
Abstract
Purpose
Evaluate the ability of patients to return to work (RTW) following arthroscopic meniscal allograft transplantation (MAT) for meniscal deficiency.
Methods
Consecutive patients undergoing MAT were retrospectively reviewed at a minimum of 2 years postoperatively. Patients completed a subjective work questionnaire, Visual Analogue Scale for pain, Single Assessment Numerical Evaluation, and satisfaction.
Results
Forty-seven patients who were employed within 3 years prior to surgery (average age: 30.2 ± 6.9 years) were contacted at an average of 3.5 ± 0.9 years postoperatively. Forty-six patients (97.8%) returned to work by 2.7 ± 2.6 months postoperatively, and 44 patients (93.6%) returned to the same level of occupational intensity. Patients who held sedentary, light, medium, or high intensity occupations were able to RTW at a rate of 100.0%, 100.0%, 88.9%, and 85.7% (P = 0.4) by 1.1 ± 1.0 months, 2.5 ± 2.5 months, 3.5 ± 3.2 months, and 4.3 ± 2.8 months (P = 0.3) postoperatively. Thirty-eight patients (80.9%) were at least somewhat satisfied, and 43 patients (91.5%) would still have the operation if presented the opportunity. No patient underwent revision MAT or conversion to arthroplasty.
Conclusion
In patients with painful meniscal deficiency, MAT provides a high rate of RTW (97.8%) by 2.7 ± 2.6 months postoperatively. However, some patients may be unable to return to their previous level of occupational intensity. Although statistically insignificant, patients with higher intensity occupations may have a lower rate and longer duration until RTW than those with less physically demanding occupations. Information regarding RTW is imperative for appropriately managing postoperative expectations.
Introduction
In patients who have undergone subtotal or total meniscectomy, knee biomechanics are altered, which leads to and accelerates the progression of tibiofemoral osteoarthritis.1,2 Although total knee arthroplasty can produce reliable outcomes when treating end-stage osteoarthritis, concern for implant failure and activity restrictions has led to an increased consideration of biologic treatments in younger patients with symptomatic joint disease.3-5 In patients with persistent pain and meniscal deficiency, meniscal allograft transplantation (MAT) may be indicated to reduce symptomatology and reconstitute the native force distribution across the tibiofemoral joint. 6 Although relatively uncommon in comparison to other meniscal procedures, 7 the incidence of MAT is increasing, especially in patients younger than 25 years of age.8,9
MAT yields statistically significant improvements in patient-reported outcome measures as well as a low rate of revisions or conversion to total knee arthroplasty.9-16 Even with concomitant cartilage restoration procedures, patients exhibit significant improvements in functional outcome metrics.14,17 Furthermore, 67% to 85.7% of patients are able to return to sport following MAT. 18 However, Zaffagnini et al. demonstrated that although 74% of patients are able to return to sport by 9 months postoperatively, only 49% of patients were able to return to their preinjury level of play.19,20 Despite favorable outcomes following MAT, return to work (RTW) may represent an important outcome metric in young, active patients who comprise the majority of the workforce. However, the rates of RTW are not well described in patients undergoing MAT.
The purpose of this investigation is to assess the timeline of RTW following MAT. We hypothesize that patients in higher-intensity occupations will demonstrate a lower rate of return to their previous level of work intensity and a longer duration of absence from work in comparison to patients in lower intensity occupations.
