
Abstract
Objective
Developmental dysplasia of the hip (DDH) is the most common skeletal development in children and could result in secondary osteoarthritis. This study aims to clarify the alternations of subchondral trabecular bone remodeling and microstructural properties during the development of DDH, and the potential influence of these alternations on the overlying cartilage degeneration and DDH progression.
Design
Traditional straight-leg swaddling method was adopted to establish DDH model in newborn Sprague Dawley rats. Hip joint specimens from normal or DDH rats were used. Typical features of DDH in radiological examination were observed by x-ray analysis. Micro–computed tomography analysis was applied to evaluate the microstructural properties of subchondral bone at postnatal weeks 2, 4, and 6. Histological and immunohistochemical analyses were adopted to appraise subchondral bone remodeling activity and cartilage degeneration. The associations among subchondral bone, articular cartilage, and DDH severity were analyzed via multiple linear regression analysis.
Results
Compared with control group, the subchondral bone in DDH group displayed a gradual trend of deteriorated microstructure and worsening biomechanical properties along with aberrant bone remodeling, which might be responsible for the inhibition of stress transmission from the articular cartilage to the subchondral bone and thus leading to the cartilage degeneration and accelerated DDH progression.
Conclusions
Our findings indicate that alternations of subchondral trabecular bone in a time-dependent manner could contribute to the DDH progression and the amelioration on subchondral bone might be a favorable therapeutic candidate for DDH.
Keywords
Introduction
Developmental dysplasia of the hip (DDH) is a common congenital abnormality, which impairs the acetabulum and occasionally the proximal femur over a lifetime.1,2 The hip instability caused by DDH can lead to inhomogeneous stress distribution and raise the risk of chondral degeneration and secondary osteoarthritis (OA).3-5 A cross-section survey revealed that the prevalence of DDH was 1.52% among Chinese adults; the total medical costs pose a heavy financial burden on the Chinese medical system. 6 For DDH patients, if they cannot be detected early and treated appropriately, most of them will develop serious hip OA and require total hip replacement (THA).7-9 The best way to prevent hip dysplasia from progressing to secondary OA is to diagnose it as soon as possible and restore the natural anatomical hip structure before the cartilage degeneration becomes irreversible. 10 Therefore, the key issue is to illustrate the specific progress and the underlying biomechanisms in the development of DDH.
Recently, some studies have suggested that microstructural changes in subchondral trabecular bone might be a crucial factor for the development of primary OA using imaging technologies, such as the micro–computed tomography (µCT).11-14 Meanwhile, Liu et al. 15 found that the subchondral bone biomechanical properties in OA patients extracted by micro–finite element analysis (μFEA) were closely related with the variations of subchondral bone microstructure and had a profound effect on OA progression. We have formerly illustrated that the changes in subchondral bone could bring about the accelerated OA progression while OA co-occurred with osteoporosis in the same individuals. 16 However, there are few studies about whether these changes could affect the DDH ongoing, which needs to be further clarified. Moreover, it is not clear whether the onset of DDH is initiated in cartilage or subchondral bone. In our previous study, we have compared structural and biomechanical properties of subchondral trabecular bone and their relevance with cartilage degradation between advanced DDH patients and primary OA patients. Our findings revealed that DDH patients had deteriorating microstructures and inferior biomechanical properties of subchondral trabecular bone, which might have a connection with cartilage damage. 17 Nevertheless, our previous study merely analyzed patients with advanced symptoms of DDH and did not observe the dynamic changes of subchondral trabecular bone remodeling, microstructural properties, and their relationship with cartilage degeneration during the whole development of DDH, which so far remains unknown. Solving these above-mentioned problems will enable us to better understand the biomechanical changes underlying the pathogenesis of DDH and establish a subchondral trabecular bone–related targeting treatment.
In this study, we performed a straight-leg swaddling model on Sprague Dawley rats to investigate the alternations in subchondral trabecular bone and their relationships with cartilage degeneration in the development of DDH. We aimed to clarify the changes of subchondral bone remodeling and microstructural properties in the time dimension during the development of DDH and explore the effect of these changes on the overlying cartilage damage. We hypothesize that during the DDH progress, the subchondral bone might gradually undergo aberrant bone remodeling and cause the deterioration of microstructure and biomechanical properties, thereby impairing normal hip joint structure and finally leading to severe DDH symptoms.
