
Abstract
Objective
Aim of this systematic review was to describe all classification systems for knee osteochondritis dissecans (OCD) lesions, evaluating their accuracy and reliability, as well as their use in the literature on knee OCD.
Design
A systematic review of the literature was performed in July 2021 on PubMed, WebOfScience, and Cochrane Collaboration (library) to describe all published classification systems for knee OCD lesions and quantify the use of these classifications in the literature.
Results
Out of 1,664 records, 30 studies on 33 OCD classifications systems were identified, describing 11 radiographic, 13 MRI, and 9 arthroscopic classifications. The search included 193 clinical studies applying at least one OCD classification, for a total of 7,299 knee OCD cases. Radiographic classifications were applied to 35.8%, MRI to 35.2%, and arthroscopic classifications to 64.2% of the included studies. Among these, in the last two decades, the International Cartilage Repair Society’s (ICRS) arthroscopic classification was the most described approach in studies on knee OCD. Overall, there is a lack of data on accuracy and reliability of the available systems.
Conclusions
Several classifications are available, with ICRS being the most used system over the time period studied. Arthroscopy allows to confirm lesion stability, but noninvasive imaging approaches are the first line to guide patient management. Among these, radiographic classifications are still widely used, despite being partially superseded by MRI, because of its capability to detect the earliest disease stages and to distinguish stable from unstable lesions, and thus to define the most suitable conservative or surgical approach to manage patients affected by knee OCD.
Level of evidence:
Systematic review, level IV.
Introduction
Osteochondritis dissecans (OCD) is a focal, idiopathic pathologic process of the osteochondral unit, 1 with the knee being the most affected joint.2,3 This condition involves primarily the subchondral bone and has the potential for secondary instability with disruption of the overlying articular cartilage, which could result in the separation of the osteochondral fragment. These alterations can severely impair joint function and lead to the development of early osteoarthritis (OA). 4 Accordingly, the choice of the most appropriate treatment is crucial to improve patient symptoms and prevent OA, especially considering the young age of the affected patients.3,5 Several options are currently available, ranging from conservative management 6 to surgical approaches with fragment fixation, drilling, or osteochondral replacement procedures.7,8
The algorithm for OCD management needs to consider several factors, like the skeletal maturity, the presence of cartilage degeneration, the stability of the lesion and its probability to heal.8-10 A proper OCD classification is therefore crucial to choose the best treatment approach for OCD lesions. From 1888, when Konig first named the disease, 11 the need to better understand the different types of OCD lesions led to the development of several classifications systems. Different methods have been proposed either based on radiologic or arthroscopic evaluations, all presenting specific advantages and drawbacks in terms of costs, invasiveness, and ability to detect key diagnostic aspects. 12 To date, a consensus about the most suitable classification system is still lacking. The absence of a universally recognized classification method makes it difficult to compare the results of the current literature and to provide the clinicians with clear indications to properly identify and treat each specific OCD lesion.
Aim of this systematic review was to describe all classification systems for knee OCD lesions, evaluating their accuracy and reliability, as well as their use in the literature on knee OCD.
Materials and Methods
A systematic review of the literature was performed on the existing OCD classifications systems. The search was conducted on July 27, 2021, on the three medical electronic databases PubMed, WebOfScience, and Cochrane Collaboration (library) using the following parameters: ([OCD] OR [osteochondritis dissecans]) AND (knee). The guidelines for Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) were used. 13 All the results were screened and analyzed separately by two independent observers (L.S. and S.A.A.). A selection to exclude duplicates was performed. In the first step, the following inclusion criteria for relevant articles were used during the initial screening of titles and abstracts: articles of any level of evidence, written in English language, with no time limitation, reporting about knee OCD. Exclusion criteria were articles written in other languages, preclinical studies, and articles focusing on other joints or other pathologies than knee OCD. In a second step, full texts of the selected articles were examined, and papers were further selected to the purpose of the present review for the analysis of two main aspects:
To describe all published classification systems for knee OCD lesions. Reference lists from the selected papers were screened to detect other articles describing new OCD classification systems. In this step also articles in other languages and systematic reviews were selected, if reporting a previously not described OCD classification.
To quantify the use of these classifications in the literature; the full texts of the clinical studies about knee OCD lesions were examined according to the inclusion and exclusion criteria defined in the first step of the systematic review. Moreover, systematic reviews and articles that did not use OCD classifications to describe patient series affected by OCD were excluded.
Relevant data (year, study design, classification system, classification criteria description, and number of OCD cases analyzed) of all the included studies were extracted and collected in a database by two observers (L.S. and S.A.A.), with involvement of a third author (L.A.) to reach consensus in case of disagreement, to be analyzed for the purpose of the present manuscript.
