
Abstract
Objective
Osteochondritis dissecans (OCD) lesions are a relevant problem that affects the long-term prognosis of young patients. The purpose of this study was to analyze the evidence on potential and indications of nonsurgical treatment strategies for knee OCD.
Design
The search was conducted on 3 medical electronic databases according to PRISMA guidelines, including reports of any level of evidence dealing with the conservative management of knee OCD. Of 1688 identified records, 55 full-text articles were screened: 27 studies met the inclusion criteria, for a total of 908 knees, and were used for the analysis.
Results
No high-level studies were found: 24 articles were case series and 3 case reports, reporting on different treatments summarized in (1) restriction of physical activity, (2) physiokinesitherapy and muscle-strengthening exercises, (3) physical instrumental therapies, (4) limitation of weightbearing, and (5) immobilization. The analysis showed an overall healing rate of 61.4%, with large variability (10.4%-95.8%). A conservative treatment based on restriction of sport and strenuous activities seems a favorable approach, possibly combined with physiokinesitherapy. Negative prognostic factors were also identified: larger lesion size, more severe lesion stages, older age and skeletal maturity, discoid meniscus, and clinical presentation with swelling or locking.
Conclusions
The literature on conservative treatments for knee OCD is scarce. Among different non-surgical treatment options, strenuous activity restriction seems a favorable approach, whereas there is no evidence that physical instrumental therapy, immobilization, or weightbearing limitation could be beneficial. However, further studies are needed to improve treatment potential and indications for the conservative management of knee OCD.
Introduction
Osteochondritis dissecans (OCD) is a pathology involving the osteochondral unit, resulting in sequestration of subchondral bone with or without articular cartilage involvement and instability. 1 Although many theories on its etiopathogenesis have been historically proposed, 2 the exact nature of OCD remains unclear. According to the current literature, it can be attributed to either biological (i.e., genetic causes, deficit of ossification centers and endocrine disorders) or mechanical factors (i.e., tibial spine impingement, discoid meniscus, and biomechanical alterations, together with injuries and overuse). These factors act synergically in the pathogenetic progression of the disease by causing subchondral bone ischemia or fracture, which finally determines the onset of OCD. 3
OCD has a prevalence of 15 to 29/100,000 among the general population and an incidence increasing over time. 4 It mostly affects young patients, with a male-to-female ratio of 5:3, mainly between 10 and 20 years old. 1 According to the status of the growth plate, OCD is classified in juvenile (JOCD) and adult (AOCD). The difference between juvenile and adult types is crucial in determining prognosis and treatment. AOCD rarely heals without operative intervention, which includes removal or fixation of the detached fragment, drilling of the lesions, and the restoration of the osteochondral unit through regenerative techniques or the implant of an allograft. JOCD lesions are characterized by a considerably better overall prognosis than AOCD,5-7 but they may also require surgical treatment for unstable lesions or if conservative treatment fails. Stable JOCD lesions are generally managed conservatively, but there is no consensus about the real efficacy and the best nonoperative treatment. 8
The purpose of this study was therefore to systematically review the current literature on conservative management, in order to assess the available evidence on the potential and the indications of the nonsurgical treatment strategies of knee OCD lesions.
Materials and Methods
A systematic review of the literature was performed on the conservative treatment of knee OCD. The search was conducted on September 1, 2017 using the following parameters on 3 medical electronic databases (PubMed, Scopus, and the Cochrane Collaboration): (osteochondritis dissecans) AND (knee). The guidelines for Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) were used. 9 The screening process and analysis were conducted separately by 2 independent observers (LA and AC). In the first step, the articles were screened by title and abstract. The following inclusion criteria for relevant articles were used during the initial screening of titles and abstracts: studies of any level of evidence, reporting clinical results, written in the English language, with no time limitation, dealing with the conservative management of knee OCD. Exclusion criteria were articles written in other languages, reviews and expert opinions, or manuscripts focusing on other joints. In the second step, the full texts of the selected articles were screened, with further exclusions according to the previously described criteria. Reference lists from the selected papers were also screened. Relevant data (type of study, number of patients, age of patients, lesion site, size and stage, type of treatment, follow-up duration, clinical and radiological results) were then extracted and collected in a unique database with consensus of the two observers with disagreements resolved by consensus with a third author (FP), to be analyzed for the purposes of the present article.
