
Abstract
Purpose
To determine the time to achieving minimal clinically important difference (MCID) and patient acceptable symptomatic state (PASS) for commonly administered patient-reported outcome (PRO) measures and risk factors affecting achievement of clinically significant outcomes in patients undergoing meniscal allograft transplantation (MAT).
Methods
A prospectively maintained MAT registry was retrospectively reviewed from April 2014 to May 2019. Patients who underwent revision MAT or did not complete preoperative PROs or one post operative time point were excluded. Patients who underwent concomitant procedures were included in the analysis. PROs were administered preoperatively and at 6 months, 1 year, and 2 years postoperatively. Previously defined MCID and PASS thresholds were utilized and Kaplan-Meier survival curve analysis with interval censoring was used to calculate the cumulative percentages of MCID and PASS achievement at each follow-up time interval (5-7, 11-13, and 23-25 months).
Results
Eighty patients (age: 28.35 ± 9.76, 50% male) who completed preoperative, 6-month (n = 69, 86% compliance), and 1-year (n = 76, 95% compliance) PROs were included. The majority of patients (>50%) achieved MCID and PASS on most included PROs. Workers’ compensation status was found to significantly delay achievement of MCID and PASS on all PROs except for PASS on Knee Injury and Osteoarthritis Outcome Score (KOOS) quality of life (QoL). Higher body mass index (BMI) significantly delayed time to achieving MCID on KOOS Pain and activities of daily living (ADL), as well as PASS on KOOS Symptoms and KOOS QoL.
Conclusion
This study suggests that the majority of patients have clinically significant improvements in pain and function after MAT, with more than 50% of patients experiencing clinically significant improvement within the first postoperative year. Workers’ compensation status and high BMI may prolong time to achievement of MCID and PASS after MAT.
Introduction
Meniscal deficiency alters knee biomechanics by increasing contact pressure while decreasing contact area, which can contribute to the development of osteoarthritis.1-4 A widely acceptable procedure for treating patients with unicompartmental pain and meniscal deficiency is meniscal allograft transplantation (MAT) with many studies suggesting that this procedure reduces pain, increases function,5-8 and may be able to restore knee biomechanics closer to native levels.9-11 Studies have demonstrated increases in patient-reported clinical outcomes at short-term time points after MAT; benefits of MAT are also observed in long-term—minimum 10 years—evaluation of patients, with patients reporting improved pain with 90% satisfaction.5,7
Patient improvement following a MAT procedure may be monitored using subjective patient-reported outcome (PRO) scores. While postoperative changes in outcome scores may increase, it may not represent a significant change in patient’s perception of their condition. Clinically significant outcomes (CSOs), such as the minimal clinical important difference (MCID) and patient acceptable symptomatic state (PASS), can help define the change in postoperative outcome scores that would correspond with varying levels of patient perception.12,13 MCID attempts to define the smallest postoperative change perceivable by the patient and that could warrant a change in the current treatment.12,13 PASS, in contrast, describes the threshold at which a patient is satisfied with their symptom level. 13
Prior studies have defined CSOs, such as MCID and PASS, for commonly administered PROs after MAT. 14 The purpose of this study was to determine the time to achieving MCID and PASS for commonly administered PROs after MAT and to identify any risk factors affecting achievement of CSOs in patients undergoing MAT. This study hypothesized that increased body mass index (BMI), work-related claims, and higher baseline PROs would increase the time to achieve MCID and PASS. 14 By determining the time to MCID and PASS, physicians and patients can have another tool in following progress and setting expectations of improvement after MAT.
Methods
This study received institutional review board approval at Rush University Medical Center with a corresponding waiver of consent. A prospectively maintained MAT registry was retrospectively reviewed from April 1, 2014, to May 31, 2019. All procedures included in this analysis were performed by the two senior authors (ABY and BJC). All patients who underwent MAT regardless of whether a concomitant procedure was performed, completed preoperative PROs, and were at least 6 months postoperative were initially included in the study. Those who underwent revision MAT or failed within the study period and patients who did not complete preoperative PROs and at least one complete set of postoperative PROs were excluded. An emphasis was placed on patients who completed their 6-month and 1-year PROs instead of 2-year PROs based on prior literature that demonstrated significant improvements in PROs by 1 year and high achievement of CSOs at this time point. 14 Efforts were made to maximize patients at these earlier time points at the expense of those with long-term outcomes.
