
Abstract
Objective
The purpose of this manuscript is to analyze the evidence regarding etiopathogenesis of knee osteochondritis dissecans (OCD) lesions through a systematic review, so to summate the current understanding of the origin and progression of this pathologic articular processes.
Design
A systematic review of the literature was performed on the PubMed and Cochrane databases on October 2017 by 2 independent authors and included all levels of evidence. This included all English language literature, pertaining specifically to etiopathology of knee OCD with exclusions for review articles and expert opinion. Of 965 identified records, 154 full-text articles were assessed for eligibility and 86 studies met the inclusion criteria.
Results
According to these studies, the etiology of OCD can be of a biological or mechanical origin: 40 articles proposed a biological hypothesis, including genetic causes (27), ossification center deficit (12), and endocrine disorders (9); conversely, 52 articles supported a mechanical hypothesis, including injury/overuse (18), tibial spine impingement (5), discoid meniscus (16), and biomechanical alterations (20) as the cause of the onset of OCD. The pathogenic processes were investigated by 36 of these articles, with a focus on subchondral bone fracture and ischemia as the ultimate events leading to OCD.
Conclusions
Biological and mechanical factors are found to result in subchondral bone remodeling alterations, acting independently or more likely synergically in the progression of knee OCD. The former includes genetic causes, deficit of ossification centers and endocrine disorders; the latter, tibial spine impingement, discoid meniscus, and biomechanical alterations, together with injuries and overuse. The resultant subchondral bone ischemia and/or fracturing appears to determine the onset and progression of OCD.
Level of Evidence
Systematic review of level II-IV studies, level IV.
Introduction
Osteochondritis dissecans (OCD) is a pathology known for centuries, 1 even before König 2 coined the term in 1888, which is currently in use. It defines a pathologic process involving the osteochondral unit, resulting in delamination and sequestration of subchondral bone with or without articular cartilage involvement and instability. 3 Orthopedic surgeons, family doctors, and sports medicine specialists should be aware of this condition, since OCD is not a rare source of knee pain and dysfunction, mostly affecting young patients between 10 and 20 years of age, 3 with a prevalence of 15 to 29 per 100,000 population and an incidence reported to be increasing.4,5 Its impact on those affected varies significantly, with skeletal age at time of symptoms onset being the most important prognostic factor, in terms of selecting intervention algorithm and predicting outcome success. Thus, the disease is essentially divided into two categories according to the time of clinical recognition as either juvenile OCD or adult OCD. The former affects skeletally immature patients and has a generally better prognosis 6 the latter is typical of young adult patients (defined by closed physis) and typically presents a poorer prognosis. 7 Theories on the etiopathogenesis are postulated to explain both the occurrence, progression and thus the prognosis of OCD. Historically, traumatic events were deemed to be the cause of the loose bodies, but over the centuries this theory was dispelled by others, such as “quiet necrosis” by Sir James Paget or the inflammatory theory of König. 1 Although the shortcomings of these hypotheses were highlighted by subsequent advancements in research, the exact nature of OCD remains elusive.
The purpose of this study is to assess the available evidence on the etiopathogenesis of knee OCD lesions through a systematic review, to better understand the origin and progression of the pathologic processes and possibly identifying areas for future curative therapeutic intervention.
Methods
A systematic review of the literature was performed. The search was conducted on the PubMed and Cochrane databases on October 2, 2017 using the following parameters: ((osteochondritis dissecans) AND (knee)). The guidelines for Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) were used. 8 The screening process and analysis were conducted separately by two independent observers. In the first step, the articles were screened by title and abstract. Inclusion criteria for relevant articles used during the initial screening were reports of all levels of evidence, English language, no time limitation, specific to etiopathology of knee OCD. Exclusion criteria were reviews and expert opinions, or manuscripts with focus on joints other than the knee. In the second step, the full texts of selected articles were evaluated for exclusion according to same criteria. Reference lists from the selected papers and from the excluded reviews were reviewed for potential further potentially inclusive reports. Relevant data (type of study, number of patients, demographic of study population, lesion site, proposed theory for etiology and pathogenesis, and remarks) were then extracted. The etiologic theories about OCD proposed in the selected articles were the divided into biological and mechanical, based on the prevalent hypothesis endorsed in each study. A unique data set, composed of consensus of the 2 observers (LA and AC), was established and then analyze for the purposes of the present manuscript.
Results
The PubMed and Cochrane search after duplicates removal identified 965 potential abstracts for inclusion, which were screened, as shown in Figure 1 , for a total of 154 full-text articles assessed for eligibility. Sixty-eight full-text articles were further excluded, thus leaving a total of 86 studies to meet the inclusion criteria and use for the literature analysis. These included studies from 1953 to 2017 and ranged from cohort studies up to 133 patients to laboratory studies up to 64 specimens. Of interest an increasing number of studies, almost half of the included articles, have been published in the past 7 years (42/86) ( Fig. 2 ).
