
Abstract
Objective
The aim of this study was to compare the clinical outcome of cartilage repair with autologous chondrocyte implantation (ACI) in patients with osteochondritis dissecans (OCD) lesions and full-thickness cartilage lesions.
Design
This study included a cohort of 115 consecutive patients with a cartilage lesion of the knee treated with ACI. Of the patients, 35 had an OCD lesion and 80 a full-thickness cartilage lesion. During a follow-up period from 2 to 13 years all treatment failures were identified. The failure rate between OCD lesions and full-thickness cartilage lesions was compared with Kaplan-Meier analysis. Patient-reported outcome was evaluated 2 years postoperatively with the Lysholm score.
Results
During the follow-up 21 out of 115 patients encountered a treatment failure. The failure rate for full-thickness cartilage lesions was 19.1% and for OCD lesions 43.3% over the 10-year follow-up. Patient-reported outcome improved from baseline to 2 years postoperatively. The improvement from baseline was statistically significant, and the Lysholm score improved more than the minimal clinically important difference. The patient-reported outcome showed no difference between lesion types at 2 years.
Conclusions
In the presented retrospective study, the failure rate of first-generation ACI was higher in OCD lesions than in large full-thickness cartilage lesions, suggesting that OCD lesions may associate with properties that affect the durability of repair tissue. Future prospective studies are needed to tell us how to best repair OCD lesions with biological tissue engineering.
Keywords
Introduction
Cartilage lesions of the knee may cause pain and functional impairment.1-3 The majority of the defects are full-thickness cartilage lesions with relatively intact subchondral bone.4,5 Deeper osteochondral defects are usually caused by osteochondritis dissecans (OCD), a rare disease of unknown origin.6,7 In these lesions, the pathognomonic finding is an osteochondral fragment, which may detach from the surrounding joint surface.8,9 The damaged joint area is unable to regenerate, and unrepaired OCD defects seem to increase the risk of osteoarthritis.10,11 Therefore, these lesions are often repaired surgically. The proportion of patients with OCD lesions is typically less than 10% of all patients requiring cartilage repair surgery. 12 The optimal surgical treatment for OCD lesions remains unclear.8,13,14
Autologous chondrocyte implantation (ACI) is a cell therapy developed to produce hyaline-like cartilage repair tissue, resulting in enhanced clinical outcomes.12,15-21 ACI has shown good and durable long-term results in large full-thickness cartilage lesions, in which other techniques have not provided sustainable results.17-19,22-25 Therefore, ACI is recommended for use especially in large cartilage lesions.12,20 ACI is also a feasible method to repair OCD defects. 26 However, comparison of treatment of full-thickness cartilage lesions and OCD lesions is lacking, and therefore, it is unclear whether the outcome of ACI is similar in these 2 types of cartilage lesions.
The aim of this study was to compare the clinical outcome of cartilage repair with ACI in patients with OCD lesions and in patients with full-thickness cartilage lesions. Additionally, we analyzed the effect of factors related to patients and lesions on the clinical outcome of this procedure.
Materials and Methods
Patients
The study included a cohort of first 115 consecutive patients with a cartilage lesion of the knee treated with ACI at Jyväskylä Central Hospital between 1997 and 2008 ( Table 1 ). Of the patients, 35 had an OCD lesion and 80 a full-thickness cartilage lesion. All patients were followed until the end of the year 2010. Written informed consent was obtained from all patients. The study protocol was approved by the Ethics Committee of Jyväskylä Central Hospital.
Baseline Characteristics of Patients with Osteochondritis Dissecans (OCD) Lesion or Full-Thickness Cartilage Lesion.
