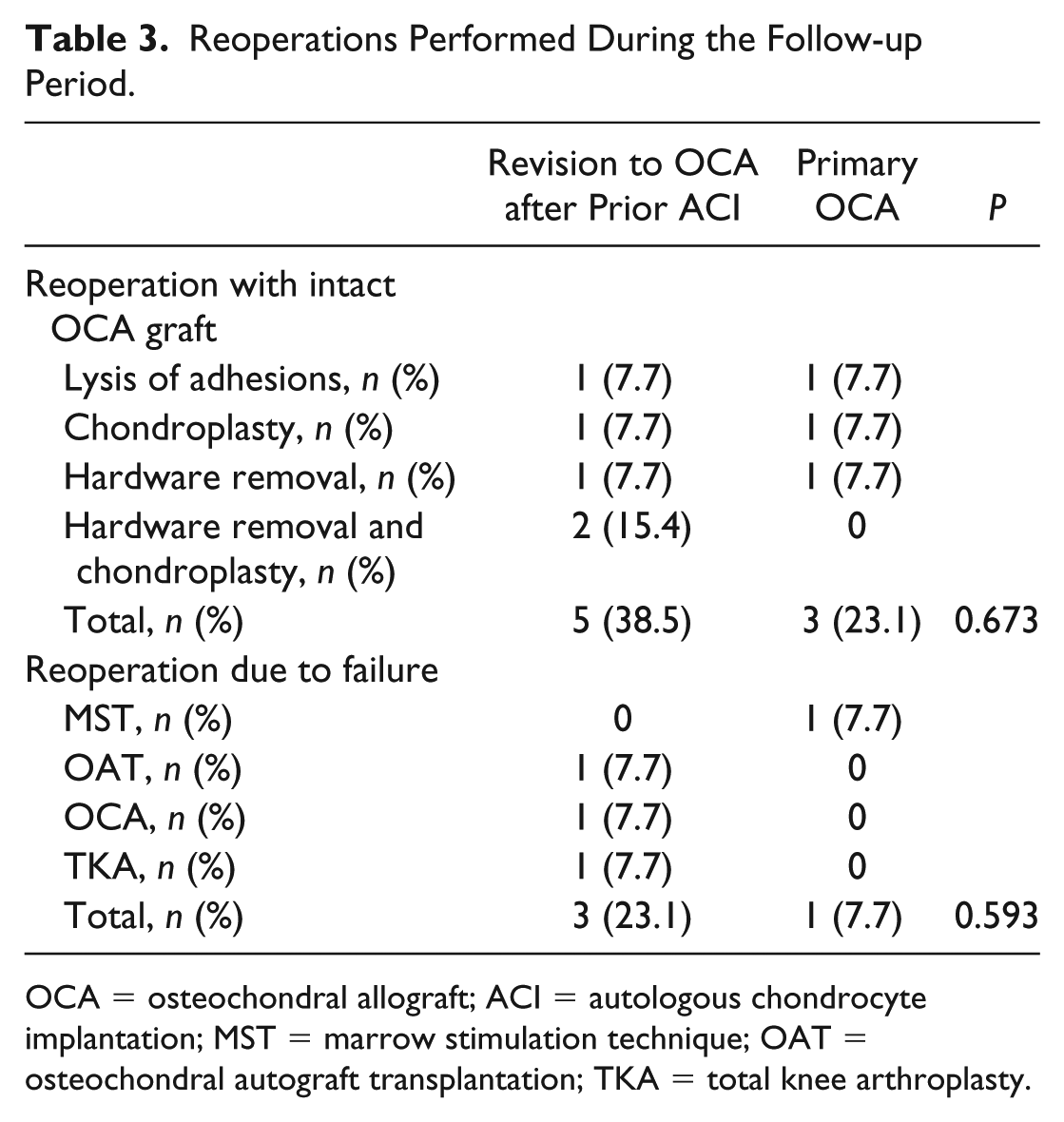
OCA = osteochondral allograft; ACI = autologous chondrocyte implantation; MST = marrow stimulation technique; OAT = osteochondral autograft transplantation; TKA = total knee arthroplasty.