Methods
Animals and DDH Model
A total amount of 48 male neonatal Sprague Dawley rats (~5 g) were used in the present study. The experimental procedures relating to rats were approved by the Institutional Animal Care and Use Committee (IACUC) of our hospital (approval code: SYXK [Shanghai, China] 2020-0072). The newborn rats were kept at following environment: temperature 20°C~22°C, relative humidity 45%~65%, 12 hours/12 hours light/dark cycle at a specific pathogen-free facility. The rats were randomly distributed to DDH model group (n = 24) or control group (n = 24) by a randomization table, which was blinded to avoid the bias of this study. After that, rats in separate cages were provided with general food and water. As is shown in
Figure 1A
, the DDH model was induced by a straight-leg swaddling method, which involved fixation of the hip and knee with medical tapes at the positions of hip adduction and extension for postnatal 10 days as previously described.18,19 Rats in control group received no interventions. Subsequently, 8 rats from the DDH group and 8 rats from the control group were randomly selected and sequentially euthanized under the overdose of pentobarbital sodium at postnatal weeks 2, 4, and 6. At each time point, the rats were subjected to the x-ray analysis immediately after killing, and the whole pelvises containing complete acetabulum and femoral heads were isolated for further analysis (
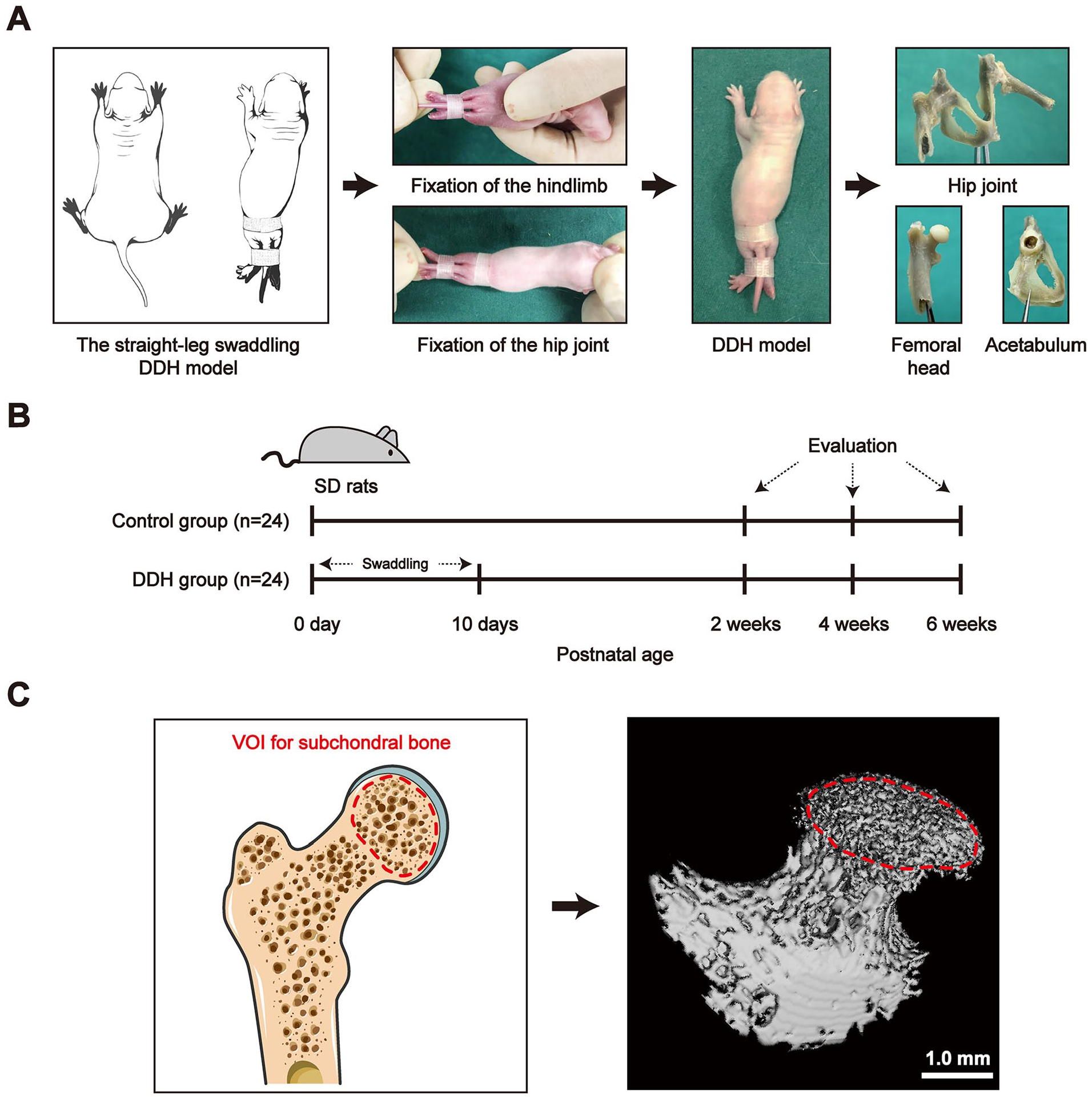
Schematic diagram for the experimental design. (
X-Ray Analysis
High-resolution radiographs of the standard ventrodorsal hip extended view (SVDV) of pelvis in rats were taken at postnatal weeks 2, 4, and 6, using an x-ray machine (Faxitron X-ray Corporation, USA) with a 3-second exposure time. Several measurements were carried out assessing the extent of hip joint displacement as reported before, including acetabular index (AI), lateral center-edge angle (LCE angle), femoral coverage percent (FC percent), and distraction index (DI). 20 Briefly, AI is described as the angle between a parallel line intersecting the point of the ilium and ischium and another line running from the above-mentioned point to the outer edge of ilium inferior margin. LCE angle is measured by a vertical line and another line connecting the femoral head center with the acetabulum lateral edge. FC percent is evaluated as the percent of the femoral head covered by the acetabular rim. DI is calculated considering d/r. The d refers to the interval between acetabulum center and femoral head center. The r refers to the radius of the femoral head.
Micro-Computed Tomography Analysis
A high-resolution μCT system (Micro-CT 80; Scanco Medical AG, Switzerland) was employed to scan the whole pelvises and hip joints from both groups from each time point at 10 μm isotropic voxel size. We determined the femoral head subchondral bone as the volume of interest (VOI) using the semiautomatic contouring method, which was extracted by the reconstructed 3-dimensional image (VOI for subchondral bone,
Histological and Immunohistochemical Analysis
After x-ray analysis and µCT scanning, 4% paraformaldehyde was used for the fixation of all femoral head specimens for 24 hours. Thenceforth, fixed samples were decalcified in 10% EDTA solution for about 3 weeks, followed by the dehydration and paraffin embedding. The embedded samples were cut into serial sections (5 μm) and stained with hematoxylin and eosin (H&E) and Safranin O-Fast Green. The cartilage degeneration level was measured according to the Osteoarthritis Research Society International (OARSI) scoring system. 21 Five sequential sections from each sample were processed and estimated. For Terminal Deoxynucleotidyl Transferase-mediated dUTP Nick-End Labeling (TUNEL) staining, the apoptotic chondrocytes were detected using the In Situ Cell Death Detection Kit, Fluorescein (Sigma-Aldrich) according to the manufacturer’s instructions. The number of positively stained cells were calculated by Image-pro Plus software.
Immunohistochemical (IHC) staining was performed to evaluate sections of the decalcified femoral head samples. All sections were deparaffinized and processed with antigen retrieval in citrate buffer. After that, sections were treated with primary antibodies including matrix metalloproteinase-3 (MMP-3; Abcam, UK) and osteocalcin (Abcam, UK) at 4°C overnight. Followed by 3 times of rinse in 0.1 M PBS, sections were incubated with horseradish peroxidase-labeled secondary antibody for 1 hour. Diaminobenzidine was used to develop the substrate color. For the osteoclasts staining, tartrate-resistant acid phosphatase (TRAP) staining was applied according to the protocol of a commercial TRAP staining kit. An optical microscope (Leica Microsystems AG, Germany) was employed to obtain images and the number of positively stained cells were calculated by Image-pro Plus software. In addition, 5 sequential sections in each specimen were stained and 5 areas in each section were evaluated.