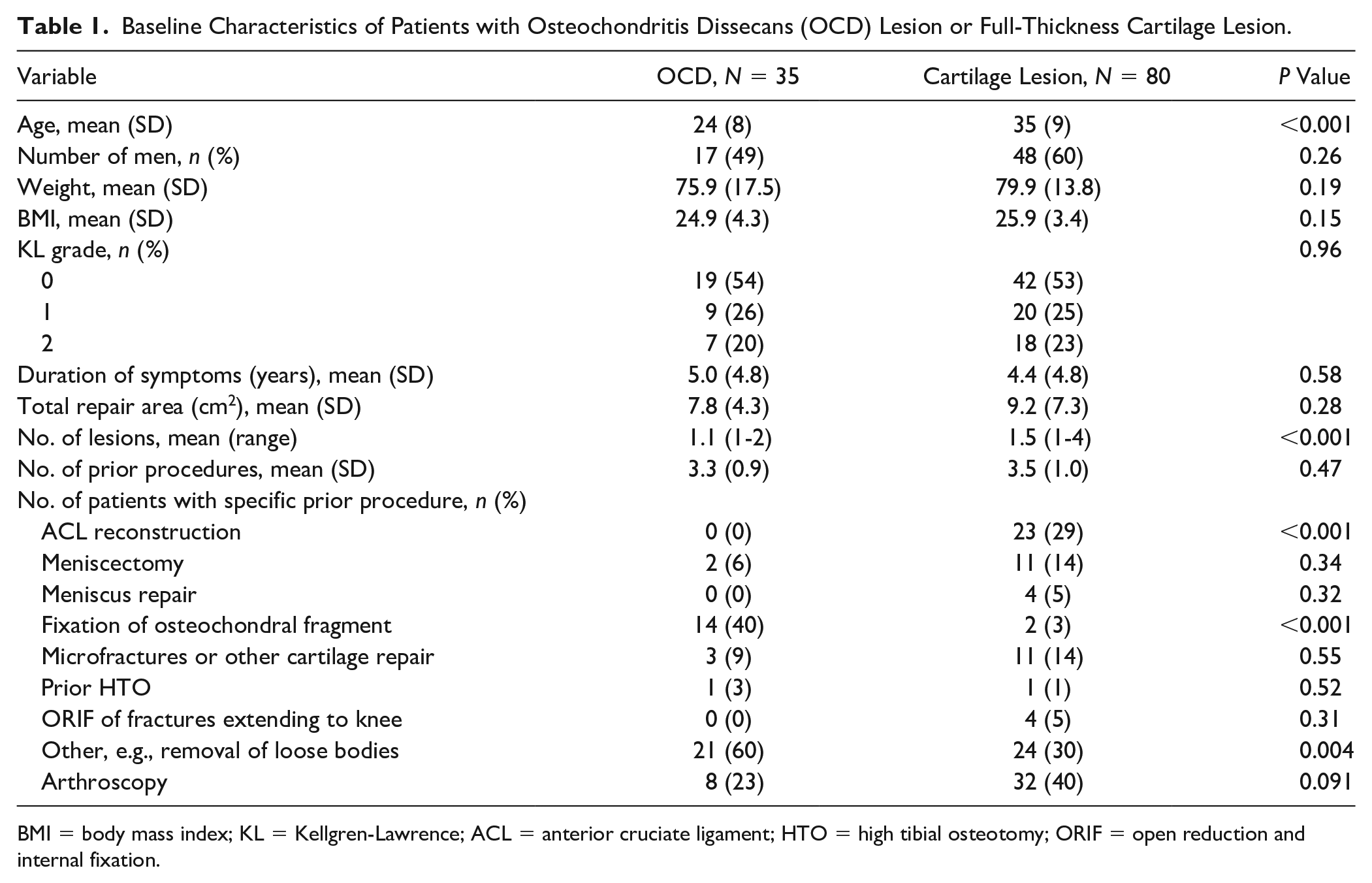
BMI = body mass index; KL = Kellgren-Lawrence; ACL = anterior cruciate ligament; HTO = high tibial osteotomy; ORIF = open reduction and internal fixation.
