
Abstract
Objective
The purpose of this systematic review was to determine (1) treatment options for bipolar cartilage lesions of the knee, (2) patient-reported outcomes following various surgical treatments, and (3) complication and failure rates following surgery.
Design
A literature search of PubMed, the Cochrane Library, and CINHAL was performed using PRISMA guidelines. Patients were included if they had bipolar cartilage lesions of the knee treated surgically. Lesion characteristics, surgical technique, patient-reported outcomes, complication rates, failure rates, and survivorship were recorded.
Results
Fourteen studies yielded 301 knees treated surgically. Patient age ranged from 15 to 74 years. Surgical techniques included 138 autologous chondrocyte implantation (ACI), 156 osteochondral allograft transplantation (OCA), and 7 osteochondral autograft transfer system (OATS). Seven studies reported a concomitant procedure rate that ranged from 0% to 88%. Eight studies reported that both reciprocal lesions received surgical treatment, while 6 studies did not specify. Lesion size ranged from 1 to 41 cm2. All reported postoperative improvements in patient-reported outcomes, but the measures were very heterogeneous. There were no major complications and the rate of minor complications ranged from 0% to 50%. Survivorship ranged from 40% to 100% for OCA, 76% to 95% for ACI, and 100% for the 1 study evaluating OATS.
Conclusions
Bipolar cartilage lesions of the knee typically involve a large surface area and are most commonly treated with ACI or OCA, while OATS may be an option for smaller lesions. Improvements in mid-term patient-reported outcomes were reported for all surgical procedures and they can be performed safely with a low rate of major complications.
Keywords
Introduction
Cartilage lesions involving the knee have proven difficult to treat. 1 Unfortunately, they are becoming more common in the active population and can lead to significant morbidity. 2 Because of this, a variety of surgical techniques have been developed. 3 For isolated femoral lesions larger than 2 cm2, autologous chondrocyte implantation (ACI) and osteochondral allograft transplantation (OCA) have produced good results.3,4 Osteochondral autograft transfer system (OATS) is ideal for smaller lesions where donor site morbidity is minimal.3,5,6 Microfracture has produced variable outcomes. 3 Chondral defects involving the proximal tibia and patella are even more difficult to treat, especially in the setting of a reciprocal femoral lesion.7,8 These bipolar lesions have led to inferior outcomes and a higher failure rate following surgical treatment when compared to simple, unipolar injuries.7,9
No obvious, evidence-based treatment algorithm for bipolar cartilage lesions of knee exists. It is unknown whether treatment of both reciprocal lesions or treatment of only one surface lesion is sufficient. 10 Hannon et al 4 demonstrated similarly improved results for bipolar chondral defects involving the tibiofemoral compartment when the femoral defect was treated with OCA and the tibial defect was treated with either microfracture or debridement. Furthermore, these patients were matched to a cohort of patients with isolated femoral defects treated with OCA and equivalent outcomes were observed. OCA for both the tibial and femoral reciprocal lesions has produced highly variable success rates.8,11 Mirzayan et al 12 reported good outcomes following OCA for reciprocal lesions involving the patellofemoral compartment at mid-term follow up, but other results have not been as promising.8,13,14 Additionally, postoperative improvements have been reported following ACI for bipolar defects involving both the tibiofemoral and patellofemoral compartments.15-20 OATS is generally considered to be contraindicated for larger bipolar lesions due to donor site limitations, but it has been described.17,21,22
Although it is currently unknown what treatment option is best for these bipolar cartilage injuries in the knee; it is well established that these lesions naturally progress to arthritis if left treated.23,24 Given the significant impact of this problem, a better understanding of the treatment options is desired. Accordingly, the purposes of this systematic review were to determine (1) treatment options for bipolar chondral lesions of the knee, (2) patient-reported outcomes following various surgical treatments, and (3) complication and failure rates following surgery.
Methods
Literature Search
A comprehensive search was performed on October 30, 2018 of the available literature following the guidelines provided by Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) ( Fig. 1 ). Multiple databases were searched, including PubMed (MEDLINE), the Cochrane Central Register of Controlled Trials & Cochrane Library, and CINHAL (Cumulative Index for Nursing and Allied Health Literature) and the search period parameters were set from January 1, 1990 to October 30, 2018. A Boolean search was performed utilizing the following terms: ((bipolar lesion OR bipolar lesions OR kissing lesion OR kissing lesions OR patellofemoral allograft OR patellofemoral autograft OR tibiofemoral allograft OR tibiofemoral autograft) AND (knee OR patellofemoral OR tibiofemoral)) and articles were catalogued using Microsoft Excel (2010; Microsoft Corp, Redmond, WA). This initial search resulted in 330 articles from PubMed, 3 articles from CINAHL, and 27 articles from the Cochrane Library. The reference list of articles was reviewed for any articles that may have been missed from the initial search and an additional 7 articles were included. After removal of duplicates, 363 articles underwent further screening for inclusion in this study.
