
Abstract
Objective
To compare (1) the reoperation rates, (2) risk factors for reoperation, (3) 30-day complication rates, and (4) cost differences between autologous chondrocyte implantation (ACI) and osteochondral allograft transplantation (OCA) of the knee in a large insurance database.
Design
Subjects who underwent knee ACI (Current Procedural Terminology [CPT] code 27412) or OCA (CPT code 27415) with minimum 2-year follow-up were queried from a national insurance database. Reoperation was defined by ipsilateral knee procedure after index surgery. Multivariate logistic regression models were built to determine the effect of independent variables (age, sex, tobacco use, obesity, diabetes, and concomitant osteotomy) on reoperation rates. The 30-day complication rates were assessed using ICD-9-CM codes. The cost of the procedures per patient was calculated. Statistical comparisons were made. All P values were reported with significance set at P < 0.05.
Results
A total of 909 subjects (315 ACI and 594 OCA) were included (mean follow-up 39.2 months). There was a significantly higher reoperation rate after index ACI compared with OCA (67.6% vs. 40.4%, P < 0.0001). Concomitant osteotomy at the time of index procedure significantly reduced the risk for reoperation in both groups (odds ratio [OR] 0.2, P < 0.0001 and OR 0.2, P = 0.009). The complication rates were similar between ACI (1.6%) and OCA (1.2%) groups (P = 0.24). Day of surgery payments were significantly higher after ACI compared with OCA (P = 0.013).
Conclusions
Autologous chondrocyte implantation had significantly higher reoperation rates and cost with similar complication rates compared with OCA. Concomitant osteotomy significantly reduced the risk for reoperation in both groups.
Introduction
Knee chondral or osteochondral lesions are common with the reported prevalence as high as 66% in several studies.1-4 These lesions have little potential for self-repair due to the avascular nature of articular cartilage.5-7 As such, if left untreated, these chondral defects may lead to osteoarthritis at an early age.8,9 Multiple surgical options for treating symptomatic cartilage defects in the knee have been described with an estimated 200,000 to 300,000 cartilage procedures performed annually in the United States.10-15
Debridement, microfracture, or osteochondral autograft transplantation are most commonly indicated in chondral defects less than 2 cm2.12,13 However, in larger defects, autologous chondrocyte implantation (ACI) or osteochondral allograft transplantation (OCA) are more viable options.11,14,15 Since it was first reported in 1994, studies have found favorable outcomes following the use of ACI with graft survivorship up to 87.5% at 10 years.15-19 Osteochondral allograft transplantation also has a long track record of success with graft survivorship up to 91.0% at 10-year follow-up and 86% of patients satisfied at 5 years following surgery.20-24
However, it is unclear which cartilage restoration technique is the most effective strategy for chondral defects as there are limited data directly comparing ACI and OCA with regard to objective clinical outcomes. The purpose of this study was to compare (1) the reoperation rates, (2) risk factors for reoperation, (3) 30-day complication rates, and (4) cost differences between ACI and OCA of the knee in a large insurance database. The authors hypothesized that there would be no significant differences in (1) reoperation rates, (2) comorbidities would increase the risk for reoperations, (3) 30-day complications rates would be similar, and (4) cost would be similar between ACI and OCA of the knee.
Method
The MarketScan Commercial Claims and Encounters database (Truven Health Analytics, Ann Arbor, MI) from January 1, 2007 to December 31, 2016 was used for this study. This database is a collection of commercial inpatient, outpatient, and pharmaceutical claims. Only outpatient records in MarketScan were queried for this study. The MarketScan database contains International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) and 10th revision, Clinical Modification (ICD-10-CM), Current Procedural Terminology (CPT), Diagnosis-Related Group (DRG) codes as well as National Drug Codes (DEA).
Patients who underwent open ACI or open OCA of the knee in the outpatient setting with a minimum of 2-year follow-up were queried in the database using CPT codes 27412 and 27415, respectively. Records of the index surgery were reviewed for analysis. Patients without a CPT modifier for laterality (left or right) were excluded. Patients who had both procedures were excluded, thus making the cohorts mutually exclusive. Additionally, patients undergoing concomitant ligament reconstruction procedures were excluded. Patient-level variables, including age at time of surgery, sex, and comorbidities (obesity, tobacco, myocardial infarction, congestive heart failure, peripheral vascular disease, cerebrovascular disease, dementia, chronic pulmonary disease, rheumatic disease, peptic ulcer disease, liver disease, diabetes, hemiplegia, renal disease, malignancy, AIDS/HIV, tobacco use) were recorded based on claims data ( Table 1 ).
Patient Demographics.