Surgical Treatment
The ACI was performed as described by Brittberg et al. 15 Briefly, a cartilage biopsy was first obtained in a knee arthroscopy. Chondrocytes were isolated and cultured to create an autologous chondrocyte suspension in the cell culture laboratory (Sahlgrenska University Hospital, Gothenburg, Sweden). Open knee surgery was performed to repair the cartilage lesion. The lesion was debrided to subchondral bone. A periosteum patch was sutured to the surrounding cartilage margins. The seam was then finished with fibrin glue (TISSEEL; Immuno AG, Vienna, Austria) to create a watertight cover over the lesion. The chondrocyte suspension was injected under the periosteum, and the seam was closed with a final suture and fibrin glue. In deep (>10 mm) OCD lesions, the bone defect was repaired with autologous bone transplantation before ACI as described by Peterson et al. 26 In this technique, the bone defect was filled with an autologous bone graft and covered with a periosteum patch, which was sutured and the seam covered with fibrin glue (TISSEEL; Immuno AG, Vienna, Austria). Thereafter another periosteum patch was sutured to the surrounding cartilage margins and autologous chondrocytes were implanted as described above. Of the OCD lesions, 14 were deeper than 10 mm and were repaired with a sandwich technique.
An osteotomy was performed when the mechanical axis was measured to be abnormal. The clinician assessed the mechanical axis during a clinical examination before cartilage repair. If the axis was suspected to be abnormal, full-length standing weight-bearing X-rays of the lower limbs were obtained to assess the axis deviation in more detail.
Outcome Measures
The outcome was measured with failure rate and patient-reported outcome. The failure rate was calculated with the Kaplan-Meier method based on treatment failures. The patient-reported outcome was evaluated at 2 years according to the Lysholm score. 27 Our study applied the failure definition introduced by Moseley and coworkers. 18 A failure was defined if new cartilage repair procedure (e.g., bone marrow stimulation) or knee arthroplasty was needed, or if the repair tissue was found insufficient or deteriorated. Patient-reported outcome was obtained at the visits to the hospital or by mail.
Data Collection and Analysis
Baseline data were collected at the time of the intervention. Collected data included patient demographics (gender, age, weight, height), lesion- and knee-related factors (etiology, duration of symptoms, number of lesions, area of lesions, prior and concurrent procedures), and patient-reported outcome scores (Lysholm score, where 100 points indicates no symptoms or disability). Patients were asked to fill the Lysholm score at all visits to the hospital during the follow-up and with additional contacts by mail. All postoperative visits considering the operated knee were documented during the follow-up. All this clinical information was used for failure rate analysis. The follow-up of 24 patients ended prematurely because they moved to another hospital district. Their truncated follow-up (in average 3.0 [SD 2.5] years) was included in time-to-event statistics as censored data.
To evaluate radiographic osteoarthritis, the baseline and follow-up radiographic images were analyzed and graded according to the Kellgren-Lawrence classification by a musculoskeletal radiologist (MS). For the analysis, all non–digital images were scanned.
Statistics
The data were presented as means with standard deviations (SDs) or as counts with proportions (%). Statistical comparisons were made using the chi-square test, Fisher-Freeman-Halton test, t test, or bootstrap-type t test. The bootstrap method was used when the theoretical distribution of test statistics was unknown or in case of violation of assumptions (e.g., nonnormality). Time-to-event data were described by Kaplan-Meier failure rate curves and evaluated using the log-rank (with exact permutation) test. Cox proportional hazards model was used to estimate adjusted hazard ratio (HR) for failure rates between the groups. The normality of the variables was tested by using the Shapiro-Wilk W test. Stata 15.1 (StataCorp LP, College Station, TX) was used for all analyses.