Results
The database search identified 1,688 records whose abstracts were screened and selected according to the inclusion/exclusion criteria. As shown in Figure 1 , a total of 55 full-text articles were assessed for eligibility. Twenty-eight full-text articles did not meet the inclusion criteria, and were further excluded, thus leaving a total of 27 studies (published from 1953 to 2017, Fig. 2 )5,6,10-34 to be used for the literature analysis, reporting the results on a total of 908 knees treated conservatively for OCD.
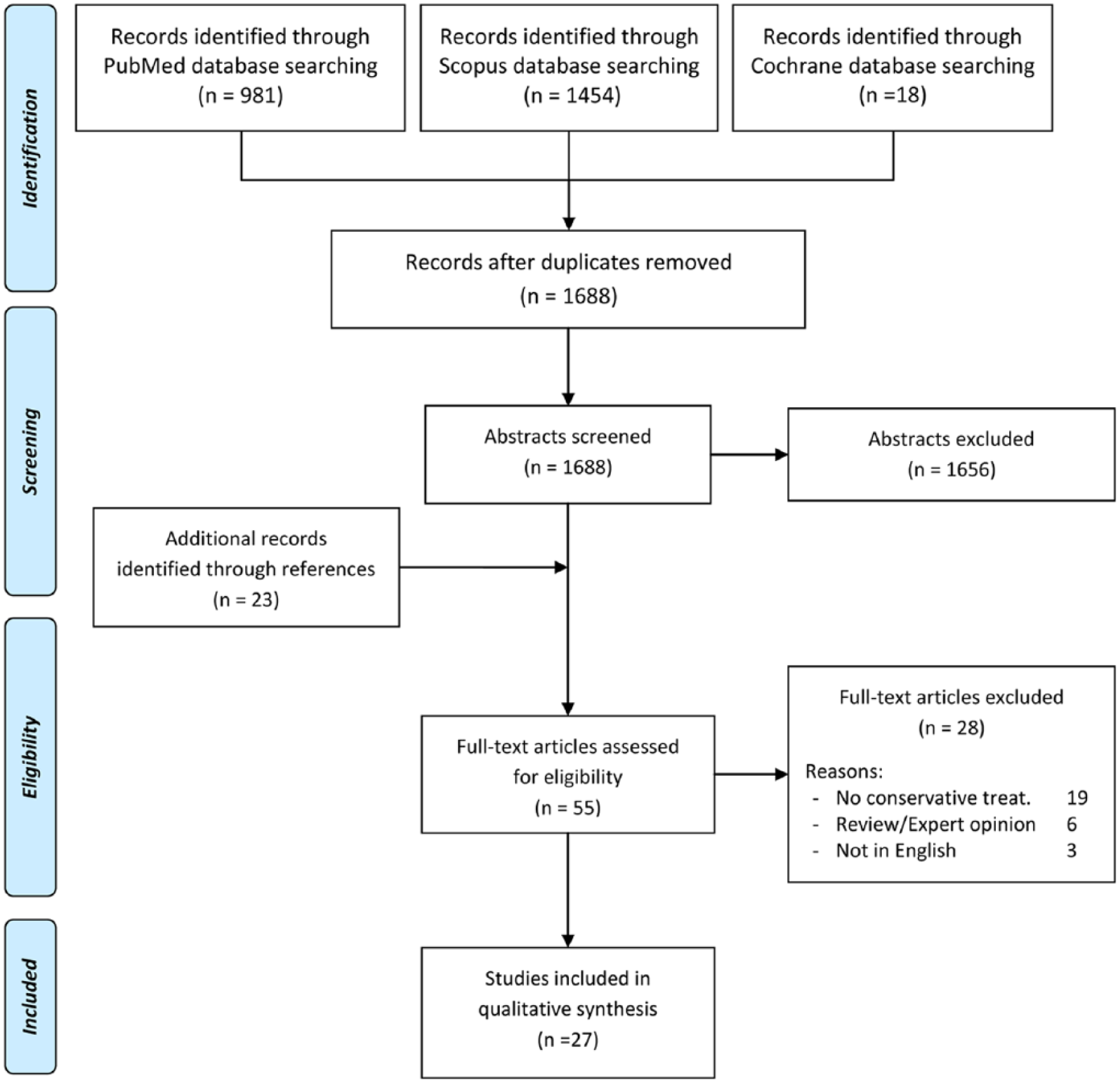
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) flowchart of the systematic literature review.