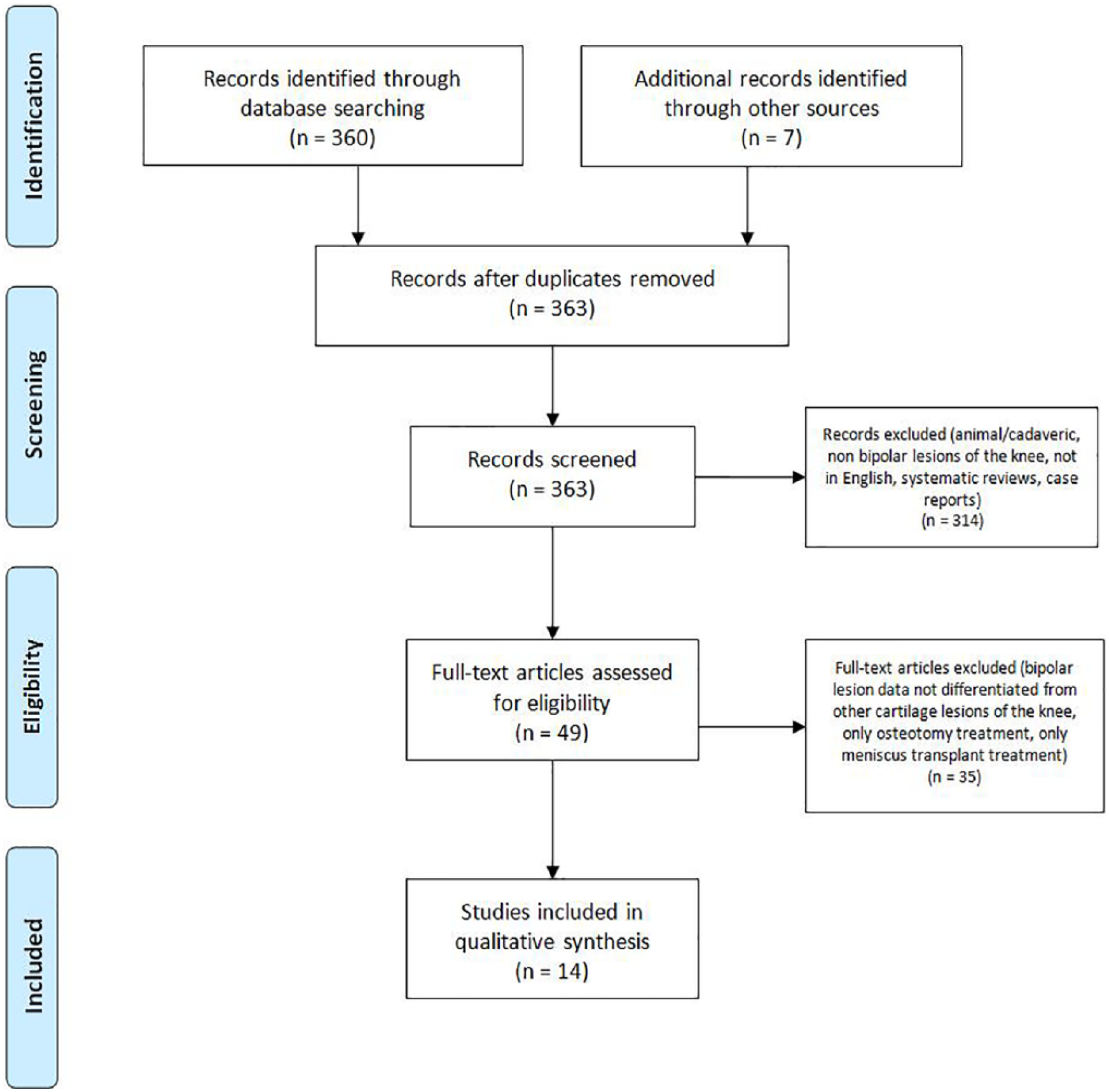
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) flow diagram demonstrating the study selection process.
Selection Criteria
Titles and abstracts of these 363 studies identified via the search criteria were independently reviewed by 2 authors (CDB, HPM) and only studies eliminated in consensus were removed from the list. Systematic reviews, case reports, cadaveric and animal studies, studies not involving the knee and studies with unavailable full English texts were removed.
Inclusion criteria utilized for the evaluation of the remaining full-text articles were as follows: a confirmed series or cohort of patients with a bipolar cartilage lesion of tibiofemoral or patellofemoral joint, operative treatment of the lesion and documented survivorship, patient reported, clinical, functional, and/or radiographic outcome measures. Exclusion criteria included systematic reviews, case reports, cadaveric and animal studies, studies not involving bipolar lesions of the patellofemoral or tibiofemoral joint, studies with unavailable full English texts, and isolated osteotomy procedure or isolated meniscus transplant procedure without a cartilage restoration procedure being performed.
Several studies contained cohorts of patients that included isolated cartilage lesions of the knee as well as multifocal cartilage lesions of the knee. Only studies containing patients that explicitly fulfilled the inclusion/exclusion criteria were reported in our analysis. If a study presented a table that provided individual patient demographics, surgical treatment, and outcomes that differentiated patients with bipolar lesions from the rest of the patients in the study, those individual patients were included for analysis. If distinguishing between patient cohorts in a study was not possible and a table or comment with each individual patient’s data was not provided in the study, then it was excluded. An attempt was made to contact the corresponding author in one study to obtain the differentiated information, but this was not successful.
Quality Assessment
Since there were no randomized controlled trials identified throughout the search that met inclusion criteria, each study was assessed for bias using the methodologic index for nonrandomized studies (MINORS) scoring system. MINORS is a validated tool designed for assessing the quality of nonrandomized surgical studies based on a scoring scale from 0 to 16 or 0 to 24 depending on the type of study. For noncomparative studies, a maximum score of 16 can be achieved as there is an 8-item checklist with each item being scored from 0 to 2. For comparative studies a maximum score of 24 can be achieved as there is a 12-item checklist with each item being scored from 0 to 2. Higher scores indicate a lower level of bias. Each study was independently reviewed and scored by 2 authors (CDB and HPM) with any disagreements being resolved by consensus discussion. MINORS score results of each study ( Table 1 ) are presented as a percentage score to allow for normalization between comparative and noncomparative studies. Level of evidence was determined by utilizing the criteria presented in the Oxford Centre for Evidence-Based Medicine.