Statistical Analysis
Data were processed by the SPSS 19.0 statistical software and presented as mean ± standard deviations (SDs). The comparison of two groups across different time points were conducted using 2-way analysis of variance (ANOVA) and Turkey’s test for post hoc tests. Furthermore, to explore the correlation of DDH severity and subchondral bone properties in the control and DDH groups, multiple linear regression analyses with microstructure and biomechanical properties of the subchondral bone were performed for the OFA (Orthopedic Foundation for Animals Hip) score, LCE angle, FC percent, percentage of MMP-3+ chondrocytes, and subchondral trabecular bone remodeling activity. For the linear regression analysis, 2-tailed Pearson correlation analyses were adopted. P < 0.05 was considered as statistically significant.
Results
Analysis of Macroscopic Observation and Radiography Measurements
Macroscopic observations of the hip joint morphology from control and DDH groups are presented in
Figure 2A
. From the hip general view of the DDH group, the articular capsule of the hip joint became thickened and hypogenetic articular cartilage was unable to be visualized, which proves the usability of our DDH modeling. Conversely, the joint capsule was thin and transparent enough to observe the cartilage in control group. In addition, the shallow acetabulum and flat femoral head were discovered in DDH group at postnatal weeks 2 and 4, which indicated the development of dysplasia hip joint. At postnatal weeks 4 and 6, false acetabulum appeared along with shallow acetabulum. The hip grading of both groups at different time points was classified according to the OFA scoring system,
22
which suggested that the severity of hip deterioration in the DDH group was constantly aggravating over time (
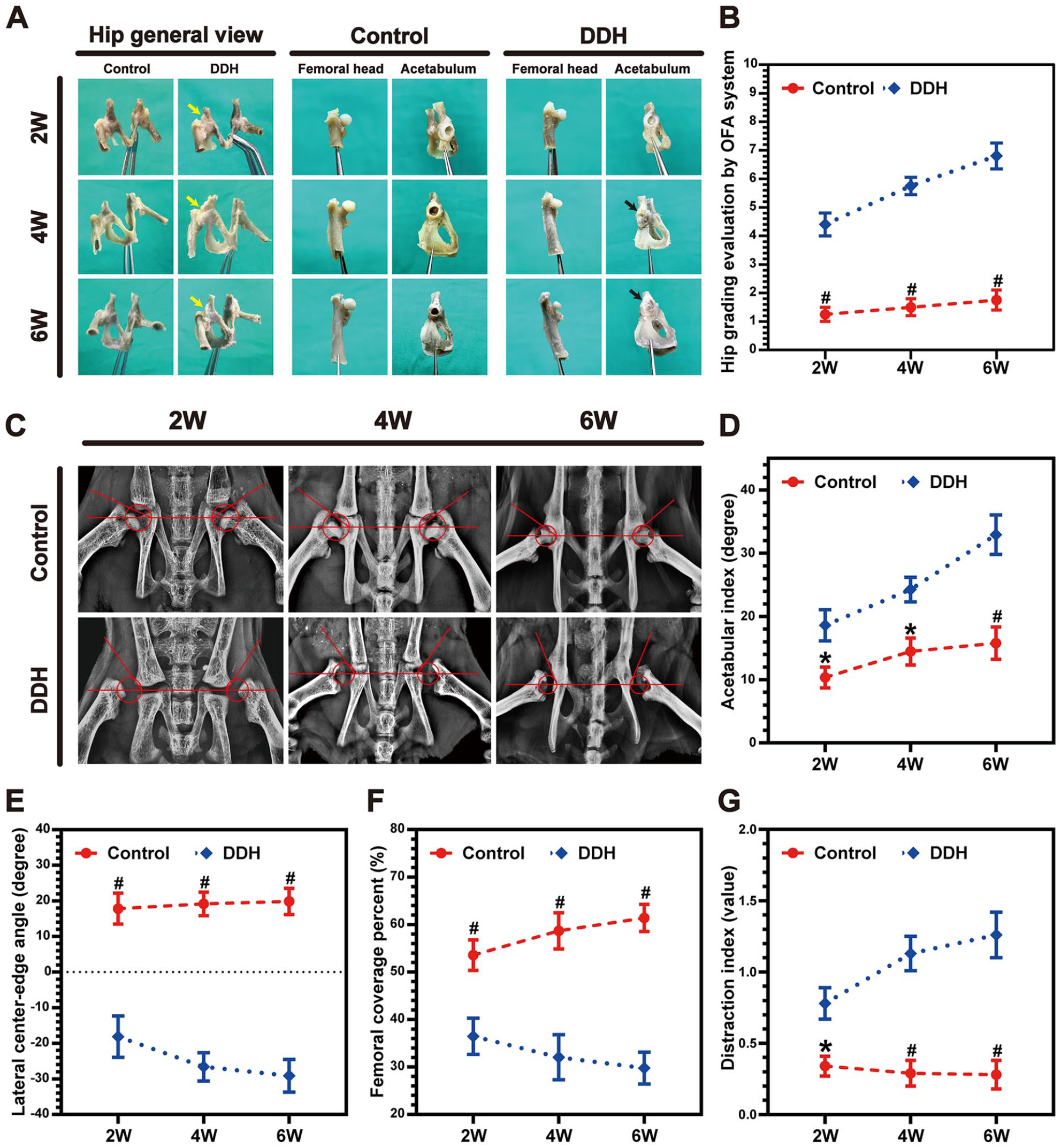
Macroscopic view of the hip joint and analysis of the hip joint x-ray images at different time points. (
Radiographic evaluation plays a critical role in the diagnosis of DDH. Among various radiographic measurements, x-ray analysis provides a direct view into the anatomical structure and developmental situation of hip joint. In