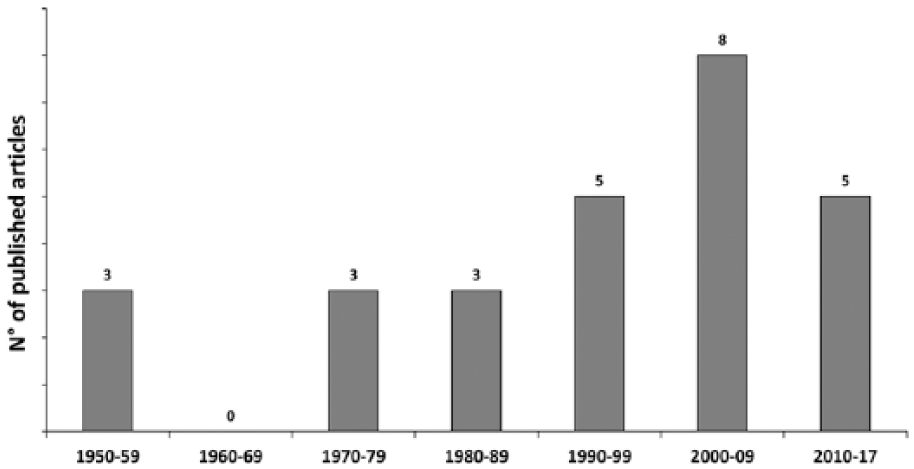
Conservative treatment studies published over time.
No randomized trials or comparative studies were found. Twenty-four articles were case series and 3 case reports. Overall, the studies were heterogeneous regarding the populations analyzed (young and adult patients, stable and unstable lesions), the treatment applied (different techniques and their combination, duration and application modalities), and the evaluation methods (healing definition, follow-up) ( Table 1 ). The patients described in these articles were mostly young patients, affected by stable lesions, thus the conservative treatment was the first-line approach. In particular, 5 different types of treatment could be summarized: (1) restriction of physical activity, (2) physiokinesitherapy and muscle-strengthening exercises, (3) physical instrumental therapies (iontophoresis and extracorporeal shock wave therapy [ESWT]), (4) limitation of weightbearing (partial with crutches or total with wheelchair), and (5) immobilization (with cast or brace). Only 12 studies focused on a single treatment (5 on activity restriction,11,12,14,28,34 2 on physical instrumental therapy,23,32 5 on immobilization),15,21,24,31,33 whereas 14 studies5,6,10,13,16-20,22,25,26,29,30 reported the results achieved with different treatments used either in combination in the same patient or with different indications among patients of the same surveys. Moreover, one study 27 only mentioned that patients were treated without surgical procedures, not specifying the kind of conservative treatment applied. Results were reported at short-term follow-up (<2 years) in 7 studies,12,18-20,23,32,33 at mid-term follow-up (2-8 years) in 9 studies,5,6,11,13-16,21,24,28 and at long-term follow-up (≥8 years) in 5 studies.10,17,22,27,29
Detailed Description of the Studies Selected in the Systematic Review. a
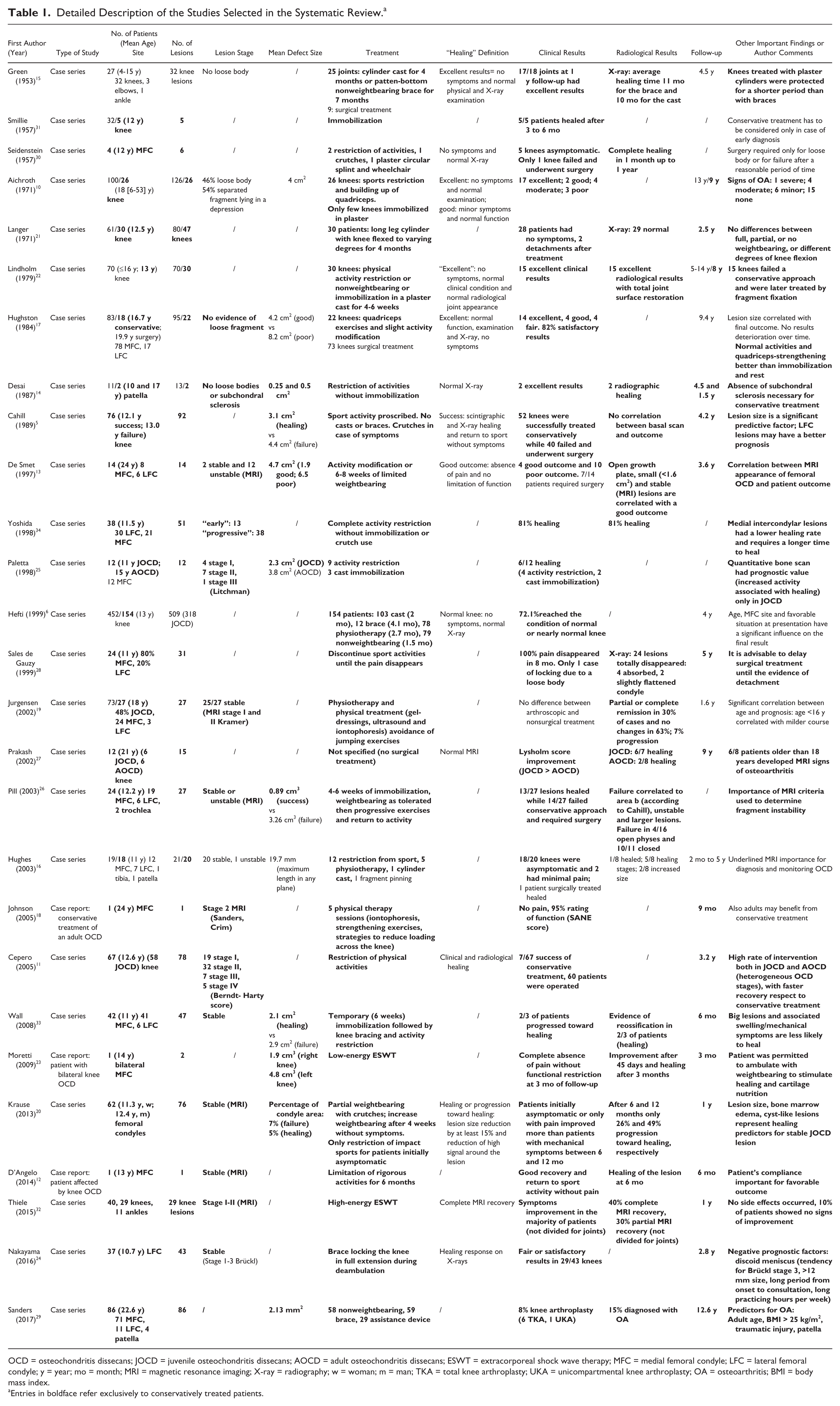
OCD = osteochondritis dissecans; JOCD = juvenile osteochondritis dissecans; AOCD = adult osteochondritis dissecans; ESWT = extracorporeal shock wave therapy; MFC = medial femoral condyle; LFC = lateral femoral condyle; y = year; mo = month; MRI = magnetic resonance imaging; X-ray = radiography; w = woman; m = man; TKA = total knee arthroplasty; UKA = unicompartmental knee arthroplasty; OA = osteoarthritis; BMI = body mass index.