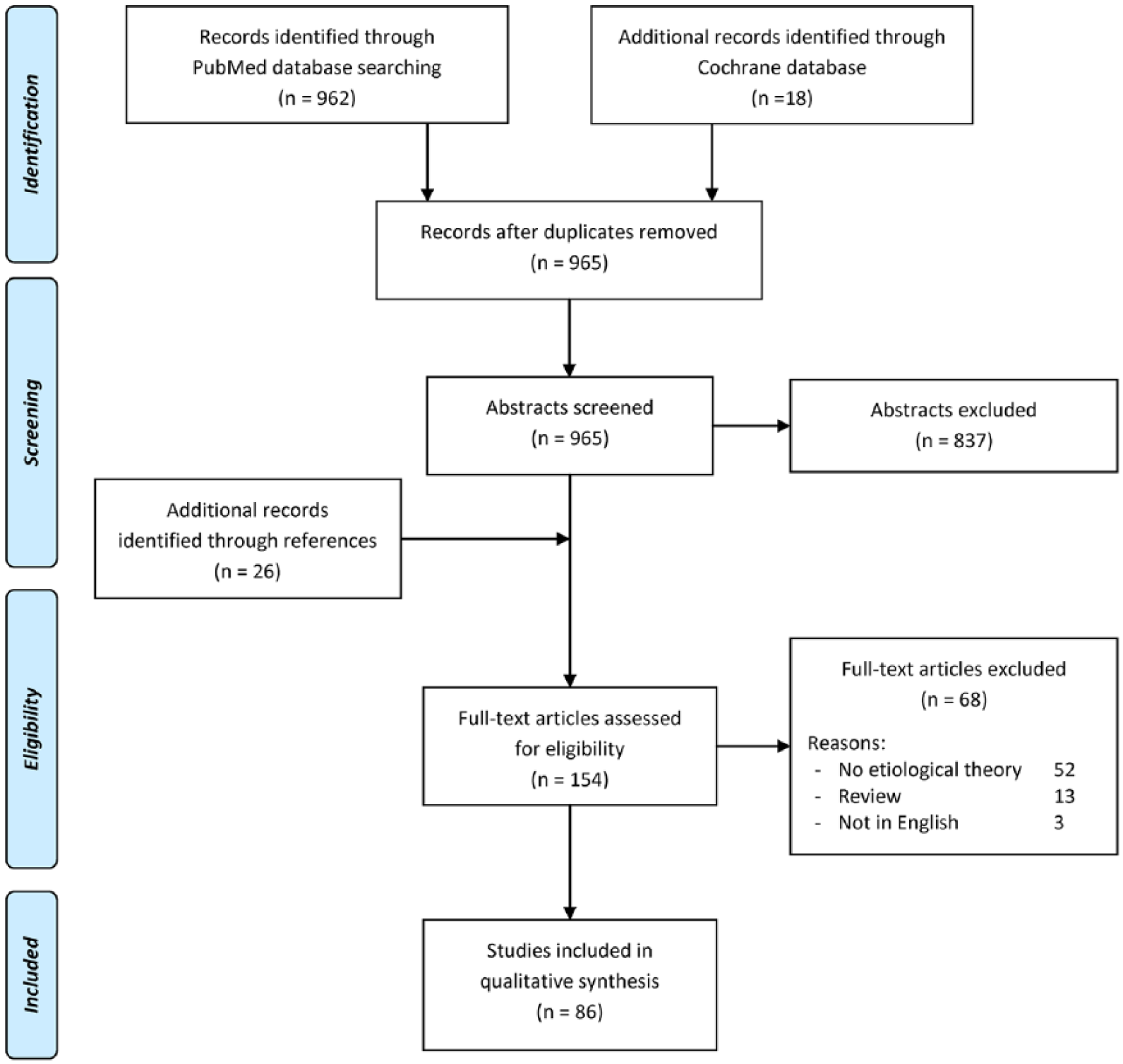
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) flowchart of the systematic literature review.