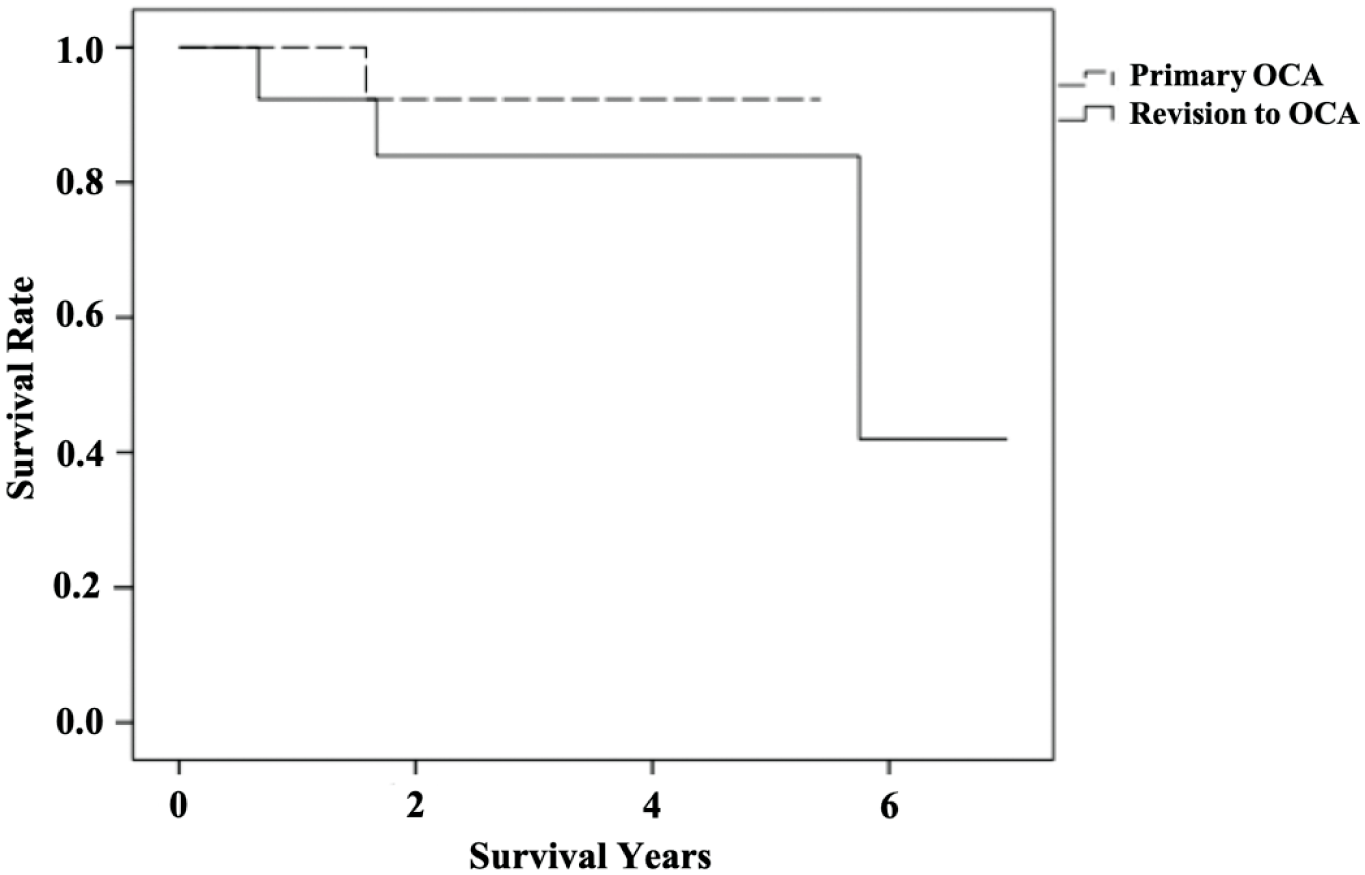
Kaplan-Meier survival curves. Survival rate after either primary osteochondral allograft transplantation (Primary OCA [osteochondral allograft]) or revision to osteochondral allograft transplantation after prior failed autologous chondrocyte implantation (Revision to OCA). The endpoint was defined as the failure of the graft.
