
Abstract
Knee injuries are common in football, frequently involving damage to the meniscus and articular cartilage. These injuries can cause significant disability, result in loss of playing time, and predispose players to osteoarthritis. Osteochondral allografting is an increasingly popular treatment option for osteoarticular lesions in athletes. Osteochondral allografts provide mature, orthotopic hyaline cartilage on an osseous scaffold that serves as an attachment vehicle, which is rapidly replaced via creeping substitution, leading to reliable graft integration that allows for simplified rehabilitation and accelerated return to sport. The indications for meniscal replacement in football players are currently still evolving. Meniscus allografts offer potential functional, analgesic, and chondroprotective benefits in the meniscectomized knee. In the player at the end of his or her professional/competitive career, meniscal allografts can play a role in averting progression of chondropenia and facilitating knee function and an active lifestyle. This article is intended to present a concise overview of the limited published results for osteochondral and meniscal allografting in the athletic population and to provide a practical treatment algorithm that is of relevance to the clinician as well as the patient/football player, based on current consensus of opinion.
Keywords
Introduction
Participation in competitive football has long been associated with an increased incidence of knee arthritis, with meniscal deficiency generally considered a key risk factor in this process. 1 In contrast, the natural fate of acute articular cartilage lesions, while common, has been mostly implied but not yet elucidated in this patient population. However, the role of cartilage lesion progression in this degenerative process has recently come under renewed scrutiny.2,3 While osteoarticular and meniscal allografting have a well documented history of predictable long-term functional improvement regarding activities of daily living, their respective indications in active athletes are still evolving, and the data on their efficacy in returning these athletes to competitive sports remain sparse. 4 This article is intended to present a concise review of these limited published results and to provide a practical algorithm that is of relevance to the clinician as well as the patient/athlete, based on current consensus of opinion.
Osteochondral Allografting
Conceptually, osteochondral allografting (OCA) has appeal as the cartilage repair technique that most reliably restores orthotopic, mature hyaline cartilage in large articular defects. Allografts are able to address both cartilaginous as well as associated osseous defects with a compound graft in a single-step procedure without inducing donor site morbidity, yielding a robust biomimetic repair construct that allows for accelerated rehabilitation. 5
Their osteoarticular nature give allografts unique application in the treatment of adolescent osteochondritis dissecans (OCD) after physeal arrest ( Fig. 1 ) and as a salvage procedure for knees that have failed prior cartilage repair surgery, which has shown to potentially induce structural changes in the subchondral bone that may negatively affect subsequent cartilage procedures. 6
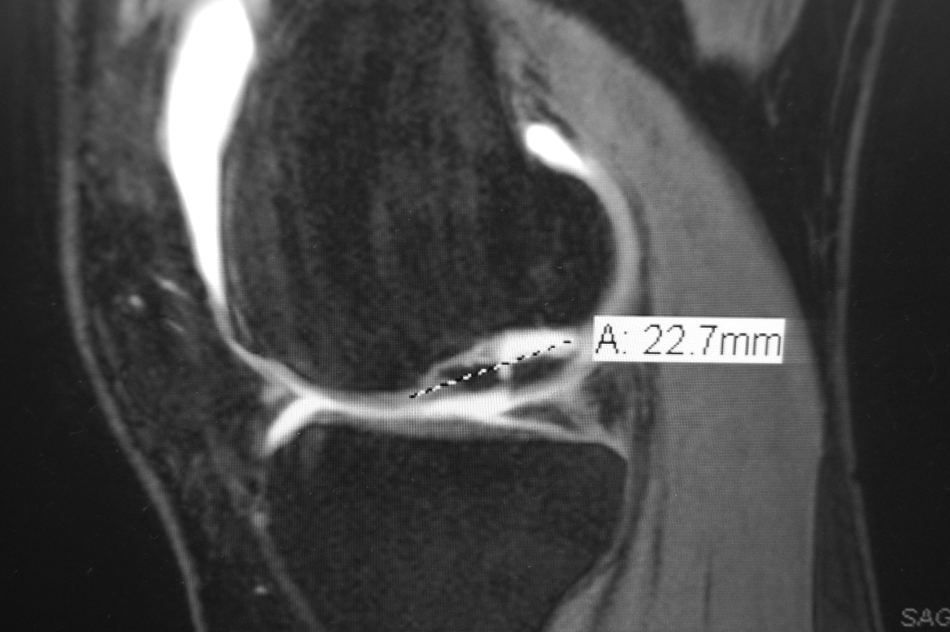
Sagittal T2-weighed magnetic resonance image of the left medial femoral condyle in a 19-year-old female athlete with closed physes, depicting an International Cartilage Repair Society (ICRS) grade III to IV osteochondritis dissecans (OCD) lesion with associated knee effusion. Note the bright fluid signal demarcating the lesion bed and fracture line through the displaced fragment.