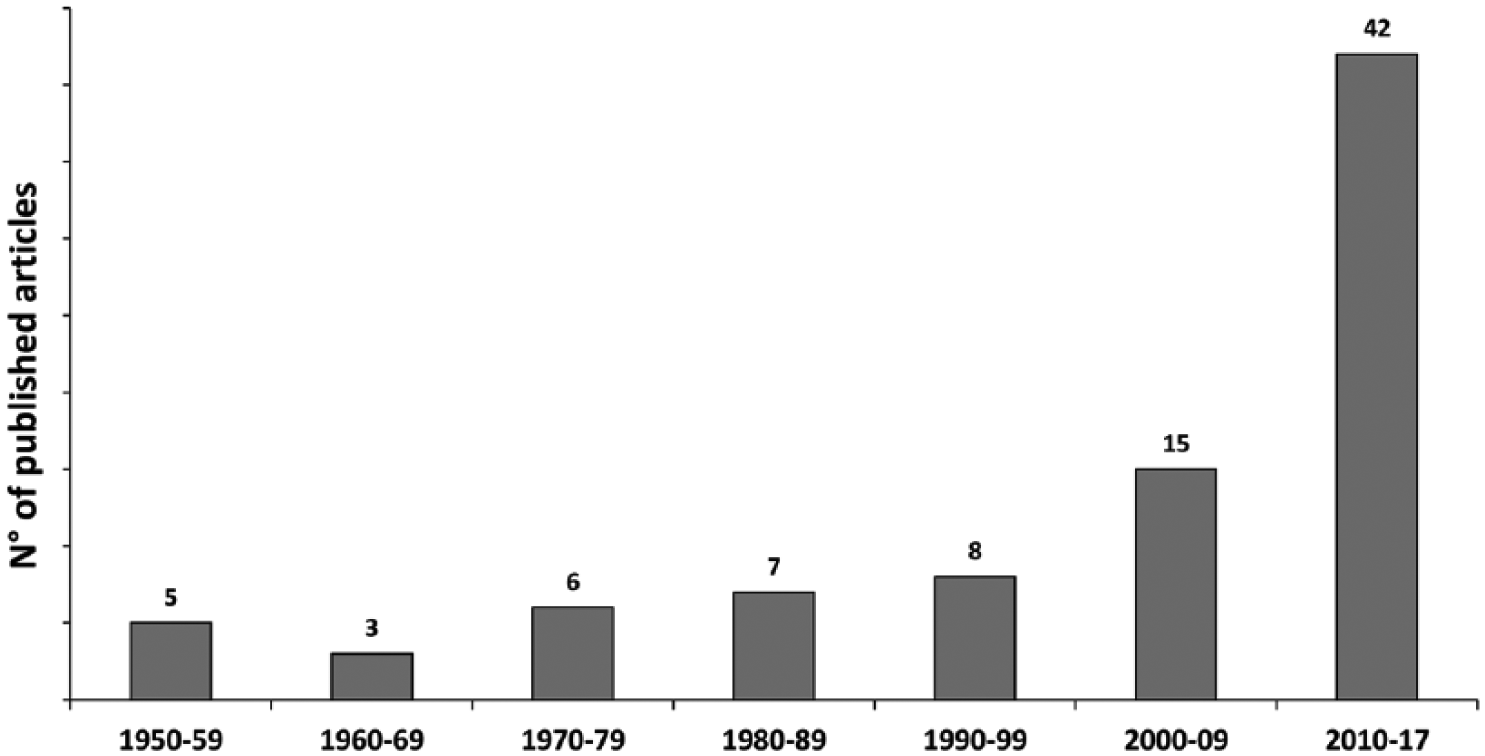
Etiopathogenesis studies published over time.
The levels of evidence of the included studies included: 39 case reports, 31 case series, 11 laboratory studies and 5 comparative studies. Among the included studies, 40 articles proposed a biological hypothesis,9-47 including genetic causes (n = 27), ossification center deficit (n = 12), and endocrine disorders (n = 9). Conversely, 52 articles supported a mechanical hypothesis,12,13,17,29,34,35,47-92 including injury/overuse (n = 18), tibial spine impingement (n = 5), discoid meniscus (n = 16), and biomechanical alterations (n = 20) as the cause of OCD onset.
Among biologic theories, genetic factors are the most investigated, with 27 studies on 548 patients. Theories vary from an autosomal dominant pattern of inheritance in older studies,39,40 to the association with genetic determined diseases12,27 and to gene mutations causing protein alteration leading to OCD in more recent articles.20,21,44 Other biological hypothesis concerned a deficit in the ossification center; one of the first theories was described in 1955 34 and was analyzed in 12 studies on 153 patients, or lastly endocrinological factors (including vitamin D deficit,10,42,43 glucocorticoid alterations, 14 human growth hormone (hGH) deficiency, 18 or association with endocrinologic and sexual abnormalities), 36 stressed in 9 studies reporting data of 180 patients.
Among mechanical theories, the traumatic theory was the first one described in the early 1950s. 35 This hypothesis, however, has evolved from that of a single event macrotrauma to one proposing repetitive microtraumatic. None the less, it remains one of the most accepted of the proposed etiologies with 18 articles on 297 patients. The other mechanical theories have gained interest more recently. Biomechanical alterations represent one of the most described theory, reported in 20 studies on 527 patients. This category includes lower limb deviation,59,91 ligament or meniscus instability,50,53 knee anatomical features,56,88 shearing stress on patella,71,80 or knee activity–related position. 87 Discoid meniscus was first described in 1984 as factor associated with OCD lesions, and subsequently gained increasing credit, being described in 16 studies on 260 patients. The majority of those described the association between lateral discoid meniscus and lateral femoral condyle (LFC) OCD, but the presence of medial discoid meniscus has also been associated with OCD of the medial femoral condyle (MFC). 51 Discoid meniscus plays its role in the etiopathogenesis of OCD both if normal or torn, and also related meniscal surgical procedures may influence the history of OCD lesions. 89 Finally, tibial spine impingement represents a most recent theory, first described in the late nineties, and it was supported by 5 studies on 97 patients. However, this may explain only the “classic” OCD lesion (secondary to juxtaposition), on the notch side (lateral aspect) of the MFC.