Results
The search identified a total of 1,664 records after duplicates removal (
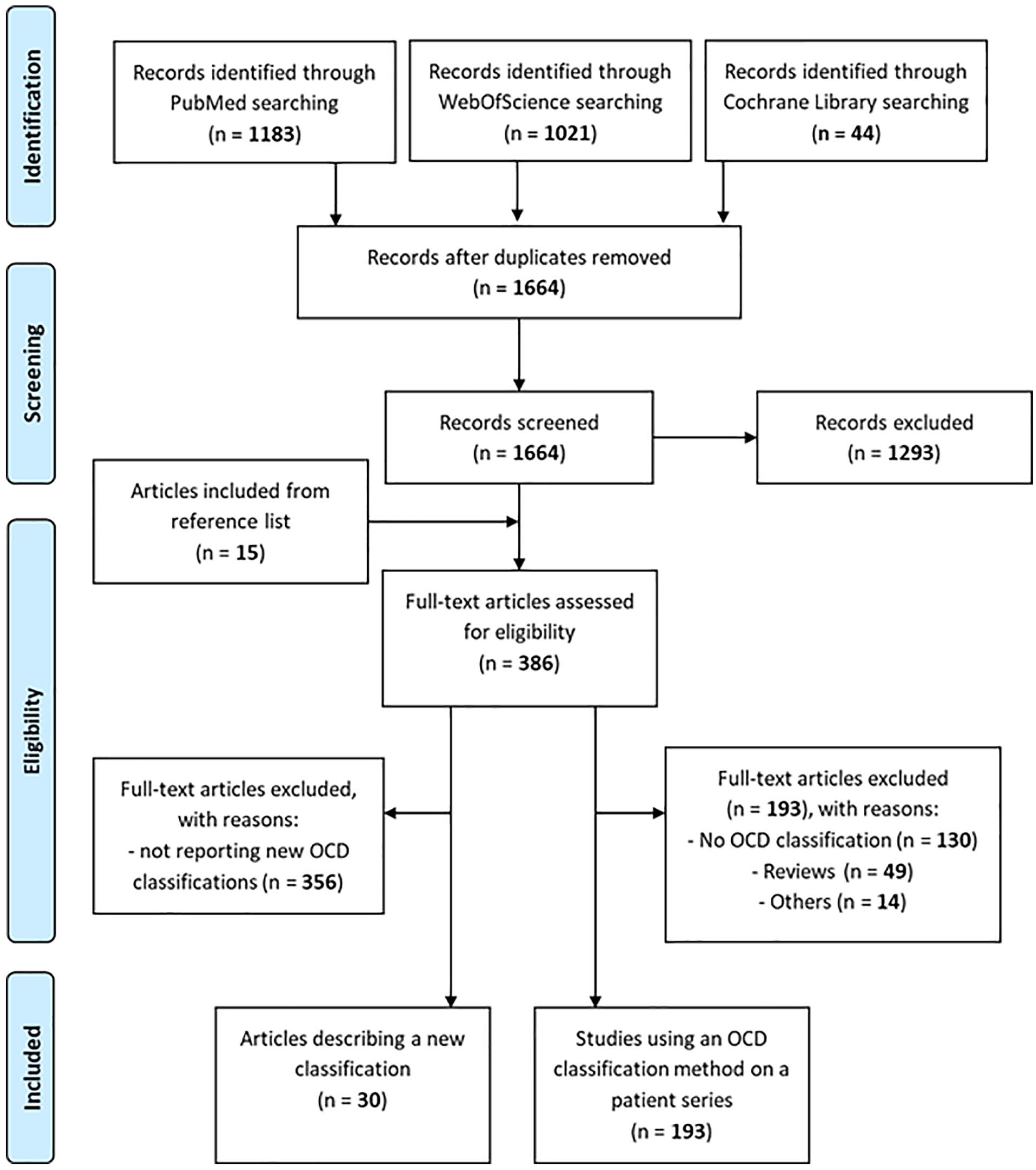
PRISMA flow-chart of the systematic literature review.
OCD Classifications
The 30 articles proposed 11 radiographic classifications (1 using a combination of x-rays and bone scan), 13 MRI classifications, and 9 arthroscopic classifications.
X-ray classifications
X-rays have been used to classify OCD severity in 7 studies, OCD location in 3 studies, and one study focused on both severity and location 14 ( Table 1 ).
X-ray Classifications.
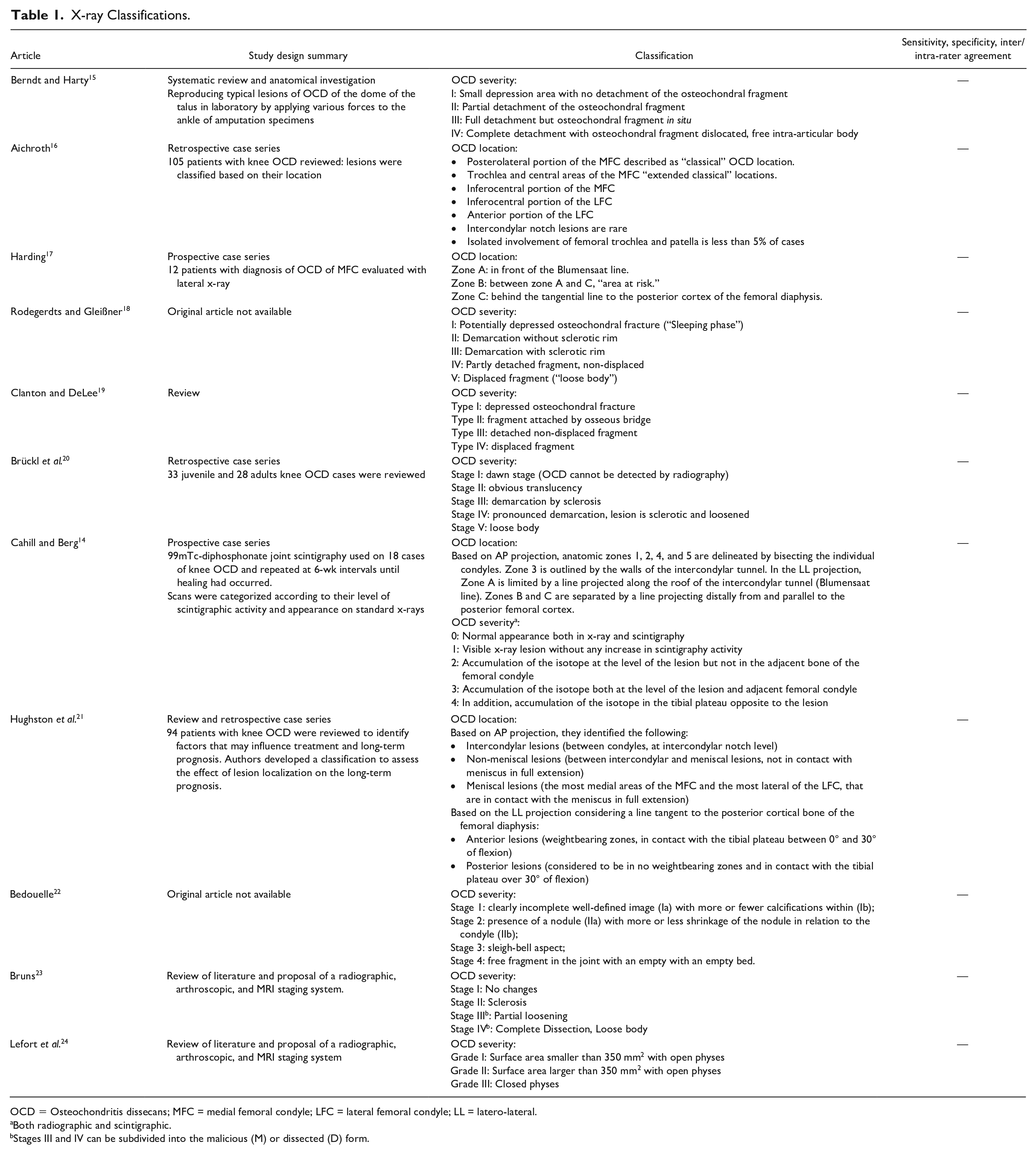
OCD = Osteochondritis dissecans; MFC = medial femoral condyle; LFC = lateral femoral condyle; LL = latero-lateral.