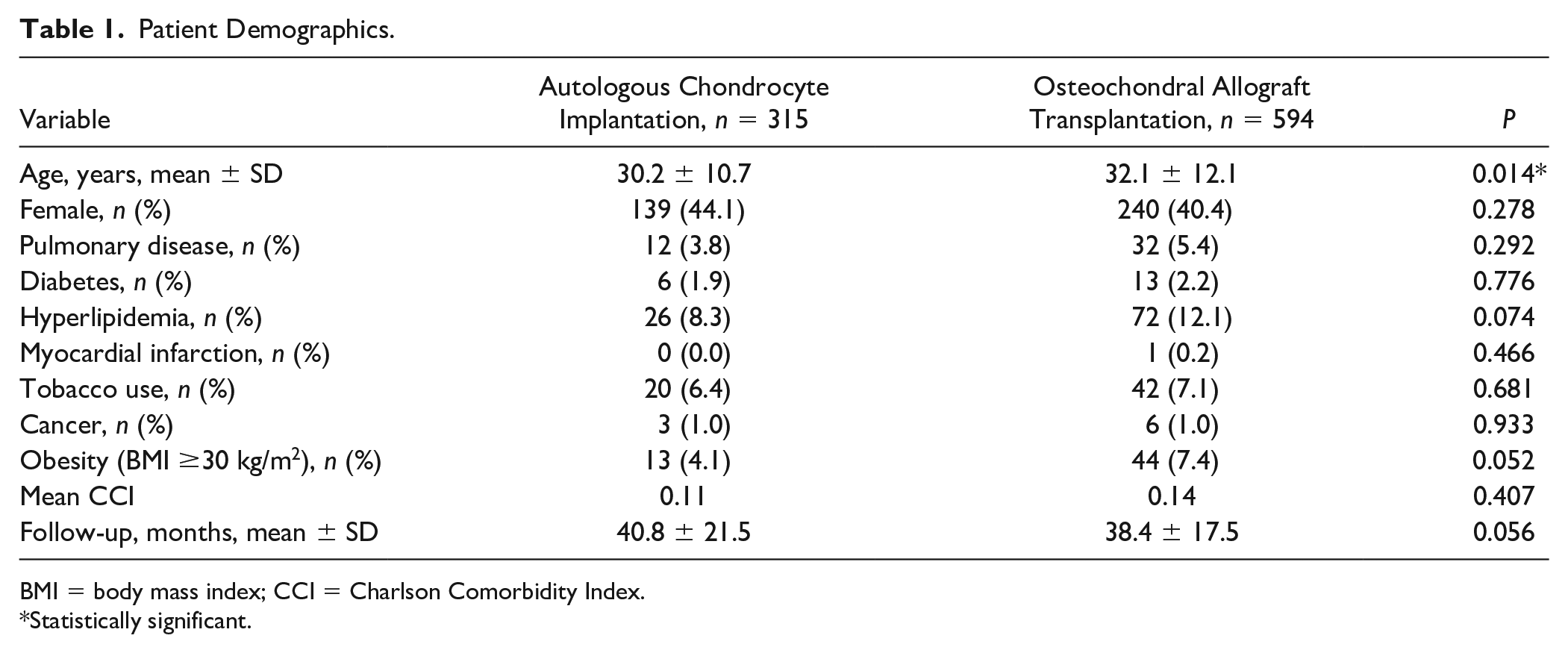
BMI = body mass index; CCI = Charlson Comorbidity Index.
Statistically significant.
The primary outcome measure was rate of ipsilateral reoperation. Reoperation was defined by ipsilateral ACI (CPT code 27412), OCA (CPT codes 27415 or 29867), osteochondral autograft transplantation (CPT code 29866), synovectomy (CPT codes 29875 or 29876), chondroplasty (CPT code 29877), microfracture (CPT code 29879), manipulation under anesthesia (CPT code 27570), lysis of adhesions (CPT code 29884), arthroscopic loose body removal (CPT code 29874), debridement for infection (CPT codes 27301, 27303, 27310, 29871), osteotomy (CPT codes 27457, 27450, or 27418), partial knee replacement (CPT code 27446), and total knee replacement (CPT code 27447) that occurred after the index surgery date.
Ipsilateral reoperation was queried using CPT codes and the CPT modifiers for laterality to ensure that the procedures were reoperations and not contralateral procedures. The time period for potential reoperation was up to a maximum of 9 years postoperatively, depending on when the index ACI or OCA was performed. Multivariate logistic regression models were built for each cohort to determine the effect of independent variables (age, sex, tobacco use, obesity, diabetes, and concomitant osteotomy) on reoperations rates.