Interestingly, analyzing the number of articles published over the decades by etiology ( Fig. 3 ), a shift is seen in the past 20 years from biologic toward mechanical hypothesis. In fact, 55% of the articles published in the past century supported a biologic theory, while 61% of the studies published from 2000 to 2017 supported the mechanical hypothesis. Overall, based on the number of studies supporting their importance, the strongest factors are genetic causes (27), biomechanical alterations (20), injury/overuse (18), and discoid meniscus (16). Fewer studies supported the importance of ossification center deficit (12), endocrine disorders (9), and tibial spine impingement (5). Nevertheless, also these factors are likely to significantly contribute to the onset of OCD in some patients, with the importance of each factor and the interplay among concomitant factors leading to OCD being related to the specific case.
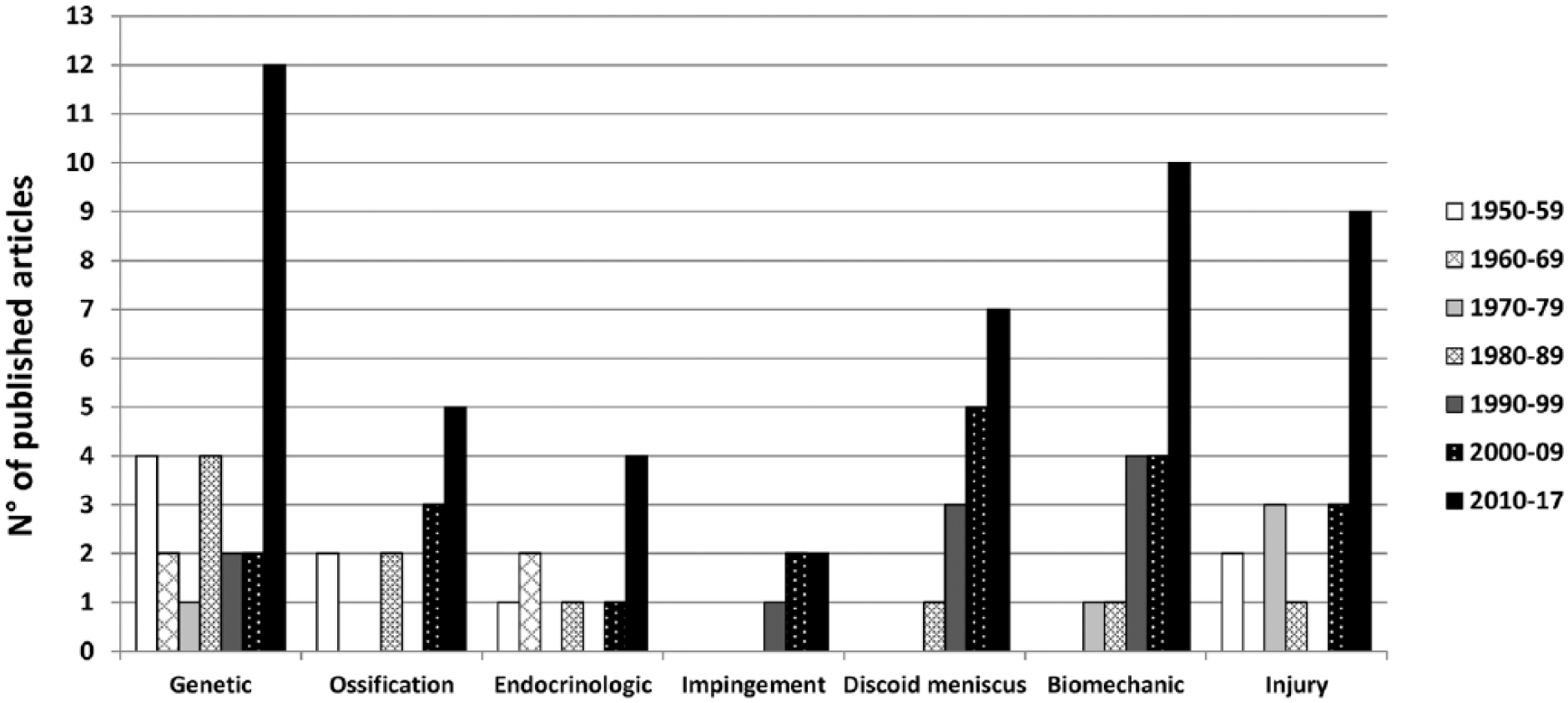
Trend of etiological hypothesis over time.