Methods
Institutional review board approval was obtained prior to initiating this investigation. This was a retrospective analysis of patients who underwent meniscal allograft transplant from 2013 to 2015 by the senior author. Patients included in this investigation were also included in previous investigations.12,14,21,22 Indications for arthroscopic MAT include age less than 50 years with painful medial or lateral meniscal deficiency as shown on magnetic resonance imaging or previous knee arthroscopy. Inclusion criteria for this study were patients who received an isolated MAT in a knee with normal alignment that did not necessitate an osteotomy and were available for minimum 2-year follow-up. Patients who previously underwent meniscectomy, debridement, cartilage procedure (microfracture, osteochondral allograft transplantation [OCA], or autologous chondrocyte implantation) were also included in the analysis. Patients were excluded if they were 18 years or younger at the time of surgery or underwent concomitant high tibial osteotomy, distal femoral osteotomy, tibial tubercle osteotomy, or anterior cruciate ligament reconstruction. Those undergoing revision MAT were also excluded from this analysis. Patients either had preserved articular cartilage or focal chondral deficiency that was amenable to repair or restoration. Indications for cartilage restoration were based upon size of the lesion and Outerbridge grade. 14 Femoral defects greater than 5 mm, greater than Outerbridge grade III, or involvement of the subchondral bone were treated with an osteochondral allograft. Autologous chondrocyte implantation was performed on lesions greater than 2 cm2 without subchondral bone involvement—typically in the patellofemoral joint. Microfracture was performed on smaller lesions (<1 cm2) on the femur and most Outerbridge grade III or higher tibial lesions. Osteochondral allograft lesions were performed on lesions less than 10 mm in diameter.
Patients with a functional telephone number or e-mail address were contacted to complete a detailed survey regarding patient satisfaction and work outcomes. As part of the survey, patients completed a Single Assessment Numerical Evaluation (SANE), Marx Activity Scale, and Visual Analog Scale for pain (VAS-Pain). Patients who did not complete the questionnaire did not respond to multiple phone calls, e-mails, or standard mail and were not included in this investigation. This work questionnaire has been previously used to describe outcomes following orthopedic procedures.23-32 Occupational intensity was divided into high, medium, low, or sedentary occupations ( Table 1 ).23-32 Preoperative diagnosis, demographic information, complications, and surgical history were obtained from patient records. Preoperative radiographs were assessed by 2 reviewers (DRC, AA) for the degree of osteoarthritis using the Kellgren-Lawrence (K-L) grading system.
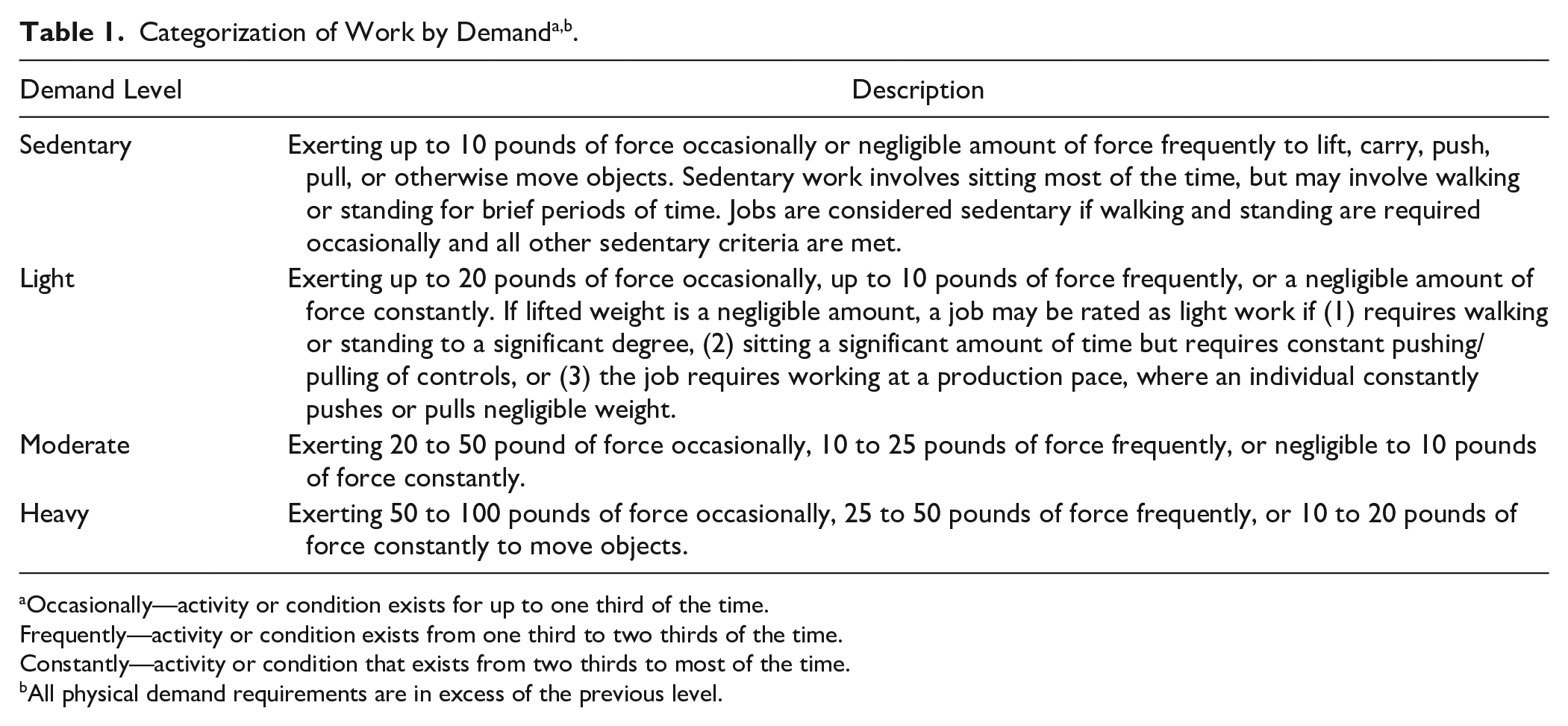
Occasionally—activity or condition exists for up to one third of the time.
Frequently—activity or condition exists from one third to two thirds of the time.