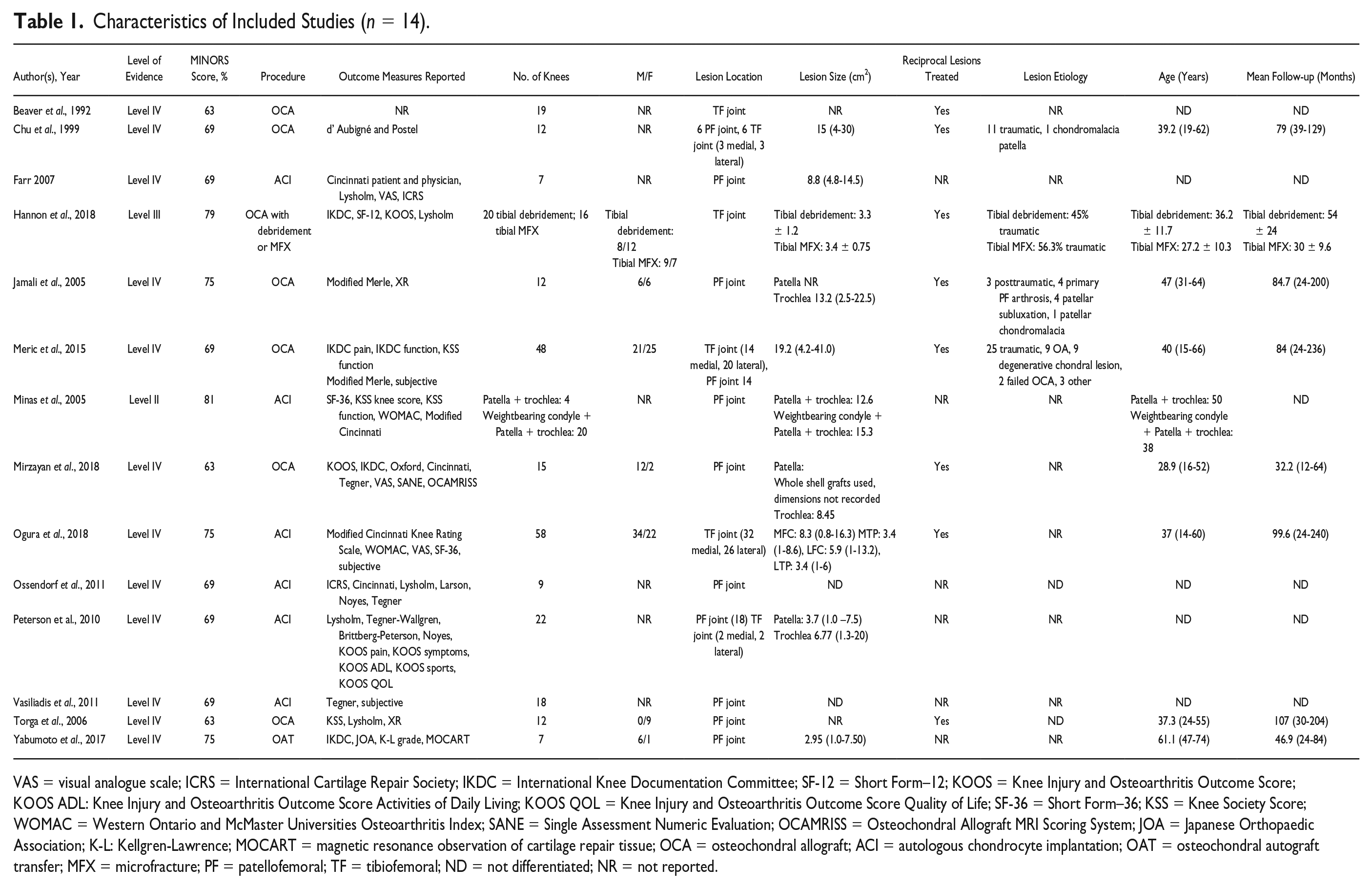
Characteristics of Included Studies (n = 14).
VAS = visual analogue scale; ICRS = International Cartilage Repair Society; IKDC = International Knee Documentation Committee; SF-12 = Short Form–12; KOOS = Knee Injury and Osteoarthritis Outcome Score; KOOS ADL: Knee Injury and Osteoarthritis Outcome Score Activities of Daily Living; KOOS QOL = Knee Injury and Osteoarthritis Outcome Score Quality of Life; SF-36 = Short Form–36; KSS = Knee Society Score; WOMAC = Western Ontario and McMaster Universities Osteoarthritis Index; SANE = Single Assessment Numeric Evaluation; OCAMRISS = Osteochondral Allograft MRI Scoring System; JOA = Japanese Orthopaedic Association; K-L: Kellgren-Lawrence; MOCART = magnetic resonance observation of cartilage repair tissue; OCA = osteochondral allograft; ACI = autologous chondrocyte implantation; OAT = osteochondral autograft transfer; MFX = microfracture; PF = patellofemoral; TF = tibiofemoral; ND = not differentiated; NR = not reported.
Data Extraction and Analysis
The data extracted from each study that met final selection criteria included study properties (year, level of evidence, number of knees), patient demographics (age, lesion etiology, lesion location, lesion size, whether or not both lesions was treated, follow-up period), surgical procedure, concomitant procedures, outcomes (patient-reported, functional, clinical, radiographic), complications, failures, survivorship, and reoperations. As there were an inadequate number of comparative studies and reported outcomes were heterogeneous, pooling of results was not performed and instead ranges were reported. In studies with cohorts of both bipolar cartilage lesions of the knee and other cartilage lesions of the knee, only patients with bipolar cartilage lesions of the knee were included in our analysis and any data that utilized a combination of those cohorts was excluded. Forrest plots were created in JMP Pro, and 95% confidence intervals were calculated for binomial outcomes according to the adjusted Wald method.