The 30-day postoperative complication rates were also assessed for both cohorts using the ICD-9-CM codes. These included bursitis, anemia, knee dislocation, infection, nerve injury, neurologic complications, cardiac complication, heterotopic ossification, sepsis, wound complication, deep vein thrombosis (DVT), pulmonary embolus (PE), hematoma, pulmonary complication, urinary tract infection (UTI), and delirium.
The cost of the procedures per patient was calculated using the DRG system. This included the entire reimbursement by the insurer on the day of surgery. The cumulative cost of the procedure per patient was also calculated at 9 months and 2 years postoperatively including the cost of reoperations.
Statistical comparisons of cohort demographics, reoperations, postoperative complications, and payments were made. The significance of differences in means of continuous variables between the two groups was determined by the Student t test. The differences in categorical variables between groups was determined by the chi-square test. Odds ratios (ORs) were calculated with respective 95% confidence intervals (CIs). Percentages in this study were a representation of proportion of the cohort. All P values were reported with significance set at P < 0.05.
As this study includes only analysis of secondary de-identified data, it was not considered human subject research and received exemption from the institutional review board approval at our institution.
Results
A total of 909 subjects (315 ACI and 594 OCA) out of 2,158 (682 ACI and 1476 OCA) met inclusion criteria and were included in the study with a mean follow up of 39.2 months ( Table 1 ). Demographics were similar between groups except subjects in the OCA group were statistically older (32.1 vs. 30.2 years old, P = 0.014).