The cascade of events leading to OCD was specifically described in 36 articles, with subchondral bone fracture (28 articles) or subchondral bone ischemia (8 articles) as the most common final pathogenetic mechanisms ( Fig. 4 ). While subchondral bone is almost universally recognized as the primarily affected tissue, one article suggested that OCD is a cartilaginous disease with the subchondral bone secondarily damaged. 19
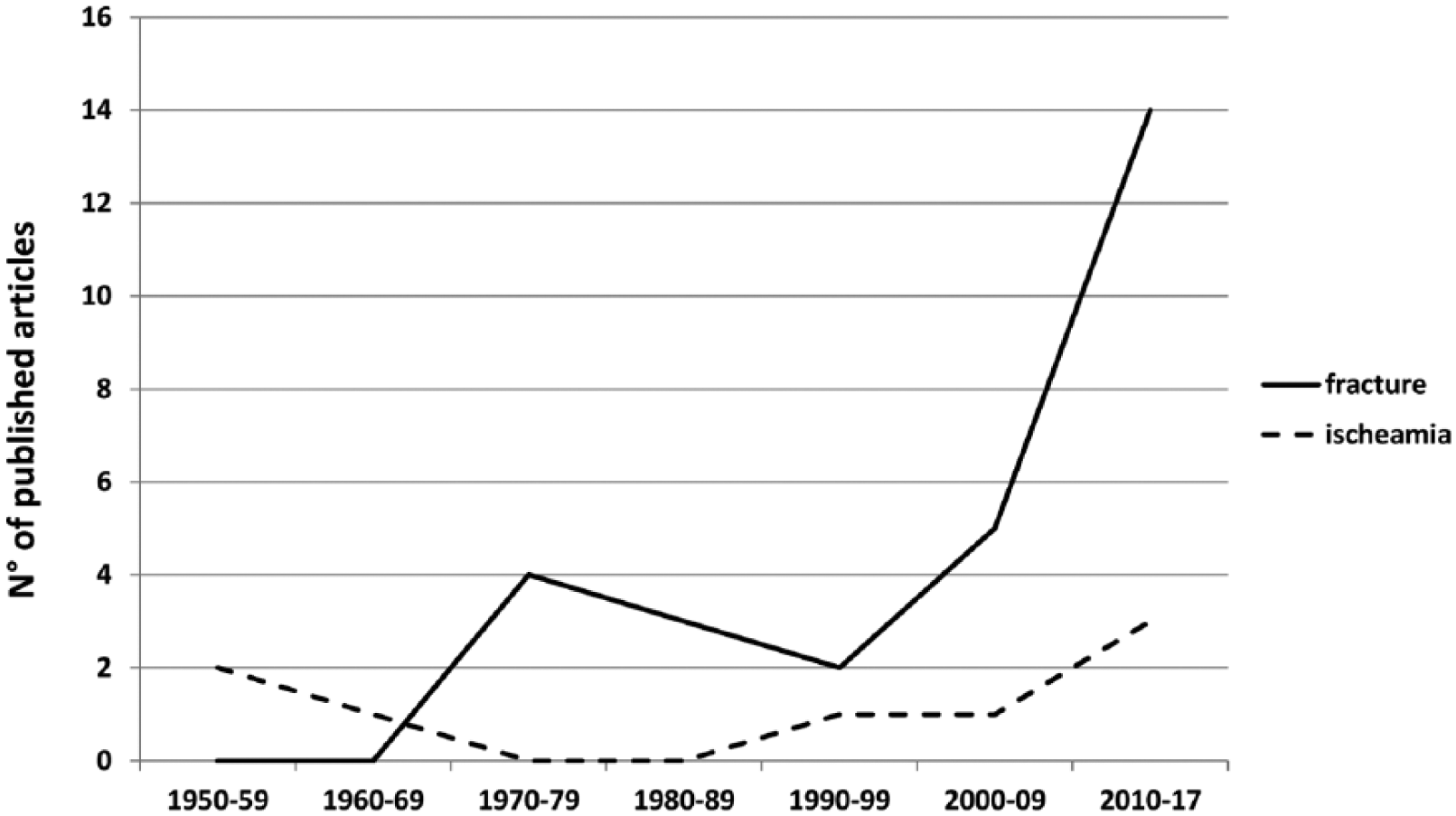
Trend of pathogenetic theories over time.
More detailed aspects of the selected studies, including type of study, number of patients, age, lesion site, proposed theory for etiology and pathogenesis, and results, are reported in Table 1 .
Detailed Description of the 86 Studies Selected in the Systematic Review.
hGH = human growth hormone; JOCD = juvenile osteochondritis dissecans; LFC = lateral femoral condyle; LM = lateral meniscus; MFC = medial femoral condyle; MRI = magnetic resonance imaging; MZ = monozygotic; OA = osteoarthritis; OCD = osteochondritis dissecans.