Results
Forty-nine full texts were manually reviewed for inclusion. Ultimately, 14 studies were included and analyzed for this systematic review. Study characteristics are reported in Table 1 . MINORS scores ranged from 63% to 81%. Twelve studies were classified as level of evidence IV, 1 was classified as level III, and another was classified as level II. The 14 studies evaluated 301 knees with bipolar knee cartilage lesions that were surgically treated. Patient age ranged from 15 to 74 years. A variety of surgical techniques were utilized, including 156 treated with OCA, 138 treated with ACI, and 7 treated with OATS.
Surgical Treatments and Indications
Lesion etiology and chosen surgical treatments are reported in Table 1 . OCA and ACI were the most commonly studied techniques, with 7 studies (n = 156 knees) for OCA and 6 studies (n = 138 knees) for ACI. Six of the 7 studies for OCA involved bulk allografts. Seven studies documented whether concomitant procedures were performed. One study reported none and the other 6 reported a rate of 33% to 88% in their patients ( Table 3 ). The specific concomitant procedures included: meniscus transplant, anterior cruciate ligament reconstruction, anteromedialization, distal fibular osteotomy, posterolateral corner reconstruction, retinacular release, high tibial osteotomy, distal femoral osteotomy, tibial tubercle osteotomy, and medial patellofemoral ligament reconstruction. Eight of 14 studies reported that both reciprocal lesions were treated with OCA, ACI, or OATS ( Table 1 ). The remaining studies did not specify if both reciprocal lesions were treated.
Patient-Reported Outcomes
The patient-reported outcome measures were very heterogeneous as shown in Table 2 . Postoperatively, all studies reported improvements in subjective scores. Follow-up ranged from 12 to 240 months. Four studies evaluating OCA or ACI reported mean postoperative improvements in KSS function scores ( Fig. 2 ).
Reported Outcome Scores, Imaging, and Arthroscopy.
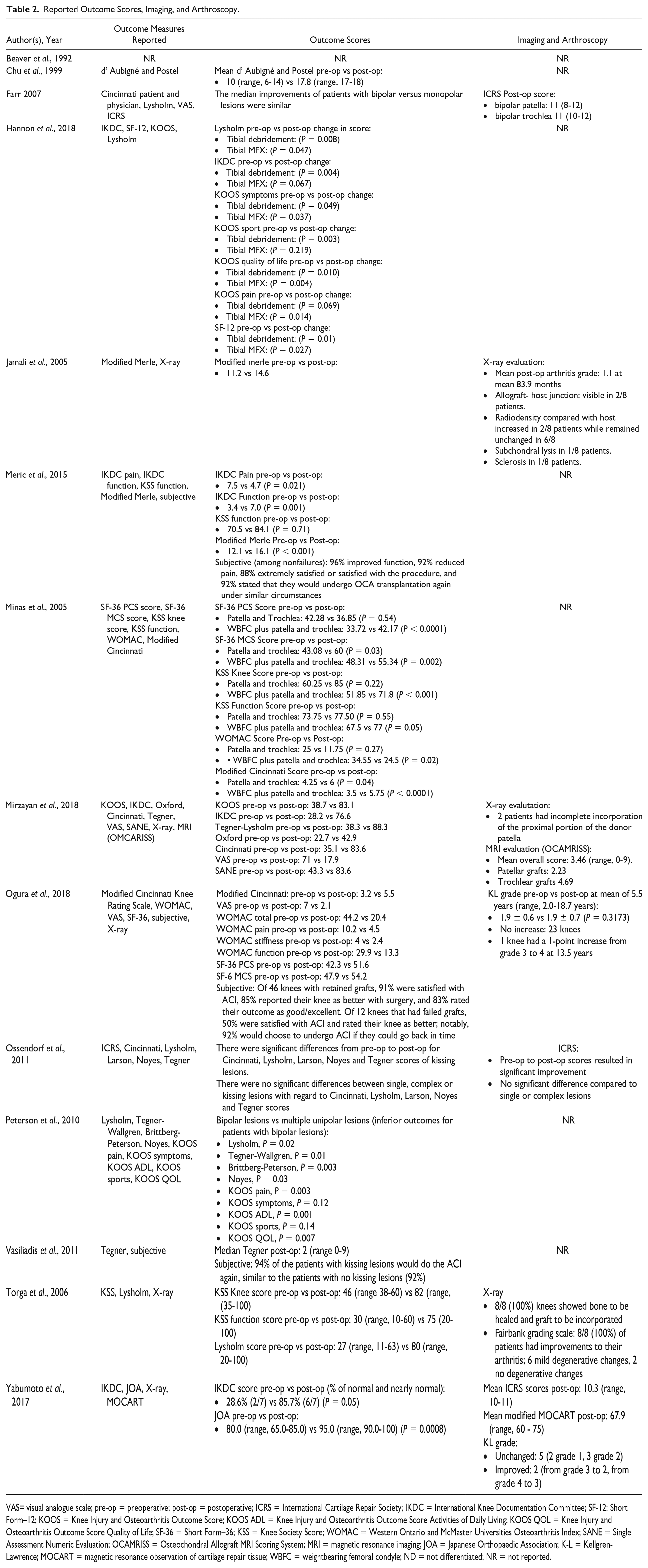
VAS= visual analogue scale; pre-op = preoperative; post-op = postoperative; ICRS = International Cartilage Repair Society; IKDC = International Knee Documentation Committee; SF-12: Short Form–12; KOOS = Knee Injury and Osteoarthritis Outcome Score; KOOS ADL = Knee Injury and Osteoarthritis Outcome Score Activities of Daily Living; KOOS QOL = Knee Injury and Osteoarthritis Outcome Score Quality of Life; SF-36 = Short Form–36; KSS = Knee Society Score; WOMAC = Western Ontario and McMaster Universities Osteoarthritis Index; SANE = Single Assessment Numeric Evaluation; OCAMRISS = Osteochondral Allograft MRI Scoring System; MRI = magnetic resonance imaging; JOA = Japanese Orthopaedic Association; K-L = Kellgren-Lawrence; MOCART = magnetic resonance observation of cartilage repair tissue; WBFC = weightbearing femoral condyle; ND = not differentiated; NR = not reported.