Results
During the follow-up 21 out of 115 patients met the criteria for failure. Of these 21 patients, 10 had a cartilage lesion and 11 an OCD lesion. All failed patients had prolonged knee pain and reduced function. In addition, some had locking or catching type of sensations. In the cartilage lesion group, 5 patients had insufficient repair tissue fill, and 5 had osteoarthritis (OA). Of the insufficient repairs, 2 were treated with microfractures and 3 with a new ACI. Of the patients with OA, 3 patients received a total knee arthroplasty, and 2 patients with early and moderate OA were treated conservatively. In the OCD lesion group, 3 patients had insufficient repair tissue fill and 7 patients had their repair tissue detached from the osteochondral junction. The 3 insufficient repairs were treated with microfractures. Of the 7 patients with detached grafts, 2 received microfractures, 2 received a new ACI, 2 were scheduled to receive a new ACI later, and 1 patient with additional early OA was treated conservatively. Additionally, one patient in the OCD lesion group had arthroscopically adequate looking graft, but numerous subchondral cysts found in magnetic resonance imaging. These cysts were assumed to explain the severe knee symptoms, and the patient was thus treated with a new ACI. Of the 14 bone-grafted OCD lesions, 3 resulted in failure ( Table 2 ). The Kaplan-Meier analysis showed a significant difference in the 10-year failure rate between