
Abstract
Objective
To identify the prevalence of mood disorder diagnoses in patients undergoing cartilage transplantation procedures and determine the relationship between mood disorders, opioid usage, and postoperative health care costs.
Design
Patients with current procedural terminology (CPT) codes for osteochondral autograft transplantation (OAT), osteochondral allograft transplantation (OCA), and autologous chondrocyte implantation (ACI) were identified in the Truven Health Marketscan database (January 2009-September 2014). Patients were grouped based on having a preoperative mood disorder diagnosis (preMDD). Preoperative opioids, postoperative opioids ≥90 days, and health care costs within the year postoperative were compared for those with and without mood disorders. Costs were analyzed, adjusting for preoperative cost, sex, age, and opioid usage, for those with and without mood disorders.
Results
A total of 3,682 patients were analyzed (ACI: 690, OAT: 1,294, OCA: 1,698). A quarter of patients had preMDD (ACI: 25.4%, OAT: 20.6%, OCA: 22.7%). Postoperative opioid use was more prevalent in preMDD patients (OAT: 37.1% vs. 24.1%, P < 0.001; OCA: 30.4% vs. 24.8%, P = 0.032; ACI: 33.7% vs. 26.2%, P = 0.070) (odds ratio [OR] ranged from 1.29 to 1.86). First-year postoperative log-transformed costs were significantly greater for preMDD patients (ACI: $7,733 vs. $5,689*, P = 0.012; OAT: $5,221 vs. $3,823*, P < 0.001; OCA: $6,973 vs. $3,992*, P < 0.001; *medians reported). The estimated adjusted first postoperative year cost increase for preMDD OCA patients was 41.7% (P < 0.001) and 28.0% for OAT patients (P = 0.034). There was no statistical difference for ACI patients (P = 0.654).
Conclusion
Cartilage transplantation patients have a high prevalence of preoperative mood disorders. Opioid use and health care costs were significantly greater for patients with preoperative mood disorder diagnoses.
Level of Evidence:
Level III, retrospective therapeutic study.
Introduction
Mental health comorbidities affect a wide array of pre- and postoperative orthopedic outcomes. 1 It is estimated around 20% of adult patients being evaluated for an orthopedic condition meet the PROMIS threshold for moderate anxiety. 2 Approximately, 35% of patients undergoing femoroacetabular impingement syndrome (FAIS) and 27.4% of patients undergoing rotator cuff repair have a diagnosis of anxiety and/or depression and 16% of patients undergoing meniscus repairs have a preoperative mood disorder diagnosis (preMDD).3-5 Poor preoperative mental health is associated with worse pre- and postoperative outcomes in FAIS.6-9 Mental health diagnoses such as depression and anxiety negatively affect postoperative patient-reported pain and function outcomes,10,11 and patient satisfaction. 12
The negative impact of mood disorders on outcomes can be further seen in the form of health care utilization, with mood disorders being associated with greater risk for long-term postoperative opioid use.13-18 Specifically, mental health disorders are associated with increased perioperative opioid use in hip arthroscopy and rotator cuff repair patient populations and worse patient-reported outcomes.3,4,8,19 Last, in addition to poor outcomes and opioid usage, patients with mood disorders have increased health care costs than those without mood disorders.3,4,20
The relationship between mental health and outcomes in patients undergoing articular cartilage surgery remains unclear. Mental health research in patients undergoing articular cartilage surgery is primarily evaluated through self-reported patient-reported outcome instruments. In patients undergoing knee autologous chondrocyte implantation (ACI), postoperative patient-reported outcomes were most strongly associated with the patient’s mental health score (12-Item Short Form Health Survey (SF-12)) rather than the cartilage defect size. 21 On the contrary, preoperative mental health scores were not predictive of postoperative outcomes scores for patients undergoing osteochondral allograft transplantation (OCA). 22 Even less is known about the interaction between mental health diagnosis, cartilage treatment, and perioperative opioid use. Postoperative opioid usage in patients receiving an osteochondral transplantation was examined using the Humana claims database, but the study was limited by its design; the sample size was too small to delineate the interaction between mental health diagnoses and postoperative opioid usage. 23
As the prevalence of mental health diagnoses in patients undergoing articular cartilage procedures is unknown, it is difficult to develop an effective treatment strategy to limit the negative impact of mental health comorbidities.24-27 The purpose of this study was to identify the prevalence of mood disorder diagnoses in patients undergoing cartilage transplantation procedures pre- and postoperatively and subsequently determine the relationship between mood disorders, opioid usage, and postoperative health care costs. Based on the current literature, we hypothesized that (1) more than 20% of cartilage patients would have concomitant preMDD and (2) those with a preMDD would have increased postoperative health care costs and a greater prevalence of prolonged postoperative opioid usage (>90 days).
Methods
We performed a retrospective cohort study, defined by the Oxford Center of Evidence Based Medicine’s 2011 Levels of Evidence as a Level III, 28 through a population-based analysis using the Truven Health Marketscan database to evaluate mood disorders, opioid usage, and health care costs in patients undergoing cartilage transplantation procedures.
Data Source
The Truven database comprised over 135 million unique individuals from Marketscan Commercial claims and encounters and Medicare Supplemental databases (Truven Health Copyright© 2012, 2017 Truven Health Analytics Inc). Due to the de-identified nature of the database, the study did not require institutional review board approval per our institution’s policies.