Both radiographic and scintigraphic.
Stages III and IV can be subdivided into the malicious (M) or dissected (D) form.
The first x-ray-based OCD classification was described by Berndt and Harty 15 in 1959 and focused on OCD severity, being originally used for OCD of the talus and then widely adopted also for knee lesions. This system recognizes 4 grades of OCD severity, emphasizing the process of progressive detachment of the osteochondral fragment, grading it from a stable lesion to a complete displacement with the presence of an intra-articular body. Similar criteria for defining lesion severity depending on fragment stability or detachment were also applied in the subsequent classifications of Clanton and Delee, 19 Rodegerdts and Gleißner, 18 and Brückl et al., 20 with the last two also describing sclerosis and translucency to better identify the earlier stages. In 1988, Bedouelle et al. 22 proposed the assessment of other lesion features including the presence of calcification and the appearance as a nodule with more or less shrinkage or with a sleigh bell aspect. Later, Bruns in 1997 23 implemented in the concept of growing instability the distinction of malicious or dissected forms in the more advanced stages, which corresponded also to MRI and arthroscopic findings. Finally, Lefort et al. 24 in 2006 introduced a classification based both on the extension of the lesion and the physeal status.
The first radiographic classification focused on lesion location was introduced by Aichroth in 1971, 16 describing seven categories of specific locations according to their relative frequency, with the lateral posterior portion of the medial femoral condyle defined as the “classical” OCD location. In 1977, Harding 17 focused on lesions of the medial femoral condyle dividing them in 3 zones and identifying an “area at risk” between the Blumensaat line (tangent to the roof of the intercondylar notch in lateral-lateral projection) and the tangential line to the posterior cortex of the femoral diaphysis. In 1984, Hughston et al. 21 proposed a new “anatomical” radiographic classification using the meniscus as reference. Based on the AP projection, they identified “Intercondylar lesions,” “Non-meniscal lesions,” and “Meniscal lesions,” while on the LL projection anterior and posterior lesions were differentiated based on the tangential line to the femoral posterior cortex already used by Harding. Cahill and Berg 14 proposed in 1983 a location system dividing the knee into 5 zones in medial-lateral direction, similarly to Hughston et al., and 3 zones in anteroposterior direction, in a similar fashion to the older Harding classification. Moreover, they combined x-ray findings and 99mTc scintigraphy to describe 5 grades of OCD severity. Bone scan findings were indicative of the extent of progression or healing of OCD, although its use has been subsequently replaced by MRI.
Bone scan and nuclear medicine imaging
Cahill and Berg 14 classification included not only radiographs, but also 99mTc-diphosphonate joint scintigraphy, performed on 18 cases of knee OCD and repeated at 6-week intervals until healing had occurred. Based on scintigraphic activity and x-ray appearance, the authors developed a 0 to 4 grading system. Bone scan findings were indicative of the extent of progression or healing of OCD.
MRI classifications
In the last decades, MRI has progressively gained importance for evaluating the knee, especially concerning cartilage pathologies. Currently, it is the most important radiological exam to diagnose and to follow-up knee OCD lesions, and to this aim, 13 classification systems have been described (Table 2). The most important focus of these classifications is the lesion stability/instability, which is key to decide the conservative/surgical management. All the existing classification systems describe intact articular cartilage for stable or low-grade lesions while authors agree that high-signal intensity in T2-weighted sequences between parent bone and fragment is an indicator of instability, even though in some cases, the high-signal intensity was described to also indicate healing or fibrous tissue at the interface.25-27
MRI Classifications.
