
Abstract
Objective
We aimed to evaluate the outcomes, survivorship, and complications following multi-surface cartilage procedures at minimum 2-year follow-up.
Design
Patients with either (1) single-surface osteochondral allograft transplantation (OCAT) with third-generation matrix-induced autologous cultured chondrocyte implantation (MACI) or particulated juvenile cartilage implantation (DeNovo), or (2) multiple-surface OCAT ± associated MACI/DeNovo procedures for grade IV chondral or osteochondral defects about the knee with minimum 2-year follow-up were analyzed. Patient-reported outcome measures (PROMs), including International Knee Documentation Committee (IKDC) and Knee Injury and Osteoarthritis Outcome Score (KOOS) subscales, were obtained preoperatively and at minimum 2 years postoperatively. The percentage of patients who met the minimal clinically important difference (MCID) for each PROM was reported. Failure was defined as revision OCAT, conversion to patellofemoral/total/unicompartmental joint arthroplasty, or Arthrosurface HemiCAP placement.
Results
Of 257 patients identified, 35 were included. There was a significant increase in IKDC, KOOS-pain, KOOS-symptom, KOOS-sport, and KOOS-quality of life scores from preoperative to postoperative evaluation (P < 0.03 for all). More than 50% of patients met the MCID for each PROM. There were 2 failures, 1 of the patella and 1 of the medial femoral condyle, at 39.7 and 38.6 months postoperatively, respectively.
Discussion
Multi-surface cartilage procedures are a safe, efficacious treatment option for multifocal cartilage defects about the knee at short-term follow-up.
Keywords
What Was Known About the Subject
• Osteochondral allograft (OCA) transplantation has been well described as a safe and effective treatment for large grade IV chondral and osteochondral defects about a single location in the knee, yet there is relatively little information regarding the safety and efficacy of OCA transplant for multiple chondral and osteochondral defects about the knee.
What This Study Adds to Existing Knowledge
• The study builds on the existing literature surrounding the outcomes and survivorship of osteochondral allograft transplantations (OCATs) by including patients with concomitant OCAT and autologous chondrocyte implantation for multiple-surface chondral or osteochondral defects about the knee.
Introduction
Cartilage restoration procedures, including osteochondral allograft (OCA) transplantation, autologous chondrocyte implantation (ACI), and osteochondral autograft transfer (OATS), have become more prevalent in the United States over the past 2 decades. 1 Given the growing popularity of the aforementioned procedures, the rate of development of novel cartilage restoration techniques continues to increase. However, despite numerous recent advances in the field of cartilage restoration, the short-term, midterm, and long-term results of these procedures remain mixed in the literature.2-5
Although the incidence of multi-surface grade-IV chondral or osteochondral defects about the knee has yet to be elucidated, it is not uncommon for patients to present with grade-IV chondral or osteochondral defects on multiple surfaces of a joint, particularly in joints such as the knee, that experience high loads during weight-bearing. These lesions can be severely debilitating, and patients with focal chondral defects can have an impairment in their quality of life to the same degree as a patient with end-stage knee osteoarthritis. 6 Young patients with multi-surface grade-IV chondral or osteochondral defects pose a particular challenge to surgeons. The decision must be made to either proceed with partial or total knee arthroplasty, which has numerous disadvantages in this population, or consider multi-surface cartilage restoration procedures.
OCA transplantation has been well described as a safe and effective treatment for large grade-IV chondral and osteochondral defects about a single location in the knee,7-9 yet there is relatively little information regarding the safety and efficacy of OCA transplant for multiple chondral and osteochondral defects about the knee. Although 2 recent investigations of outcomes following multi-surface OCA transplantation about the knee found that patients have good outcomes at midterm follow-up,10,11 no studies to date have evaluated the outcomes following OCA transplant with and without concomitant cell-based cartilage restoration procedures, including MACI and particulated juvenile cartilage implantation (DeNovo). It is critical that we gain an understanding of the safety, efficacy, and survivorship of these procedures as they are often performed in tandem. Current treatment algorithms for cartilage repair include defect-specific indications that call for specific techniques, for example, osteochondral versus cell-based repair. In patients with multifocal disease, occasionally, different defects exhibit characteristics that would indicate them for different cartilage repair options.