Discussion
This systematic review presented the entire spectrum of evidence on the etiopathology of OCD in the knee. The main study finding is that, based on the results provided by the selected articles, OCD can be caused by biological and/or mechanical factors. Furthermore, most of the studies identified subchondral bone fracture and ischemia as the ultimate cause in the pathogenetic processes leading to knee OCD.
It has to be pointed out that the level of evidence for the literature on OCD etiopathogenesis is generally low, with several case reports and studies reporting a relatively low number of patients. More over these studies are very heterogeneous for what concerns methods and results, thus making impossible to perform a quantitative evaluation of the overall data reported. Nevertheless, the theories documented in the current literature were reported, summarized and critically analyzed to best fit the spectrum of hypotheses into a etiopathogenic categorical framework ( Fig. 5 ).
Framework of the etiopathogenetic theories documented in the current literature.
Biological Etiological Factors
Genetic Hypothesis
Several authors9,11-13,15,16,19-23,27,28,30,32,33,35-41,44,46,47,93 found a familial occurrence of OCD and some also identified specific gene alterations which can directly or indirectly cause the disease. Stattin et al. 20 identified a possible candidate gene, the ACAN gene, which encodes a protein involved in the organization of the aggrecan network, whose alteration leads to the disruption of extracellular matrix interactions causing a familial OCD with an autosomal dominant inheritance. Extra-cellular matrix alterations were also investigated by Jackson et al., 21 who found that patients with type IX collagen gene mutations presented OCD lesions combined with multiple epiphyseal dysplasia and a form of mild myopathy. They postulated that the expression of mutant type IX collagen may elicit a stress response involving endoplasmic reticulum and mitochondrial function. Skagen et al. 19 speculated a role for altered chondrocyte extracellular matrix synthesis that may cause similarly effect endoplasmic reticulum storage. This effect then disturbs the endochondral ossification leading to OCD.
Alterations of bone remodeling and bone quality were found to be associated with OCD in 2 case reports about patients affected by systemic disease. Kilic et al. 27 described a patient with hyper IgE syndrome who developed a knee OCD lesion, proposing osteopenia related to the immunologic condition may represent an etiological factor. Park et al. 12 described development of OCD in a patient affected by Wilson disease, suggesting a correlation between the osteochondral lesion and osteoporosis, osteomalacia, and copper deposition in joints typical of this genetically determined condition.
Several reports describe patients affected by OCD within families and among several generations, stressing the importance of a genetic susceptibility and considering the frequent involvement of both in monozygotic twins.11,13,15,19,22,30,35,47 Nevertheless, Petrie et al. 94 examined first- and second-degree relatives of 34 patients with OCD and found only 1 affected by OCD, concluding that the most common form of this disorder is not familial.
Ossification Deficit Hypothesis
Defects in the ossification centers of the distal femur are thought to predispose to OCD lesions.15,17,19,24-26,29,30,32,34,45 Ribbing 34 was the first (1955) to describe an accessory bone nucleus detachment in childhood, that may partly fuse during adolescence into the adjacent cancellous bone, remaining partially separated from the latter by islands of persisting cartilage. The incomplete connection between the vascular system of the bone nucleus causes a locus minoris resistentiae, which enables mild injury or strain to produce a slight dislocation with deleterious effects and the separation of the osteochondral unit. Pathologically this seemed consistent with analysis of loose bodies later performed by Barrie. 29 Conversely, Laor et al. 17 suggested how an exogenous chronic mechanical insult can affect endochondral ossification of the physis resulting in juvenile OCD.
The detection of pathologic ossification can be challenged by the presence of physiologic variants. In fact, in skeletally immature patients, early stages of OCD might be confused with normal ossification variants, which might account for the “better prognosis” of JOCD with respect to AOCD. 26 Jans et al. 58 confirmed the independent occurrence of normal variants and OCD in a comparative study on large cohorts of patients: 12% out of 116 patients affected by OCD presented normal ossification variants, the same percentage reported in the analysis of the healthy population. A correct differential diagnosis is thus fundamental to prevent unnecessary treatment: location in the inferocentral posterior femoral condyles with intact overlying cartilage, accessory ossification centers, spiculations, residual cartilaginous model, and lack of bone marrow edema are features of normal variants and not typical of OCD.