Entries in boldface refer exclusively to conservatively treated patients.
The success of the treatment was assessed by different criteria: the absence of symptoms, a normal knee function, or a radiological improvement. The analysis showed an overall healing rate of 61.4% (487/793), ranging from 10.4% to 95.8% (excluding case reports and studies with less than 5 patients) in the different cohorts analyzed (one study 32 did not report separately the results obtained in different joints and another 29 only reported the need for arthroplasty at long-term follow-up, thus their results could not be considered). While the heterogeneity of these cohorts led to a wide range of reported outcomes, it also allowed to identify some factors having a negative prognostic value on the results of conservative treatments: larger lesion size,5,13,17,20,24,26,33 more severe lesion stages,13,24,26 older age and skeletal maturity,6,19,26,27 medial location in weightbearing areas (although without consensus among different authors),5,6,26,33,34 discoid meniscus, 24 long period from onset to medical consultation, 24 and clinical presentation with swelling or locking.6,33 Moreover, higher body mass index, patellar OCD lesions, and adult OCD were associated to increasing risk of developing osteoarthritis (OA). 29 In a retrospective study, regardless from the conservative management used, 15% of patients at a mean 13 years’ follow-up developed OA, with a cumulative incidence of 30% at 35 years. 29 More detailed aspects of the selected studies, including type of study, number of patients, age, lesion site and stage, treatments, follow-up, and results are reported in Table 1 .
Discussion
The main finding of this analysis is that conservative treatment of knee OCD may provide favorable results in a relevant percentage of patients, but at the same time the available literature does not provide enough evidence in terms of most suitable treatment options and indications.