The aim of this study is to evaluate the outcomes, survivorship, and complications following multi-surface cartilage procedures, including multi-location OCA transplantation and single-location OCA transplantation with concomitant MACI or DeNovo procedures at minimum 2-year follow-up. It is hypothesized that patients will have good outcomes and low failure rate at short-term follow-up following the aforementioned procedures.
Methods
Patient Selection
Following institutional review board approval, we performed a retrospective review of patients ages 15 through 55 years undergoing osteochondral allograft transplantation (OCAT) with or without associated third-generation matrix-induced autologous cultured chondrocyte implantation (MACI) on a porcine collagen membrane or DeNovo for focal grade-IV (>2 cm2) chondral or osteochondral defects of the patella, trochlea, or femoral condyles by one of 2 senior sports medicine fellowship–trained orthopedic surgeons (S.M.S., A.H.G.) at a single tertiary care metropolitan institution between May 2016 and December 2021. Patients were identified by procedure type (OCAT) in a query of the electronic medical record database.
Patients were included in the study if they underwent OCA transplantation of at least one surface of the knee with concomitant MACI or DeNovo procedures of at least one surface of the knee or multi-surface OCA transplantation with or without concomitant MACI/DeNovo procedures. Patients with preoperative and minimum 2-year postoperative International Knee Documentation Committee (IKDC) scores were included. Patients were excluded from the study if they only underwent MACI/DeNovo or OCA transplantation of one surface of the knee, if they did not have both preoperative and postoperative IKDC scores, or if they had less than 2 years minimum clinical follow-up.
Chart review was performed to obtain demographic information as well as information regarding the type of procedure performed. Degenerative lesions were defined as lesions occurring in the absence of trauma or patellar instability episode. Traumatic lesions were defined as lesions occurring secondary to direct trauma or patellar instability.
Surgical Technique—OCAT
All OCA grafts were provided by JRF Ortho. A medial or lateral parapatellar arthrotomy was used to expose the cartilage defect, which was sized and reamed under constant cold irrigation, limiting the depth to less than 8 mm. Care was taken to remove a minimal amount of healthy subchondral bone. A corresponding graft was fashioned from the allograft based on diameter and depth of the recipient’s reamed defect as measured in 4 quadrants. The graft was then placed into the recipient site with manual pressure and seated flush with the surrounding cartilage. Bioabsorbable pins were used to provide mechanical stability for uncontained OCD (osteochondritis dissecans) lesions. Postoperatively, patients were restricted to touch-down weight-bearing on crutches for 4 weeks, with range of motion as tolerated at the knee if they underwent cartilage restoration procedures of the femoral condyles. The patients were made to perform weight-bearing as tolerated for cartilage restoration procedures isolated to the patellofemoral joint. Patients were allowed to return to sports at 6 months postoperatively for isolated OCA and at 8 to 12 months postoperatively for OCA performed with concomitant MACI/DeNovo procedures.
Surgical Technique—MACI
MACI is performed as a 2-stage procedure. For the first stage, a standard diagnostic arthroscopy is performed, with chondroplasty as needed. Two hundred to 300 mg of healthy cartilage is harvested from the intercondylar notch, placed in a culture medium, and sent to the lab for processing.
The second stage occurs at a minimum of 1 month following the first stage once the autologous chondrocytes are ready for implantation. A standard open approach is used to access the osteochondral defect, and the defect site is prepared with curettes to remove the calcified cartilage. A “cookie cutter” or foil is used to create an outline of the defect, and the MACI is cut to match the size of the defect. A layer of fibrin glue is placed into the defect, and then MACI is placed into the defect with cells lying face down. A thin layer of fibrin glue is then placed at the periphery of the MACI.
Surgical Technique—DeNovo
DeNovo implantation consists of a single-stage procedure. Diagnostic arthroscopy is performed to confirm lesion characteristics, and a standard open approach is used to access the osteochondral defect. Foil is pressed into the defect to create a mold. On the back table, the cartilage fragments are arranged in one continuous layer and cured using fibrin glue. One packet of DeNovo covers a defect with a diameter of 2.0 to 2.5 cm2. The implant is then inserted into the defect using fibrin glue, about 1 mm below the shoulder of the defect.
MACI/DeNovo/OCA Selection
MACI or DeNovo were performed on either the patella or trochlea for lesions <15 mm in diameter. If the lesion was >15 mm in diameter on any surface, then OCA transplantation was performed.