Figure 2C
, the anteroposterior pelvic x-ray results demonstrated that the acetabulum fossa was initially formed at postnatal week 4 in control group, which became deeper at postnatal week 6. Meanwhile, the shape of femoral head became fuller during the follow-up period. By contrast, the structure of acetabulum seemed to have disappeared in DDH group and the femoral head showed a dislocation from postnatal weeks 2 to 6. Furthermore, we performed several measurements on x-ray images, including acetabular index (AI), lateral center-edge angle (LCE angle), femoral coverage percent (FC percent), and distraction index (DI), which indicated the femoral head malposition. The AI and DI in DDH group raised dramatically from postnatal weeks 2 to 6, while the AI and DI in control group maintained at a significantly lower degree than the DDH group (
Analysis of Femoral Head Cartilage Degeneration
Histological analysis, TUNEL staining, and IHC analysis were applied to examine the degeneration of femoral head cartilage in both groups. The morphology of cartilage layer was plumper in the control groups than that of DDH groups according to the H&E and Safranin O staining. Moreover, cartilage layer of the DDH groups showed a flat appearance and destructed cartilage surface at week 6 and the transition area of cartilage to subchondral bone seemed much looser (
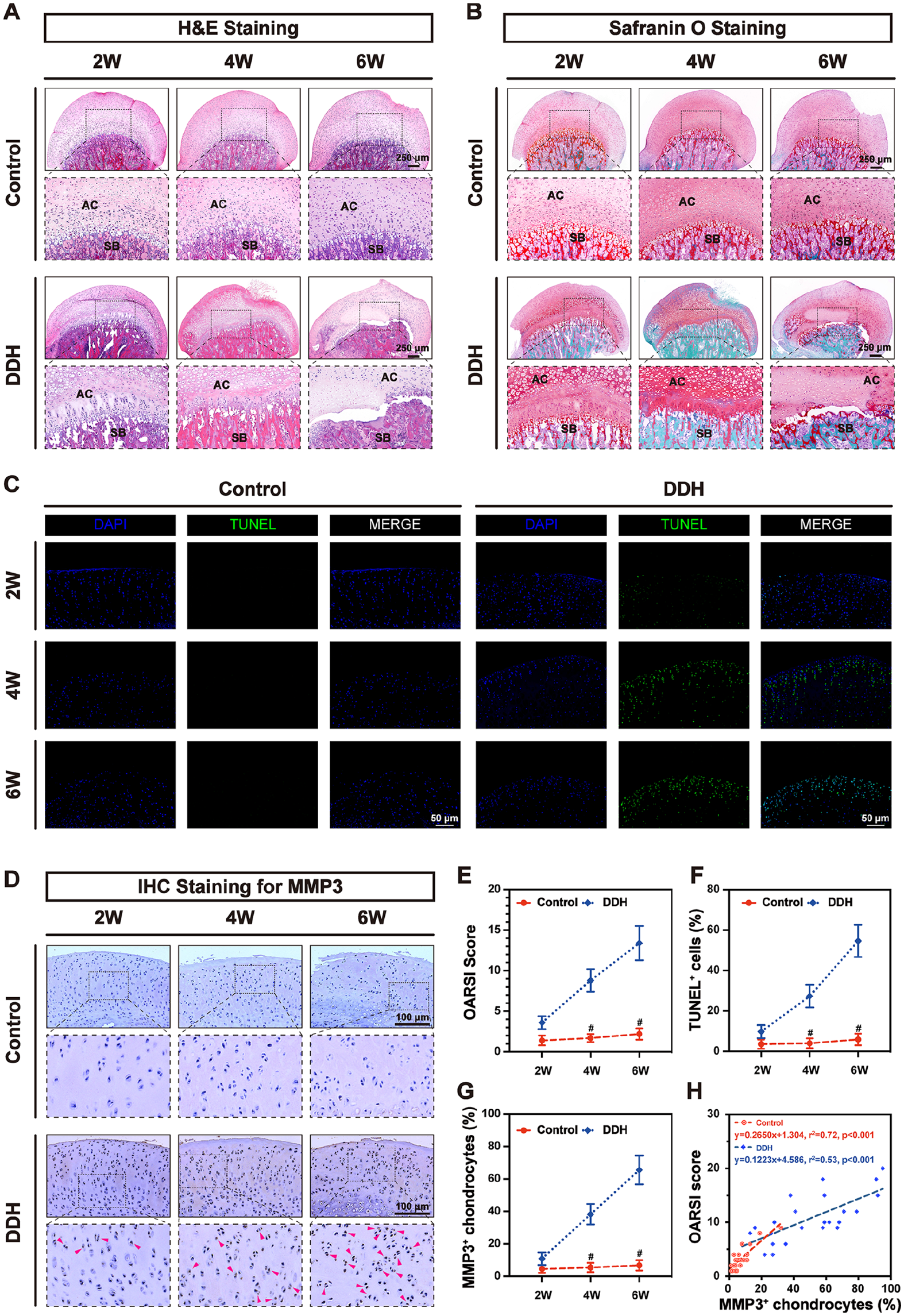
Analysis of the femoral head cartilage at different time points. (
Micro-CT Scanning Analysis
The µCT was performed to visualize the 3D structure of hip joint and femoral head formation at different time points. According to the anteroposterior (AP) view and lateral view of reconstructed μCT images, the shallow acetabulum and femoral head malposition in the DDH group were clearly recognized (
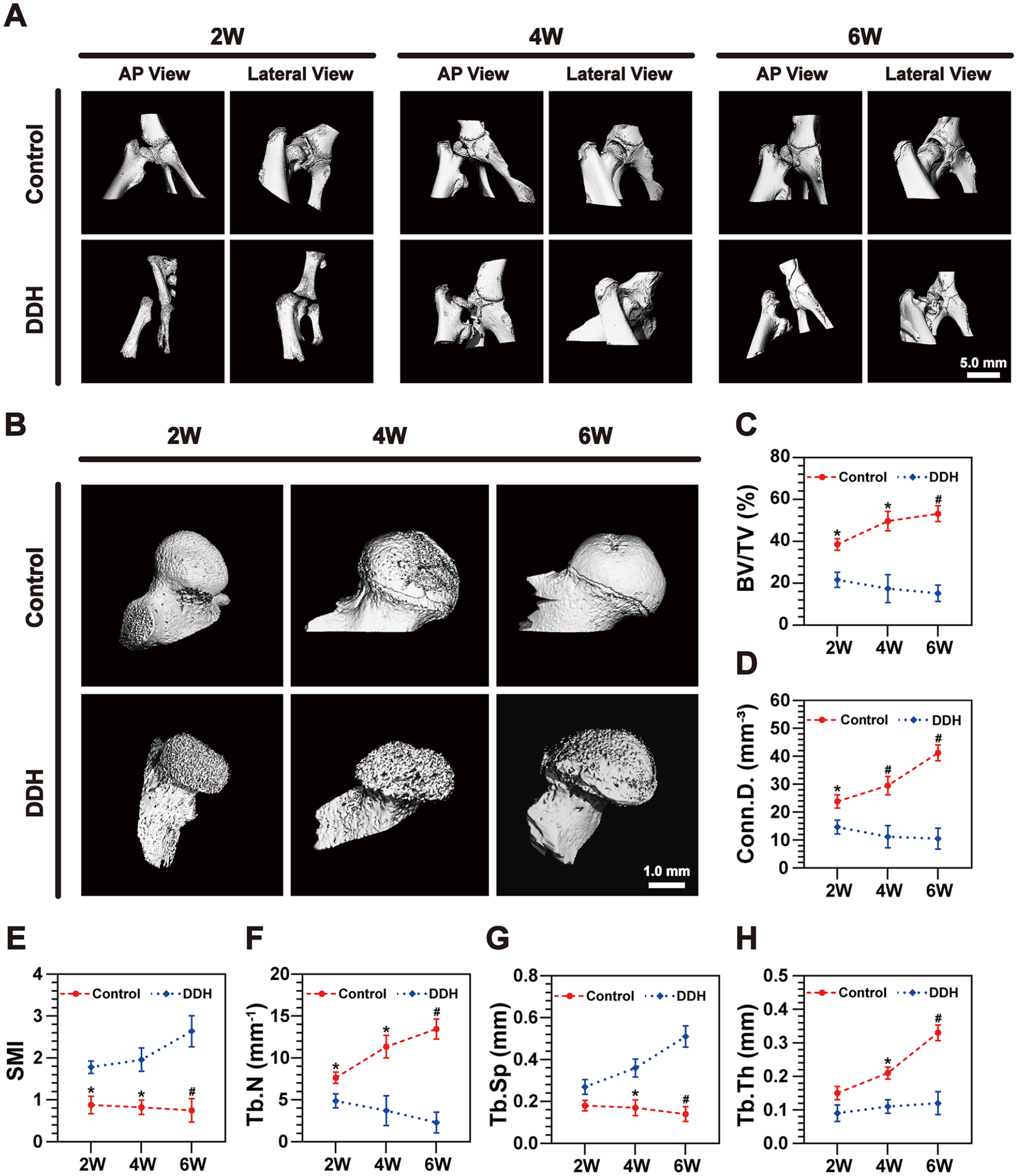
The μCT reconstruction of the hip joint and analysis of subchondral bone microstructural properties at different time points. (
Analysis of Subchondral Bone Remodeling
The subchondral bone remodeling activity was investigated by immunohistochemistry and presented in