patients with full-thickness cartilage lesions and those with OCD lesions ( Fig. 1 ). First failures were identified 1 year after surgery. Over 1.5 years of follow-up, failures were observed with comparable frequencies in both lesion types. Thereafter, the failure rate became higher in OCD lesions than in full-thickness cartilage lesions. At 5 years, the failure rate for full-thickness cartilage lesions was 9.5% (95% confidence interval [CI] = 4.6% to 19.0%) and for OCD lesions 32.2% (95% CI = 18.0% to 53.3%). At 10 years, the failure rate for full-thickness cartilage lesions was 19.1% (95% CI = 0.0% to 34.6%) and for OCD lesions 43.3% (95% CI = 25.9% to 65.9%). The difference in failure rate between the lesion types was significant (P = 0.006, log-rank). The hazard ratio for treatment failure was 3.02 (1.08 to 8.43) in patients with OCD lesions relative to patients with full-thickness cartilage lesions, when adjusted for lesion size, BMI, age, gender, duration of symptoms, and number of earlier procedures.
Details of 21 Patients with a Treatment Failure during Follow-Up a .
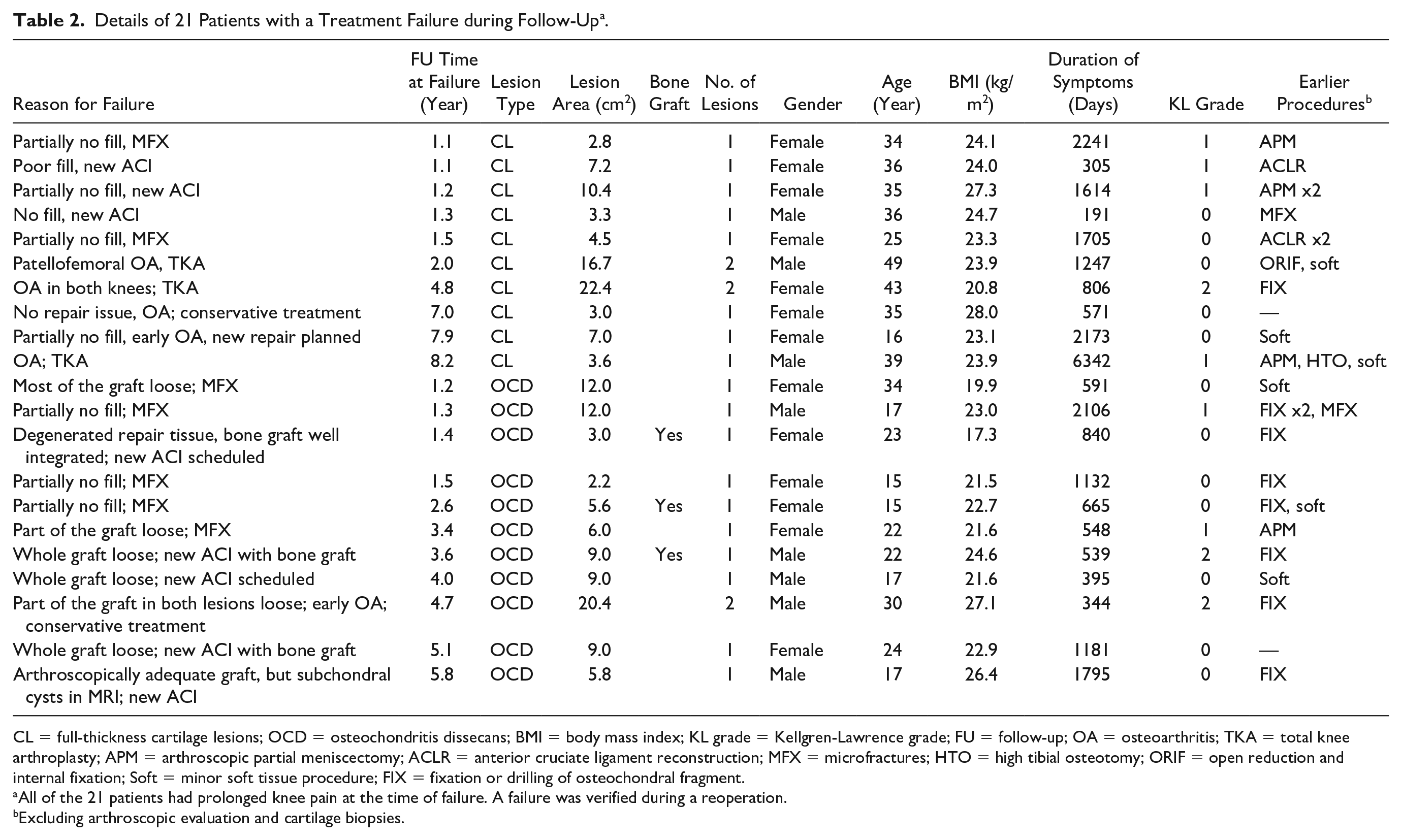
CL = full-thickness cartilage lesions; OCD = osteochondritis dissecans; BMI = body mass index; KL grade = Kellgren-Lawrence grade; FU = follow-up; OA = osteoarthritis; TKA = total knee arthroplasty; APM = arthroscopic partial meniscectomy; ACLR = anterior cruciate ligament reconstruction; MFX = microfractures; HTO = high tibial osteotomy; ORIF = open reduction and internal fixation; Soft = minor soft tissue procedure; FIX = fixation or drilling of osteochondral fragment.