Concomitant Realignment Procedures
Concomitant high tibial osteotomy (HTO) was added if the patient had >3 degrees varus hip-to-ankle alignment. Distal femoral osteotomy (DFO) was added if the patient had >3 degrees valgus hip-to-ankle alignment. Tibial tubercle osteotomy (TTO) was added if the patient had a tibial tubercle-to-trochlear groove (TTTG) distance of >15 mm or Caton Deschamps Index (CDI) of >1.2.
Patient-Reported Outcome Measures (PROMs)
IKDC and Knee Injury and Osteoarthritis Outcome Score subscales, including pain (KOOS-pain), other symptoms (KOOS-Sx), function in activities of daily living (KOOS-ADL), function in sport and recreation (KOOS-sport), and knee-related quality of life (KOOS-QoL) were obtained preoperatively and at minimum 2 years postoperatively.
The minimal clinically important difference (MCID) values for OCA transplantation were used for analysis for each PROM obtained from prior studies. Specifically, the MCID values were as follows: 9.8 for IKDC, 12 16.7 for KOOS-pain, 12 10.7 for KOOS-Sx, 13 25 for KOOS-sport, 12 and 18.8 for KOOS-QoL. 13
Statistical Analysis
Descriptive statistics, including means, standard deviations, frequencies, and percentages were used to evaluate patient and lesion characteristics. Normally distributed continuous data were reported as means ± standard deviations, whereas non-normally distributed continuous data were reported as a median value with interquartile range (IQR). Data for the change in PROMs, including IKDC and all KOOS sub-scores, were normally distributed per the results of the Shapiro-Wilk test; therefore, paired t tests were used for analysis when evaluating the preoperative to postoperative change in PROMs. The percentage of patients who met the MCID for each PROM was also