Figure 5
. In DDH groups, there were significantly fewer osteocalcin+ osteoblasts and more TRAP+ osteoclasts in subchondral bone than control at different time points, implying that the abnormal bone resorption activity in DDH groups took a predominant place of subchondral bone remodeling during continuous DDH progression, while the bone formation activity played a major role throughout the normal development in control groups. From the time-course quantitative results in
Figure 5B
and
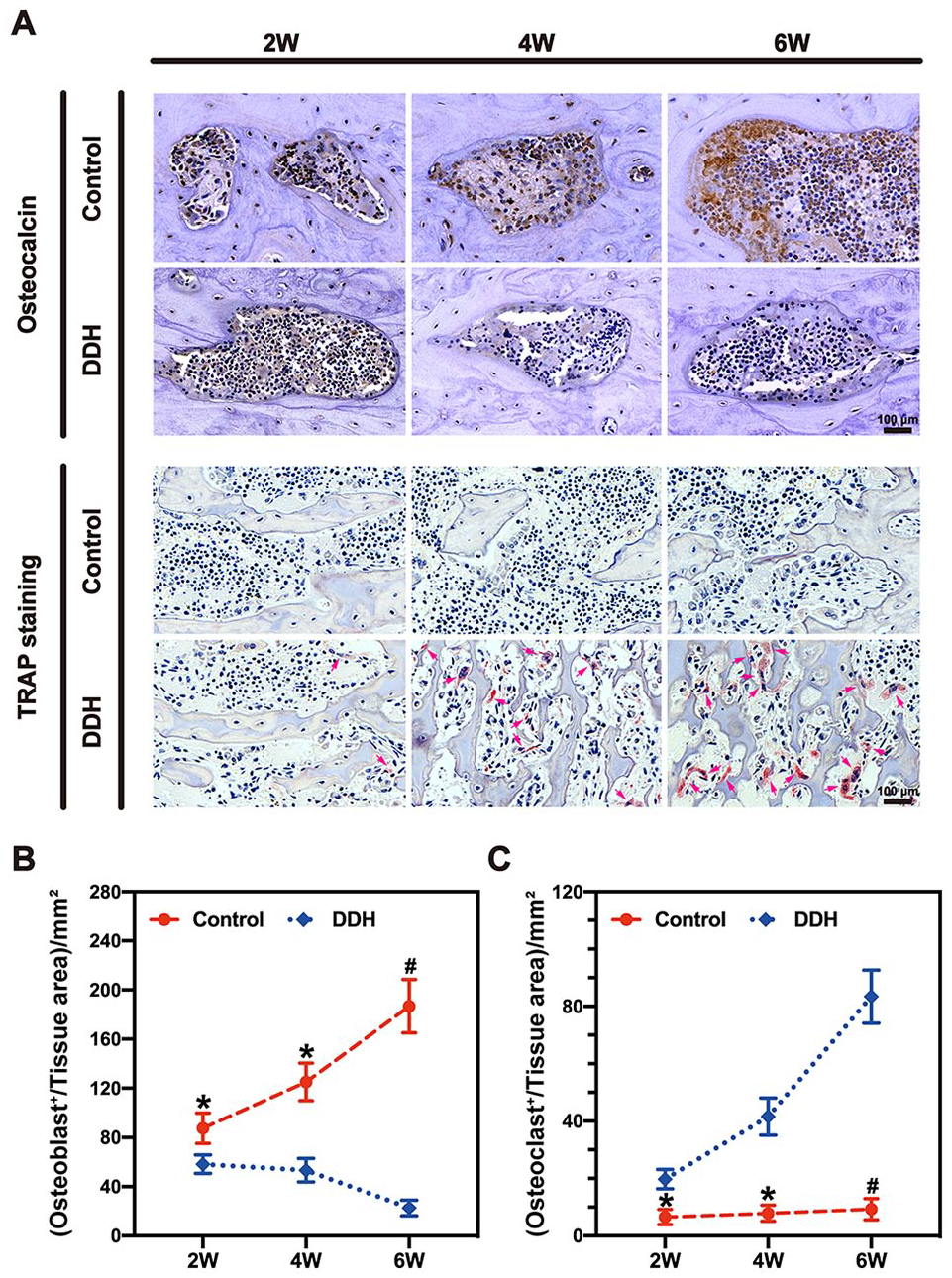
Analysis of the Osteocalcin+ osteoblasts and TRAP+ osteoclasts activity in subchondral bone at different time points. (
Multiple Linear Regression Analysis between Subchondral Bone, Cartilage Degeneration, and DDH Severity
As is shown in
Table 1
, the multiple linear regression analysis was employed to illuminate the correlation between subchondral bone microstructural properties and remodeling activity. Because of the very few of TRAP+ osteoclasts in control group, the relevance between TRAP and subchondral bone properties seems to be indistinct. The results of
Table 1
suggested that the subchondral bone formation activity (OCN) was positively correlated with most of the subchondral bone microstructural properties (BV/TV, Conn.D, Tb.N, Tb.Th) and negatively correlated with SMI and Tb.Sp in both groups, whereas the resorption activity (TRAP) displayed a strong association with BV/TV, Conn.D, SMI, Tb.N, and Tb.Sp in DDH group (r2 > 0.3, P < 0.05). Moreover, multiple linear regression analysis was also adopted to illuminate the correlation between the subchondral bone microstructural properties and DDH severity (OFA score, LCE angle, FC percent, and MMP-3) in
Table 2
. Evidently, the correlation coefficients for these subchondral bone properties were higher in DDH group, implying that subchondral bone properties acted as a pivotal part during the DDH development. Together, the results of
Tables 1
and
Correlation Coefficient of Linear Regression between Subchondral Bone Microstructural Properties and Subchondral Bone Remodeling.