Constantly—activity or condition that exists from two thirds to most of the time.
All physical demand requirements are in excess of the previous level.
Surgical Techniques
Meniscal Allograft Transplant
The technique for arthroscopic MAT with a bone slot technique has previously been described and was implemented in every patient in this series.14,21,33 Diagnostic arthroscopy was initially performed using standard anteromedial and anterolateral portals. The meniscus was assessed, and all remaining meniscal tissue was removed leaving a peripheral rim of 1 to 2 mm. The integrity of the cartilage in the medial and lateral compartments was also assessed and any chondral defects was treated with osteochondral allograft transplantation, microfracture, or autologous chondrocyte implantation. A 2-cm longitudinal transpatellar incision was made and a 4-mm arthroscopic burr was used to create a reference slot between the meniscal horn footprints along the tibial plateau. A guide wire was advanced through the reference slot toward the posterior cortex. An 8-mm cannulated reamer was placed over the guide wire to create a slot in the tibial plateau. A 1-cm deep × 8-cm wide slot was created using an 8-mm × 10-mm box cutter.
The meniscal allograft, while attached to the bone block, was prepared on the back table. A sagittal saw was used to prepare the allograft to a 7-mm wide and 10-mm deep bone block. The meniscal allograft transplant was introduced into the medial or lateral compartment via an accessory posteromedial or posterolateral incision and the bridge was inserted into the slot. Once the graft is fully seated, the bridge is secured anteriorly with a 5.75 mm SwiveLock anchor (Arthrex Inc., Naples, FL). The meniscal allograft is also secured to the remnant meniscus and capsule with vertical mattress sutures in an inside-out technique.
Rehabilitation Protocol
Following MAT, patients are partial-weight bearing/heel/toe-touch only for the first 6 weeks postoperatively and were allowed to progress to full weight bearing after this time. For the first 2 weeks postoperatively, patients were advised to use a brace locked in extension at all times. After which, patients were allowed to remove the brace at night until 6 weeks postoperatively, and then the brace was fully discontinued. Patients advanced range of motion as tolerated without weight bearing. It was recommended that patients maintain full extension during the first 2 weeks by sleeping with the brace locked in full extension.
Statistical Analysis
Statistical analysis was conducted using Microsoft Excel (Microsoft, Seattle, WA). Descriptive analysis of continuous variables included means and standard deviations, whereas frequencies and percentages were used to report discrete variables. A subgroup analysis of isolated MAT and MAT with concomitant OCA/microfracture. Chi-square analysis was used to compare the rate of RTW, while Student’s t test and ANOVA analyses were used to compare the duration of RTW among occupational intensities. Statistical significance was set at P < 0.05.