reported. Failure was defined as revision OCAT, conversion to patellofemoral/total/unicompartmental joint arthroplasty, or Arthrosurface HemiCAP placement (Anika Therapeutics, Bedford, MA). Data analysis was performed with STATA (StataCorp LLC, College Station, TX). Statistical significance was determined at the α < .05 level.
Results
A total of 257 patients underwent OCA transplantation between May 2016 and December 2021, 35 of whom (14%) remained for analysis following application of inclusion and exclusion criteria. Of the patients included in the study, 15 (43%) were female. The average age was 40.0 ± 9.6 years and average BMI was 27.0 ± 4.1 kg/m2 ( Table 1 ). Seventeen (49%) were right-knee cases. Seventeen patients (49%) had concomitant or previous TTO, DFO, or HTO ( Table 1 ). The majority of osteochondral defects were degenerative (25, 71%), with the remaining occurring secondary to trauma (10, 29%). The median follow-up time was 32.1 months (IQR: 24.2-34.7 months, Table 1 ).
Demographics for All Patients (N = 35).
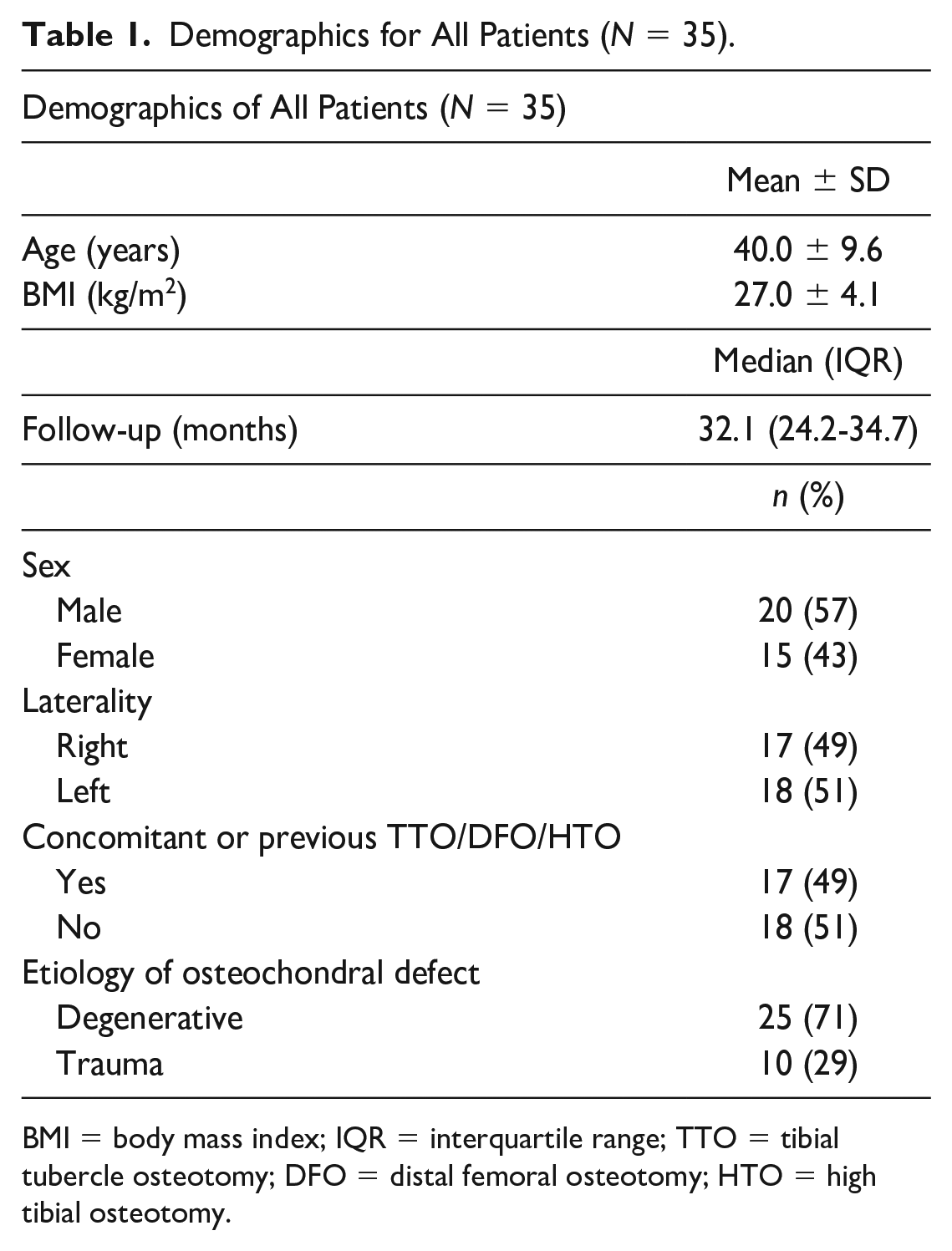
BMI = body mass index; IQR = interquartile range; TTO = tibial tubercle osteotomy; DFO = distal femoral osteotomy; HTO = high tibial osteotomy.
Twelve patients (34%) included in our cohort had 2 or more OCA plugs only. Two patients (6%) had 2 or more OCA plugs + MACI, 1 patient (3%) had 2 or more OCA plugs + DeNovo, 3 patients (9%) had 1 OCA plug + MACI, and 4 patients (11%) had 1 OCA plug + DeNovo ( Table 2 ).
Osteochondral Allograft Plug Number and Concomitant Cartilage Restoration Procedures.
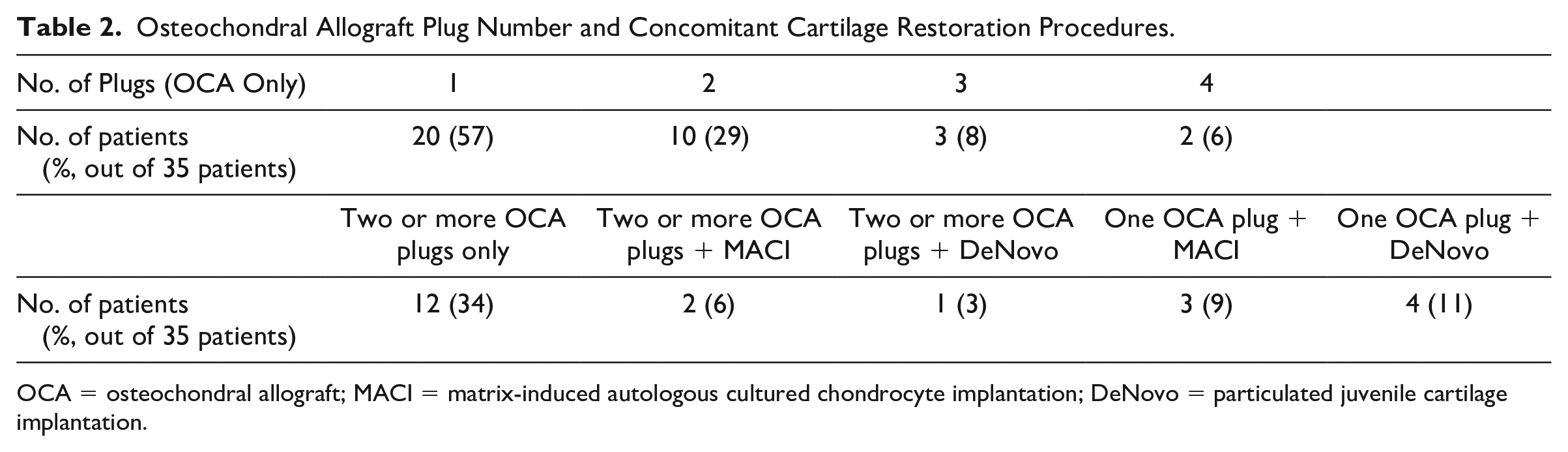
OCA = osteochondral allograft; MACI = matrix-induced autologous cultured chondrocyte implantation; DeNovo = particulated juvenile cartilage implantation.