In fact, the majority of data derive from a small number of low level studies, like case reports or case series, mainly observational, while there is a lack of well-designed randomized controlled trials. Moreover, most of these studies are old, and no significant efforts have been produced in more recent years to increase the study design level and investigate the real potential of conservative treatments for knee OCD. What emerges from the available literature is indeed the lack of consensus about the best conservative protocol to achieve lesion healing, with many proposed strategies. The variety of nonsurgical treatment options may be summarized in (1) restriction of physical activity, (2) physiokinesitherapy and muscle-strengthening exercises, (3) physical instrumental therapies (iontophoresis and ESWT), (4) limitation of weightbearing (partial with crutches or total with wheelchair), and (5) immobilization (with cast or brace).
Most of the authors stressed the importance of a first line nonoperative treatment approach involving restriction of physical activities.5,10-14,16,17,19,20,22,28,30,34 Patients were instructed to stop activities that could cause excessive repetitive and compressive stress on the affected knee, including all strenuous contact sports, running, jumping, squatting and long periods of standing. The treatment was to be continued until symptoms disappeared and radiological aspects progressed toward healing. Good results have been achieved with a complete activity restriction in studies on young patients, also when affected by patellar OCD 14 without immobilization or crutches use, with a clinical or radiological healing rate ranging from 81% to 96%.28,34 Only one study 11 reported a low healing rate of 10%, but applying activity restriction for a heterogeneous population affected also by advanced disease stages. A complete healing can be gained in 6 months, but the full patient’s compliance is crucial, especially considering the young age of the typical patients affected by JOCD. 12
Other authors combined the activity restriction protocol with strengthening exercises for quadriceps and physiokinesitherapy, limiting only to selected knees the immobilization in a plaster. Good results were shown in mid-sized surveys on mixed populations both at mid-term and at long-term follow-up, with 80% to 90% asymptomatic knees16,17 and limited signs of OA. 10
The use of physical instrumental therapy has gained an increasing role in OCD treatment over time. In 2002, Jurgesen et al. 19 treated 27 stable lesions with a conservative approach based on physiotherapy, avoidance of jumping exercises and physical treatment consisting of gel-dressings, ultrasound, and iontophoresis. In a mixed population of JOCD and AOCD they demonstrated radiological signs of partial or complete remission only in 30% of cases, with no changes in 63% of cases and worsening in 7% of cases. In 2005, Johnson 18 reported the case of an adult stable OCD of the medial femoral condyle treated with 5 physical therapy sessions consisting of iontophoresis, strengthening exercises and instruction in strategies to minimize loading across the knee. At 9 months’ clinical follow-up the patient referred no pain, associated with good knee function. In 2009, Moretti et al. 23 treated a 14-year-old boy affected by bilateral knee OCD with low-energy ESWT, whose rational has been suggested to be the increased release of nitric oxide and synthesis of prostaglandin E2 and glycosaminoglycan from cartilage, together with the concomitant decrease of inflammatory factors such as tumor necrosis factor–α and interleukin-10. 35 They observed a complete absence of pain without functional restriction at 3 months’ follow-up; the radiological images demonstrated an improvement of the lesions after 45 days and complete healing after 3 months. A different kind of ESWT (high-level ESWT) was used and analyzed by Thiele et al. 32 in knee and ankle lesions, reporting 40% of complete healing and 30% of partial healing at 1-year MRI.
More restrictive treatment protocols, including limited weightbearing and knee immobilization, have been also investigated. Three articles analyzed the results of limited weightbearing, associated with activity restriction, in symptomatic patients.5,13,20 An overall low success rate was reported in these studies. Cahill et al. 5 obtained satisfactory results only in 52 out of 92 knees with JOCD, while 40 knees failed and underwent surgical treatment within 4 years. Similarly, Krause et al. 20 treated 76 knee JOCD lesions: only 26% and 49% of the lesions (after 6 and 12 months, respectively) had progressed toward healing or were completely healed. Moreover, they were able to prove the correlation between the presence of specific MRI signs, that is, cystic-like lesions, and the clinical outcome after nonoperative treatment. Finally, De Smet et al. 13 reported good results only in 4 out of 14 patients, but these results are probably biased by the high rate of unstable lesions and the average age of the patients including a high percentage of AOCD.