Results
Forty-seven patients who met inclusion criteria were included in the final analysis. A total of 117 patients underwent arthroscopic MAT by the senior author from 2013 to 2015. Thirty patients were lost to follow-up, leaving 87 patients (74.4%) eligible for inclusion in this investigation. Patients undergoing concomitant ACL reconstruction (n = 9), high tibial osteotomy (n = 4), distal femoral osteotomy (n = 4), tibial tubercle osteotomy (n = 1), or revision MAT (n = 3) were excluded from this analysis. Of the remaining 67 patients, 47 (70.1%) were employed within 3 years of surgery and were included in the final analysis. Demographics of the included patients are provided in Table 2 . Thirty-four patients (72.3%) underwent at least one concomitant cartilage procedure, including osteochondral allograft transplantation (n = 31; 66.0%) and microfracture (n = 3; 6.4%). There were 29 patients (61.7%) who had a MAT and OCA/microfracture in the same compartment. Eleven patients (23.4%) received a second concomitant cartilage procedure with the most common combination being OCA to the lateral femoral condyle with microfracture on the tibial plateau (n = 8; 17.0%).
Patient Demographics.
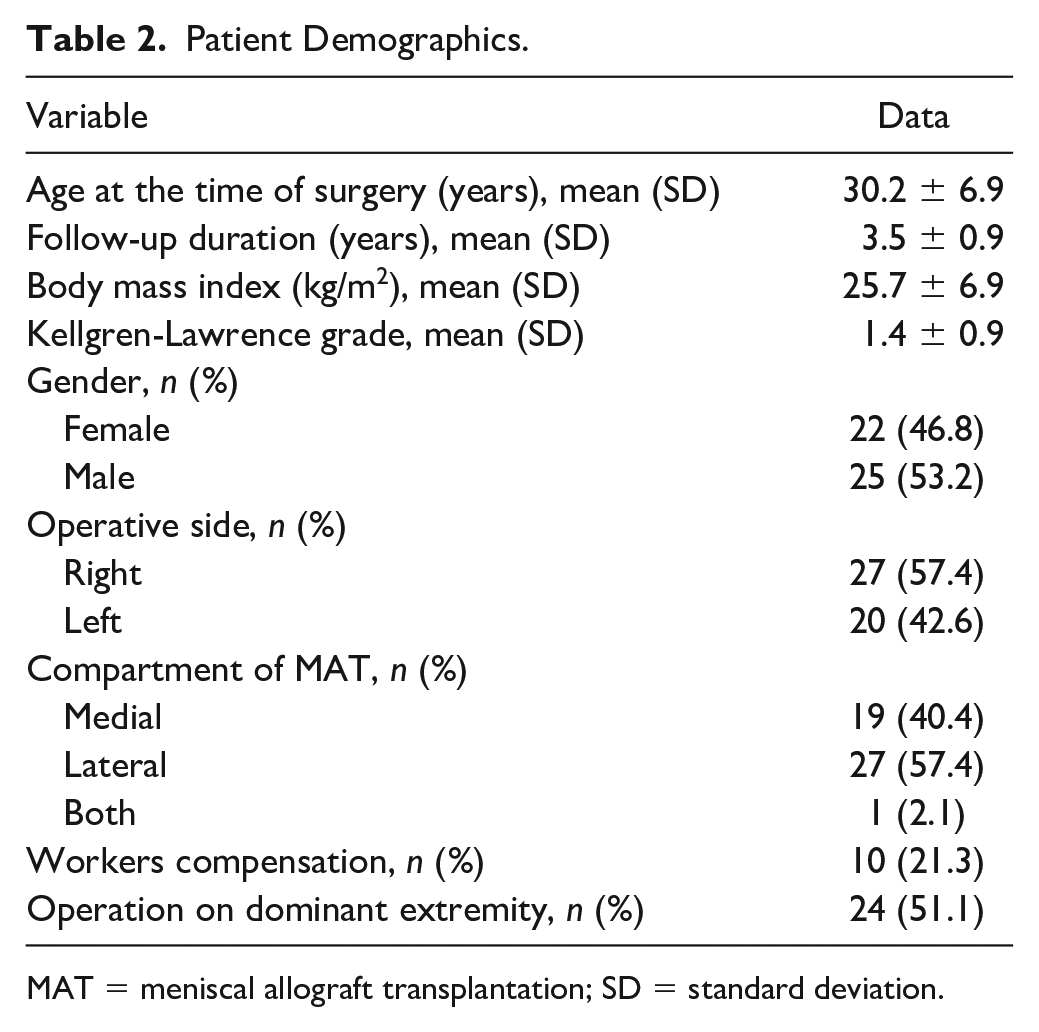
MAT = meniscal allograft transplantation; SD = standard deviation.