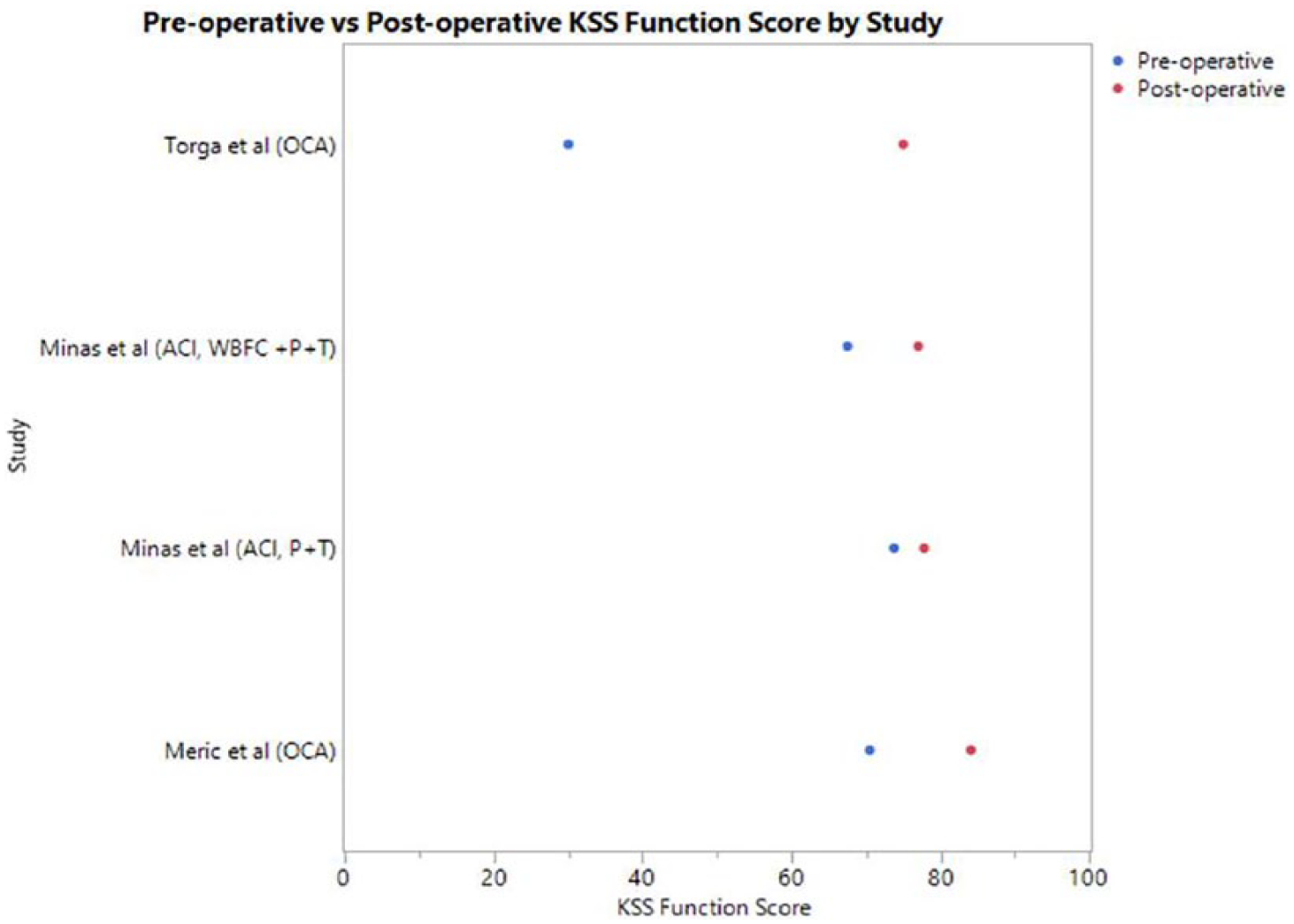
Mean pre- and postoperative Knee Society Score (KSS) function scores. WBFC = weightbearing femoral condyle; P = patella; T = trochlea.
Complications and Survivorship
No major complications were reported following any surgical treatment of bipolar knee cartilage lesions as presented in Table 3 . Nine studies reported survivorship for bipolar lesions only ( Fig. 3 ). Failure rates and survivorship for all studies are shown in Table 3 .
Complications, Reoperations, and Failures.