Study Cohort
Patients were included if they were treated with either an arthroscopic or open osteochondral autograft, arthroscopic or open osteochondral allograft, or an ACI procedure, identified through corresponding current procedural terminology (CPT) codes ( Table 1 ) between January 2009 and September 2014. Patients were excluded if they had either had (1) incomplete insurance coverage in the year before or after the index surgical procedure, or (2) if they had a knee cartilage procedure in the year before or after the index surgical procedure to eliminate confounding opioid prescriptions and associated health care costs.
CPT Codes for Cartilage Transplantation Procedures Evaluated within the Truven Database.
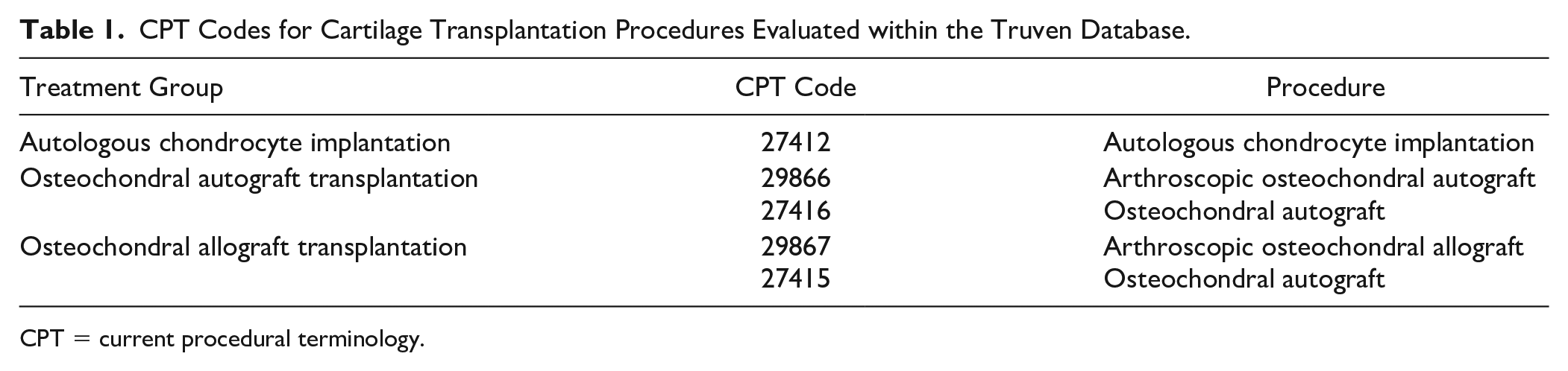
CPT = current procedural terminology.
Exposure Variable
Patients with one or more claims related to mood disorders during the year prior to and following surgery were identified using International Classification of Diseases–9 (ICD-9) codes and respective subsets: 296 (episodic mood disorders), 298 (other nonorganic psychoses), 300 (anxiety, dissociative, and somatoform disorders), 309 (adjustment reaction), and 311 (depressive disorder, not elsewhere classified).3,4 Mood disorder codes related to anxiety and depression were included due to the association between depression and anxiety and poor postoperative outcomes in patients undergoing other cartilage restoration procedures8,29,30 In some instances, the anxiety or depression codes may include another mood disorder, such as a depression with predominant disturbances of other emotions (anxiety). Thus, all mood disorder ICD-9 codes were included for completeness and to allow for comparison between different diseases and conditions previously reported in the literature.3,4
Outcome Assessment
The Truven Health Marketscan database provides information on paid health claims for patients in the United States. The database contains a robust collection of private insured data. 31 Health care costs in the study were defined as the total of any net health care utilization costs, including any deductibles, co-pays, or co-insurance, that the patient incurred during the year prior to and following surgery excluding the cost of medication. These costs were summed for a total health care cost value for both the preoperative and postoperative year to determine utilization of resources by this patient population. 3
Opioid usage was identified via National Drug Code (NDC) numbers associated with an opioid containing medication, such as an opioid agonist (e.g., oxycodone), partial agonist (e.g., tramadol), or opioid combinations (e.g., hydrocodone-acetaminophen). Opioid use was quantified using the date an opioid prescription was filled for each patient. Based on the date an opioid prescription was filled in comparison with the surgery date, the use of opioids was quantified as a binary variable (any preoperative use and prolonged postoperative use defined as 90 or more days postoperatively).
Statistical Analysis
Due to right-skewness in the cost variables, a log transformation was employed to allow for the use of traditional parametric analysis methods. 32 Transformed net health care costs were compared between those with and without mood disorders, both in the year preceding and following a knee cartilage procedure, using 2-sample t-tests. Qualitative variables (sex and the 2 binary opioid use variables described above) were compared between those with and without a preoperative mood disorder using Pearson chi-squared tests. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated. An analysis of covariance (ANCOVA) was used to determine if postoperative procedural costs were significantly different for those with and without mood disorders with adjustments for the covariates of preoperative cost, sex, age, and both pre- and postoperative opioid usage. Across all analyses, a P value of less than 0.05 was considered significant. Analyses were completed using R, version 4.0.4 (R Foundation for Statistical Computing; Vienna, Austria) except for ORs which were completed using MedCalc, version 19.4 (MedCalc Software, Ostend, Belgium).