Joint immobilization through the use of cast or brace was evaluated in 9 studies.6,15,21,22,24,26,30,31,33 In the oldest article, published in 1953, Green and Banks 15 proposed a conservative treatment with a plaster leg cylinder cast for an average of 4 months or a patten-bottom nonweightbearing brace on the affected side for an average of 7 months. They treated 25 knees affected by JOCD lesions, obtaining excellent results in 17/18 joints at 1-year follow-up; radiographic evaluation showed that the average time required for evidence of healing was 11 months for the brace and 10 months for the cast. In 1957, Seidenstein 30 treated 1 patient by means of a plaster circular splint in slight flexion, removed after 3 weeks and followed by activity restriction on a wheelchair and avoidance of weightbearing for a period of 8 months, whereupon X-ray showed complete healing. In the same year, Smillie 31 published the results of immobilization in 5 pediatric patients, obtaining a complete healing in 3 to 6 months in every case. A few years later, Langer and Percy 21 treated 30 young patients with the use of a long leg cylinder with knee flexed to varying degrees for an average of 4 months, obtaining a symptom-free condition in 28 of them, without any difference among full, partial, or no weightbearing or different degrees of knee flexion. A shortening of the immobilization treatment duration can be observed in the literature of the following years. Lindholm and Österman 22 treated 30 young patients with physical activity restriction or nonweightbearing or immobilization for 4 to 6 weeks in a plaster cast, obtaining a low rate of healing: 15 out of 30 knees reached excellent clinical and radiological results with total joint surface restoration, whereas the other 15 knees failed the conservative approach and were later treated by fragment fixation. Also Pill et al. 26 suggested 4 to 6 weeks of immobilization with as tolerated weight-bearing, followed by progressive range of motion and exercises, with good results in 13/27 lesions. Interestingly, the cases presenting worst results were characterized by closed physis and larger or unstable defects. Wall et al. 33 adopted a specific therapeutic protocol to enforce knee rest in skeletally immature patients by placing the patient in a cylinder or long leg cast initially for 6 weeks. If X-ray showed reossification at 6 weeks, the patient was placed into a double-hinged, unloader-type brace. The brace was adjusted into valgus for medial compartment lesions and into varus for lateral lesions, sports restriction was also implemented until further ossification of the lesion was seen. At 6 months’ follow-up, 2/3 rate of healing was obtained. Hefti et al. 6 performed a large multicenter study on a mixed population; 103 lesions were addressed by 2 months cast and 12 by 4 months brace. They reported an overall normal or nearly normal condition of the knee in 72.1% of the patients at 4 years’ follow-up, even if it was not possible to identify specific outcomes according to the different treatment approaches adopted in these series. This large study also allowed to underline prognostic factors, useful to identify what kind of patients and lesions may benefit from a conservative approach. This aspect has been further investigated by a recent study by Nakayama et al. 24 who found a strong negative correlation for patients with discoid meniscus, and a tendency for lower outcome for Brückl stage 3, lesions diameter larger than 12 mm, long period from onset to consultation, and long practicing hours per week. In general, the different prognostic factors identified by the studies included in this review, were lesion size,5,13,17,20,24,26,33 location,5,6,26,33,34 stage,13,24,26 patients’ age and skeletal maturity,6,19,26,27 etiology, 24 as well as clinical presentation.6,24,33
The size of the OCD lesion was recognized as a prognostic factor by several studies,5,13,17,20,24,26,33 with bigger lesions presenting worst results and a lower healing rate, even though the authors suggested different cutoff values, thus not allowing an absolute prognostic indication. With regard to the studies specifically reporting conservative treatments for stable lesions, Cahill et al. 5 observed 3.1 cm2 mean size in healed patients against 4.4 cm2 in failures, while Wall et al. 33 described a mean size of 2.1 and 2.9 cm2 for healed and failed lesions, respectively. Krause et al. 20 assessed a cutoff based on the percentage of condylar area affected by the OCD lesions, being 5% in healed and 7% in failed lesions. Nakayama et al. 24 found a tendency for worse outcome in lesions larger than 12 mm in sagittal radiographs. Regarding the location, medial lesions were reported to have a worst outcome,5,33,34 except for one study where a higher healing rate was found for lesions located on the medial femoral condyle near the fossa. 6 Another study found that failures were correlated to the presence of lesions in the central part of condyles in the sagittal view, regardless of the medial and lateral site. 26 Three studies13,24,26 investigating different lesion stages, found worst results for unstable lesions at MRI, confirming that the conservative treatment should be limited to patients with stable lesions. The onset of OCD associated with the presence of a discoid meniscus was found to be severely prognostic in a study on 43 knees. 24 The authors speculated that contact with oversized meniscus induces excessive stress at the articular surface during motion, and repetitive overload applied to weaker osteochondral structures in the growing period may affect the healing process of the bony lesion. The OCD lesion in this region may develop after discoid meniscectomy due to a similar pathomechanism. 34
Beside the lesion characteristics, factors related to the patient were also found to influence OCD prognosis. The initial clinical assessment of the patient may have a prognostic value: Wall et al. 33 showed that lesions causing swelling and mechanical symptoms are less likely to heal, while Hefti et al. 6 stressed the importance of the absence of swelling in order to achieve significantly better results after conservative treatment. Moreover, also the period from onset to consultation has a prognostic value, 24 likely because the treatment delay may allow progression in disease processes and joint homeostasis changes. Finally, patients’ age is an important factor. In fact, Hefti et al., 6 Jurgensen et al., 19 and Pill et al. 26 found a significant better outcome in patients with open physes than in those with closed physes. Moreover, studies on patients with a higher average age,19,20 and therefore a higher skeletal maturity, presented the lowest success rate of 30%, which affects the overall results reported in the literature not reflecting the outcome suggested by the other available studies on the conservative approach.