All of the 21 patients had prolonged knee pain at the time of failure. A failure was verified during a reoperation.
Excluding arthroscopic evaluation and cartilage biopsies.
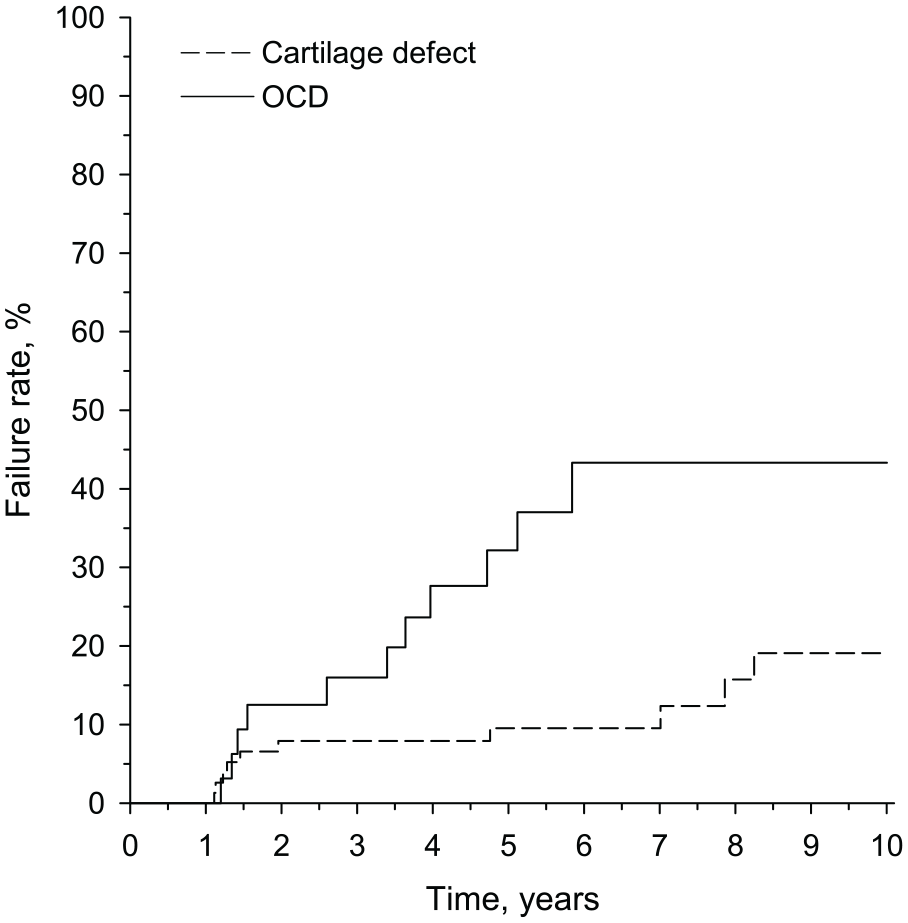
Calculated failure rate according to Kaplan-Meier analysis for patients with full-thickness cartilage lesions and osteochondritis dissecans (OCD) lesions. The difference in failure rate between OCD lesions and full-thickness cartilage lesions during the 10-year follow-up was significant (log-rank, P = 0.006).
Patient-reported outcome was analyzed from 80 patients at 2 years postoperatively according to the Lysholm score. The remaining 35 patients had missing pre- or postoperative Lysholm scores and were therefore excluded. Twenty of these 80 patients had an OCD lesion. In both groups, the Lysholm score improved from baseline (P < 0.001 in patients with full-thickness cartilage lesions and P = 0.020 in patients with OCD lesions). However, no significant difference in Lysholm score was observed between the groups at baseline or at 2 years ( Table 3 ).
Lysholm Score of Patients with an Osteochondritis Dissecans (OCD) Lesion or a Full-Thickness Cartilage Lesion at a Median Follow-up of 24 Months (IQR: 13, 38).
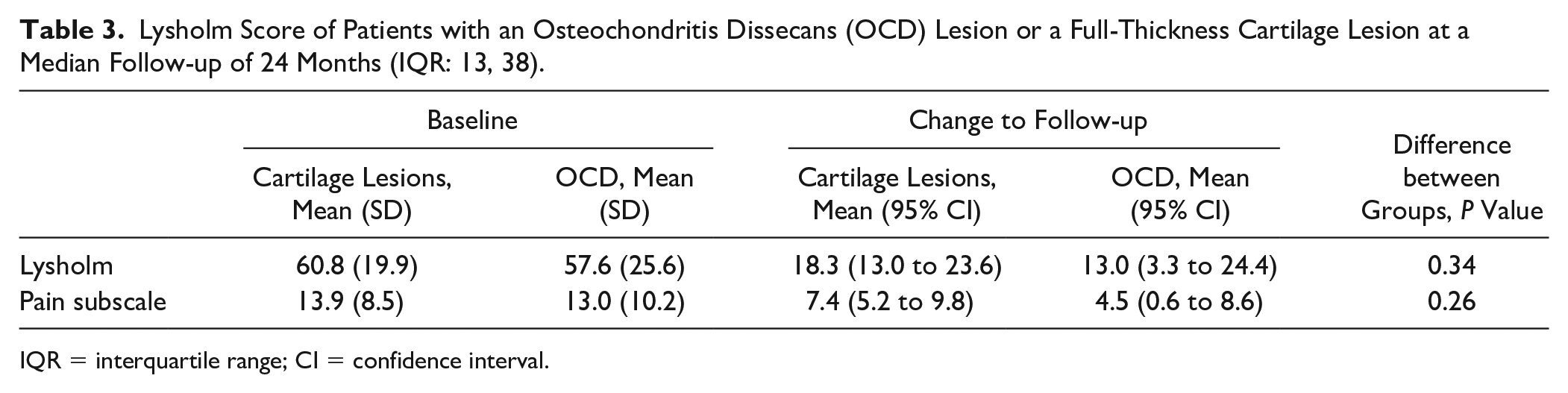
IQR = interquartile range; CI = confidence interval.