The most frequently reported indications to pursue a MAT were pain relief (91.5%), to continue to play sports (60.0%), prevent arthritis (42.6%), and a desire to RTW (21.3%). Every patient underwent at least one prior surgery on the ipsilateral leg prior to their MAT, with the average number of procedures being 3.02 ± 1.8. Forty-two patients (89.4%) previously underwent a meniscectomy/meniscal repair, 4 patients (8.5%) underwent a microfracture, and 15 patients (31.9%) previously received an ACL reconstruction.
Postoperative Complaints and Complications
The average postoperative VAS-Pain was 2.9 ± 2.3, while the average postoperative SANE score was 66.2 ± 25.2. Thirty-eight patients (80.9%) were at least somewhat satisfied with their surgery, and 43 patients (91.5%) would still have had the operation again if presented the opportunity to alter their decision.
Forty-three patients (91.5%) reported complaints with their knee at some point postoperatively. The most common complaints were stiffness (44.7%), symptoms of catching and locking (36.2%), chronic pain (34.0%), frequent swelling (31.9%), occasional pain (25.5%), and instability (21.3%). Thirteen patients (27.7%) returned to the operating room at least once following the index MAT, with 11 patients (23.4%) undergoing additional arthroscopy, a single patient (2.1%) received a hardware removal, and a single patient (2.1%) had a realignment osteotomy that was not planned as a staged procedure. No patients underwent a revision MAT.
Work Outcomes
Forty-six patients (97.9%) who were employed prior to surgery returned to work at an average time of 2.7 ± 2.6 months following MAT, and 43 patients (93.6%) were able to return to the same level of occupational intensity. Ten patients (21.3%) were covered by workers’ compensation at the time of surgery, of which, 9 patients (90.0%) were able to RTW by 4.4 ± 3.7 months postoperatively.
Patients who held sedentary, light, moderate, or heavy intensity occupations were able to return to their previous level of occupational intensity at a rate of 100.0%, 100.0%, 88.9%, and 85.7% at an average of 1.1 ± 1.0 months, 2.5 ± 2.5 months, 3.5 ± 3.2 months, and 4.3 ± 2.8 months, respectively ( Table 3 ). However, there was no statistical difference between the level of occupational intensity and the rate of return to the previous level of occupation (P = 0.4) or the duration of RTW (P = 0.3).
Rate and Duration to Return to Work to the Same Level of Occupational Intensity.