Results
A total of 4,058 patients met the CPT code criteria for inclusion. Of the 4,058 patients, 376 patients were excluded for having more than one cartilage surgery billed within the same year. The remaining 3,682 patients were analyzed (690 ACI patients, 1,294 osteochondral autograft transplantation (OAT) patients, and 1,698 OCA patients) (Fig. 1). Out of the 3,682 patients, 827 patients (22.5%) had a preMDD, and 977 patients (26.5%) had a postoperative mood disorder diagnosis. The distribution of diagnosis by surgical procedure is presented in Table 2 .
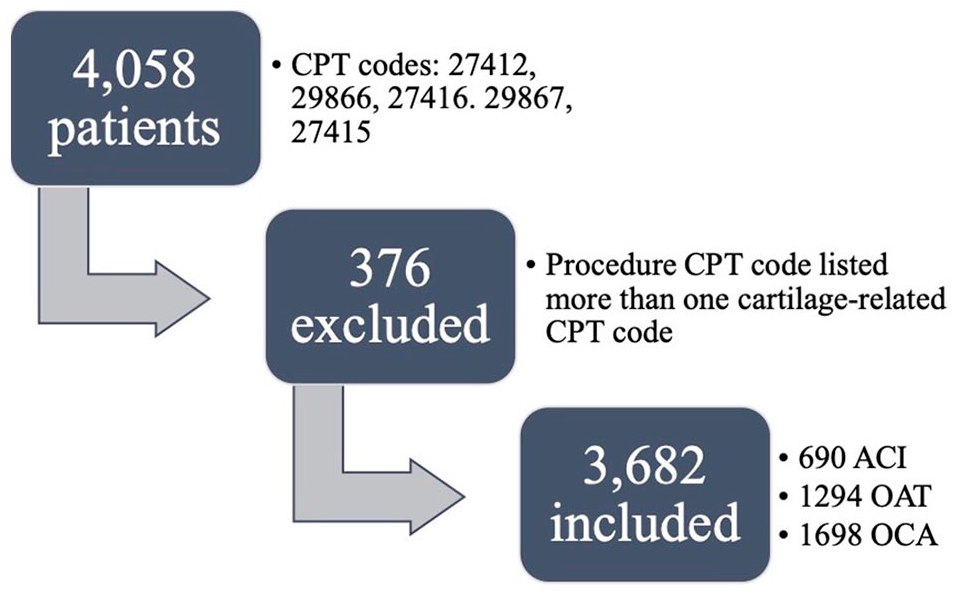
Claims patient flow chart. CPT = current procedural terminology; ACI = autologous chondrocyte implantation; OAT = osteochondral autograft transplantation; OCA = osteochondral allograft transplantation.
Frequency of Mood Disorder Diagnosis by Surgical Procedure.
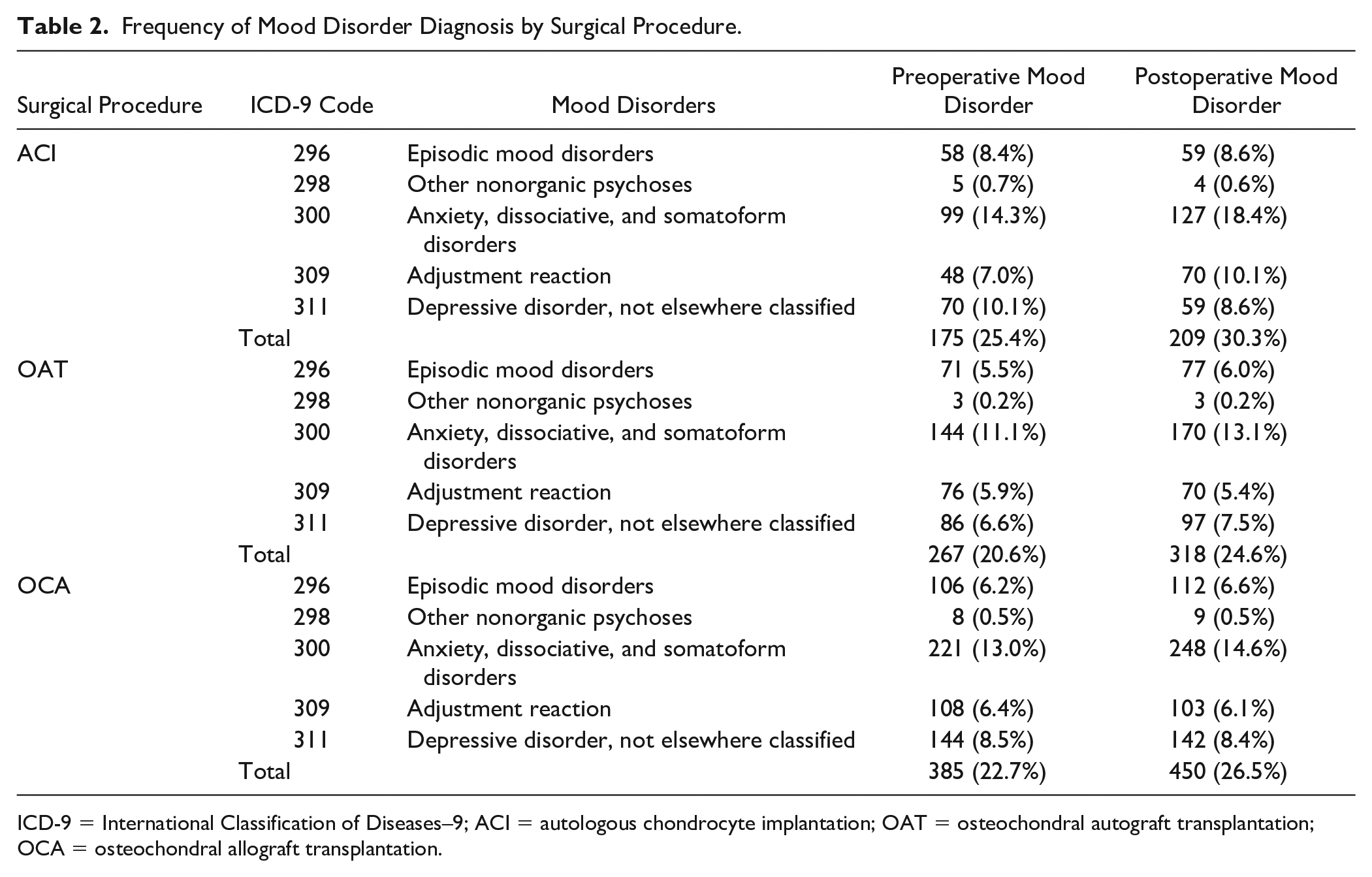
ICD-9 = International Classification of Diseases–9; ACI = autologous chondrocyte implantation; OAT = osteochondral autograft transplantation; OCA = osteochondral allograft transplantation.