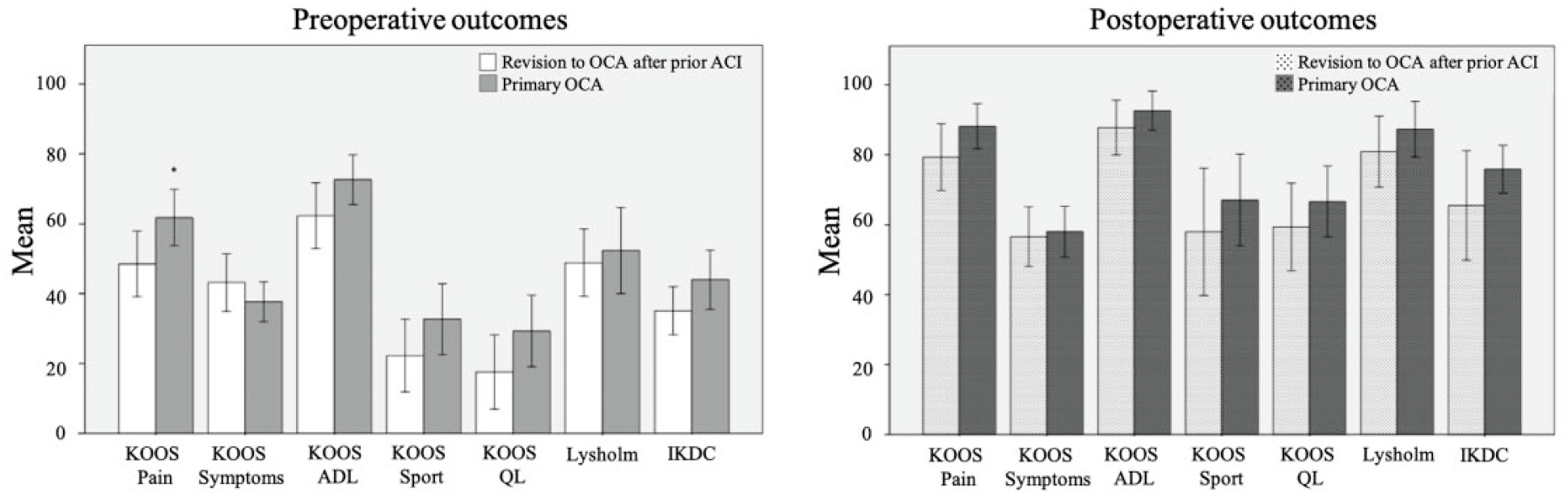
Pre- and postoperative patient-reported outcome measures between patients undergoing revision to OCA (osteochondral allograft) after failed ACI (autologous chondrocyte implantation) and primary OCA. Asterisk demonstrates significance (P < 0.05).
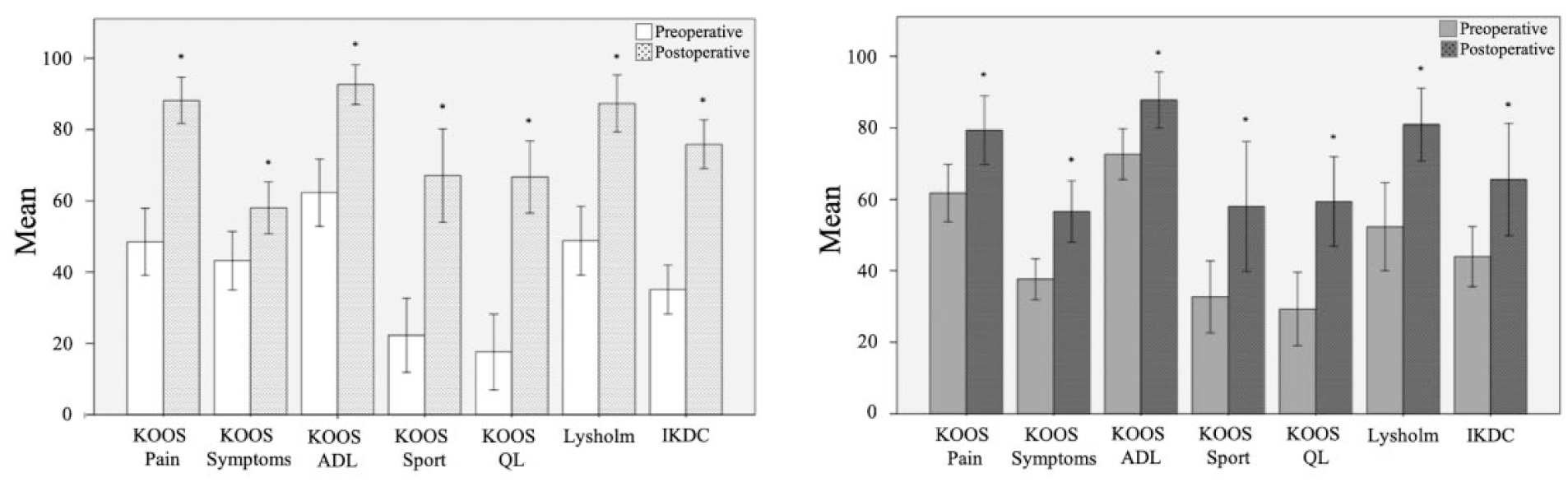
Improvement of patient-reported outcome measures from pre- to postoperative in patients undergoing revision to OCA (osteochondral allograft) after failed ACI (autologous chondrocyte implantation) and primary OCA. Asterisk demonstrates significance (P < 0.05).
Discussion
The key finding of the present study is that patients undergoing revision to OCA after failed ACI present with similar clinical outcomes compared with those who underwent primary OCA at mid-term follow-up. There were no significant differences in reoperation rates and graft survival rates between both groups. These results suggest that OCA is a viable treatment option in patients with prior failed ACI, resulting in favorable outcomes.