Data Collection
Chart review was performed to record relevant demographic and intraoperative variables. Specifically, demographic variables included patient’s age, BMI, procedure laterality, and smoking status (current, former, nonsmoker). Intraoperative variables included medial versus lateral compartment MAT, concomitant procedures, and number of focal chondral defects. International Knee Documentation Committee (IKDC) score and Knee Injury and Osteoarthritis Outcome Score (KOOS) were administered preoperatively and at 6 months, 1 year, and 2 years postoperatively. For each PRO, patients were sent the survey electronically 1 month prior to the relevant time point. Each patient had a 2-month window (1 month prior to and 1 month after) to complete the PRO. Thus, in the study, IKDC and KOOS surveys were available to patients to complete at 5-7, 11-13, and 23-25 months. The exact date that the patient completed each PRO within each window was documented. This date was used in the analysis in calculating and assessing time to achievement.
Surgical Technique
MAT was performed as previously described using a bone slot technique. 15 Inferomedial and inferolateral portals were established, and a diagnostic arthroscopy was performed. The cartilage surfaces of the tibiofemoral and patellofemoral compartments were evaluated, as well as the ligamentous and meniscal structures. The presence and location of meniscal pathology were then confirmed. A trephination of the medial collateral ligament (MCL) was performed for medial MATs, and the pathologic meniscus was removed with a basket and shaver followed by more aggressive soft-tissue debridement, with preservation of the meniscal rim. Once the proper footprints were identified, a guide pin followed by a reamer and then a rasp was used to create the slot. The allograft was then prepared on the back table to size using an anterior cruciate ligament (ACL) saw. The size of the graft was assessed to ensure it fits in the appropriate slot. A traction suture was then placed between the posterior horn and the body of the meniscus, the bone bridge was passed through the slot, and the graft was inserted into the joint with the assistance of the traction suture. The graft was fixed posteriorly via an all-inside technique and was fixed along the periphery with the use of 8 to 10 vertical mattress sutures via an inside-out technique, and the anterior meniscus was also sutured through the insertion portal to the capsule via open visualization. Finally, the bone bridge was fixed transosseously with a screw or anchor. Any additional cartilage procedures (n = 55), such as osteochondral allografting and/or realignment osteotomy (n = 15), and/or ACL reconstruction (n = 10), were then performed.
Rehabilitation Protocol
In the immediate postoperative period, the patient’s leg was placed in a hinged knee brace that allows motion from extension to 90° of flexion. During the first 6 weeks postoperatively, heel-based partial weight-bearing was allowed as tolerated. Physical therapy was initiated immediately postoperatively as tolerated. Use of the brace was discontinued and full range of motion and full weight-bearing were allowed beginning at 6 weeks postoperatively. After 12 weeks, the focus of physical therapy shifted with a focus on increasing strength using specific drills. Postoperative rehabilitation lasted as long as 6 to 18 months, depending on procedure complexity and patient goals. Return to sports or significant activity was usually allowed around 9 months postoperatively.
Statistical Analysis
The following MCID and PASS thresholds used in the present study were reported in previously published literature—IKDC: MCID 9.9, PASS 36.0; KOOS Pain: MCD 9.9, PASS N/A; KOOS Symptoms: MCID 9.7, PASS 73.0; KOOS ADL (activities of daily living): MCID 9.5, PASS N/A; KOOS Sport: MCID 13.3, PASS N/A; KOOS QoL (quality of life): MCID 14.6, PASS 53.0. 14 Previously reported PASS values for KOOS Pain, Symptoms, and Sport did not reach an area under the curve (AUC) >0.70 and thus were not included in the analysis. Detailed methodology used to calculate MCID and PASS has been described previously.16-18 Briefly, delta MCID and absolute PASS values were calculated based on PRO scores at baseline and postoperatively. The MCID was derived by calculating one-half of the standard deviation from the delta (difference between postoperative and baseline values) PRO scores. The PASS values were derived using an anchor-based methodology by comparing differences in PRO scores between patients responding “satisfied” and “unsatisfied” to the satisfaction anchor question.
Time to MCID and PASS was calculated as previously described.19,20 Briefly, follow-up was categorized into 3 standardized time intervals based on automated PRO delivery: 6 months (PRO completion between 5 and 7 months), 1 year (PRO completion between 11 and 13 months), and 2 years (PRO completion between 23 and 25 months). The average time required for MCID and PASS achievement was calculated using the exact time within each follow-up period according to the earliest postoperative time interval where each patient reached the respective CSO threshold scores.
The Shapiro-Wilk test was used to assess the parametric assumption of normality for continuous data. Kaplan-Meier survival curve analysis with interval censoring was used to calculate the cumulative percentages of MCID and PASS achievement at each follow-up time interval (5-7, 11-13, and 23-25 months). The influence of demographic and intraoperative factors on earlier or delayed achievement of MCID and PASS was investigated using Weibull parametric survival regression analysis for both IKDC and KOOS subscales. 21 Patient factors included in the regression analyses were age, sex (male vs. female), insurance status (workers’ compensation [WC] vs. other), BMI, the number and location of defect(s), whether a concomitant cartilage procedure or osteotomy procedure was performed, and preoperative PRO score. Statistical significance was defined as P < 0.05. Statistical analysis was performed using RStudio software version 1.2.1335 (R Foundation for Statistical Computing, Vienna, Austria) and STATA v13 (STATACorp, College Town, TX).