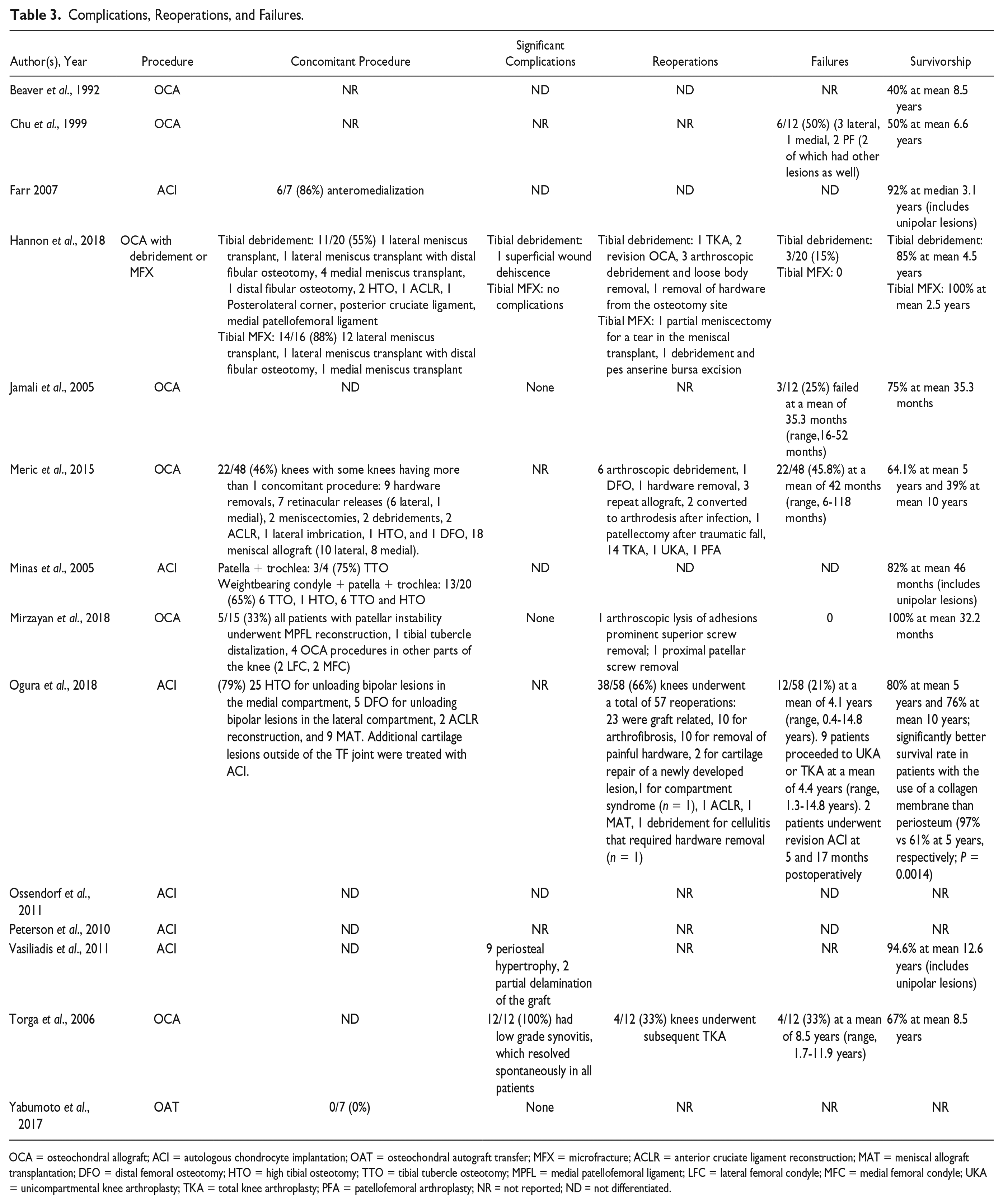
OCA = osteochondral allograft; ACI = autologous chondrocyte implantation; OAT = osteochondral autograft transfer; MFX = microfracture; ACLR = anterior cruciate ligament reconstruction; MAT = meniscal allograft transplantation; DFO = distal femoral osteotomy; HTO = high tibial osteotomy; TTO = tibial tubercle osteotomy; MPFL = medial patellofemoral ligament; LFC = lateral femoral condyle; MFC = medial femoral condyle; UKA = unicompartmental knee arthroplasty; TKA = total knee arthroplasty; PFA = patellofemoral arthroplasty; NR = not reported; ND = not differentiated.