The surgical technique for instrumented OCA dowel plugs is particularly reproducible for focal lesions of the femoral condyle. Solid graft fixation in congruency with the articular surface is paramount and can usually be achieved via press fit, which may be supplemented by bioabsorbable fixation devices in situations lacking ideal circumferential containment, such as encountered in marginal OCD lesions ( Figs. 2 and 3 ), or multiple overlapping grafts for oblong lesions. Care should be taken to minimize the amount of transplanted allograft bone to reduce its antigenic load and to optimize the graft’s role as an osteoconductive scaffold by facilitating osseous consolidation via creeping substitution by the host bone. Total graft thickness should be limited to no more than 10 mm, with deeper lesions requiring additional autologous bone grafting, as previously described. 7

Intraoperative view of the same osteochondritis dissecans (OCD) lesion in its typical location on the lateral border of the weightbearing portion of the medial femoral condyle. Note the unstable cartilaginous rim and partially empty OCD bed due to fragmentation, with attempted fibrous healing of the defect.
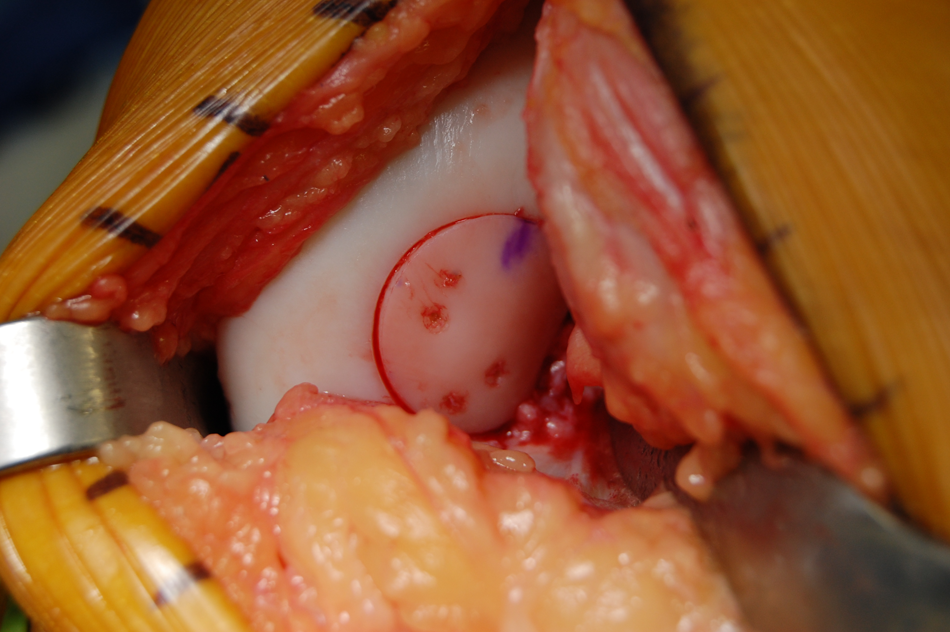
Intraoperative view of the same osteochondritis dissecans (OCD) lesion after resurfacing with a fresh osteochondral allograft dowel, showing a surgical ink mark for proper graft orientation. Note the congruous fit and the auxiliary fixation with bioabsorbable fixation devices due to the lack of containment owing to the proximity of the OCD lesion to the intercondylar notch.