Results
Eighty patients (mean age: 28.35 ± 9.76 years, M:F 40:40, mean BMI: 27.17 ± 5.34 kg/m2) were included in the final analysis. A total of 69 patients (86%) completed 6-month PROs and 76 patients (95%) completed 1-year PROs; 46% (n = 37) completed 2-year PROs. Demographics are displayed in Table 1. The cohort included 11 WC patients. The majority of patients had at least one focal chondral defect that was identified intraoperatively and 68% of patients underwent a concomitant cartilage procedure (e.g., autologous chondrocyte implantation, osteochondral allograft transplantation, or microfracture).
Demographics of the Cohort.
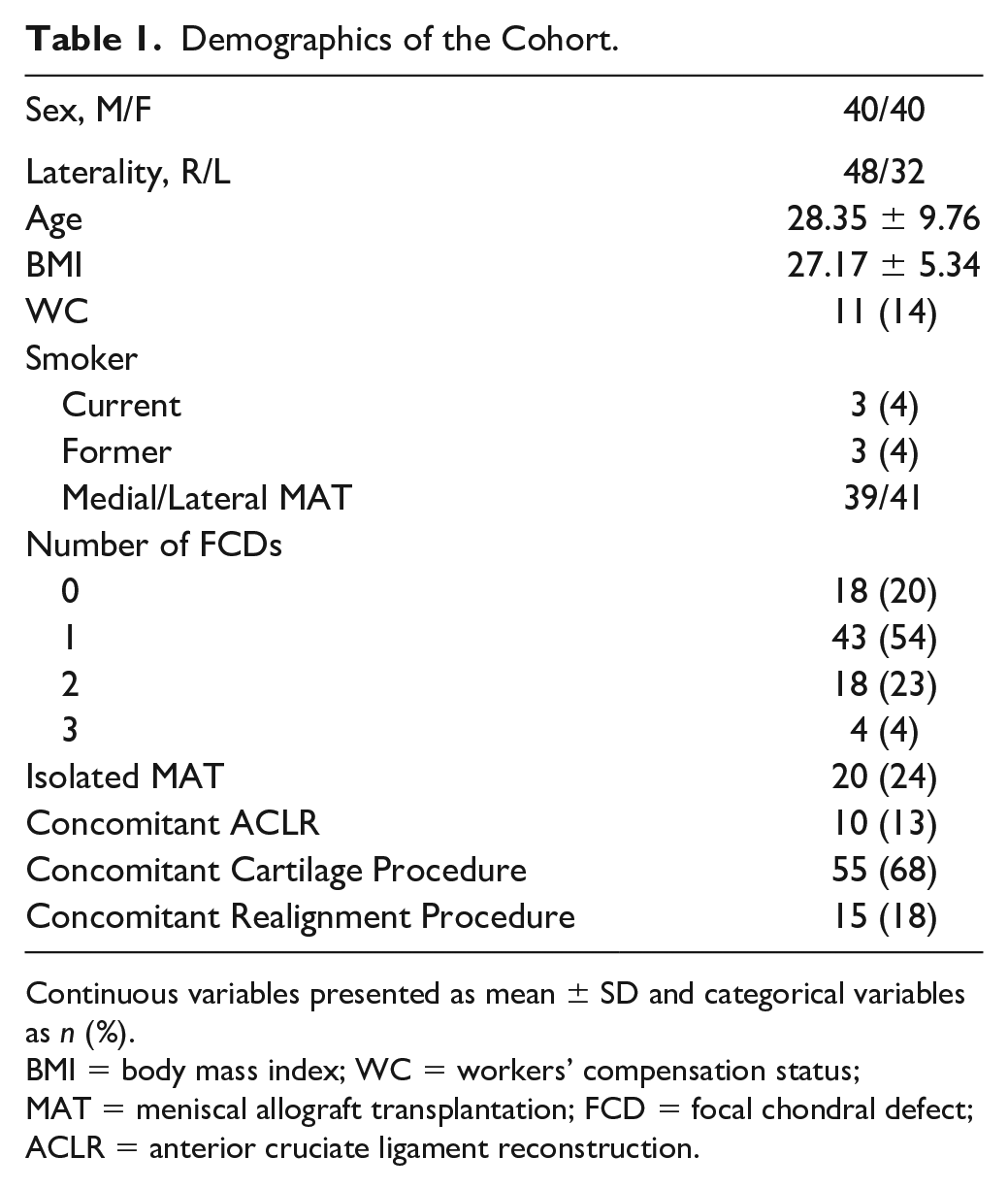
Continuous variables presented as mean ± SD and categorical variables as n (%).