Lesion size, BMI, age, gender, lesion area, duration of symptoms, KL grade, additional bone grafting, and number of earlier procedures showed no effect on failure risk or patient-reported outcome. In the radiographic analysis, the KL score increased during the 10-year follow-up, but no difference emerged between the groups.
Four patients encountered adverse events after ACI. A patient sustaining skin blistering at the site of the tourniquet and having radiating pain of the lower limb recovered spontaneously during the follow-up. A superficial wound infection was treated successfully with antibiotics. A minor wound dehiscence was managed with wound closure strips. One deep venous thrombosis was encountered and treated with low-molecular-weight heparin and warfarin.
Discussion
This study showed that ACI resulted in a durable outcome less often in OCD lesions than in full-thickness cartilage lesions. Treatment failures were more frequent in OCD lesions. Previous studies show that ACI produces durable outcome in both cartilage lesions and OCD lesions.12,20,22,28 Contrary to previous reports, our study shows higher failure rate for ACI in OCD lesion, suggesting that the durability of ACI might differ between the lesion types.
The first treatment failures were observed after 1 year of follow-up. Failures were detected frequently over the next year in both lesion types. Thereafter, failures were still detected frequently in OCD lesions, while in full-thickness cartilage lesions failures became more infrequent. The failure rate of full-thickness cartilage lesions was comparable to previous reports.17-19,29 In line with the current guidelines, the size of the full-thickness lesions was relatively large.12,20 Notably, the failure risk was unaffected by lesion size, confirming the observation of Nawaz et al. 19 These findings support the evidence that ACI is capable of repairing large full-thickness cartilage lesions of the knee in a sustainable manner. However, in OCD lesions ACI performed worse than expected. Even though some OCD lesions were deep and needed additional bone grafting, this had no effect on the failure risk. As OCD is a rare disease, the sample sizes in clinical studies have been relatively small. 18 Typically, patients with OCD lesions have been included in groups of patients with other types of complex cartilage lesions or in groups containing all cartilage lesions.17-19 Only a few studies have reported separately the outcome of ACI in OCD lesions.22,26,28 In the study of Peterson and coworkers, 26 patients with OCD lesions showed greater improvement in the Lysholm score at 2 years than in our study. In another study, patients with OCD lesions and full-thickness cartilage lesions have shown comparable clinical outcome according to the Lysholm score in long-term follow-up. 22 Failure rate was not reported in these studies. Minas and coworkers reported the failure rate of ACI with autologous bone grafting in 24 patients who had an osteochondral lesion of the knee due to OCD or avascular necrosis (AVN). 30 Deviating from ours, they included also patients with AVN, and all patients in their study received a bone graft. In comparison to our study, their failure rate estimate seems lower, but the 95% confidence intervals overlap with those of ours. Carey and coworkers reported the results of ACI in the largest series of OCD patients. 28 The characteristics of their patients, and the OCD lesions, differ only marginally from our study. In their study, the lesions were smaller and bone grafting was used less frequently. Their definition for failure differs slightly from ours, as our study defines a failure also if the repair tissue was insufficient or deteriorated. In comparison to our study, their study seems to show lower failure rate in OCD patients. However, the difference is statistically uncertain, as the 95% confidence intervals of the failure rate estimates overlap at 5 years and, marginally, at 10 years of follow-up. Altogether, our failure rate estimate for ACI in patients with OCD lesions seems higher compared to previous reports. However, comparisons between different studies remain somewhat uncertain due to the relatively wide confidence intervals in many studies. This indicates a need for studies with higher number of patients with OCD lesions. In contrast to previous studies, our study compared the results of ACI in OCD lesions and cartilage lesions. This enabled methodologically equal evaluation of outcome of ACI in OCD patients relative to the more common full-thickness cartilage lesions. The data show that ACI fails more frequently in OCD lesions than in full-thickness cartilage lesions. Thus, OCD lesions might have unique properties that reduce the durability of the repair tissue.