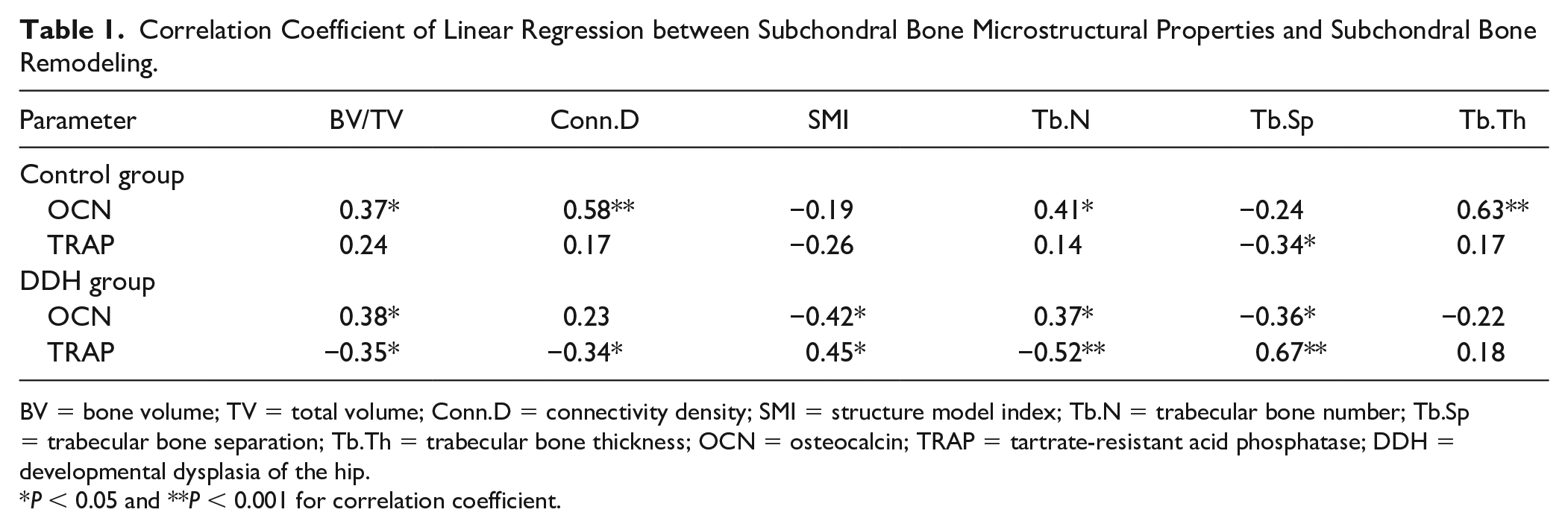
BV = bone volume; TV = total volume; Conn.D = connectivity density; SMI = structure model index; Tb.N = trabecular bone number; Tb.Sp = trabecular bone separation; Tb.Th = trabecular bone thickness; OCN = osteocalcin; TRAP = tartrate-resistant acid phosphatase; DDH = developmental dysplasia of the hip.
P < 0.05 and **P < 0.001 for correlation coefficient.
Correlation Coefficient of Linear Regression between Subchondral Bone Microstructural Properties and DDH Severity (Including Articular Cartilage Degeneration).