Endocrine Hypothesis
Hormonal alterations might affect bone metabolism by inducing a process of bone remodeling and subsequent onset of osteochondral lesions. A link between various endocrine abnormalities and OCD was first suggested in 1981 by Mubarak and Carrol, 30 who observed a common occurrence of endocrine dysfunction in their patients, but the endocrine theory was further explored only recently.10,14,18,30 In 2013, Kröger et al. 14 documented 13 cases of OCD in children with juvenile idiopathic arthritis, and suggested either an alteration of the articular surface due to the persistent synovitis, or the possible detrimental effects of glucocorticosteroid injections on cartilage metabolism. Hussain et al. 18 focused instead on changes in hGH levels (it is still not clear whether it is the deficit itself or the hormone supplementation) which may lead to atypical ossification nuclei and subsequent OCD lesions. Finally, in 2014, Bruns et al. 10 shed light on another contributing factor in the progression of the pathology, with 21 out of 23 patients affected by OCD presenting low vitamin D3 levels.
Mechanical Etiological Factors
Injury and Overuse
Historically, the most advocated theory is the traumatic one, even though a singular macrotrauma was not found to be common, but rather a curiosity.12,13,29,31,35,48,55,58,60-62,68,69,79,81,86,92 Shea et al. 55 reported the case of a patient who developed OCD after an acute traumatic event and proposed a correlation between femoral condyle bone contusion and disease development as an explanation for the OCD finding. What seems more likely is repetitive microtrauma or chronic loading might play a role in the OCD etiopathogenetic process. These events can act by themselves48,55,58,60-62,68,79,81 or in combination with other predisposing factors, (e.g. biological or the other mechanical factors).
Tibial Spine Impingement Hypothesis
In 1933, Fairbank was the first to suggest the role of tibial spine impingement against the lateral aspect of the medial condyle as an etiological factor for OCD: abnormal shear forces, caused by the impingement, are generated during internal rotation of the tibia with loading in flexion. 95 Bramer et al. 67 extended this hypothesis noting increased external tibial torsion might play a role, compensating for the externally rotated position of the foot. Although this theory fails to account for OCD lesions at other sites, it has been subsequently advocated by several authors, thus suggesting that impingement is a valid explanation for OCD in specific joint locations.49,63,67,73,84
Discoid Meniscus Hypothesis
A link between the discoid meniscus variant and femoral condyle OCD is well described.13,51,54,64-66,69,72,74,76,78,82 The alterations of joint mechanics produced by the presence of a discoid meniscus may cause an increase in peak loading forces to the subchondral bone lesion predisposing onset of fragment formation. 66 This hypothesis is supported by the fact that the lateral location is uncommon for OCD except in patients with discoid lateral meniscus. 65 Furthermore, Deie et al. 65 even linked the type of lateral discoid meniscus, complete or incomplete, to OCD at specific sites of the lateral femoral condyle.
Although it is likely that the abnormal menisci may cause OCD due to the effect of repetitive abnormal stress on weaker osteochondral growing structures, 63 it is still unclear whether the link derives more from the presence of an intact discoid meniscus,65,82 a torn discoid meniscus,51,78 or if it is secondary to the alterations provoked by the meniscectomy of the discoid meniscus.64,66,69,74
More controversial is the role of skeletal maturity on the effects of discoid meniscus presence. While Mitsuoka et al. 72 underlined the consequences of the abnormal stress produced by a discoid meniscus on the weaker osteochondral structures in the growing period, Kilcoyne et al. 82 stated that the link between discoid meniscus and OCD extended also beyond the skeletally immature phase.
Biomechanical Alteration Hypothesis
Abnormal biomechanics may have chronic effects on the articular load distribution with a marked impact on the joint homeostasis, which may also contribute to onset of OCD.47,50,52,53,56,57,59,63,64,67,70,71,74,75,77,80
Many conditions can account for this, such as meniscectomy, joint instability, genu recurvatum, and condylar flattening, that increase contact forces at the joint and explain chronic repetitive microtrauma.5,96 Camathias et al. 53 suggested that meniscal instability, specifically a hypermobile anterior horn, might be a decisive factor in the origin of OCD. The meniscus in this condition may work like a “doorstop,” so that the peripheral edge of the loose meniscus impinges repeatedly between the tibial plateau and femoral condyle as the knee moves from flexion to extension, in the end damaging the corresponding femoral osteochondral unit. 53
Other examples of OCD associated with biomechanical alterations include: a greater tibial slope, 52 a more prominent lateral femoral condyle, 56 or the agenesis of both cruciate ligaments causing anteroposterior instability. 50 Similarly, varus or valgus deviations of the knee lead to increased mechanical loading of the respective knee compartments.57,59,75 Besides femoral condyles, the patellar surface may also suffer from abnormalities, thus causing a biomechanical disequilibrium: an atypical patellar surface 71 as well as a recurrent patellar subluxation can cause a repetitive shear stress during knee flexion.47,77,80 All these conditions might result in a chronic mechanical insult of the osteochondral unit and subsequent development of OCD.