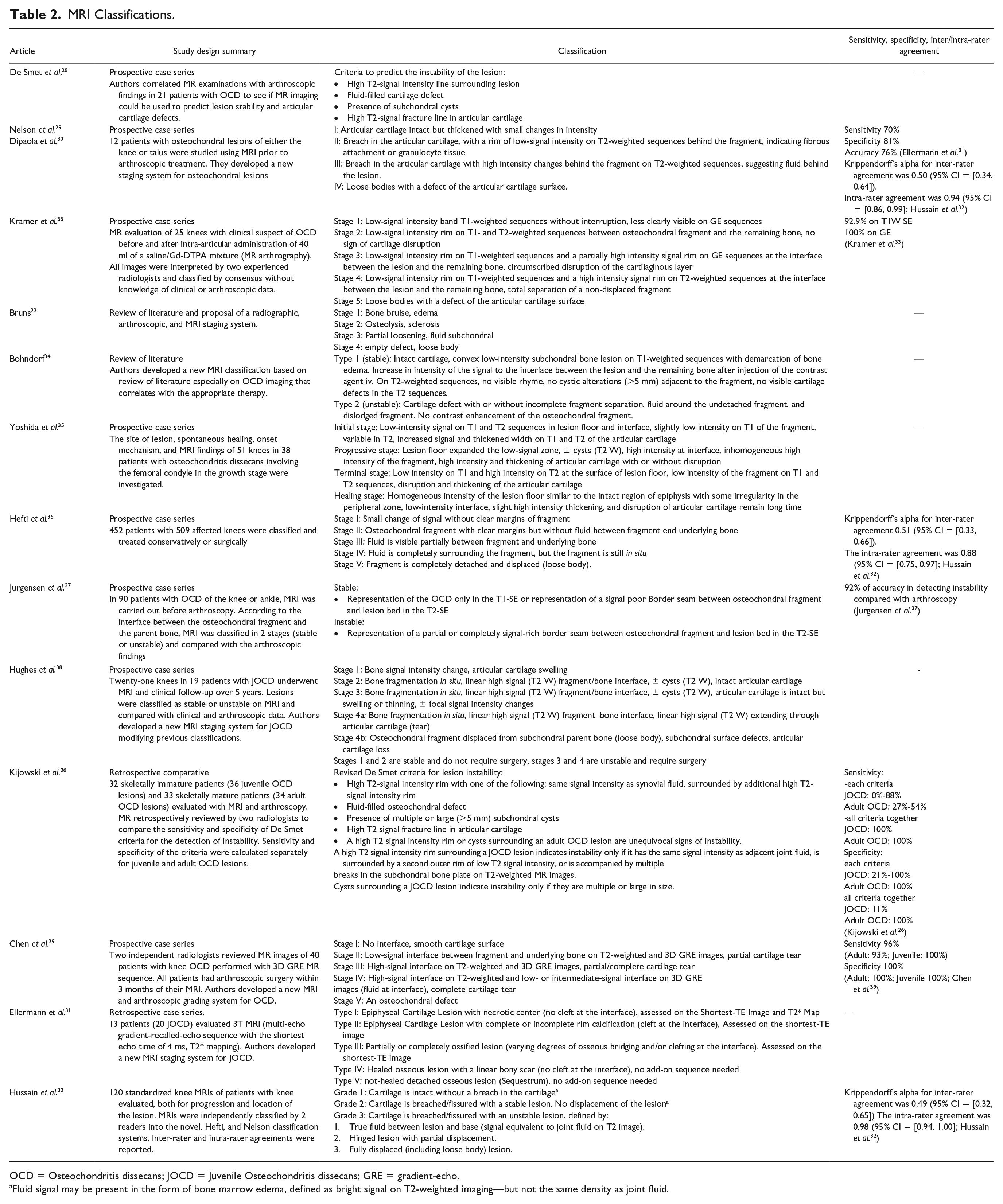
OCD = Osteochondritis dissecans; JOCD = Juvenile Osteochondritis dissecans; GRE = gradient-echo.
Fluid signal may be present in the form of bone marrow edema, defined as bright signal on T2-weighted imaging—but not the same density as joint fluid.
The first MRI criteria to predict the instability of the OCD lesion were formulated by De Smet et al. 28 in 1990 (high T2-signal intensity line surrounding the lesion, fluid-filled cartilage defect, presence of subchondral cysts, high T2-signal fracture line in articular cartilage) and were subsequently used and revised by Kijowski et al. 26 These criteria did not provide a detailed classification of the lesions with specific stages but rather an evaluation of the risk of instability. However, Nelson et al. 29 and the following paper of Dipaola et al. 30 can be considered the first to describe in 1991 an MRI-based classification system. They described a 4-stage MRI classification based on T2-weighted sequences, with Stages I and II considered to be stable and Stages III and IV instable lesions. Later, in 1992, Kramer et al. 33 proposed the use of a contrast agent (MR arthrography) to improve the sensitivity of MRI in staging OCD, using T1- and T2-weighted sequences and GE sequences. They proposed a 5 stages classification introducing a stage with only subchondral bone alterations without cartilage involvement. The same concept of bone-originating lesion based on the detection of fluid (either synovial fluid or gadolinium in case of absent effusion) between fragment and underlying bone was also used by Hefti et al. 36 in 1999 to develop a new 5 stages classification. Contrarily, in 1998, Bohndorf 34 differentiated OCD lesions only into 2 types in relation to the stability and the need for surgery: Type 1 (stable lesions not requiring surgery) and type 2 (unstable lesions where surgical intervention is recommended). Similarly, Jurgensen et al. 37 in 2002, published a new classification differentiating two types of OCD lesions considering their stability based on T1 and T2 sequences. Later, Chen et al., 39 in 2013, proposed a new 5 stages classification system adding a three-dimensional (3D) T1-weighted gradient-echo (GRE) MR sequence to the routine protocol to better differentiate fluid from granulation tissue and consequently to better detect unstable lesions. Finally, Hussain et al., 32 in 2021, proposed a simpler 3-group classification with a reported excellent intra-rater agreement and moderate inter-rater agreement.