Using this technique in a study treating 25 young (mean age, 31.3 years), athletically active patients with stand-alone dowel grafts for focal lesions (size, 435 ± 166 mm2; equivalent to a dowel size between 20 and 25 mm in diameter), Robertson et al. demonstrated that 21 of 25 (84%) returned to at least some level of athletic activity (including football) at a mean follow-up of 4.5 years. While 60% of athletes returned to high-level sports participation comparable to their preinjury activity level, 28% of patients in this study avoided pivoting sports postoperatively. 8 To our knowledge, this currently is the only published data expressly on return to sport after osteochondral allografting. In a study on fresh osteochondral allografting of the femoral condyles, McCulloch and colleagues reported that Knee injury and Osteoarthritis Outcome Score (KOOS) sport and recreation function subscale scores significantly improved from 18 preoperatively to 46 postoperatively in their overall cohort. Active patients not pursuing worker’s compensation fared better, improving from a mean of 19 to 58 in the KOOS sports and recreation function. Of note, 10 of the 25 patients in this study underwent concomitant meniscal transplantation. Although their subjective outcome scores were not significantly different, their KOOS sports and recreation function was markedly lower at final follow-up, improving from 20 to 39 postoperatively. Four patients who underwent concomitant high tibial osteotomy achieved an improvement from 15 to 54 on the same scale. Overall, patients gauged that their knee was functioning at 79% of the level of their unaffected knee at a mean follow-up of 3 years. 9
These studies emphasize the importance of appropriate surgical indications and proper patient selection. Likewise, symptom chronicity, as well as resultant muscular conditioning and activity level, are important determinants of postoperative recovery. These factors all play into seasonal considerations in planning osteochondral allograft reconstruction, subsequent rehabilitation, and return to football activity. Traditionally, postoperative recommendations included protected weightbearing for a period of 3 months after small fragment allografting. However, in recognition of the inherent stability of contained press fit dowel grafts, the current trend is towards increasingly shorter postoperative intervals of partial weightbearing, owing to the immediate mechanical properties conveyed by the compound osteoarticular nature of the grafts. Likewise, range of motion is not usually restricted, and braces are not routinely employed after osteochondral allografting unless involving the patellofemoral joint, where deep flexion might otherwise induce shear stresses that could jeopardize graft integrity. For the clinician, it might be helpful to consider the postoperative period analogous to fracture care in that dynamization of the graft and advancing the weightbearing status have to take into account the intraoperative stability of the graft-host interface and radiographic evidence of graft incorporation that is readily assessable on plain radiographs.
In competitive athletes, the clinician has to balance the demands of functional rehabilitation with the risk of early graft collapse and failure. In this context, it is good to remember that allografting is also a denervating surgery. While this effect is desirable for pain relief, it also means that pain or the absence thereof is not a very sensitive indicator of the graft milieu in the immediate postoperative period, not unlike allograft cruciate ligament reconstruction. Shirzad et al. assessed the results of an immediate weightbearing protocol following fresh OCA of the femoral condyle with single or multiple dowel plugs in 32 consecutive patients. 10 Average age in their cohort was 35 years, average lesion size was 4.8 cm2, and OCD was the preeminent diagnosis, carried by 19 of 25 patients. Grafts that included indirect weightbearing regions of the femur were larger (10.3 cm2 v. 4.2 cm2), requiring multiple grafts. At 6-month follow-up, significant clinical improvement was observed in all subscales of the KOOS, International Knee Documentation Committee (IKDC), and SF-36 score compared to baseline. Degree of osseous incorporation was assessed using the modified Cahill/Berg classification on computer tomography scans, which indicated that grafts implanted to direct weightbearing regions had >75% incorporation (21 of 27 grafts) compared to <50% incorporation in the indirect weightbearing regions (9 of 16 grafts). Greater improvement was seen with the 19 single dowel grafts, compared to 13 multiple grafts. Incorporation of <50% was associated with fragmentation. They concluded that fresh OCA with full postoperative weightbearing as tolerated shows osseous incorporation and improved short-term clinical outcomes. The immediate weightbearing protocol led to stable incorporation in single dowel plug OCA but was associated with increased risk of graft fragmentation in the cohort treated with multiple contiguous grafts.
While some dynamization of the graft may aid in osseous healing, patients need to be cautioned and reminded to stay within their functional envelope dictated by dynamic rehabilitation parameters such as range of motion and quadriceps function, as above. Currently, in our practice, patients are empirically kept toe-touch weightbearing for a period of 2 to 4 weeks, depending on their extensor mechanism function (especially quadriceps strength) and range of motion. Graft displacement and early collapse or fragmentation have not been relevant clinical issues using these precautions. Running with subsequent return to football activities is usually allowed around the 4-month time point, once the functional envelope of the lower extremity is successfully restored and normal running gait with the ability to maintain dynamic axial alignment is observed. Return to competitive football can reasonably be expected by 6 months after osteochondral allograft dowel transplantation for focal cartilage lesions of the knee.