In general, this review documented an overall success rate of 61.4%, but this average value should be interpreted with caution due to the heterogeneous study populations, with patients of either open or closed physis and a wide age range, treated with different strategies and with a different evaluation in terms of outcome and follow-up. In fact, the definition itself of healing/success differs among studies. Moreover, imaging results are seldom analyzed and reported. Only one study 29 was focused on the long-term development of OA, reporting a cumulative incidence of 30% at 35 years, with higher risk for patients with higher body mass index, patellar OCD lesions and adult OCD. All these aspects are limitations for the literature analysis, and more in general represent the limitations of the poor available evidence on this topic. Table 2 highlights the most important aspects underlined by this literature review, to be considered for clinical treatment decision, as well for any future study design on this topic, with references to already documented clinical relevance, if present.
Important Aspects for Clinical Treatment Decision and for Future Study Design on the Conservative Treatment of OCD.
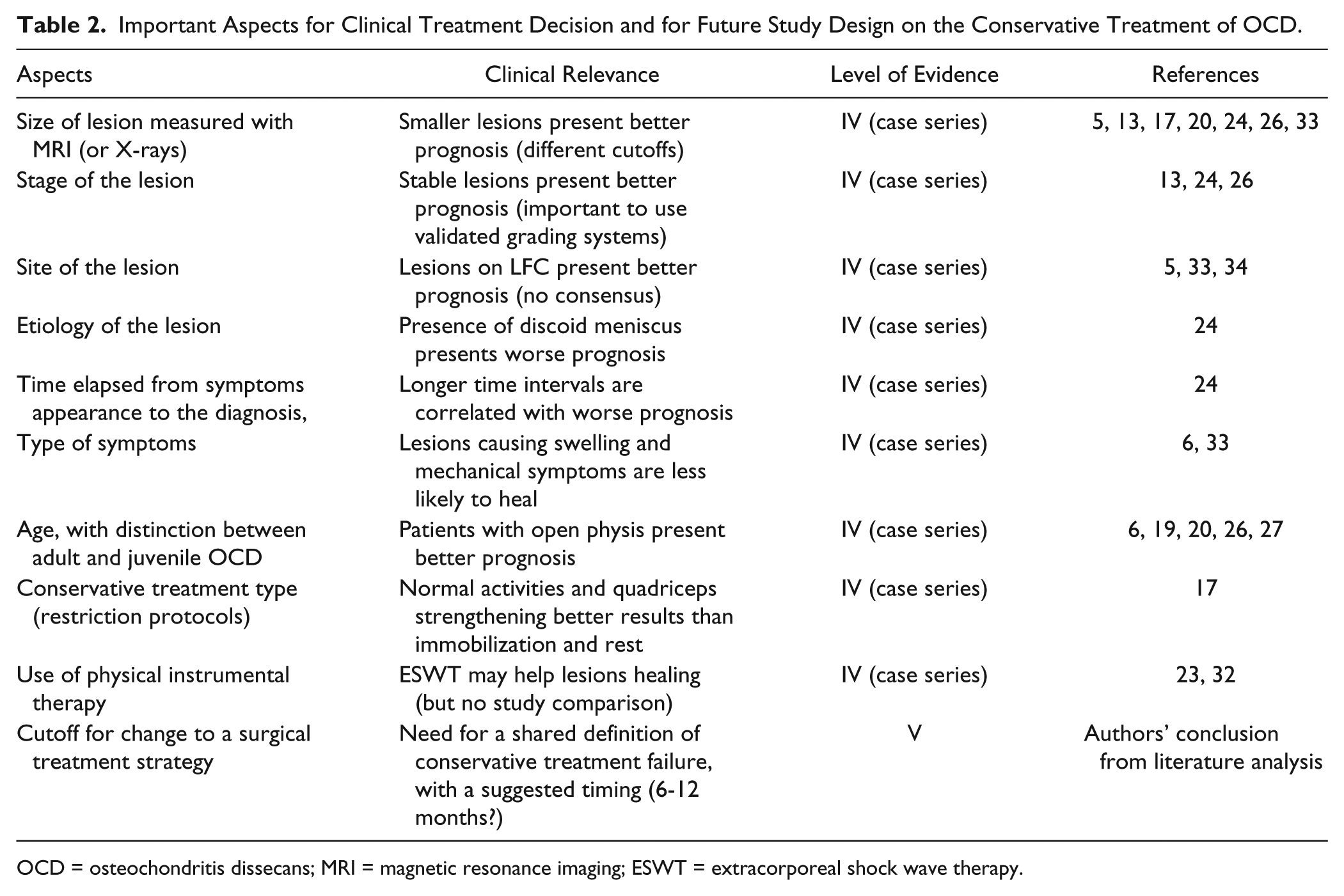
OCD = osteochondritis dissecans; MRI = magnetic resonance imaging; ESWT = extracorporeal shock wave therapy.
According to the current review, a conservative treatment based on restriction of sport and strenuous activities seems a favorable approach, whereas there is no evidence that further activity restriction could be beneficial, 10 thus suggesting the possibility to allow daily activities, possibly combined with quadriceps strengthening, without the need for immobilization and rest. 17 Moreover, even though the heterogeneity of these studies may bias the strength of the literature indications, a beneficial effect of weight-bearing limitation is not supported by clear evidence. Finally, physical instrumental therapies, either applied for their supposed disease modifying or symptom control effects, are only documented in anecdotic reports. Based on the current literature, no evidence-based advices can be made about the optimal timing for changing from a conservative to a surgical treatment strategy. Nevertheless, it has been generally considered when conservative treatment failed, with patients having no improvement or worsening of the symptoms or at MRI evaluation, within 6 to 12 months. While some time is necessary to allow conservative treatment to be effective, no evidence is actually available on a cutoff time to guide physician to decide toward a more aggressive surgical approach. Thus, until scientific evidence will help understanding this delicate aspect, the treatment timing decisions remains unclear and based on the