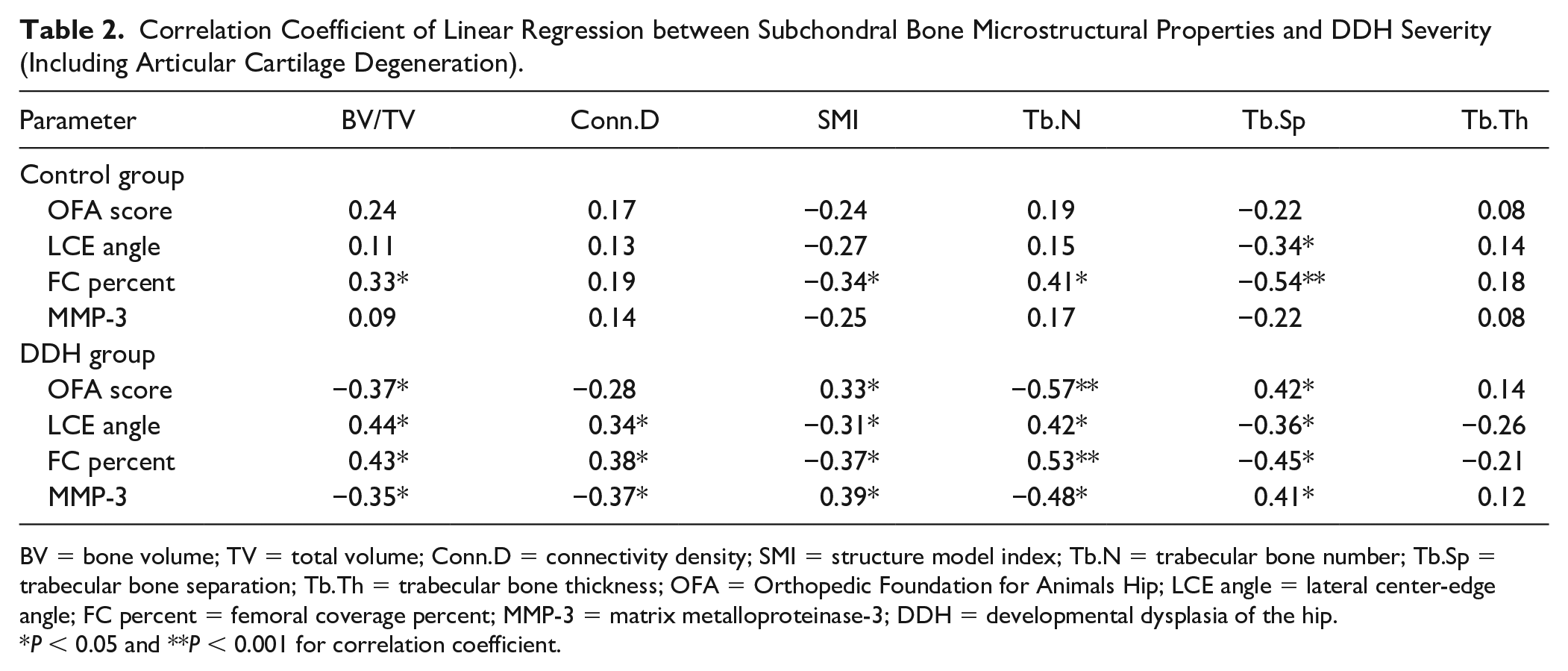
BV = bone volume; TV = total volume; Conn.D = connectivity density; SMI = structure model index; Tb.N = trabecular bone number; Tb.Sp = trabecular bone separation; Tb.Th = trabecular bone thickness; OFA = Orthopedic Foundation for Animals Hip; LCE angle = lateral center-edge angle; FC percent = femoral coverage percent; MMP-3 = matrix metalloproteinase-3; DDH = developmental dysplasia of the hip.
P < 0.05 and **P < 0.001 for correlation coefficient.
Discussion
In this study, we generated DDH rats using the traditional straight-leg swaddling model to explore the alternations in subchondral trabecular bone microstructural properties and remodeling activity, as well as their correlations with cartilage damage during the DDH progression. We have previously conducted a series of retrospective analyses on patients with advanced DDH and demonstrated that the subchondral bone had undergone many changes and was closely related to the degeneration of overlying cartilage, which eventually induced serious OA symptoms. Moreover, although severe arthritis symptoms may occur in advanced DDH, the specific changes in the remodeling activity and subchondral bone properties were not the same as those of primary OA. 17 In the continuous progression of DDH, the femoral head suffers a long-term dislocation trend and abnormal biomechanical environment, leading to secondary OA in the advanced stage. Prior studies have demonstrated that transformations of subchondral bone acted as a vital role during primary OA, whereas its continuous changes in the time dimension of DDH progression and the effect on secondary cartilage damage remains unknown.23-26 Therefore, we selected postnatal 2-, 4-, and 6-week DDH rats (according to previous report) 27 to carry out a series of experiments in the present study and found that subchondral bone developed a succession of abnormal remodeling along with DDH exacerbation. Clarifying the relationships between subchondral bone alternations and DDH development could help to elucidate the underlying biomechanisms of this congenital disease. Furthermore, the improvement in subchondral bone with bone-metabolism agents may help mitigate DDH progression.
From our results of macroscopic view, x-ray and μCT reconstructed images, we observed the successfully induced dysplasia hip and typical manifestations of ongoing DDH in rats. Our previous study has demonstrated the imbalance of the biomechanical environment homeostasis occurred in advanced DDH. 17 Owing to a continuous process, the stabilization of biomechanical environment around the femoral head is destined to be gradually broken along with the deterioration of DDH in an age-dependent manner. Considering the relatively greater rigidity and strength than covering cartilage, the subchondral bone bears most of the biomechanical forces transmitted from the joint area. 28 As a matter of fact, the load-bearing capability of subchondral bone, that is, its biomechanical property rely on the microstructure and bone remodeling activities of itself. The positive correlation between microstructure and biomechanical properties in subchondral bone has been proved according to various studies.16,17,29-33 Aizah et al. 34 had originally proposed that significant changes of subchondral bone remodeling occurred at the very early stage in a rat OA model. Although severe OA symptoms appear in the late stage of DDH, the role of subchondral bone in the whole progression of DDH has not been illustrated yet. Our current study showed that though the general view of the hip joint as well as the histological and IHC analysis of cartilage in the DDH group displayed almost no differences with the control group at early stage (2 weeks), the subchondral bone microstructural properties appeared to be inferior, suggesting that alternations in subchondral bone emerged earlier than cartilage degeneration. Moreover, the results indicated that the peak period of progression was from weeks 4 to 6 and was consistent with the period of accelerated deterioration of subchondral bone microstructural properties, suggesting that the alternation of subchondral bone is the key factor in the acceleration of DDH development. The multiple linear regression analysis showed these subchondral bone changes could give reasons for the aggravating cartilage damage in different stages.
Subchondral bone constantly undergoes dynamic changes of bone resorption and formation, and the precise harmony between osteoclasts and osteoblasts is crucial for maintaining metabolite homeostasis.35-37 Our previous studies have demonstrated that abnormal bone remodeling could occur once the equilibrium of osteoclasts and osteoblasts was broken, resulting in exacerbation of the subchondral bone, and eventually leading to severe arthritis manifestations.16,17,30,33 In the current study, the abnormal remodeling in DDH rat subchondral bone has also been observed at the cellular level as relatively active osteoclast activity and sluggish osteoblast activity throughout the disease progression. Furthermore, linear regression analysis revealed that the abnormal remodeling issue was highly correlated with the deteriorated microstructural properties of subchondral bone. We believe that in the initial stage of DDH, the unstable biomechanical condition around malformed hip joint leads to abnormal subchondral bone remodeling, which emerges in the early stage and results in the accelerated aggravation of microstructure and serious degeneration of articular cartilage in the middle and late stages. Indeed, the alliance between subchondral bone microstructural properties and DDH severity was also proved by linear regression analysis, implying the disease progression was based on the incremental deteriorative subchondral bone suffered from abnormal bone remodeling.