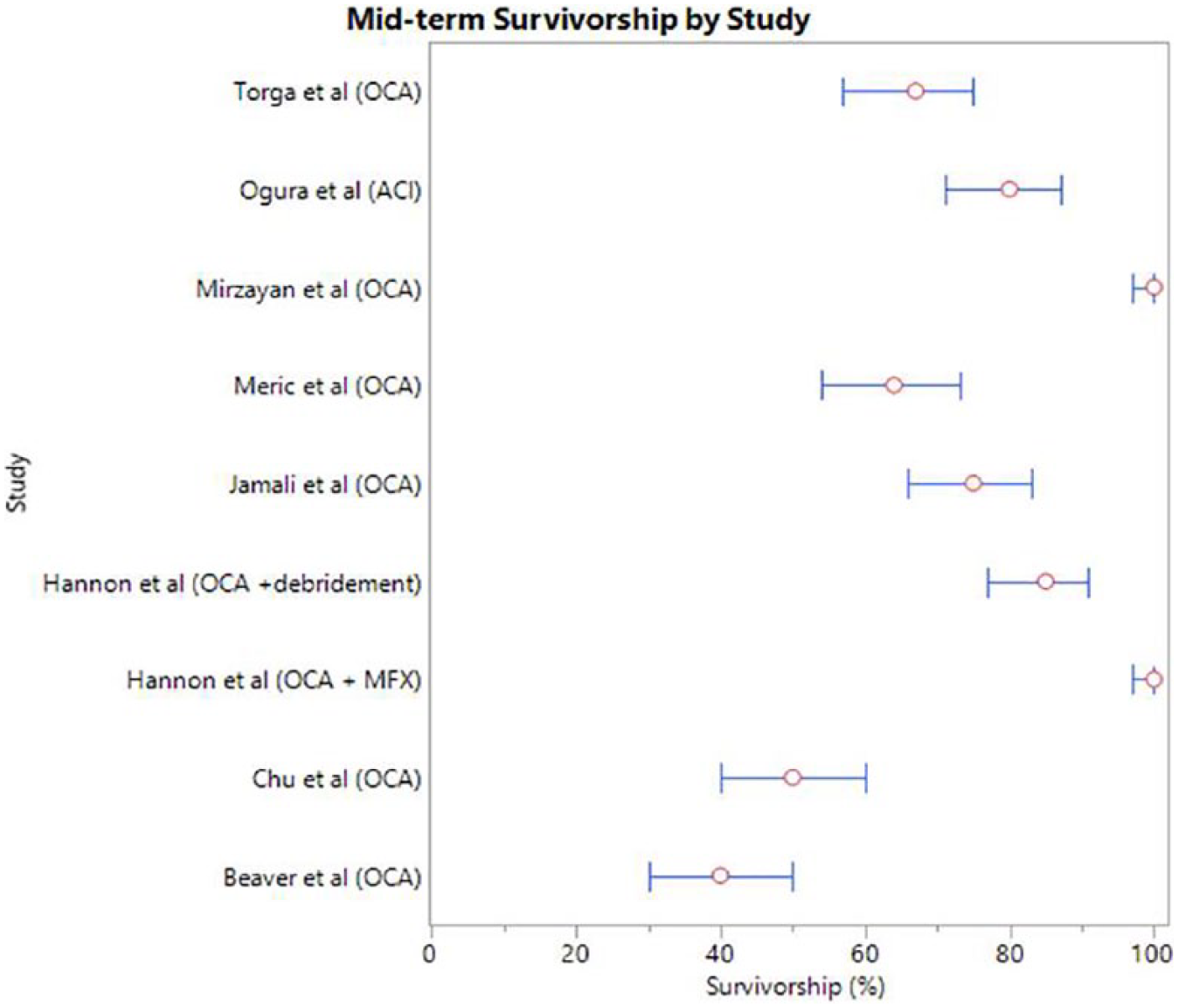
Survivorship by study at mid-term follow up for bipolar lesions. Red circles represent the survivorship of the patient cohort. The 95% confidence interval is identified by a thin blue line with bars (only includes studies that reported survivorship for bipolar lesions alone). Specific follow-up time for survivorship is provided in Table 2 . MFX = microfracture; OCA = osteochondral allograft; ACI = autologous chondrocyte implantation.
Discussion
This systematic review found that ACI and OCA are the most common procedures performed for bipolar cartilage lesions involving the knee primarily due to their large surface area. OATS was less commonly performed, but it may be a viable option for smaller lesions. Excluding failures, all procedures led to improved patient-reported outcomes. A majority of the OCA procedures involved bulk allografts, and these had a high failure rate, especially for lesions involving the tibiofemoral compartment. Although OCA has produced good results in the patellofemoral compartment, ACI or femoral OCA with a combination of tibial microfracture or debridement may be the best option in the tibiofemoral compartment.
The most common procedures performed for treatment of bipolar lesions involving the knee were ACI and OCA. This is not surprising as bipolar lesions involve more surface area and are many times larger which makes other options such as OATS relatively contraindicated. 8 One study by Yabumoto et al. 21 did evaluate OATS for bipolar lesions in the patellofemoral compartment. They report using autograft aggressively even for larger lesions. OCA was performed in 7 studies, including 156 knees, of which 61 (39%) involved the patellofemoral compartment. ACI was performed in 6 studies including 138 knees, of which 76 (55%) involved the patellofemoral compartment. Lesions treated with OCA (2.1-41 cm2) were slightly larger than those treated by ACI (0.8-20 cm2). OCA is typically indicated over ACI when the subchondral bone is involved as ACI does not replace or repair this.3,12 However, if the subchondral bone is healthy, ACI may be an attractive option since it allows preservation of the native subchondral bone. 3 There was a significant amount of concomitant procedures associated with OCA and ACI procedures, which is common in all cartilage restoration procedures to address associated pathologies such as malalignment or meniscal deficiency. 3
The studies included in this systematic review used a variety of patient-reported outcome measures to evaluate response to surgical treatment. This heterogeneity made direct comparison of different surgical treatments challenging, but all demonstrated subjective postoperative improvements at final follow up. The included studies were performed between 1992 and 2018, and the patient-reported outcome measures have changed during this time, which may have contributed to the heterogeneity. A number of studies included comparisons of patients with bipolar lesions and unipolar lesions with varied findings.4,15,16,18,20 Ossendorf et al. 16 and Farr 20 performed ACI for treatment of patellofemoral bipolar lesions and found similar improvements in postoperative subjective outcomes when compared to patients receiving treatment for unipolar lesions. On the other hand, Peterson et al. 15 and Vasiliadis et al. 18 found inferior results for bipolar lesions when compared with unipolar lesions after treatment with ACI. Hannon et al. 4 found similar results for patients with bipolar lesions treated with femoral OCA and then tibial microfracture or debridement when matched to a cohort of patients with unipolar femoral lesions treated with OCA alone. Although there is a general feeling that bipolar lesions are at an increased risk of failure and may represent a more progressed stage of osteoarthritis,12,25 the present review demonstrates that improvements can be achieved following surgical treatment for bipolar lesions as long as the graft survives.