Pathogenetic Mechanisms
Many of the selected articles refer to a pathogenetic progression of OCD through either ischemia28,31,35,58 or subchondral fracture.11,14,18,22,26,27,29,48-50,54,60,61,66,68,71,75,78-81 Whether there is interplay of these 2 conditions or how they are interdependent remains unclear. Uozumi et al. 61 following a histologic analysis hypothesized that the pathologic progression depends on the cause of OCD. Thus, resulting subchondral bone changes reflect the pathologic “primum movens.” In the case of ischemic etiology, the initial change in the subchondral area is necrosis followed by subchondral fracture. In support of a primarily vascular cause, Campbell and Ranawat 31 point to the simultaneous occurrence of OCD and Osgood-Schlatter disease in childhood and early adolescence. Thereby suggesting a regional vascular insufficiency based metabolic disturbance of the long bone during rapid growth periods, as a common etiology. 31 If the underlaying cause is a repetitive microtrauma, it is possible to find a subchondral fracture with subsequent bone necrosis due to the lack of the blood supply from the basal side. 61
In any case, regardless of the initiating events, there is agreement on the primary involvement of the subchondral bone in the development of OCD.11,14,16,18,22,26-29,31,34,35,48-50,53-55,58,60,61,66,68,71,75,77-82 In fact, besides an isolated position suggesting that OCD is a cartilaginous disease with the subchondral bone secondarily damaged, 19 all other authors referred to the ischemia or fracture of the subchondral bone as etiological “primum movens” acting primarily on the subchondral bone.
Ischemia
Green and Banks 35 emphasized the role of ischemic subchondral bone back in 1953. Their histological examination confirmed the basic process in OCD is an aseptic necrosis involving the subchondral bone and subsequent changes are secondary. They speculated that in the earlier phases of the pathologic progression the cartilage remains healthy, because of the nutrition received from the synovial fluid. As dead bone is absorbed, the cartilage gradually loses its mechanical and structural support, becoming more susceptible to trauma and exogenous factors. A few years later, Ribbing 34 introduced the hypothesis of ossification nuclei defects, stressing how the bone nucleus partially connected to the cancellous bone represents a locus minoris resistentiae, which enables low-intensity trauma to produce harmful effects on the blood supply of the bone nucleus.
Campbell and Ranawat 31 subsequently classified OCD as idiopathic aseptic necrotic lesions of the growing epiphysis. Their histological examinations showed a large area beneath the detached fragment which had the characteristic findings of a bone infarct. This, together with the intact overlying articular cartilage, confirmed the necrosis of the underlying bone as a primary event for the formation of the loose body.
The idea of subchondral bone ischemia was recently emphasized by Jans et al., 58 who supported the involvement of arterial end branches for the developmental OCD sequence beginning with the separation of the subchondral bone. However, they also advocated repetitive microtrauma as the cause of the compromised blood supply in rapidly growing patients, with interplay of vascular and traumatic factors leading to the onset of OCD.
Fractures
The impingement etiology supports a traumatic mechanism of onset leading to the subchondral bone fracture. Shea et al. 55 even reported a case ascribed to a single macrotrauma, whereas others observed repetitive microtrauma that provoked a subchondral bone stress fracture which leading to OCD in otherwise normal knee joints.49,54,68 The occurrence of OCD at the patella also supports the traumatic origin. The plain patellar surface or the recurrent subluxation of the sesamoid bone during knee flexion causes repetitive microtrauma.71,77,80 Moreover, besides the biomechanical predisposition, the site of the lesion is more suggestive of a traumatic source rather than an ischemic one. In fact, whereas the type of patellar vascularization might entail proximal damage in case of a vascular mechanism, the most common OCD location is in the lower and middle thirds of the articular surface, which are the patellofemoral contact areas subjected to the maximal forces during knee flexion. 77
Constitutional factors may weaken the subchondral bone and favor the fracture mechanism. Among these, osteopenia caused by hyper IgE syndrome 27 or endocrine abnormalities alter metabolism, structure and function of the subchondral bone. 18 Changes in hGH levels may lead to atypical ossification nuclei and decreased ability of the growth plate to absorb energy, and vitamin D deficit 10 has also been indicted as predisposing factor in leaving the subchondral bone susceptible to damage and separation and eventually the development of OCD lesions.
Conclusions
According to this summation of the historic literature, the etiology of OCD can be attributed to either biological or mechanical factors. The former includes genetic causes, deficit of ossification centers and endocrine disorders; the latter, tibial spine impingement, discoid meniscus, and biomechanical alterations, together with injuries and overuse. Interplay of the hypothesized factors that affect the osteochondral unit may support a connection of the different theories in a common etiopathologic framework. These hypotheses, however, are based on generally low levels of evidence. Moreover, these studies are heterogeneous and confound performing a quantitative evaluation of the overall data reported. Despite this, we have presented and organized an account of the historical and current thinking on OCD of the knee in the English literature to better understand and compare the evidence to date. Confirmation and exploration of this framework by further study may allow further clarification of risk factors and mechanisms to be better identified. This in turn may enable customized treatment, and the development of more effective etiology-based therapies for OCD.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.