BMI = body mass index; WC = workers’ compensation status; MAT = meniscal allograft transplantation; FCD = focal chondral defect; ACLR = anterior cruciate ligament reconstruction.
Achievement of MCID and PASS is presented in Table 2. The majority of patients (>50%) achieved MCID on IKDC (52.2%), KOOS Pain (60.3%), and KOOS ADL (52.4%) and PASS on IKDC (82.6%) at 6 months. A majority of patients then achieved MCID on IKDC (72.6%), KOOS Pain (63.5%), KOOS Symptoms (62.7%), KOOS ADL (64.9%), KOOS Sport (58.7%), and KOOS QoL (56.8%) and PASS on IKDC (83.8%), KOOS Symptoms (52%) at 1 year.
Achievement of MCID and PASS.
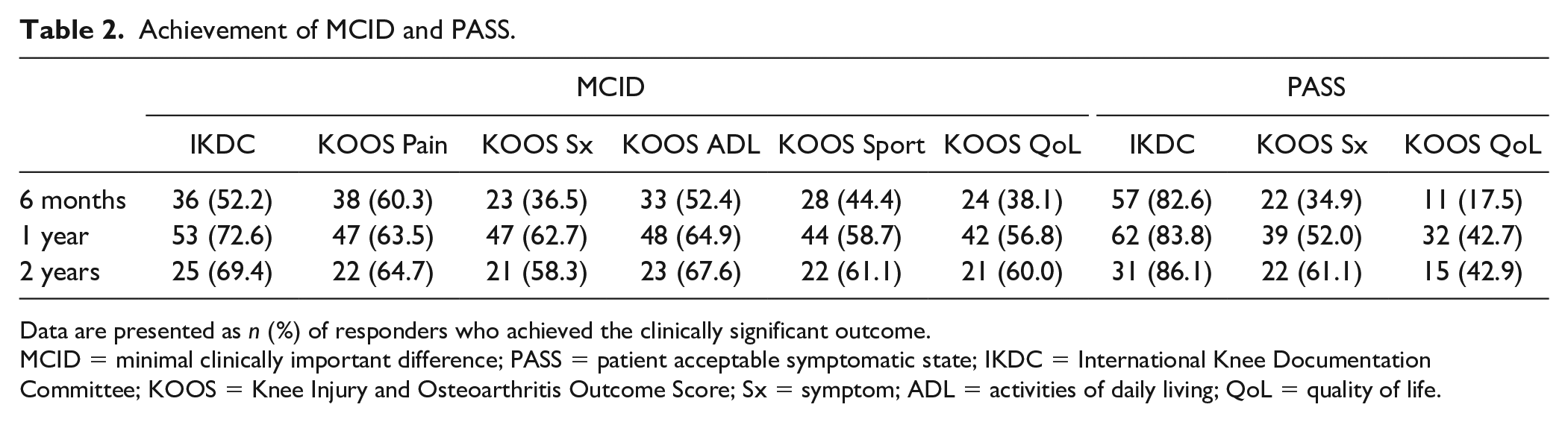
Data are presented as n (%) of responders who achieved the clinically significant outcome.
MCID = minimal clinically important difference; PASS = patient acceptable symptomatic state; IKDC = International Knee Documentation Committee; KOOS = Knee Injury and Osteoarthritis Outcome Score; Sx = symptom; ADL = activities of daily living; QoL = quality of life.
Time to MCID and PASS is presented in Table 3. For IKDC, it took a median of 6.0 months to achieve MCID and 5.6 months to achieve PASS. KOOS symptoms demonstrated a longer time to achievement at 8.0 months to achieve both MCID and PASS. Similarly, KOOS QoL took a median of 7.5 months to achieve MCID and 11.3 to achieve PASS. KOOS Pain, KOOS ADL, and KOOS Sport took a median of 5.8, 6.0, and 6.6 months to achieve MCID, respectively.
Time Required to Achieve Clinically Significant Outcomes After MAT (Months).