The interest in understanding the influence of a previous cartilage surgery on a subsequent revision cartilage restoration has increased over recent years. Many of our patients are young, increasing the likelihood of subsequent procedures over their life time. Mapping out a reasonable treatment course with consideration for potential revision procedures therefore appears advisable. Several studies reported good to excellent clinical outcomes after either primary OCA or OCA as a salvage procedure for failed prior cartilage restoration (Suppl. Table S1).10,14,16,19,20,24 However, to the best of our knowledge, this is the first study comparing clinical outcomes in patients undergoing revision to OCA after prior failed ACI or primary OCA. Gracitelli et al. 20 conducted a matched case-control study and compared patients who underwent OCA as a primary cartilage restoration (group 1, 46 knees) with patients who underwent OCA after failed previous MST procedure (group 2, 46 knees). A significant difference was found only for reoperation rates between both groups (group 1 = 24% vs. group 2 = 44%), while survivorship was similar between groups (group 1 = 87.4%; group 2 = 86% at 10 years). Both groups showed significantly improved outcomes with no significant differences between the groups, which was consistent with our results. In contrast to their study, our study did not find a significant difference in the reoperation rate between the groups. Frank et al. 10 also reported similar survival distribution after OCA (180 patients) between patients with and without a history of previous MST. In another study, Gracitelli et al. 14 analyzed a population of 164 knees treated with OCA transplantation after previous failed cartilage repair with a minimum follow-up of 2 years. Of the 164 knees, 145 underwent a previous MST procedure (88.4%), 3 underwent OAT (1.8%), 5 had previous OAT and MST procedure (3%), 5 knees underwent prior ACI with MST (3%), 1 underwent ACI and MST and synthetic plugs transplantation (0.6%), and 1 had periosteal implantation (0.6%). Sixty-eight knees (41.5%) had reoperations after OCA transplantation and 31 (19%) were considered a failure. Survivorship of the OCA transplantation was 87.8% at 5 years and 82% at 10 years. In their study, most of the patients underwent previous MST alone or in conjunction with other cartilage restoration techniques (overall 95%); therefore, the effects of cartilage restoration techniques beside MST were not clearly identified.
Prior studies also investigated the outcome of revision OCA for prior failed OCA.15,16 Horton et al. 16 reported data of 33 knees that underwent revision OCA transplantation after failed primary OCA with at least 2 years follow-up. In their study, revision OCA demonstrated inferior clinical outcomes compared to primary OCA with higher reoperation rate (22 patients [67%]) and failure rate (13 patients [39%]). 19 Both reoperation and failure rates were higher than reported for primary allografts.19,20 In contrast, the present study shows that survival and reoperation rates were similar in patients undergoing primary or revision to OCA after prior ACI.
As postoperative outcomes, reoperation and failure rates are similar to primary OCA, revision to OCA provides a reliable treatment option after failed ACI. 12 ACI, as surface procedure, requires intact subchondral bone for the successful treatment of focal chondral lesions. 25 However, OCA technique removes the damaged, abnormal subchondral bone to a depth necessary to achieve normal subchondral bone and substitutes it by the donor bone, which makes the OCA technique resistant to subchondral bone abnormalities.14,26,27 This may explain the favorable clinical outcomes of OCA after failed ACI and marrow stimulation. Several studies showed that ACI provides excellent survivorship in younger patients over a long-term follow-up.6,8 Nevertheless, in case of failure, patients are still young, such as in our study in which the mean age when the patient underwent revision to OCA after a prior failed ACI was 36.23 years. Given that young patients demonstrate increased risk of failure, less improvement, and higher dissatisfaction after total knee arthroplasty,28-30 performing another cartilage restoration instead of arthroplasty might be more desirable for this young population.
Our study is not without limitations. First, the relatively small sample size. Revision to OCA after prior failed ACI is a unique and rare procedure, performed in only 15 cases between September 2012 and February 2016. Second, the rather short follow-up period, which is a logical consequence of the rare nature of the procedure.
Conclusion
Revision of prior failed ACI with OCA is a viable treatment option with similar clinical outcomes, reoperation, and survivorship rates as primary OCA.
Supplemental Material
Supplementary_table – Supplemental material for Clinical Outcomes after Revision of Autologous Chondrocyte Implantation to Osteochondral Allograft Transplantation for Large Chondral Defects: A Comparative Matched-Group Analysis
Supplemental material, Supplementary_table for Clinical Outcomes after Revision of Autologous Chondrocyte Implantation to Osteochondral Allograft Transplantation for Large Chondral Defects: A Comparative Matched-Group Analysis by Gergo Merkely, Takahiro Ogura, Jakob Ackermann, Alexandre Barbieri Mestriner and Andreas H. Gomoll in CARTILAGE
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Our institutional review board approved this study (2018P000693/PHS).
Informed Consent
written informed consent was obtained from all patients at the time they were entered into the database.
Supplemental Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.