ACI
A total of 690 patients who underwent ACI were analyzed. The median costs in the year prior to an ACI was $10,342, interquartile range (IQR) = $5,983 to $16,443, and 175 patients (25.4%) had a preoperative diagnosis of a mood disorder. The costs in the year prior to an ACI were significantly greater for those with a mood disorder (median $12,564, IQR = $6,969-$21,424) than those without (median $9,471, IQR = $5,498-$14,485) (t = 4.98, P < 0.0001). The prevalence of diagnoses of a mood disorder increased postoperatively to 30.3% (n = 209 patients). First postoperative year costs were significantly greater for those with a mood disorder (median $8,495, IQR = $3,972-$18,574) than those without (median $5,784, IQR = $2,758-$11,145) (t = 2.54, P = 0.006). Opioid use was significantly greater for patients with mood disorders than those without ( Table 3 ) (11.8% more preoperatively and 7.5% more >90 days postoperative). In addition, patients with mood disorders had statistically higher odds of opioid usage preoperative (OR = 1.66, 95% CI = 1.17-2.37, P < 0.01) but not postoperatively (OR = 1.41, 95% CI = 0.99-2.07, P = 0.06). First-year postoperative health care costs for patients with a preoperative mood disorder was not significantly greater (6.2% increase, P = 0.654) than those without mood disorders, after adjusting for preoperative cost, sex, age, and opioid usage.
Demographic Characteristics and Opioid Usage Between Patients Undergoing ACI with and without Preoperative Mood Disorders.
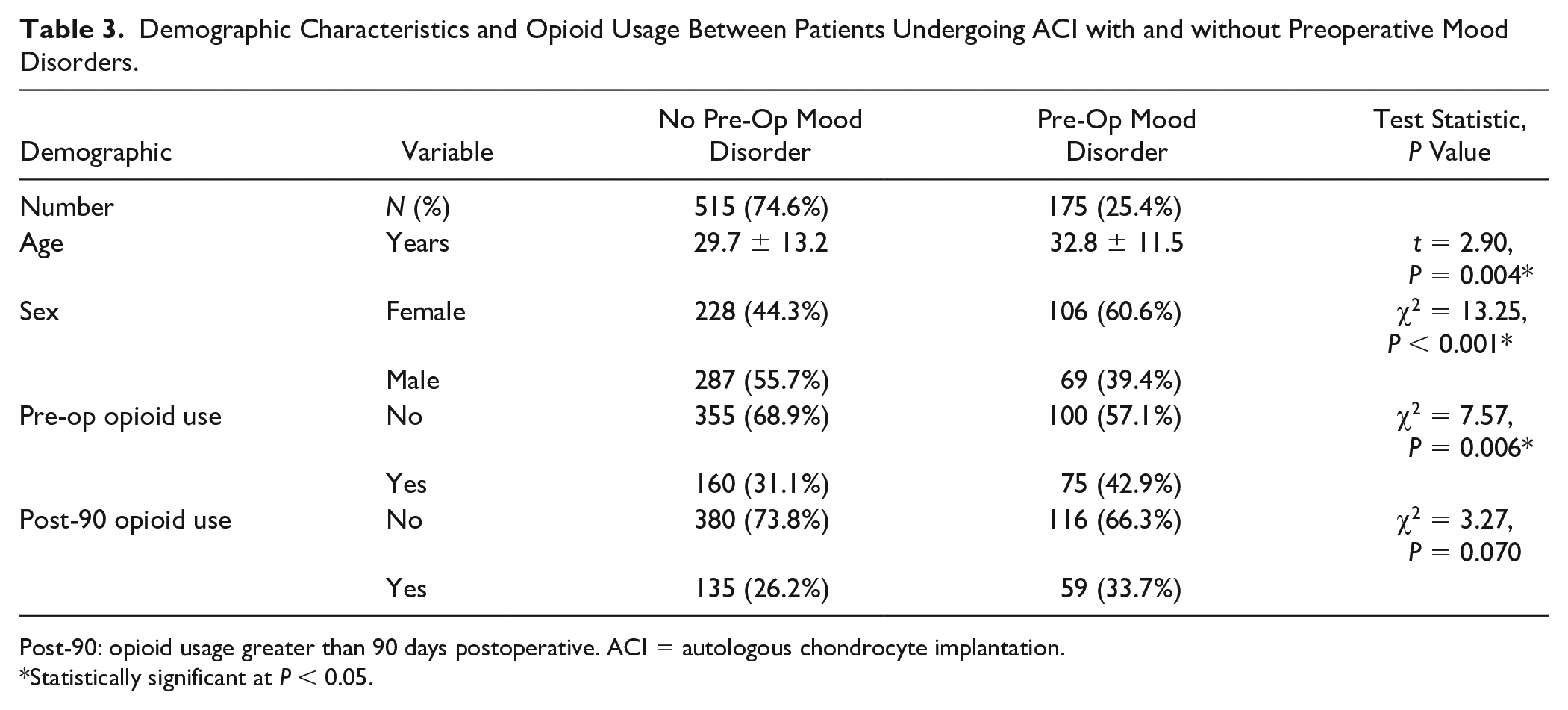
Post-90: opioid usage greater than 90 days postoperative. ACI = autologous chondrocyte implantation.