Meniscal Allograft Transplantation
Meniscal injuries, and subsequent meniscectomies, are common in football, with implications for long-term knee function and health-related quality of life. 11 Although awareness of arthritis progression has fueled an increased trend in meniscus preservation and repair, most competitive players opt for in-season meniscectomy in favor of a faster return to play. Treatment options for the symptomatic, meniscus-deficient athletic patient are limited, although certain acellular meniscal scaffolds have shown promise in regenerating meniscal volume. While a growing body of evidence encompassing over 1,000 cases suggests that meniscus allotransplantation (MAT) is effective at relieving pain in the meniscectomized knee during activities of daily living as presented by Elattar et al., data on return to sports after meniscal transplantation are sparse and controversial. 12 The average Tegner score in the 44 studies included in this meta-analysis improved from 3 to 5, which is far short of scores compatible with competitive football (Tegner score: 9). Noyes et al. reported that 25 of 38 patients (65.8%) were able to improve on their preoperative activity level after MAT. 13 However, only 5 patients (13.2%) were able to return to activities commensurate with playing football (including running, cutting, and twisting), while 8 patients (22.8%) in their cohort were not able to participate in sports at all.
Nonetheless, techniques and indications for MAT in athletic patients continue to evolve. In a more recent study on the results of arthroscopic MAT in postmeniscectomy football players, 12 of 14 (85.7%) competitive football players (mean age, 28.1 years) in the Spanish lower divisions returned to play after an average of 7.6 months. 14 All patients reported decreased visual analog scale (VAS) pain and improved subjective IKDC scores at a mean follow-up of 36 months, while functional improvements as measured in Lysholm scores were less pronounced and not unequivocal. Outcomes did not seem to be significantly related to the presence of chondral lesions at the time of surgery, although patients with a history of surgery of the ipsilateral knee besides the index meniscectomy were excluded from the study. Despite limited follow-up and sample size, this study is unique in presenting outcomes of meniscal transplantation in a pertinent football player population, showing that indications may be expanded in carefully selected and motivated patients. The postoperative immobilization period of 4 weeks in this study falls in line with the literature commonly describing prolonged nonweightbearing intervals after MAT (not unlike after acute repair of salvageable meniscal tears), which reflects the limited application for midcareer meniscal transplantation in the professional/high-level soccer player. Also, meniscal transplants are at a substantial risk for retear, which represents the most commonly encountered complication after MAT. 15 While most of these injuries can be routinely treated with meniscectomy rather than removal of the implant, this information should be an integral part of the informed consent process.
In active players with a prior subtotal meniscectomy still functioning at a high level, MAT would not be an appropriate elective procedure as not to interfere with their maintained high level of play. However, MAT may be indicated in players with severe, intractable postmeniscectomy pain that is career threatening, after other contributing pathology has been ruled out. This includes ligamentous instability, especially subtle cruciate laxity and meniscofemoral ligament injury, which can be symptomatic in the football player when stressed during use of the instep in kicking. 16 Likewise, due to the synergistic nature of the medial meniscus and anterior cruciate ligament in resisting anteroposterior tibiofemoral translation, medial meniscal deficiency should be sought in the case of a player with recurrent anterior cruciate ligament failures in the absence of identifiable technical causes.17,18 Concurrent MAT with revision anterior cruciate ligament reconstruction to reconstruct the posterior meniscal bumper is a rare but potentially valuable indication for MAT in the football player.