Other classifications have been specifically developed for Juvenile OCD (JOCD), to improve accuracy by considering the different characteristics with respect to adult forms. Yoshida et al., 35 in 1998, developed a staging system differentiating JOCD in 4 stages in relation to the natural history of the lesions and introducing a last stage called “healing stage.” In 2003, Hughes et al. 38 revisited previous classifications30,33,34,40 and developed a 4-stage system, with Stages 1, 2, and 3 considered stable and with high chance to heal with conservative treatment, whereas Stage 4 required surgery. Finally, Ellermann et al., in 2016, 31 based on the preclinical histological evidence that JOCD might occur after a focal failure of endochondral ossification, developed a 5-stage classification system, with T2* mapping added to the MRI protocol, which described also the healed osseous lesion (Stage IV) and the not-healed osseous lesion (Stage V).
Arthroscopic classifications
Nine different arthroscopic classifications (Table 3) of knee OCD lesions were found in the literature. They all present a similar scale of increasing instability, from an initial softening of the articular cartilage with a progressive detachment of the fragment from the parent bone up to the final creation of a crater with loose bodies.
Arthroscopic Classifications.
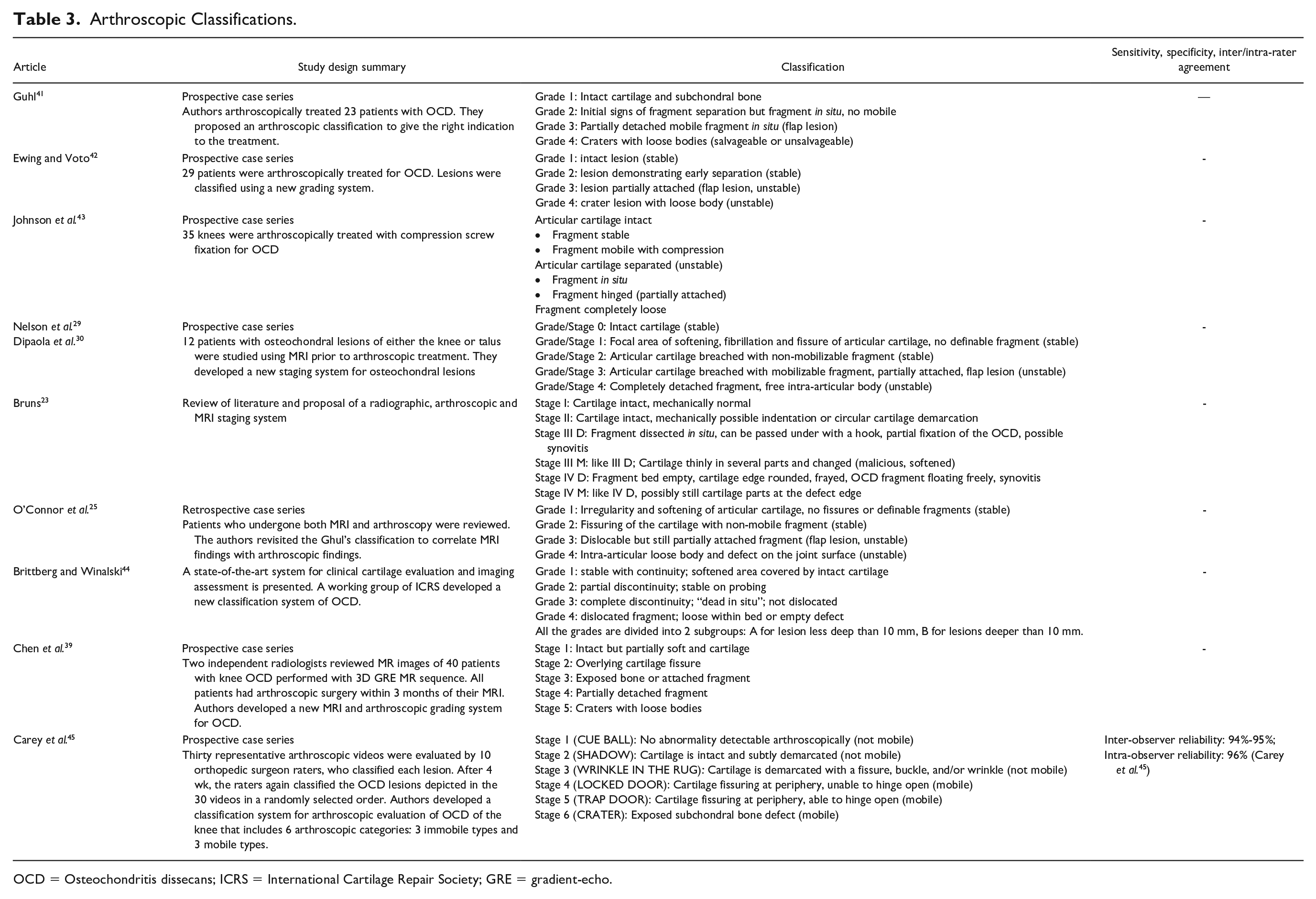
OCD = Osteochondritis dissecans; ICRS = International Cartilage Repair Society; GRE = gradient-echo.
The first arthroscopic classification for OCD has been published by Guhl 41 in 1979. This simple 4-grade classification distinguished stable lesions (Grades 1 and 2) and unstable lesions (Grades 3 and 4). Guhl’s classification laid the foundation for the formulation of the subsequent arthroscopic classifications which present overlapping aspects, like the similar one proposed in 1988 by Ewing and Voto. 42 In 1990, Johnson et al. 43 classified OCD in 3 different diagnostic groups (stable, unstable, loose body) with further division related to the integrity of articular cartilage and the separation of the fragment. In the same year, Nelson et al. 29 modulated the OCD classification system proposed by Pritsch et al. for talar lesions 40 and formulated a more detailed graduation system ranging from Grade 0 (normal cartilage) to Grade 4 (detached fragment with intra-articular loose body), which also found a correspondence with the parallel MRI classification developed in the same study. 29 The following year, Dipaola et al. 30 further elaborated this classification and its correlation with the MRI findings. Bruns in 1997, 23 O’Connor et al. in 2002, 25 and Chen et al. in 2013 39 also revised previous classification systems, correlating arthroscopic findings with new or already described MRI classification systems.