Statistically significant at P < 0.05.
OAT
A total of 1,294 patients underwent OAT procedures, and 267 patients (20.6%) had a preoperative mood disorders diagnosis. The median costs in the year prior to an OAT procedure was $3,578 (IQR = $1,912-$8,245). The costs in the year prior to OATs were significantly greater for those with a mood disorder (median = $6,156, IQR = $3,281-$12,110) than those without (median = $3,174, IQR = $1,733-$7,072) (t = 8.73, P < 0.001). The prevalence of a mood disorder diagnosis increased postoperatively to 318 patients (24.6%). First postoperative year costs were significantly greater for those with a mood disorder (median = $5,221, IQR = $2,490-$11,908) than those without (median = $3,823, IQR = $1,791-$8,011) (t = 5.05, P < 0.001). Opioid use was significantly greater for patients with mood disorders than those without mood disorders ( Table 4 ) (10.7% more preoperatively and 13% more >90 days postoperative). Patients with mood disorders had higher odds of opioid usage both preoperative (OR = 1.79, 95% CI = 1.32-2.43, P < 0.01) and postoperative (OR = 1.86, 95% CI = 1.40-2.48, P < 0.01). First-year postoperative health care costs for patients with preoperative mood disorders was 28.0% greater than those without mood disorders, after adjusting for preoperative cost, sex, age, and opioid usage (P = 0.034).
Demographic Characteristics and Opioid Usage in Patients Undergoing OATs with and without Preoperative Mood Disorders.
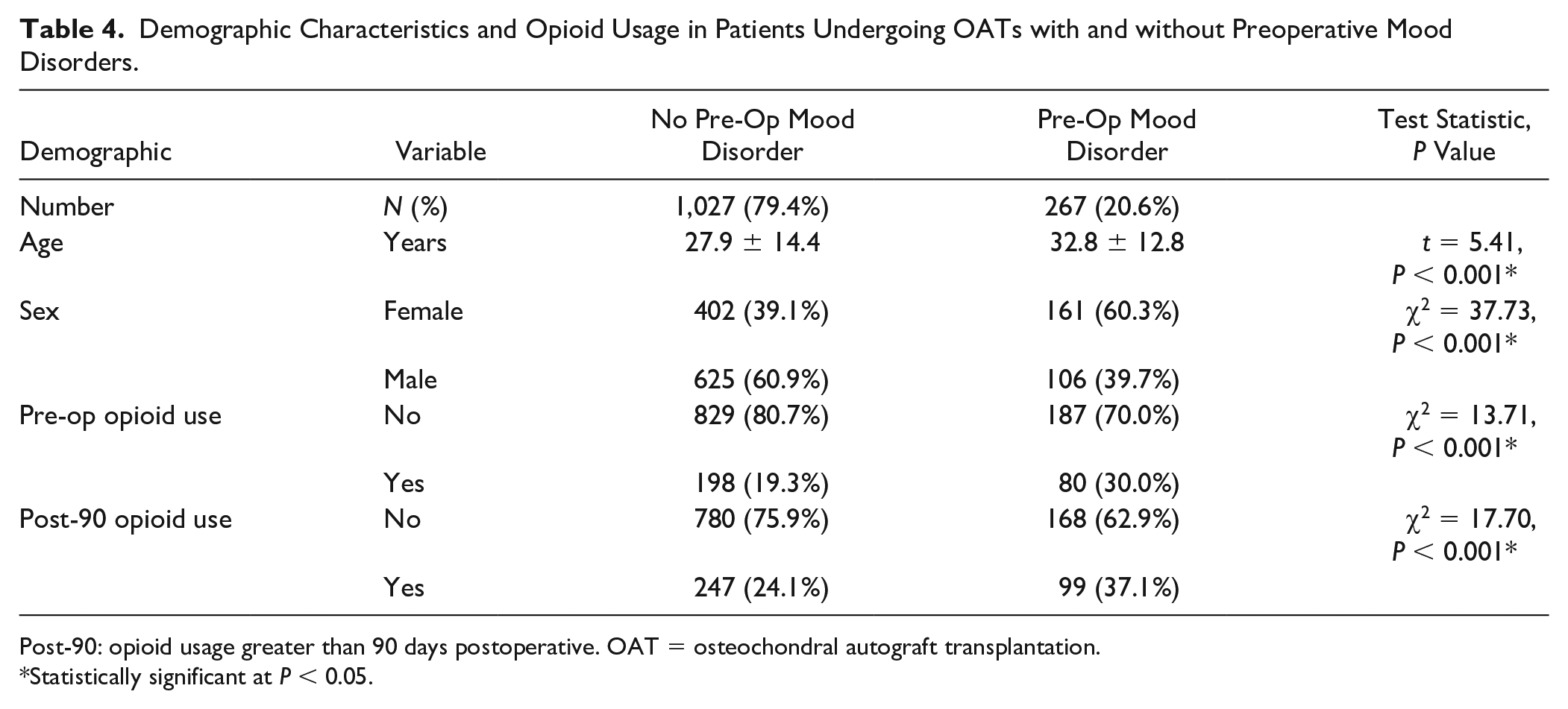
Post-90: opioid usage greater than 90 days postoperative. OAT = osteochondral autograft transplantation.