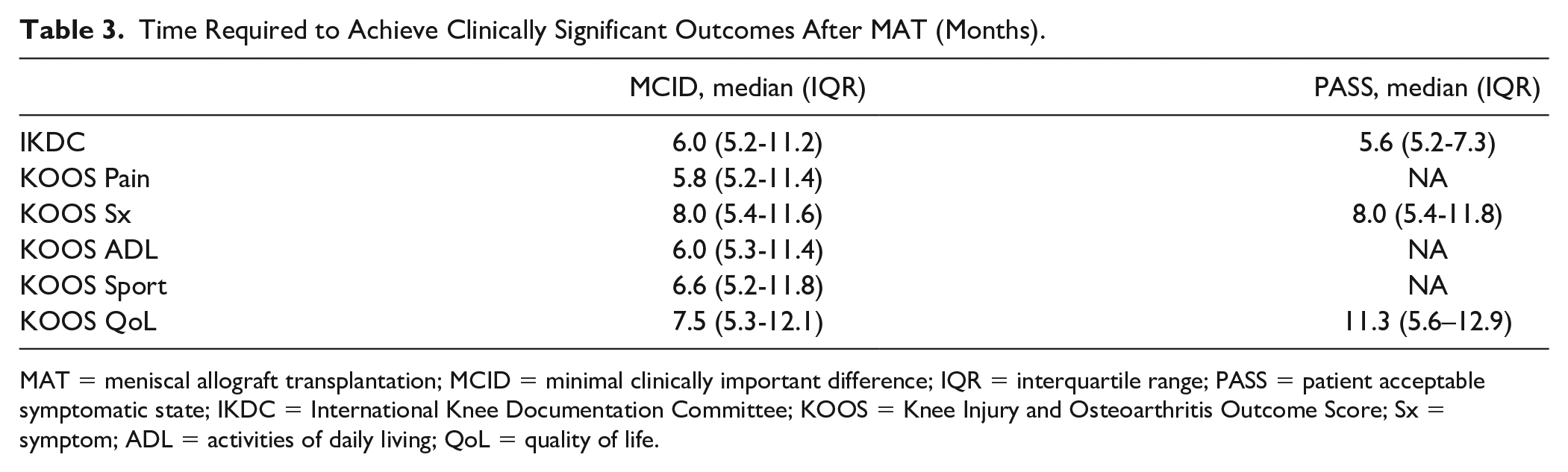
MAT = meniscal allograft transplantation; MCID = minimal clinically important difference; IQR = interquartile range; PASS = patient acceptable symptomatic state; IKDC = International Knee Documentation Committee; KOOS = Knee Injury and Osteoarthritis Outcome Score; Sx = symptom; ADL = activities of daily living; QoL = quality of life.
Multiple demographic and intraoperative factors were evaluated to determine their role on time to achieving MCID and PASS. WC status was found to delay time to achieving MCID for all PROs (hazard ratio [HR] = 0.239-0.305, P = 0.008-0.020] and PASS for KOOS Symptoms (HR = 0.171, P = 0.026) and IKDC (HR = 0.188, P < 0.001) (Table 4). Higher preoperative PRO scores were associated with delaying time to achieving MCID for all PROs (HR = 0.947-0.970, P < 0.001), while higher preoperative PRO scores were associated with shorter time to achieving PASS on KOOS Symptoms and KOOS QoL (HR = 1.030-1.043, P = 0.001) (Table 5). Greater BMI was associated with delayed MCID achievement for KOOS ADL (HR = 0.946, P = 0.020) and KOOS Pain (HR = 0.957, P = 0.010), while the number of focal chondral defects (HR = 0.083-0.255, P = 0.007-0.029) was associated with delayed MCID QoL. Concomitant realignment surgery decreased time to MCID on KOOS Sports (HR = 2.542, P = 0.008).
Factors Affecting Time Required to Achieve Minimally Clinically Important Difference.
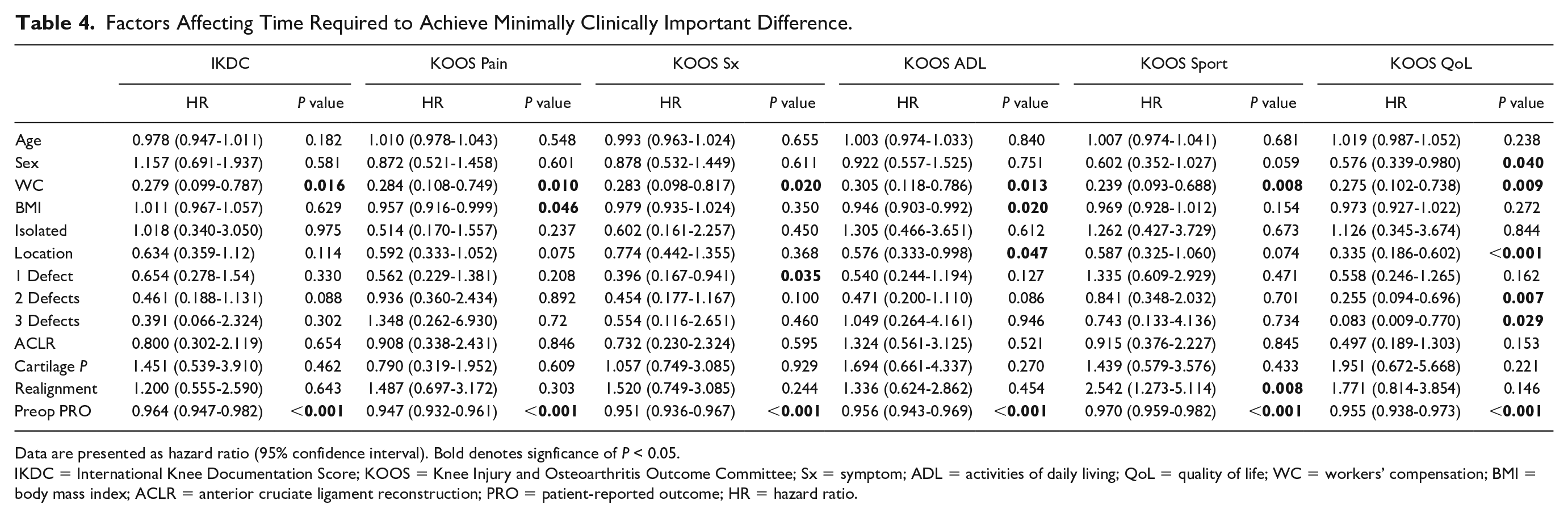
Data are presented as hazard ratio (95% confidence interval). Bold denotes signficance of P < 0.05.