In 2003, to address the need for standardized and universally accepted classification systems in cartilage pathology, the International Cartilage Repair Society (ICRS, currently International Cartilage Regeneration & Joint Preservation Society) published a staging system specific for OCD lesions of the knee. 44 This system, described by Brittberg and Winalsky, included 4 stages, each one consisting in 2 subgroups, A and B, for lesions, respectively, inferior or superior to 10 mm in depth. Finally, in 2016, Carey and other members of the Research in OsteoChondritis of the Knee (ROCK) group 45 developed a new staging system with the aim of making classification easier and more reproducible. Their staging system includes 6 categories: 3 types of lesions are considered non-mobile and 3 mobile. To improve understanding, applicability, and reproducibility, every type of lesion was named with an easy name to remember providing a simple description of the arthroscopic appearance. Helpful instructions to distinguish “borderline” lesions were also provided. Moreover, this classification was also assessed for its reliability, demonstrating an excellent inter-observer and intra-observer reliability, respectively, 0.95 and 0.96. 45
Application of OCD Classifications
The search found 193 clinical studies applying at least one OCD classification, for a total of 7,299 OCD cases in the knee joint. The number of cases described in the articles ranged between n = 1 and n = 892 with a mean of 38 OCD knee lesions examined per study. Along with the overall increase in publication numbers, many proposed classifications have been increasingly used, with the ICRS classification system rising in the last two decades and currently being the main reference in OCD literature (
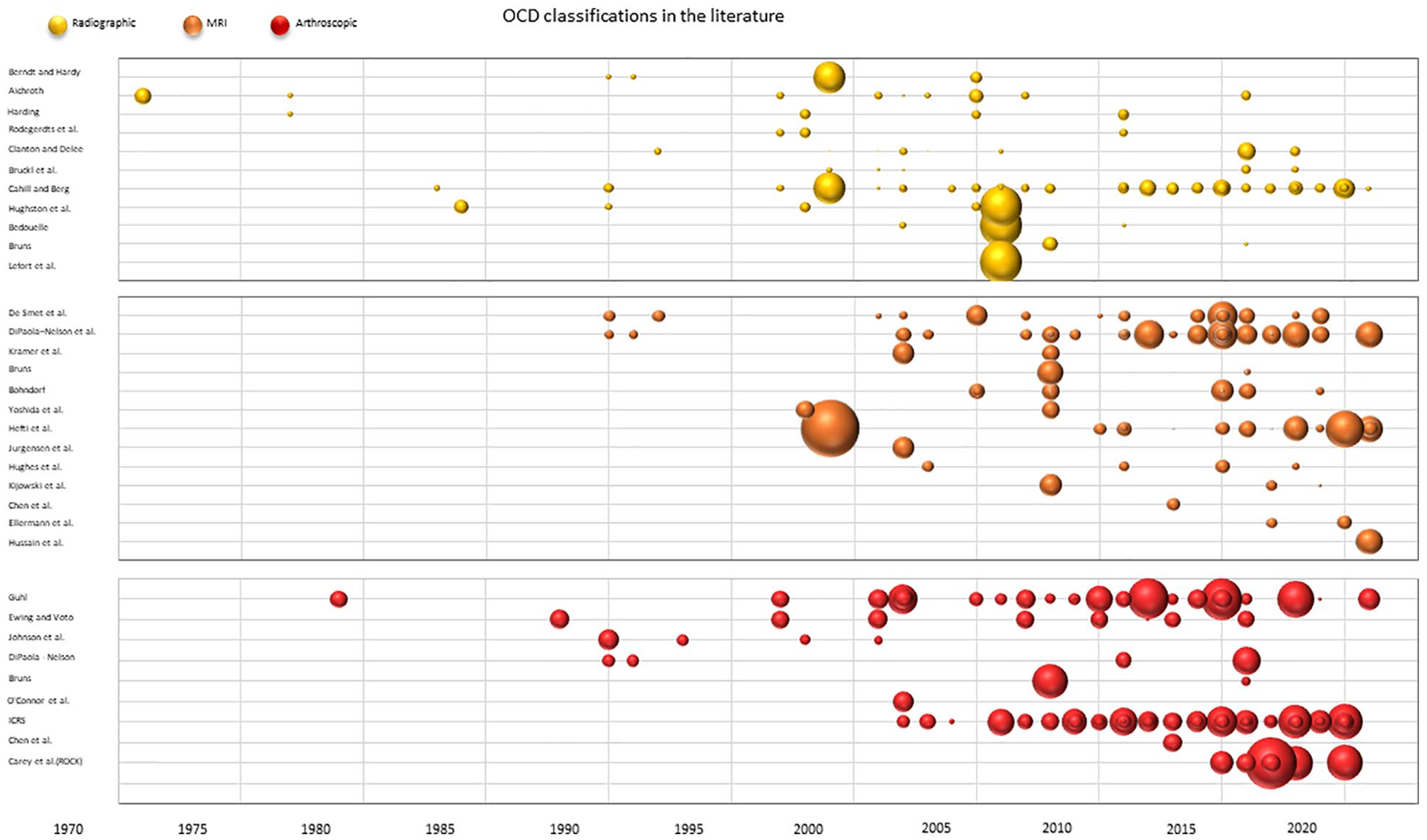
OCD classifications in the literature. The figure shows the use of all OCD classifications in the literature over time. Each bubble represents a clinical study where the respective classification is used and the size of the bubble proportionally represents the number of patients included in the study. OCD = Osteochondritis dissecans.