An emerging and potentially more controversial indication is the prophylactic meniscal replacement in the yet asymptomatic knee of adolescent athletes with a functionally complete loss of their meniscus, including cases of discoid menisci. The chondroprotective effect of MAT is speculative at this point. Animal data overall are not unequivocal, although most available histological results suggest that immediate MAT conveys superior chondroprotection compared to delayed transplantation. 19 Verdonk et al. retrospectively analyzed 42 meniscal transplants with a minimum follow-up of 10 years. Medial MAT with concomitant high tibial osteotomy showed greater functional improvement than MAT alone. Radiographic analysis was available for 32 knees and revealed no progression of joint space narrowing in 13 of 32 knees (41%), while Fairbank changes remained stable in 9 of 32 knees (28%). Magnetic resonance imaging (MRI) analysis at 1 and 10 years postoperatively showed no progression of cartilage degeneration in 6 of 17 knees (35%). Although the KOOS scores obtained at final follow-up indicated the presence of substantial disability and symptoms, as well as a reduced quality of life, the lack of radiographic disease progression suggests a potential chondroprotective effect. 20 Given the natural history of the meniscectomized knee, early meniscal replacement may be pursued, especially in the more meniscus-dependent lateral compartment. 21 Current MRI-based techniques and protocols, including quantitative T2-mapping, dGEMRIC, T1ρ, and sodium MRI, provide a quantitative measure of the fixed charge distribution in articular cartilage, allowing an assessment of cartilage metabolism that may aid in identifying patients at risk for accelerated degeneration whose joints may benefit from early intervention. 22
We prefer the bone-bridge slot technique ( Fig. 4 ), which relies on a mini-open approach with inside-out suture fixation, as it maintains the anatomic meniscal horn relationship and biomechanical hoop properties of the meniscus. Retaining a minimal donor meniscal rim and reconstituting the posterior bumper of the meniscus appear instrumental in the success of the technique. In resecting the recipient trough, care should be taken to respect the footprint of the anterior cruciate ligament, to minimize sacrificing the weightbearing tibial articular cartilage, and to avoid notch impingement due to a proud graft construct. An anteriorly placed suture anchor can act as an interference screw to supplement the bony fixation while also aiding in capsular closure.

Intraoperative view of a left lateral meniscus allograft that has been prepared for implantation using the bridge-in-slot technique. Note the dissection of the attached soft tissues and the minimal width of the bone bridge, encompassing only the width required to capture the meniscal horn attachments.
The rehabilitative protocol is not unlike that employed after repair of a large bucket-handle tear. Patients are kept partially weightbearing for 2 weeks and progress to half and then full weightbearing by 4 and 6 weeks postoperatively, respectively. Range of motion (ROM) is restricted by use of a ROM brace from 0° to 90° for the first 2 weeks, with flexion goals of 120° by 4 weeks and full ROM by 6 weeks. Early isometric and stretching exercises are encouraged, with progression to closed-chain exercises after 6 weeks. Impact loading and twisting movements should be avoided for at least 3 months. Open-chain rehabilitative exercises have a sport-specific utility in the football player and can be instituted at this time, with a gradual progression to full activities at around 6 months, assuming adequate muscular control, endurance, and balance.
Although axial alignment and ligamentous stability are recognized as being instrumental to the success of both osteochondral 23 and meniscal 24 allografting, little information is available on how concomitant procedures affect the ability to return to sports. 25 Bonnin et al. reported that 66% of young, motivated patients were able to return to strenuous sports after high tibial osteotomy. 26 In a study by Mithöfer and colleagues, 5 of 9 football players (56%) undergoing concurrent osteotomies and cartilage repair procedures returned to their sport. 27 However, in a larger study investigating general sporting activity after osteotomy, football participation decreased from 47% during the lifetime to 9.2% in the year prior to surgery, to only 4.6% postoperatively. 28 No patients in this cohort returned to competitive sports of any kind, which might also be reflective of the mean age of the time of surgery (41.2 years), although patients as young as 19 years were enrolled in the study. We do not routinely advise osteotomies in patients with mild malalignment and otherwise straightforward primary osteochondral lesions that predictably return to a high level of function. However, we are more aggressive in optimizing alignment in salvage situations and meniscal transplants. Here, concomitant surgeries can reduce rehabilitation time and avoid prolonged absence from football activities, without increasing perioperative morbidity. 29
Conclusion
In our experience, results of osteochondral allografting in the athlete mirror those in the overall population in that allografting leads to predictable pain relief and generally returns patients to their preinjury level of function. We consider large focal defects of the distal femur, as encountered in osteochondritis dissecans, as ideal indications for fresh osteochondral allografting. Meniscal allograft transplantation can be a reasonable salvage option for the painful meniscus-deficient knee in carefully selected patients, with its application in competitive athletes currently still evolving.
Footnotes
The authors declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The authors received no financial support for the research and/or authorship of this article.