The majority of cartilage procedures involved the trochlea (19 patients, 54%), followed by the patella (17 patients, 49%), the medial femoral condyle (MFC; 16 patients, 46%), and the lateral femoral condyle (LFC; 11 patients, 31%; Table 3 ). Among OCA transplants only, the majority involved the MFC (16 patients, 46%), followed by the trochlea (15 patients, 443%), LFC (11 patients, 31%) and patella (7 patients, 20%; Table 3 ). The majority of MACI and DeNovo procedures involved the patella (6 patients, 17%). Two patients (6%) had bipolar (patella/trochlea) OCA transplants ( Table 3 ).
Cartilage Transplantation Locations.
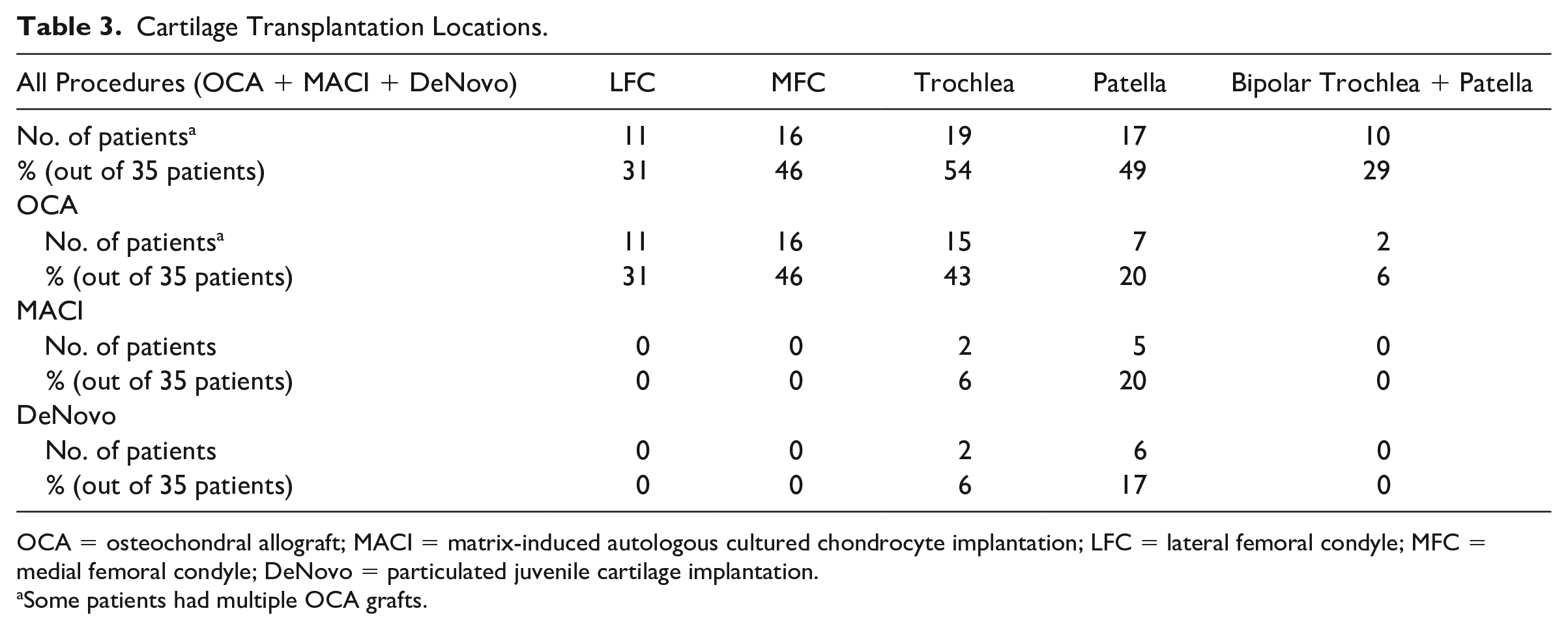
OCA = osteochondral allograft; MACI = matrix-induced autologous cultured chondrocyte implantation; LFC = lateral femoral condyle; MFC = medial femoral condyle; DeNovo = particulated juvenile cartilage implantation.