X-ray classifications
Radiographic classifications were widely adopted in the past decades and are still used. A total of 69 studies on 4,105 OCD cases (56.2% of the OCD examined) used at least one radiographic classification. Cahill and Berg classification was the most adopted, being reported in 36 studies (18.6%) on 2,053 knees (28.1% of the overall OCD literature cases examined). Hughston classification was applied in 5 studies and 1,097 cases (15.0%). Bedouelle classification was used in 3 studies and 924 cases (12.7%). The recently introduced Lefort classification was described in a multicentric study involving 892 OCD cases (12.2%). Other x-ray classifications were documented in less patients: Aichroth classification and Clanton and DeLee classification were both used in 9 studies, for 386 (6.0%) and 260 (4.2%) cases, respectively, and Bruckl et al. in 6 studies and 90 (1.4%) cases (see
MRI classifications
A total of 68 studies reporting on 2,959 (40.5%) of the lesions examined in this review employed at least one MRI classification. Nelson et al. and Dipaola et al. classification was the most frequently adopted being used in 26 studies on 1,082 OCD patients corresponding to 14.8% of the examined cases. The first described De Smet MRI criteria were adopted in 14 studies and 462 patients (6.3% of the cases). The Hefti et al. classification was used in 13 studies reporting on 1,113 OCDs (15.2% of the cases). Other classifications based on MRI were used less, as Bohndorf classification with 8 studies on 230 (3.1%) cases, and Hughes et al. classification with 4 studies on 77 (1.0%) cases (see
Arthroscopic classifications
A total of 124 studies (64.2%) corresponding to 3,511 (48.1%) of the lesions examined in this review resulted to be classified with at least one arthroscopic classification. Among the included studies, 67 (34.7%) employed the ICRS system for grading a total of 1,549 knees OCD lesions corresponding to 21.2% of the cases examined. Other arthroscopic classification systems also resulted to be frequent in the reviewed literature. Guhl’s classification was used in 33 studies and 1,028 knees, which represents 14.0% of the cases examined. The Ewing and Voto classification was used in 9 studies for grading 197 lesions (2.7%). The classification introduced in 2016 by the ROCK study group was used in 7 studies for a total of 566 lesions (7.7% of the cases; see
Discussion
The main finding of this study is that many knee OCD classification systems have been described, with the ICRS classification being the most used one, but many others are still commonly applied, based on radiographic, MRI, or arthroscopic OCD features.
The ideal OCD classification system should offer a precise and reliable grading of the lesion based on the clear description of lesion characteristics and allow the diagnosis in the early phases to avoid treatment delay. Moreover, it should be able to identify lesions with high risk of fragmentation and osteochondral detachment, defining the healing potential and therefore guiding either the conservative management or the surgical treatment. 46 The different classification systems converge to the final scenario of fragment detachment, which requires surgical treatment of refixation, excision, or reconstruction of the defect, while limits the possibility to relay on a bone marrow stimulation procedure (e.g., retro- or anterograde drilling).36,47 More challenging is the definition of the different earlier phases characterizing OCD pathology, where one of the key parameters is the stability of the OCD lesion, as this could determine the evolution toward healing or progression.27,28,48,49 In fact, while stable lesions, typical of JOCD, can be treated conservatively, unstable lesions often require surgical management. 7
The term “stability” was used in 1987 by Mesgarzadeh et al. 50 to refer to the mechanical integrity of the subchondral OCD lesion. In their study, the authors compared plain radiographs, scintigraphy, and MRI to determine the best way to assess the stability of OCD lesions. Bone scintigraphy and MR imaging were considered preferable diagnostic modalities for evaluating the mechanical status of OCD lesions.14,50,51 Still, some characteristics on plain x-rays have been associated with an increased risk of instability: larger lesion size, minimal subchondral bone on the progeny fragment, and increased thickness of the sclerotic rim, 52 and some authors24,53 suggested that the need for an MRI could be based on specific radiographic features. According to Lefort et al., 24 Grade I OCD with open physes does not require first-line imaging studies other than radiographs, while criteria for MRI are Grade II or III, surface area greater than 350 mm2, or closed physes. 53 In 2015 and 2017, the ROCK study group54,55 evaluated different radiographic features with the aim of identifying the best parameters to be used effectively in the diagnosis and treatment choice of knee OCD lesions. They concluded that many diagnostic features of femoral condyle lesions can be reliably classified on plain radiographs, such as detachment of the fragment, growth plate maturity, condylar width, lesion size, fragmentation, displacement, boundary, central radiodensity, and contour.54,55 In their studies, they found excellent inter-rater reliability when judging the overall healing of OCD femoral condyle lesions on radiographs as well as on 5 specific features (boundary, sclerosis, size, shape, and ossification). Building upon these findings, Ramski et al., in 2017, proposed a radiographic grading of healing types for OCD lesions that demonstrated good inter- and intra-observer reliability. 56 These authors retrospectively reviewed 41 consecutive knee OCD lesions treated by a single surgeon and radiographically classified healing patterns such as boundary resolution, increasing radiodensity of progeny fragment, combined or not applicable. Still, radiographic classifications present undeniable limitations, mainly related to the poor early diagnosis and a suboptimal lesion stability evaluation. Nowadays, they are mostly used to describe the location of the lesion or the healing status, while their application for assessing lesion severity and stability is indeed considered less informative.