IKDC = International Knee Documentation Score; KOOS = Knee Injury and Osteoarthritis Outcome Committee; Sx = symptom; ADL = activities of daily living; QoL = quality of life; WC = workers’ compensation; BMI = body mass index; ACLR = anterior cruciate ligament reconstruction; PRO = patient-reported outcome; HR = hazard ratio.
Factors Affecting Time Required to Achieve PASS.
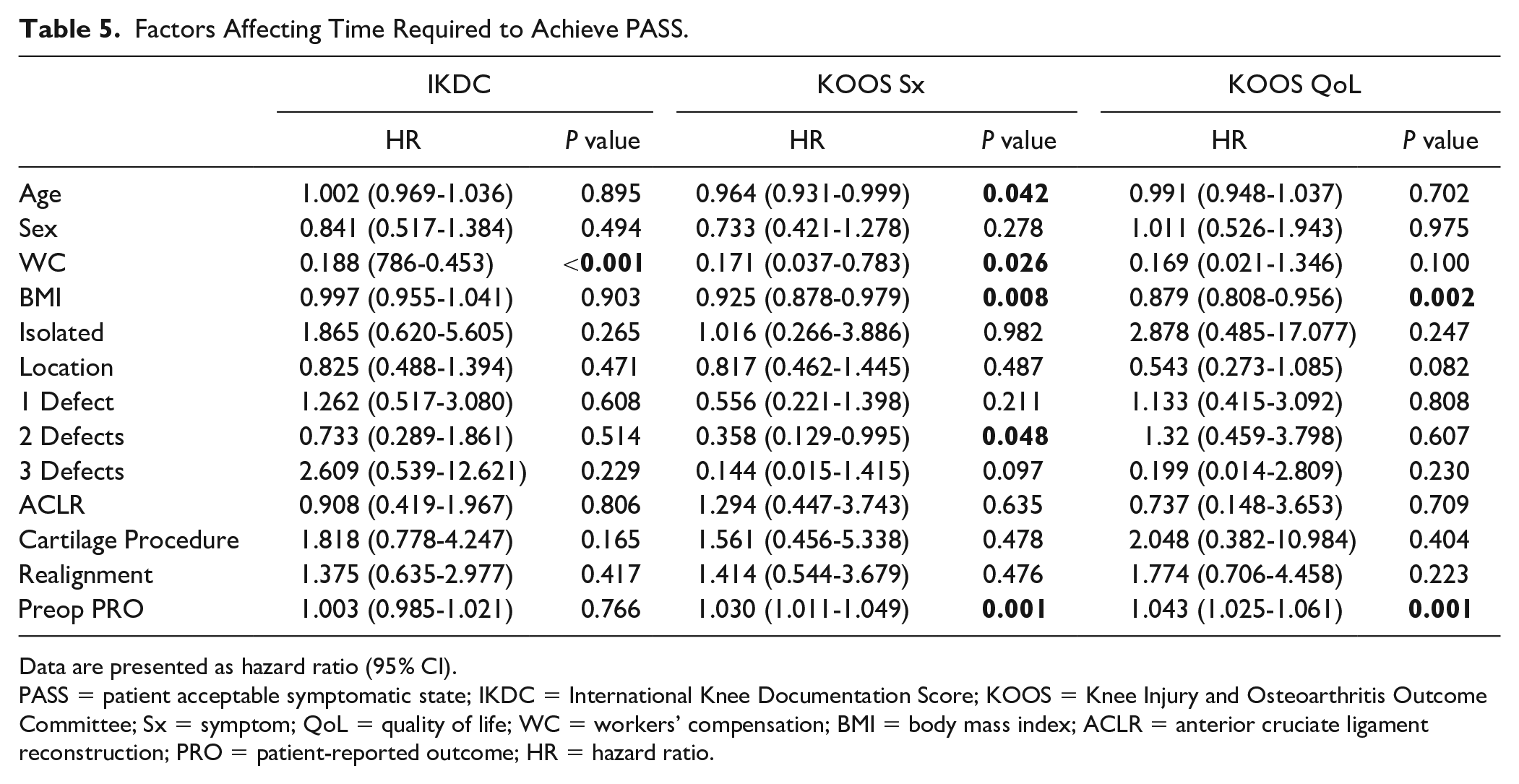
Data are presented as hazard ratio (95% CI).