Patient-reported outcome improved during the first 2 years regardless of lesion type. However, our study was unable to show any difference between patients with different lesion types. In all patients, the Lysholm score improved more than the proposed clinically significant improvement (i.e., Lysholm score improved more than 10 points). 21
OCD lesions differ from full-thickness cartilage lesions as the lesion extends also to the subchondral bone. This difference may have an impact on the higher failure rate of ACI in patients with OCD lesions. As intact subchondral bone seems to be essential for maintaining normal cartilage, the repair technique should be capable of restoring the subchondral bone both structurally and functionally.31-34 After ACI, previously injured subchondral bone results more often in a deformed bone cartilage interface.35,36 This suggests that the inability to properly restore the subchondral bone could explain the higher failure rate of ACI in OCD lesions.
Another explanation for the higher failure rate of ACI in OCD lesions might be found in the defect volume. Although research has shown that ACI is capable of repairing large lesions, the depth of the OCD lesion might become a challenge. In OCD lesions, ACI results in thick repair tissue, which might be vulnerable to mechanical loading, thereby reducing the durability of the repair. In the deepest lesions that required a bone graft, the failure rate was similar to other OCD lesions. This supports the use of additional bone graft in deep OCD lesions, although it still remains unclear whether bone grafting affects the durability of ACI in OCD lesions.
Additionally, the pathogenesis of OCD lesions is different from full-thickness cartilage lesions. OCD lesions are disease-related, whereas full-thickness cartilage lesions may occur in otherwise healthy cartilage due to mechanical trauma. OCD lesions have been associated with genetic background.37,38 Such disorders might result in reduced capability to form repair tissue, explaining the increased failure rate. Disturbed genetic pathways have been linked to extracellular matrix proteins of hyaline cartilage and development of the synovial joints.39,40 Additionally, chondrocytes acquired from animals with OCD disease seem to have reduced capability to proliferate. 41 Therefore, the underlying pathogenic mechanism of OCD might reduce the capability of ACI to regenerate optimal repair tissue. The lower durability of ACI in OCD lesions may thus be explained by several factors. Even though this is a relatively large group of OCD lesion patients, it was not large enough for more detailed analysis of reasons for lower durability.
The strength of this study was the large number of OCD patients relative to the sample sizes of OCD patients reported in other studies. In addition, the consecutive patients represented an unselected sample of typical patients requiring cartilage repair. Study limitations comprised many patients missing Lysholm scores and the lack of comparison with spontaneous healing of these lesions. Due to the missing Lysholm scores a comprehensive clinical analysis is lacking. The limited number of patient-reported outcomes did not enable comparison of clinical score between failed and nonfailed repairs. Additionally, due to the lack of patient-reported outcomes some clinical failures might not be detected. Furthermore, our study was unable to describe long-term patient reported outcome.
In this retrospective study, the failure rate of first-generation ACI was higher in OCD lesions than in large full-thickness cartilage lesions, suggesting that OCD lesions may be associated with properties that affect the durability of repair tissue. Future prospective studies are needed to tell us more how to best repair OCD-lesions with biological tissue engineering.
Footnotes
Acknowledgments and Funding
We thank the associate editor for constructive suggestions to improve the conclusions. We have made changes according to the associate editor’s suggestions. The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
The study protocol was approved by the Ethics Committee of Jyväskylä Central Hospital.
Informed Consent
Written informed consent was obtained from all patients.