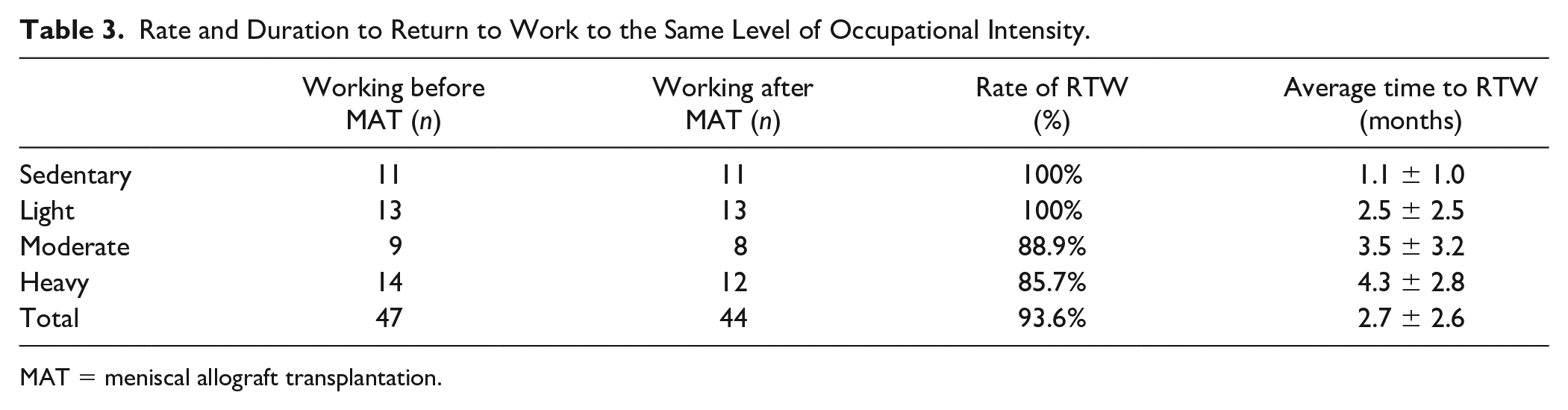
MAT = meniscal allograft transplantation.
A subgroup analysis was performed on patients with isolated MAT (n = 13) and those with concomitant OCA/microfracture (n = 34). There was no difference in the rate of RTW (92.3% vs. 100.0%; P = 0.5) and the duration of RTW (4.1 ± 3.3 months vs. 2.2 ± 2.2 months; P = 0.06).
Discussion
In this investigation, we demonstrated that 97.8% of patients returned to their previous level of occupational intensity by 2.7 ± 2.6 months postoperatively, while 93.6% of patients were able to return to their previous level of occupational intensity. Patients with workers compensation designation returned to work by 4.4 ± 3.7 months postoperatively. Although statistically insignificant, patients with higher levels of occupational intensity had a lower rate and longer duration of RTW. Since MAT is commonly performed in young, active patients that comprise the majority of the work force, it is imperative that physicians appropriately counsel patients in order to manage post-operative expectations.
Return to work following elective orthopedic procedures is an important consideration; however, information regarding one’s ability to function in the workplace following MAT is lacking. Only 20% of active military members were able to return to full duty following MAT, while a staggering 50% of military personnel were terminated from active service. 34 In the present investigation, nearly every patient was able to RTW and there was no difference in rate or duration of RTW between occupational intensities. Although high-level athletes are able to return to sport following MAT at short-term follow-up,19,35,36 it may be unreasonable to extrapolate the findings of high-functioning individuals to the military population. Compared to civilians, active duty service members have higher activity requirements and responsibilities that may not be amenable to standard postoperative care and rehabilitation. This may portend worse outcomes with respect to return to active duty in military service members that undergo MAT.
Chondral damage identified and treated by cartilage restoration at the time of MAT demonstrated no difference in complications, failures, and resulted in significant improvements in patient-reported outcome measures. 14 There was no difference in the rate or duration of RTW in isolated MAT and those who received concomitant cartilage restoration procedures. There is likely no difference since the rehabilitation protocols are identical. Furthermore, Liu et al. demonstrated that 100% of patients were able to RTW by 3.1 months following MAT with concomitant high tibial osteotomy; however, only 88.9% of patients were able to return to preoperative level of occupational intensity. 24 The rate and duration of RTW following MAT (97.8%; 2.7 months) and HTO + MAT (100.0%; 3.1 months) is relatively similar. This is likely due to identical rehabilitation protocol in both procedures as patients are kept protected weight bearing for 6 weeks in each case. A high proportion of patients who have meniscal deficiency, limb malalignment and chondral defects that undergo MAT, off-loading osteotomy, and concomitant cartilage restoration are able to RTW.