Some patients had multiple OCA grafts.
The median graft diameter was 18.5 mm (IQR: 16.0-21.0 mm; Table 4 ). The mean graft diameter was 20.2 ± 6.0 mm and 19.7 ± 2.3 mm on the trochlea and patella, respectively. Median graft diameter values were 18.0 mm (IQR: 18-20 mm) and 18.1 mm (IQR: 17-20 mm) on the LFC and MFC, respectively ( Table 4 ).
Mean/Median Osteochondral Allograft Size by Location.

LFC = lateral femoral condyle; MFC = medial femoral condyle; IQR = interquartile range.
There was a significant increase in IKDC (P < 0.001), KOOS-pain (P < 0.001), KOOS-Sx (P = 0.009), KOOS-sport (P = 0.029), and KOOS-QoL (P < 0.001) scores from preoperative to postoperative evaluation ( Table 5 ). More than 55% of patients achieved the MCID for each PROM ( Table 6 ).
Preoperative, Postoperative, and Change in PROM Values, Including IKDC and KOOS Subscales, From Preoperative to Minimum 2 Years Postoperative evaluation.
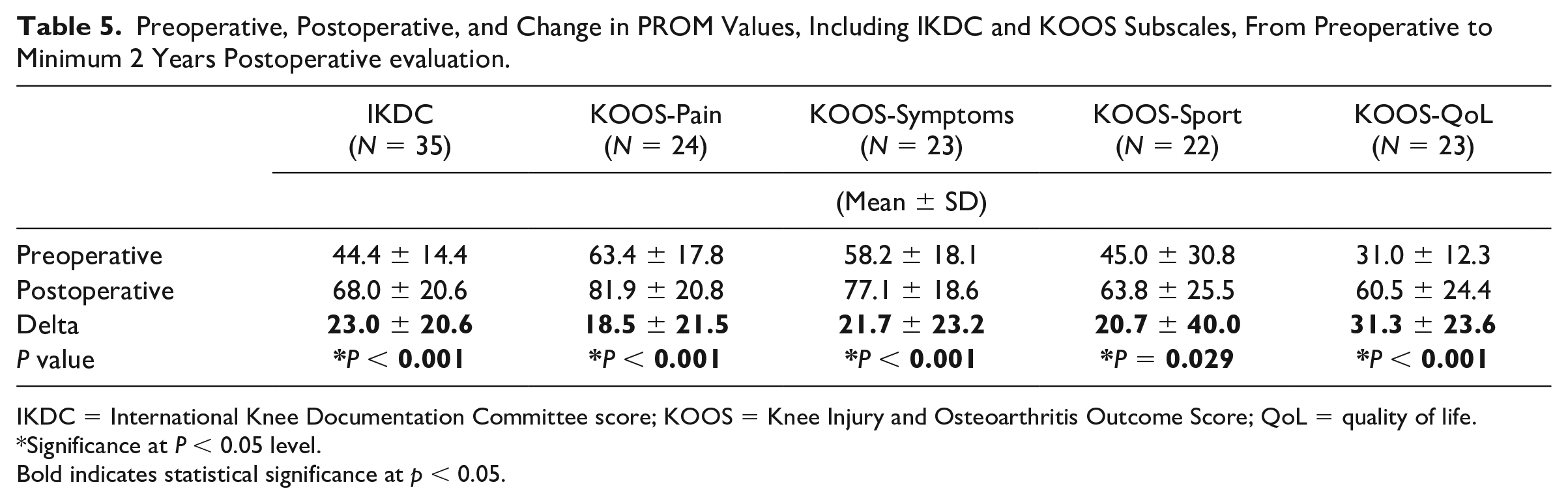
IKDC = International Knee Documentation Committee score; KOOS = Knee Injury and Osteoarthritis Outcome Score; QoL = quality of life.