PASS = patient acceptable symptomatic state; IKDC = International Knee Documentation Score; KOOS = Knee Injury and Osteoarthritis Outcome Committee; Sx = symptom; QoL = quality of life; WC = workers’ compensation; BMI = body mass index; ACLR = anterior cruciate ligament reconstruction; PRO = patient-reported outcome; HR = hazard ratio.
Discussion
The main findings of this study were that MCID on IKDC and KOOS subscores was achieved between 6 and 8 months postoperatively after an MAT with or without concomitant procedures and that the time to MCID may be delayed by patient factors such as WC status and higher BMI. In addition, time to PASS was evaluated for 3 of the PROs: IKDC, KOOS Symptoms, and KOOS QoL. Patients undergoing MAT with or without concomitant procedures can expect to achieve PASS between 5.6 and 11 months postoperatively. Similar to MCID, higher BMI and WC were found to be associated with delayed achievement. This study provides orthopedic surgeons with additional information on when patients can expect to experience noticeable improvement and can guide patient education and postoperative expectations.
In addition, this study’s results show that patients achieve MCID on IKDC, KOOS Pain, and KOOS ADL by about 6 months postoperatively. In contrast, time to MCID is delayed and typically reached between 6.6 and 8 months for KOOS Sport, KOOS QoL, and KOOS Symptoms. Similarly, patients reached PASS on IKDC at 5.6 months, while patients did not achieve PASS on KOOS Symptom and QoL until 8.0 and 11.3 months, respectively. These differences are likely due to the differences in what each PRO is testing. For example, it is not surprising that patients may experience pain relief prior to noticeable improvement in QoL. These findings of achieving MCID and PASS after MAT further support the use of this procedure in patients with symptomatic meniscal deficient knee compartments. The use of MAT is clear when compared with nonoperative treatment. A pilot randomized controlled trial of 36 patients conducted by Smith et al., 22 for example, demonstrated significantly higher PRO scores (KOOS composite, KOOS pain, and KOOS ADL) in the MAT group at 12 months after treatment.
BMI and WC status were found to significantly delay achievement of MCID and PASS for multiple PROs. Prior studies have reported mixed effects of BMI on PROs after MAT. For example, Zaffagnini et al. 23 did not find any significant effect of BMI on PROs, including KOOS, Lysholm, and visual analog scale (VAS), in a cohort of 117 patients at a mean follow-up of 4.0 ± 1.9 years. In contrast, a case-control study by Jimenez-Garrido et al. 24 reported that patients with a BMI >30 kg/m2 had significantly lower IKDC scores, on average about 12 points lower, than nonobese patients. In addition, the obese cohort had significantly higher failure rates, although this outcome measure was not assessed in the present study. Similar to a high BMI, WC status was also associated with longer achievement for both MCID and PASS for multiple measures. This is in line with literature for other sports medicine procedures that have demonstrated that WC status may both decrease the likelihood of CSO achievement and increase the time required to achieve these clinical benchmarks.16,25,26
Interestingly, we did not find that undergoing an isolated MAT decreased time to achieving CSOs and undergoing a MAT with a cartilage procedure did not delay the time to CSO achievement. This is in line with prior studies that have reported no effect on PROs based on the presence of full-thickness chondral defects. Saltzman et al., 27 for example, compared a cohort of patients following MAT without focal chondral defects (FCDs) with those with an FCD and found no significant difference in 2-year PROs nor differences in the number of patients achieving MCID. Other studies have also supported that concomitant FCDs, even those over 3 cm2, do not significantly affect patients’ postoperative PROs, although they may decrease survivorship.28,29 However, we did find mixed effects on time to CSO achievement based on the number of FCDs present. It is not possible, therefore, to derive conclusions directly from these findings because there was no clear trend between the number of lesions and time to achievement.