The senior author utilizes a non–weight bearing/heel-touch rehabilitation protocol for the first 6 to 8 weeks following surgery. This may allow patients with sedentary or light-intensity occupations to RTW sooner than those with higher-intensity vocations. Twenty-one percent of patients had a worker’s compensation (WC) claim at the time of surgery. WC patients demonstrated a lower rate of RTW (90% vs. 97.9%) and a longer duration of RTW (4.4 months vs. 2.5 months). Workers compensation status is associated with reduced ability to achieve clinically significant outcomes following MAT. 12 The exact effect of WC status on achieving clinically significant outcomes is unknown. It has been hypothesized that the process of making such claim, secondary gain, or other unidentifiable causes may result in worse outcomes in this population.12,37 Patients who do not have a worker’s compensation claim may experience greater subjective outcome improvement and may be more economically motivated to RTW following operative intervention. It is imperative that physicians and patients are aware of these findings when making the decision whether to pursue MAT.
There were no cases of revision MAT in this cohort; however, 28% of patients returned to the operating room for at least one additional procedure. Furthermore, 91.5% of patients reported at least one complaint postoperatively. The rate of reoperation following MAT is between 1% and 32%. 6 The wide range in reoperation rate may be attributed to several factors such as patient demographics, operative technique, rehabilitation protocols, patient expectations, and indications for reoperation. Nearly every patient had at least one complaint following MAT, which may be due to higher expectations in a young population. These patients may have higher intensity occupations that may lead to additional meniscal tears or degeneration. This can cause pain, swelling, and stiffness as well as additional procedures to remove torn or degenerative tissue. Although MAT is associated with a high rate of satisfaction and RTW, patients may experience residual symptoms and may return to the operating room. Nonetheless, MAT is a viable option for tibiofemoral joint preservation in appropriately selected patients.22,38,39
It is imperative that the analysis of this investigation be interpreted within the context of the study’s limitations. Differences in patient’s demographics or occupational demands may slightly inhibit the external validity of these findings. The inclusion of patients who underwent concomitant osteochondral allograft transplantation causes heterogeneity in the patient population. However, Saltzman et al. demonstrated that concomitant cartilaginous procedures do not affect outcomes of MAT. 14 This was a retrospective study and may result in recall bias, which may cause the duration of RTW to be earlier than expected. However, its design is similar to previous studies that examined RTW and patient satisfaction following orthopedic procedures.23-32 This study is also subject to nonresponse bias as 25.6% of patients were lost to follow-up. Patients lost to follow-up may represent a fundamentally different patient population than those included in this study. This investigation may also be subject to selection bias as the senior author may have deemed that certain patients may be optimal or poor candidates for MAT due to factors other than clinical or age parameters. Motivation to RTW may be affected by economic need, social situation, disability coverage, comorbidities, and health insurance coverage. However, the reason that patients returned to work was not identified. The time period that patients identified postoperative complaints was not specified. Therefore, the incidence of postoperative complaints may be inflated and be unrelated to disease progression. A subgroup analysis of isolated MAT and workers compensation status was performed; however, these results may be subject to type II error due to the small sample size. The questionnaire distributed to patients is not validated and may inhibit its interpretation across other populations. Standardized legacy patient reported outcome measures, such as International Knee Documentation Committee, Knee Injury and Osteoarthritis Outcome Score, and Lysholm were not assessed and may limit the interpretation of our findings.
Conclusion
In patients with painful meniscal deficiency, MAT provides a high rate of RTW (97.8%) by 2.7 ± 2.6 months postoperatively. However, some patients may be unable to return to their previous level of occupational intensity. Although statistically insignificant, patients with higher intensity occupations may have a lower rate and may longer to RTW than those with less physically demanding occupations. Information regarding RTW is imperative to appropriately manage postoperative expectations.
Footnotes
Authors’ Note
Authorship of the present manuscript was considered by following ICJME guidelines. All included authors contributed to either the conception, design, data acquisition, or data analysis. All authors were involved in drafting of the manuscript and had opportunity to revise the final content. The authors are agreeable to the aspects presented within this work.
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval for this study was obtained from Rush University Medical Center IRB - 15031008-IRB01.
Informed Consent
Informed consent was not sought for the present study because the study was exempt from informed consent.