Significance at P < 0.05 level.Bold indicates statistical significance at p < 0.05.
Percentage of Patients with Osteochondral Allograft Transplantation Only, Who Achieved the MCID for Each Patient-Reported Outcome Measure (PROM) at Minimum 2-Year Follow-up.
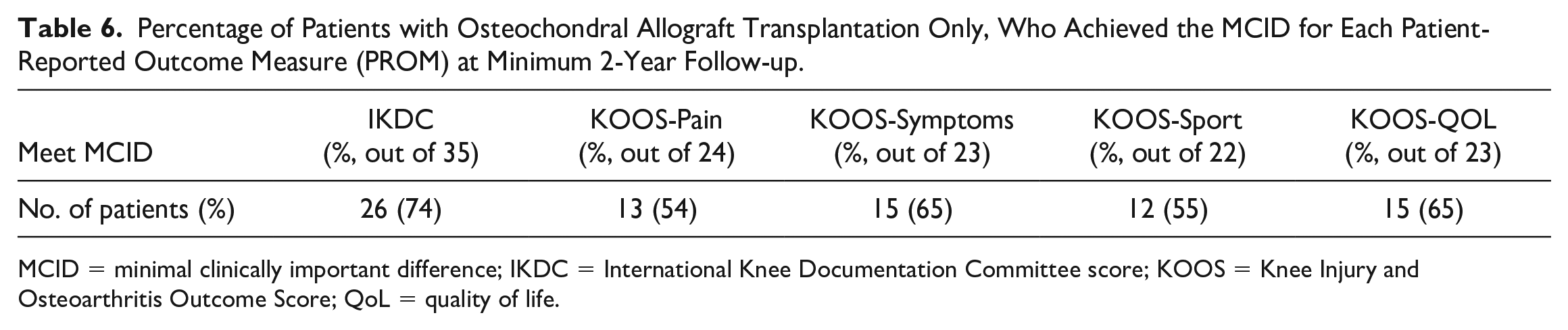
MCID = minimal clinically important difference; IKDC = International Knee Documentation Committee score; KOOS = Knee Injury and Osteoarthritis Outcome Score; QoL = quality of life.
There were 2 failures at minimum 2-year follow-up. One patient experienced failure of the OCA plug at the MFC at 39.7 months postoperatively and underwent Arthrosurface HemiCAP placement of the MFC. The second patient experienced failure of the OCA plug at the patella and underwent conversion to patellofemoral joint arthroplasty at 38.6 months postoperatively. Eighteen (51%) patients underwent reoperation, 13 of whom underwent debridement/lysis of adhesions/manipulation under anesthesia, 6 underwent removal of hardware, and 2 underwent quadriceps tendon repair ( Table 7 ).
Reoperation Rate for the Entire Cohort and OCA-Only Versus OCA + MACI/DeNovo Subgroup Analysis.