In addition, we observed that a higher baseline PRO score was associated with a delay in achieving MCID on all tested PROs. While no prior study has specifically reported how baseline PRO scores are related to the time to achieve MCID, Liu et al. 14 also found that a higher PRO score was associated with reduced odds of achieving MCID on IKDC and KOOS Pain, Symptoms, ADL, and QoL. In addition, we found the opposite relationship with PASS: higher preoperative PROs scores were associated with a decreased time to achieve PASS. Liu et al. 14 also reported that preoperative PRO score did not significantly affect achievement of PASS on any PRO. We hypothesize that a higher baseline PRO prevents as much improvement and increases time to MCID because you can reach the ceiling on the PRO. In contrast, PASS is an absolute value on the PRO, not a change in the PRO, and so if a patient has a higher baseline PRO, it may be easier to achieve PASS postoperatively and this could be achieved at an earlier time point. It should be noted, however, that this study did not perform a subanalysis of outcomes of patients who had higher or lower than average PROs. Therefore, limited conclusions can be drawn on the role of baseline PROs on time to achieving CSOs after MAT.
Other factors that had variable effects on achievement included a concomitant realignment procedure and higher age. In this study, we found that the addition of a realignment procedure significantly decreased the time to MCID achievement on KOOS Sport despite the larger procedure and possibly more difficult physical rehabilitation associated with this procedure. This finding may be partially due to the observation that patients with malalignment may achieve higher PROs, as Verdonk et al. described, and because they may have had lower baseline PROs, which we found decreases time to MCID achievement.7,30 Higher age had a limited effect on the time to MCID achievement. This mixed report has also been reported in prior studies. For example, Zaffagnini et al. 23 reported no effect of higher age (>50 vs. <50, range: 16.7-68.8) on any KOOS subscore but did find that higher age was associated with worst Tegner Activity Scale scores at final follow-up.
Limitations
This study should be evaluated with certain limitations. First, this study was performed in a retrospective manner. Chart reviewing was performed to gather patient data, and PROs that were prospectively collected were retrospectively reviewed. It is possible that errors or nondocumentation from chart reviewing could have occurred. Another limitation is that the PROs included in this study were limited to 4 collection time points: preoperatively, and at 6-month, 1-year, and 2-year follow-up. Because of the intervals used, it is possible that patients achieved CSOs prior to the first collection interval at 6 months. This may suggest that earlier time points, such as 3 months, may be considered as a PRO collection time point for MAT patients. However, increasing the number of PRO intervals could significantly increase patient survey burden. In addition, this dataset had a relatively low 2-year compliance rate. Given the literature on the high PRO scores and rates of CSO achievement by 1-year postoperatively after MAT, the focus of this study was to maximize the number of available data points for the preoperative, 6-month, and 1-year data, and this was at the expense of the 2-year data. The presented results corroborate this hypothesis and demonstrate that the majority of patients achieve MCID and PASS before 1 year postoperatively. An additional limitation was that all the variables we included in the analysis did not achieve significance on every single PRO. This may be in part due to the relevancy of the specific patient factor to that PRO and because the PROs are eliciting different aspects of patients’ pain and/or function based on the questions asked. For example, pain improvement may be quick, whereas function takes longer to recover. Despite this limitation, the results presented in this study demonstrate that multiple variables play a role in time to MCID and PASS but that these variables may depend on the PRO.
Conclusion
This study defined the time to achieving MCID and PASS on IKDC and KOOS subscores for patients undergoing MAT with or without concomitant procedures. It suggests that the majority of patients have clinically significant improvements in pain and function after MAT with or without concomitant procedures, with more than 50% of patients experiencing clinically significant improvement within the first postoperative year. Patients may experience clinically significant improvements in pain prior to noticeable improvements in quality of life. WC status and high BMI may prolong time to achievement of MCID and PASS after MAT.
Footnotes
Authors’ Note
Invited Paper/Podium presentation at AOSSM-AANA Combined Annual Meeting 2021.
Author Contributions
Hailey P. Huddleston—Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work, drafting the work or revising it critically for important intellectual content, and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Evan M. Polce—Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work, drafting the work or revising it critically for important intellectual content, and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ron Gilat—Drafting the work or revising it critically for important intellectual content and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Nabil Mehta—Drafting the work or revising it critically for important intellectual content and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Mohamad Alzein—Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work, and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Navya Dandu—Drafting the work or revising it critically for important intellectual content, final approval of the version to be published, and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Kevin C. Parvaresh—Drafting the work or revising it critically for important intellectual content, final approval of the version to be published, and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Brian J Cole—Drafting the work or revising it critically for important intellectual content, final approval of the version to be published, and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Adam B. Yanke—Drafting the work or revising it critically for important intellectual content, final approval of the version to be published, and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study recieved IRB approval at Rush University Medical Center, Chicago, IL.