Based on the theories in our previous and present results, we illuminated time-dimensional changes in the subchondral bone during the development of DDH and how these changes contribute to disease progression and exacerbation (
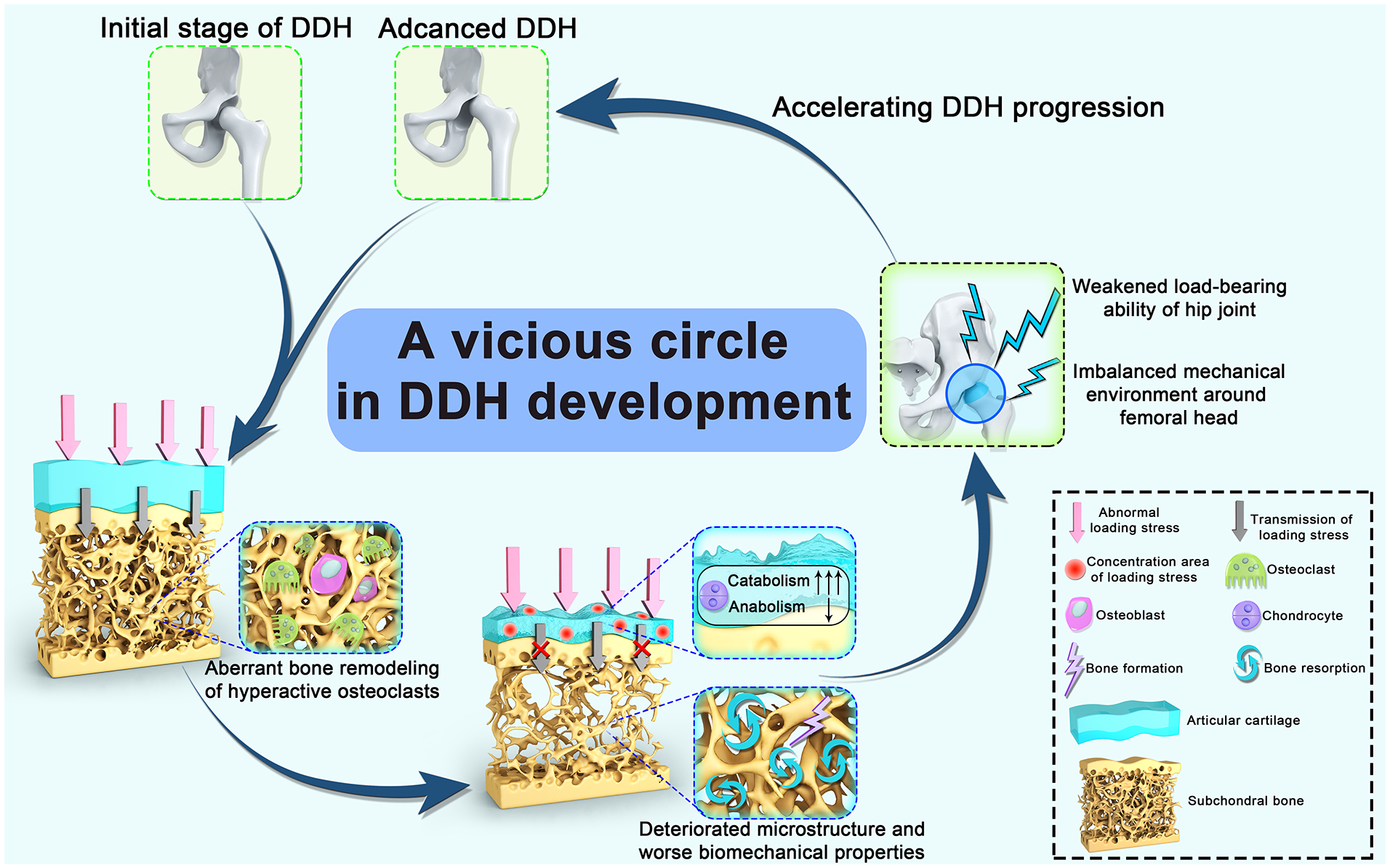
Schematic picture for the potential vicious circle in DDH development. At the initial stage of DDH, the femoral head suffers abnormal loading stress due to the congenital hip joint dearticulation, which leads to the aberrant bone remodeling of hyperactive osteoclasts in the subchondral bone. The predominant bone resorption activity in subchondral bone could account for the deteriorated microstructure and worse biomechanical properties, which restrains the stress transmission from the articular cartilage to the subchondral bone. Thus, the enhanced loading stress concentration on the cartilage layer could disrupt the cartilage metabolic homeostasis. These changes are responsible for the aggravated dislocation and weakened load-bearing ability of the hip joint, as well as imbalanced mechanical environment around the femoral head, therefore forming a vicious circle and consequently accelerating DDH progression. DDH = developmental dysplasia of the hip.
Several limitations in this study need to be declared. First, the investigation should be ideally performed on in vivo evaluations of patients in different DDH stages rather than rat models. Actually, the Xtreme-CT is a favorable technique to realize the visualization and quantitative analysis of the subchondral trabecular bone microstructure in the human body. 42 Second, the current study lacks the molecular biological mechanism underlying aberrant subchondral bone remodeling in DDH development. Our further study is dedicating to reveal the precise mechanism at cellular level. Third, due to the unclear etiology of DDH, our conclusions should be limited to the specific model for DDH used here and could not be expanded to all DDH cases in human patients.
Collectively, our study indicates that over the whole DDH progression, the subchondral trabecular bone suffers aberrant bone remodeling activity, deteriorative microstructure, and biomechanical properties that give reasons for the gradual degeneration of overlying cartilage and advanced DDH. As far as we know, this is the first study to elucidate the biomechanical causality between subchondral bone and articular cartilage during the development of DDH. These findings highlight an innovative target for the prevention and medication of DDH.
Footnotes
Author Contributions
TY, LC, BZ, and ZY were involved in the study design, data collection, and analysis. TY and FX performed animal experiment and drafted the first manuscript. HH, ZH, and MW contributed to data acquisition, interpretation, and experimental suggestions. LC, BZ, and ZY provided funding to support the study. ZY and BZ were involved in the manuscript revising. All the authors have read and approved the submitted manuscript.
Acknowledgments and Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was sponsored by the Youth Program of National Natural Science Foundation of China (No. 32000926), Shanghai Sailing Program (No. 20YF1435600), and the National Natural Science Foundation of China (No. 81870972).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Institutional Animal Care and Use Committee (IACUC) of Shanghai Jiao Tong University Affiliated Sixth People’s Hospital (approval code: SYXK [Shanghai, China] 2020-0072).