The failure rate of OCA alone for reciprocal lesions in the tibiofemoral compartment was high. Studies by Meric et al. 8 and Beaver et al. 26 reported the longest follow-up at close to 10 years with survival rates of only 39% and 40%, respectively. This failure rate is high compared with a systematic review evaluating OCA in the knee of which the majority were unipolar lesions. 27 Three studies evaluated OCA alone in only the patellofemoral compartment and found better survival rates ranging from 57% to 100%.12-14 Mirzayan et al. 12 reported 100% survivorship at 33 months following bipolar OCA in the PF compartment in 15 knees. The low rate of failure could be partly explained by the early follow-up and high percentage of males (86%), which have been shown to have improved outcomes following cartilage procedures. 8 Overall, the survival rate of ACI appeared to be consistently higher than that of OCA alone. It should be noted though that survivorship was not reported by all studies; nor was it reported specifically for patients with bipolar lesions in each study. Ogura et al.17 reported a survival rate of 76% at 10 years status post ACI for treatment of bipolar lesions of the tibiofemoral compartment. In this study, 77% of patients underwent a concurrent osteotomy, which may have contributed to the high survival rate. They found a significantly higher survival rate for patients in which a collagen membrane cover was used in comparison to a periosteum cover. The apparent superior survivorship of ACI may be the result of multiple factors. Lesions involving the subchondral bone are more severe and require the use of OCA instead of ACI, which could contribute to their lower survival rate. Six of the 7 OCA studies involved bulk allografts, which are at an increased risk of failure compared with smaller allografts. Additionally, creeping substitution occurs during the incorporation process following OCA which can lead to bone collapse and failure. 28 In instances where the subchondral bone is normal, ACI is beneficial because it allows preservation of the healthy native bone. 3 Although the failure rate of OCA in the tibiofemoral compartment was high at long-term follow-up, it did prolong time to total knee arthroplasty and provided good function.8,11
Yabumoto et al. 21 reported 100% survival in 7 patients at minimum 2-years following OATS in the patellofemoral compartment. All patients received OATS for both reciprocal lesions on the trochlea and patella. Interestingly, the mean lesion size in their study was 2.95 cm2 with 2 out of the 7 patients having lesions >4 cm2. Many would consider this a contraindication to OATS. 29 It should be noted though, that their mean lesion size was the smallest in this systematic review, which would seem appropriate. Although their quality mid-term outcomes are encouraging, they may be explained by the small cohort and 6 out of 7 patients were male, which have demonstrated better outcomes after cartilage procedures. 8
There has been discussion about whether both reciprocal lesions need to be addressed surgically. 10 In general, most studies in this systematic review treated each lesion in the same manner. Hannon et al. 4 treated bipolar lesions involving the tibiofemoral compartment with femoral OCA and then tibial microfracture or debridement. At mid-term follow-up, both groups demonstrated improved patient reported outcomes and good survivorship. These results were comparable to a matched cohort of patients with unipolar femoral lesions treated with OCA alone. Longer follow-up is necessary, but these results are promising especially in comparison to the other OCA procedures involving the tibiofemoral compartment reported in this systematic review.
The surgical technique for treating bipolar cartilage lesions of the knee vary for the tibiofemoral and patellofemoral compartments. Both typically require an arthrotomy to perform any cartilage restoration procedure, but the exposure of the tibial cartilage surface can be particularly challenging. 10 OATS for the tibia is especially difficult, but Yabumoto et al. 30 have described a retrograde technique. Preoperative planning is vital to determine whether a medial or lateral arthrotomy is appropriate. Difficult exposure of the tibia has caused some to attempt more minimalist treatment options for these lesions.4,10 Certainly, more severe defects with subchondral bone loss would require more extensive treatment.8,11
The limitations of this systematic review should be considered. PRISMA guidelines were strictly followed but it is possible that relevant studies could have been excluded unintentionally. Most studies were level IV case series lacking randomization and blinding, although there was 1 level II study and 1 level III study. Indications for surgery and lesion etiology were variable across studies. Additionally, there was a high rate of concomitant procedures, but this is common with cartilage restoration procedures. Analysis of studies with variable length of follow-up was provided in this systematic review. This makes direct comparison of various surgical techniques challenging. It should be noted that early positive results do not necessarily correlate with quality long-term outcomes. Despite these weaknesses, this is the first systematic review evaluating surgical management of bipolar knee cartilage lesions.
Conclusions
Bipolar cartilage lesions of the knee typically involve a large surface area and are most commonly treated with ACI or OCA, while OATS may be an option for smaller lesions. Improvements in mid-term patient reported outcomes were reported for all surgical procedures and they can be performed safely with a low rate of major complications.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Christopher L. Camp: Arthrex, Inc.: travel and lodging. Daniel B.F. Saris: Cartilage: editorial or governing board; International Cartilage Repair Society, Dutch Orthopaedic Society: board or committee member; Knee Surgery, Sports Traumatology, Arthroscopy: editorial or governing board; Smith & Nephew: paid presenter or speaker; Smith & Nephew, Genzyme, Tigenix: paid consultant. Aaron J. Krych: Aesculap/B. Braun: research support; American Journal of Sports Medicine: editorial or governing board; Arthrex, Inc.: IP royalties, paid consultant; Arthritis Foundation: research support; Ceterix: research support; Histogenics: research support; International Cartilage Repair Society: board or committee member; International Society of Arthroscopy, Knee Surgery, and Orthopaedic Sports Medicine: board or committee member; Minnesota Orthopedic Society: board or committee member; Musculoskeletal Transplantation Foundation: board or committee member; Vericel: paid consultant. Open Payments Database: General Payments from Arthrex, Inc., Musculoskeletal Transplant Foundation, Ceterix Orthopedics, Inc., Gemini Medical LLC, and Gemini Mountain Medical.