Statistically significant at P < 0.05.
OCA
Of the 1,698 patients who underwent an OCA procedure, 385 patients (22.7%) had a preoperative mood disorders diagnosis. The median costs in the year prior to an OCA was $5,432, IQR = $2,471 to $10,954. The costs in the year prior to an OCA procedure were significantly greater for those with a mood disorder (median = $8,656, IQR = $4,700-$15,459) than those without (median = $4,495, IQR = $2,160-$9,349) (t = 10.14, P < 0.001). The prevalence of a mood disorder diagnosis increased postoperatively to 450 patients (26.5%). First postoperative year costs were significantly greater for those with a mood disorder (median = $6,973, IQR = $3,104-$15,705) than those without mood disorders (median = $3,992, IQR = $1,952-$8,917) (t = 5.85, P < 0.001). Opioid use was significantly greater for patients with mood disorders than those without ( Table 5 ) (4.9% more preoperatively and 5.6% more >90 days postoperative). Patients with mood disorders had higher odds of opioid usage both preoperative (OR = 1.29, 95% CI = 1.00-1.66, P = 0.05) and postoperative (OR = 1.33, 95% CI = 1.03-1.71, P = 0.03). First-year postoperative health care cost for those with preoperative mood disorders was 41.7% greater than those without mood disorders, after adjusting for preoperative cost, sex, age, and opioid usage (P < 0.001).
Demographic Characteristics and Opioid Usage in Patients Undergoing OCA with and without Preoperative Mood Disorders.
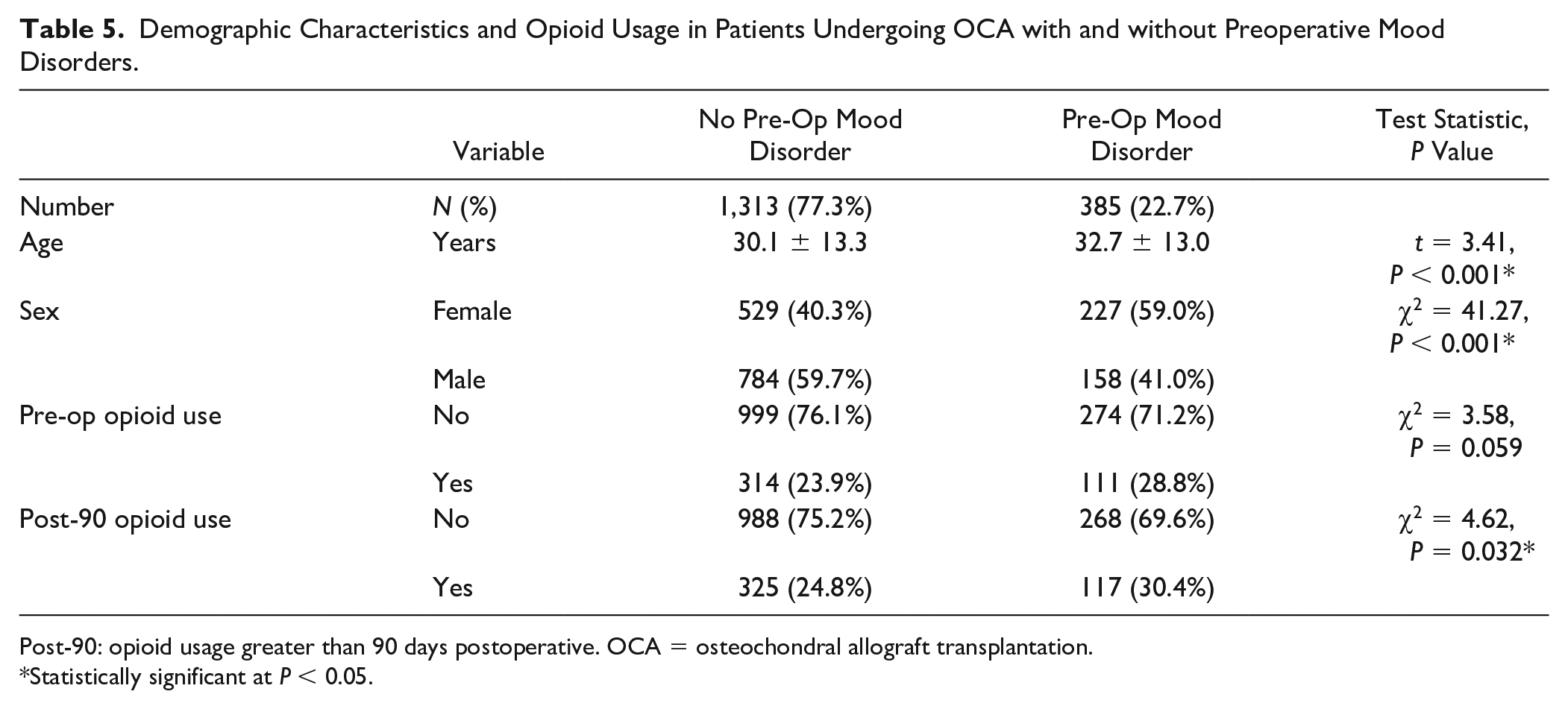
Post-90: opioid usage greater than 90 days postoperative. OCA = osteochondral allograft transplantation.