The gold standard for assessing the stability of knee OCD is the arthroscopic evaluation. This approach allows to study the entire joint and to treat OCD defect and associated lesions in the same surgical step. Nonetheless, in young patients, cracks or mobility may be absent due to the thick cartilage layer overlying the fragment, thus arthroscopic signs of instability could arise later than MRI signs. 53 Moreover, arthroscopy has the limitation of not being able to evaluate the subchondral bone, and it is an invasive procedure with related risks, which questions its use as diagnostic tool. Rather, it should be the last step of a more complex algorithm for OCD management, being indicated when surgical procedures are required and when a precise clinical and imaging diagnose has been made, mostly by the use of MRI. This systematic review presented the large number of arthroscopic classifications described in the literature, highlighting the lack of standardization and of data regarding their reliability. In fact, only the ROCK arthroscopic classification has been evaluated for its intra- and inter-observer reliability, demonstrating excellent results. 45 Despite being formulated only in 2016, the ROCK classification is increasingly applied, and its use already reached 9% of the OCD cases classified in the literature. Still, nowadays the most used is the ICRS arthroscopic classification, 44 which has been applied in more than one third of the studies. First described in 2003, this classification was developed as an arthroscopic grading system. However, the defined criteria have been largely accepted and sometimes exploited also for the imaging evaluation, 57 which presents several advantages that overcome the limitations of arthroscopic systems.
MRI is a noninvasive approach to study OCD lesions, and it is arguably the best tool for detecting the early presence of OCD, identifying stable lesions that arthroscopy may miss.26,57-60 The primary aim of all MRI classifications is to determine the stability or instability of the lesion. Several MRI features were associated with instability, like loose bodies, cysts in the subchondral bone, breaches through the articular cartilage overlying the OCD fragment, and a line of high-intensity signal between progeny fragment and parent bone on T2-weighted images.25,28,34,61 However, this signal may also represent a healing reaction,25,34,35 with the risk of misinterpreting the lesion stability and thus misleading toward the need for surgery. In the last years, more specific MRI protocols have been introduced to better distinguish stable and unstable MRI lesions. To this regard, on 3D GRE MR imaging with spectral fat suppression,62,63 the articular cartilage appears bright while fluid is dark to intermediate, helping in differentiating fluid from granulation tissue. Chen et al. 39 demonstrated excellent diagnostic capabilities in detecting unstable OCD lesions combining routine sequences with 3D GRE T1-weighted MR imaging. These good results were confirmed for both adult and JOCD, with excellent accuracy and reliability, overcoming the previous findings of Kijowski et al. 26 who stated that MRI was not reliable in predicting the stability of OCD prior to skeletal maturity.
The evaluation and classification of JOCD has been the focus of other authors. To quantify the healing potential in juvenile subjects, Wall et al. 27 evaluated the influence of different variables (patient age, lesion size, lesion location, knee symptoms, and sex) on a non-operative treatment protocol for JOCD. They developed a system “nomogram” including normalized length and width of the lesions and the presence of mechanical symptoms to predict the probability of spontaneous healing. The latest JOCD classification, published in 2016, by Ellermann et al., focused instead on the staging of the natural history of a JOCD lesion, proposing an etiopathogenetic hypothesis in which focal failure of endochondral ossification and epiphyseal cartilage ischemia would lead to a type I entirely cartilaginous lesion as the earliest disease manifestation. 31 While this hypothesis awaits further confirmation, it is worth noticing how the overall debate on the very causes of this disease remains open. 64 The lack of knowledge on key aspects of disease development and progression, as well as response to treatment, may limit the possibility for an optimal and effective management of OCD patients. Further work will be needed to define reliable characteristics to predict clinical lesion instability and prognosis. 65
A useful tool to better characterize OCD and investigate the healing prognosis can be represented by nuclear medicine imaging (CT-SPECT and PET-scan), as demonstrated in some studies on the follow-up of OCD.66,67 However, there is a drawback represented by the relatively high dose of radiation to the patients, which currently makes the presence of clinical studies on this topic limited. Thus, based on the available literature, an initial x-ray can be considered useful to assess both severity and location, focusing on the radiographic features described and validated by the ROCK group,14,54,55 followed by an MRI evaluation performed with specific sequences to analyze the stability and hypothesize the prognosis.33,39,65 While the aforementioned approaches provide important information, the arthroscopic procedure remains the gold standard to evaluate OCD stability. In this setting, the lesions can be classified with ICRS and ROCK classifications,44,45 to better characterize OCDs and plan the treatment accordingly.
This study has some limitations, especially in the terms of representing the overall use of classification systems in the literature. In fact, the search focused on papers specifically referring to OCD classifications, thus not including those using other criteria not pertaining to OCD classifications. This hindered the possibility to quantify completely the application of criteria to classify and manage OCD in the current practice. Another limitation may be the absence of comparative evaluations of the quality of the classification systems to define the most suitable ones. Moreover, only a few studies assessed the effectiveness of the proposed methods by evaluating accuracy or reliability, and the prognostic value also remains unclear. Thus, further studies are needed to better understand the value of each available classification system. Nevertheless, this review defined some trends in the literature, and the results allowed to draw meaningful considerations.
Several classification systems based on radiographs, MRI, and arthroscopy have been proposed over the years to classify OCD location or severity, focusing on key features to assess lesion stability and healing potential. Arthroscopy, using the ICRS or the more recent ROCK classifications, remains the gold standard to confirm lesion stability while offering the possibility to directly perform the surgical treatment. However, noninvasive imaging approaches are the first line evaluation to guide patient management. Among these, nowadays radiographic classifications are superseded by MRI because of its capability to detect the earliest stages of the disease and to distinguish stable from unstable lesions, and thus to define the most suitable conservative or surgical approach to manage patients affected by knee OCD.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: James L Carey is in the board or committee member of International Cartilage Repair Society; is a paid consultant for JRF Ortho (USA) and Vericel Corporation (USA); received research support from Ossur (Iceland) and Vericel Corporation (USA); is in the editorial or governing board of The American Journal of Sports Medicine. All the other authors declare that they have no potential conflicts of interest regarding the publication of this paper.
Ethical Approval
Ethical approval was not sought for the present study because it is a systematic review and does not directly involve patients.