physician understanding on the development of the specific patient conditions, as well as the compliance and expectations of the patients itself. To this regard, it is advisable to consider the described prognostic factors, leaving more time to heal to lesions presenting with a more positive prognosis. Anyway, if healing of the lesions should be documented with symptoms resolution or images normalization, and at which follow-up, remains to be determined.
OCD lesions are a relevant problem that may affect the long-term prognosis of young patients and not enough attention is currently paid to their conservative management. In fact, the available studies are mainly of poor quality, and not enough research effort has been dedicated in recent years to unravel this topic. Thus, while the literature analysis only allows to offer general indications on the benefit of physical activity limitation, and on the patients with a better prognosis, further high-level studies are necessary to understand the potential of the available strategies and to optimize them in order to improve the conservative management of young patients with stable knee OCD lesions.
In conclusion, the literature on conservative treatments for knee OCD is scarce, with the majority of data derived from a small number of low-level studies, mostly old and without significant research efforts produced in more recent years. The different nonsurgical treatment options may be summarized in: restriction of physical activity, physiokinesitherapy and muscle-strengthening exercises, physical therapies, limitation of weightbearing, and immobilization. Among these, restriction of sport and strenuous activities seems a favorable approach, whereas there is no evidence that further activity restriction, physical therapy, immobilization, or weightbearing limitation could be beneficial. Not all patients may benefit from conservative treatments, and negative prognostic factors have been identified in larger lesion size, more severe lesion stages, older age and skeletal maturity as well as clinical presentation with swelling or locking. Further studies are needed to improve the conservative management of knee OCD.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Giuseppe Filardo received institutional support from Zimmer-Biomet (USA); he is consultant and received institutional support from Cartiheal (Israel); he is consultant and received institutional support from Fidia (Italy); he is consultant and received institutional support from Finceramica (Italy); he is consultant and received institutional support from Green Bone (Italy); he received institutional support from DSM Biomedical (USA); he received institutional support from IGEA Clinical Biophisic; and he received institutional support from PIRAMAL/Smith-Nephew.