Statistically significant at P < 0.05.
Discussion
The principal finding of this study is that many patients with mood disorders have greater pre- and postoperative opioid use and health care costs with cartilage transplantation procedures than those without mood disorders. Comorbid mood disorders were associated with greater postoperative opioid use that was persistent at a minimum 90 days after surgery in patients treated with OATs or OCA. Although this finding cannot be solely attributed to the presence of a mood disorder, our study suggests that those patients with mood disorders are more likely to have greater than 90 days of opioid use postoperatively. An important secondary finding is that the prevalence of preoperative and postoperative mood disorders for cartilage transplantation procedures (22.5% and 26.5%, respectively) is greater than the prevalence of mood disorders among the general U.S. adult population (19%). 33
Health care professionals are under significant scrutiny to contain health care associated costs. Cost containment is difficult to achieve without an underlying understanding of factors contributing to increased cost. Thus, it is imperative to understand potentially modifiable risk factors for greater cost and inferior outcomes. Treatable comorbid conditions like mood disorders, hypertension, smoking, heart disease, and so on have been found to be associated with postoperative pain, opioid usage, lower patient-reported outcomes, cartilage graft failure, and postsurgical complications.14,16,17,34-36 Our analysis identified that comorbid mood disorders result in significantly greater health care costs both pre- and postoperatively. After controlling for all covariates, these costs remained significantly greater for both OAT and OCA procedures. The costs were still greater for patients with mood disorders receiving ACI; however, the greater expense of ACI procedure itself is likely responsible for the loss of significance when controlling for all covariates. The reasons are likely multifactorial as a result of increased treatment costs for mental health visits and increased resource utilization during the recovery period.
Patients with mood disorders are known to be at greater risk for postoperative pain and decreased outcomes. This trend is seen across orthopedic subspecialties.3,6,8,10,11,14,17,37,38 Preoperative depression predicts long-term opioid use better than postoperative pain severity. 13 The reasons behind the association between heightened pain response and mood disorders are not well understood, but are theorized to be related to pain-catastrophizing. 39 Mental health comorbidities are known to be a risk factor for knee pain.39,40 While the patients included in this study had an identifiable and surgically treatable source of knee pain, it is possible that the pain threshold could be lowered by comorbid mental health disease thereby leading to prolonged utilization of opioids.
The preoperative prevalence of mental health diagnosis in patients undergoing articular cartilage procedures is notable. The prevalence of mood disorder diagnoses in our study is comparable with those reported preoperative in the FAIS population (40%) and postoperative in those with acute orthopedic trauma (32.6%).3,41 In the FAIS population, mood disorders are associated with decreased function/return to activity and development of chronic pain.8,42 These trends in the prevalence of mood disorders are particularly challenging, as mood disorders also correlate with difficulty in achieving the minimal clinically important differences (MCID) on patient-reported outcomes and return to function and sport following anterior cruciate ligament reconstruction.37,38 To increase the likelihood of successful outcomes and reduce opioid use and the health care cost burden, surgeons should be cognizant of diagnosed or suspected mood disorders to refer for preoperative treatment. This may be achieved by reviewing the medical chart for in some electronic medical record systems, a depression/anxiety screening is provided to the patient when registering for the appointment. If this resource is not available to a surgeon, a quick 4-item depression/anxiety screening questionnaire such as the Patient Health Questionnaires (PHQ-4) could be administered to the patient during the appointment.43,44
Given the prevalence and risk of chronic pain in those with preoperative mental health comorbidities treated for cartilage and labral lesions of the hip,3,8 similar pathologic relationships may be present in knee cartilage patients. The alarmingly high rate of persistent opioid usage at minimum 3 months postoperative in this knee cartilage surgery population would suggest that these patients are at a high risk for persistent symptoms. 45 Overall, the odds of opioid usage were 30% to 86% greater in patients with a mood disorder. The odds of preoperative use was greater for patients with mood disorders in all surgical procedures. Postoperatively, the odds of opioid usage increased for patients undergoing either an OAT or OCA. The increased odds are notable and something for clinicians to be mindful when treating patients. We cannot determine if the reason for prolonged opioid use is the result of the underlying condition that precipitated the index surgery, or if the reason for prolonged opioid use was a result of the recovery process and challenges resulting from comorbid mood disorders. Further prospective studies are needed to better assess the interplay of preoperative factors and long-term opioid usage.