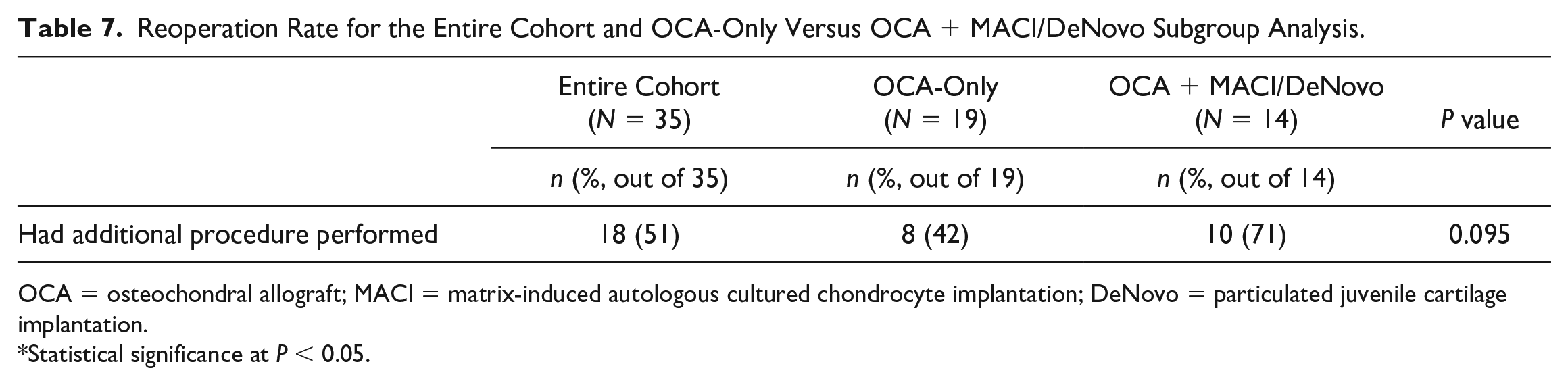
OCA = osteochondral allograft; MACI = matrix-induced autologous cultured chondrocyte implantation; DeNovo = particulated juvenile cartilage implantation.
Statistical significance at P < 0.05.
Discussion
We found that patients experienced good outcomes with a low failure rate following multi-surface cartilage repair with multiple OCA plugs or OCA with concomitant MACI/DeNovo procedures at minimum 2-year follow-up. More than half of the patients who underwent OCA transplantation without concomitant MACI/DeNovo met the MCID for IKDC. More than half of patients in our cohort underwent reoperation, and the most common procedures performed included debridement, lysis of adhesions, or manipulation under anesthesia.
Similar to Cook et al. 10 and Cotter et al., 11 we found significant improvement in PROMs from preoperative to postoperative evaluation for patients undergoing multi-surface cartilage repair. We also found that more than a third of the patients in our cohort underwent reoperation, which is similar to reoperation rates described by Cotter et al.11 (20%).
For KOOS-sport, ceiling effects likely contributed to the relatively lower percentage of patients achieving the MCID for this PROM. Among the 11 patients who did not achieve the MCID for KOOS-sport, 5 patients had preoperative scores of 80 or greater, so these patients could not achieve the MCID due to ceiling effects of this PROM. Similarly, for KOOS pain, 2 out of 9 patients who did not achieve the MCID had preoperative scores of 83.33 or greater, which precluded these patients from achieving the MCID for KOOS pain due to ceiling effects of this PROM.
The rate of concomitant realignment procedures (49%) was only slightly lower than previous OCA studies (62% 14 and 68%, 15 respectively). Of the 18 patients in this study who did not have a concomitant realignment procedure, all had CDI and TTTG values within normal limits (mean values of 1.05 ± 0.11, range: 0.86-1.17, and 13.0 ± 3.8, range: 3.2-16.9, respectively). In addition, hip to ankle alignment was neutral, very mild varus (<2°), or very mild valgus (<2°) in all patients who did not have concomitant realignment procedure. Therefore, the realignment procedures were not indicated in the patients who did not have concomitant TTO/HTO/DFO in this study.
There are several limitations to this study. This is a retrospective study, which has its inherent limitations, including lack of randomization of surgical procedures performed. In addition, we had a relatively small sample size, which may impact the power of our statistical analysis. Midterm and long-term data are also lacking. Finally, there was a range of concomitant procedures performed, including TTO, HTO, and medial patellofemoral ligament reconstruction, which could impact the generalizability of our results. However, cartilage restoration is rarely performed in isolation, and concomitant realignment procedures are critical in attempting to offload the previously overloaded compartment to preserve the newly restored cartilage. Therefore, we argue that our sample is representative of patients who undergo cartilage restoration procedures.
In sum, multiple-location cartilage procedures, including OCATs with or without concomitant MACI/DeNovo procedures, are a safe, efficacious treatment option with a low failure rate at short-term follow-up for multifocal grade IV chondral or osteochondral defects about the knee. Multi-surface cartilage restoration procedures can serve as an effective temporizing solution as we aim to delay arthroplasty in young patients. Future studies are needed to evaluate outcomes and survivorship of these procedures at long-term follow-up.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: J.S.R. receives support from the NIH T32 AR078751.
Ethical Approval
This study was approved by our Institutional Review Board (Approval # 2020-2123).