Preoperative management of comorbid mood disorders represents a viable target for potential cost savings and reduction in opioid use. Flanigan et al. 1 suggests that in patients clinical suspicion for untreated depression or any patient scoring >20 on the Center for Epidemiologic Studies Depression Scale (CES-D) is a relative contraindication for elective orthopedic surgery. 46 The authors suggest delaying surgery until a mental health provider addresses these concerns. In addition, Flanigan et al. 1 states that for a patient who does not meet the preoperative relative contraindication criteria requiring delay of surgery but may benefit from mental health treatment, they suggest using treatment end points which may be in the form of communication from the treating mental health provider, objective evidence such as physical therapy attendance records, or patient self-reported goal setting before continuing with an operative procedure. Our study as well as those identifying the effects of psychologic disorders on orthopedic outcomes support the belief that preoperative assessments should include a mental health screening. While most surgeons include subjective mental health assessments when determining patients to be appropriate for elective procedures, an objective screening would be standardized for all patients with improved accuracy and lessen the risk of bias. Studies determining the most accurate tool to assess mood disorders in patients with osteochondral defects as candidates for surgery are needed.
Our study carries common limitations of analyses of large administrative claims databases. A primary limitation is that initial coding errors may have occurred which can over- or underestimate the number of mood disorder diagnoses. To mitigate this risk, we examined the year prior to surgery for a mental health diagnosis to better capture mental health diagnoses. Patients were not stratified to contain other diagnoses of comorbid conditions in those determined to have mood disorders, which is likely to affect health care utilization costs and potentially opioid usage found in this study. Patient outcomes are not recorded, and the severity of the documented diseases are not available. Patients were included with binary criterion of a diagnosis of mood disorder identified by ICD-9 codes, and there may be patients with clinical depression or symptoms of anxiety undiagnosed prior to surgery. Even if the patient did carry a mood disorder diagnosis, the data do not indicate the personal effects of the disease, and patients may not be receiving treatment during the study period. For example, 2 patients may have the same mood disorder diagnosis and 1 patient may be more negatively affected which can affect outcomes and health care utilization. Patients may have received treatment for a mood disorder prior to surgery and no longer experience symptoms but continue to carry the labeled diagnosis in the chart records. Despite these limitations, the primary purpose of the study was to report the epidemiology of mood disorders in cartilage patients and the respective health care costs surrounding the cartilage intervention which was accomplished. The Truven database may not be representative of individuals with other insurance plans that are not included in this dataset. Our results may not be generalizable to uninsured or underinsured patients; however, the database is comprised of claims reported by many employers, which adds to the diversity and potential generalizability of the dataset.
In conclusion, there is a high prevalence of preoperative mood disorders for patients undergoing cartilage transplantation procedures. Modifiable risk factors should be optimized to reduce postoperative cost and opioid usage, as cartilage transplantation patients with mood disorders had greater pre- and postoperative health care costs and opioid use than those without mood disorders. To improve positive outcomes and avoid prolonged use of highly addictive medications in these patients while attempting to minimize the health care burden, mood disorders should be addressed and optimized preoperatively when possible, but these results also highlight the potential need for postoperative screening. Future research is needed on the effectiveness of preoperative screening and if the results from the screening materialize into referrals or care recommendations for patients undergoing knee cartilage restoration procedures. Our results support the need for a strategy to prepare patients with mood disorders for the potential challenges of a cartilage restoration surgery and an emphasis on multidisciplinary perioperative clinical care pathways that incorporate both rehabilitation exercises and aspects of psychosocial health that can maximize function and minimize pain.
Footnotes
Author Contributions
The work was completed between the University of Kentucky and Brigham and Women’s Hospital Department of Orthopedic Surgery.
Author individual contributions outlined below:
Acknowledgments and Funding
This project was not funded. However, the data used for the project was made possible through the University of Kentucky’s Clinical and Translational Science Center, which is supported by the NIH National Center for Advancing Translational Sciences (grant numbers UL1TR001998 and UL1TR000117). The content is solely the authors’ responsibility and does not necessarily represent the official views of the NIH.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Austin Stone has no conflict of interest related to the current study, but does report an unpaid relationship with AlloSource Inc and Smith & Nephew, research support from Flexion Therapeutics and AlloSource, and board membership for American Orthopaedic Society for Sports Medicine and Arthroscopy Association of North America. Cale Jacobs has no conflict of interest related to the current study, but does report being a paid consultant for Flexion Therapeutic, and research support from Flexion Therapeutics and Smith & Nephew, and editorial board membership for Journal of Sports Rehabilitation. Christian Lattermann has no conflict of interest related to the current study, but does report being a paid consultant for Joint Restoration Foundation, Samumed, and Vericel; being a member of the editorial board for Cartilage, Journal of Sports Physiology, The Knee, and Orthopaedic Journal of Sports Medicine; and board membership for the German Speaking Arthroscopy Society (ACA) and the International Cartilage Regeneration and Joint Preservation Society. Caitlin Conley has no conflict of interest related to the current study, but does report research support from Flexion Therapeutics and a relationship with the International Cartilage Regeneration and Joint Preservation Society’s Patient Registry.
Ethical Approval
The University of Kentucky’s IRB has approved the use of the de-identified Truven Health Copyright© 2012 Truven Health Analytics Inc to researchers utilizing only data from the claims data database.