There were significantly more patients who required ipsilateral reoperations after index autologous chondrocyte implantation (67.6%) compared to osteochondral allograft postoperatively (40.4%; P < 0.0001; Table 2 ). The most commonly reported reoperation was for revision ACI or OCA in each group, respectively. There were also significantly more patients who underwent osteotomy following ACI (18.4%) compared with OCA (4.7%; P < 0.0001; Table 2 ). Subjects undergoing ACI as the index procedure were also significantly more likely to undergo arthroscopic chondroplasty (12.4% vs. 5.9%, P = 0.0007), lysis of adhesions (4.4% vs. 1.9%, P = 0.023), and synovectomy (9.5% vs. 5.1%, P = 0.010) compared with patients who had OCA ( Table 2 ). There were low rates of conversion to knee arthroplasty for ACI (1.3%) and OCA (3.2%) at final follow-up. There were no significant differences in unicompartmental and total knee arthroplasty rates between groups ( Table 2 ).
Reoperations.
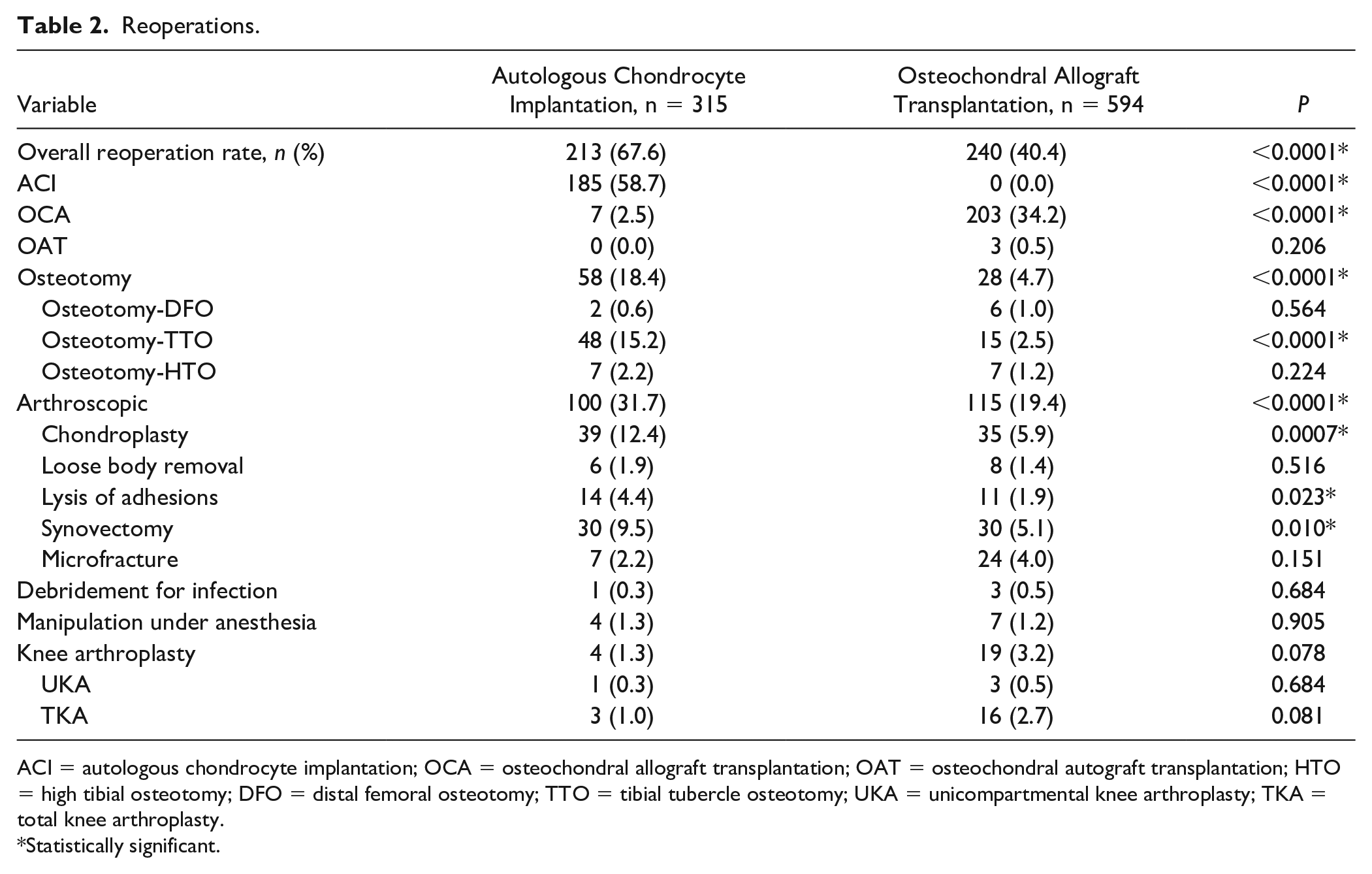
ACI = autologous chondrocyte implantation; OCA = osteochondral allograft transplantation; OAT = osteochondral autograft transplantation; HTO = high tibial osteotomy; DFO = distal femoral osteotomy; TTO = tibial tubercle osteotomy; UKA = unicompartmental knee arthroplasty; TKA = total knee arthroplasty.
Statistically significant.
There were no significant independent risk factors for reoperation after undergoing ACI in the current study ( Table 3 ). Female sex was a significant risk factor for reoperation in the OCA group (OR 1.5, P = 0.017) ( Table 4 ). Undergoing a concomitant osteotomy at the time of the ACI or OCA index procedure significantly reduced the risk for reoperation in both groups (OR 0.2, P < 0.0001 and OR 0.2, P = 0.009, respectively).
Multivariate Regression Analysis to Identify Predictors of Autologous Chondrocyte Implantation (ACI) Reoperation.
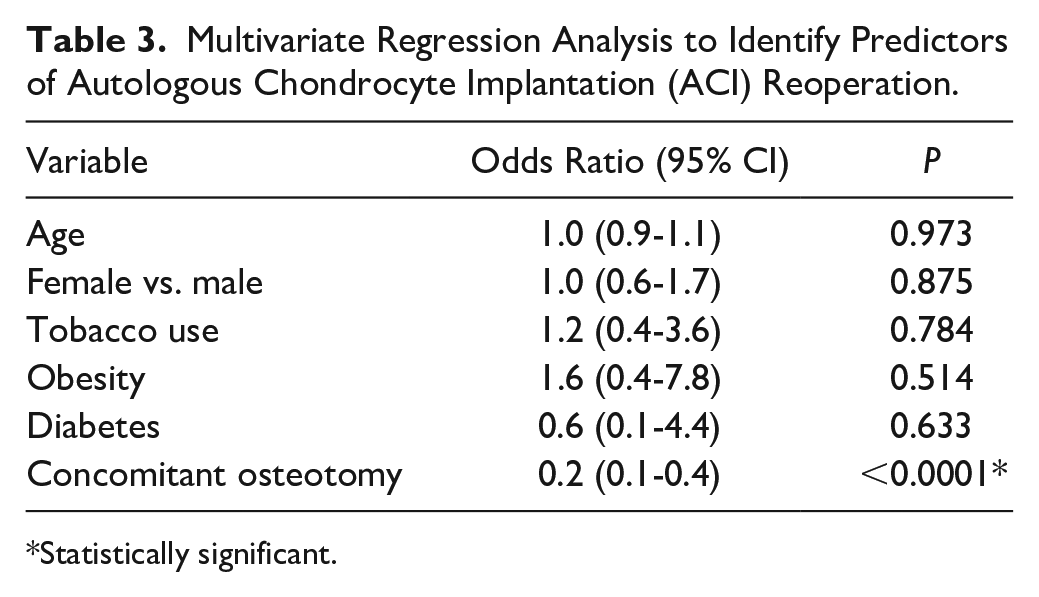
Statistically significant.
Multivariate Regression Analysis to Identify Predictors of Osteochondral Allograft Transplantation (OCA) Reoperation.
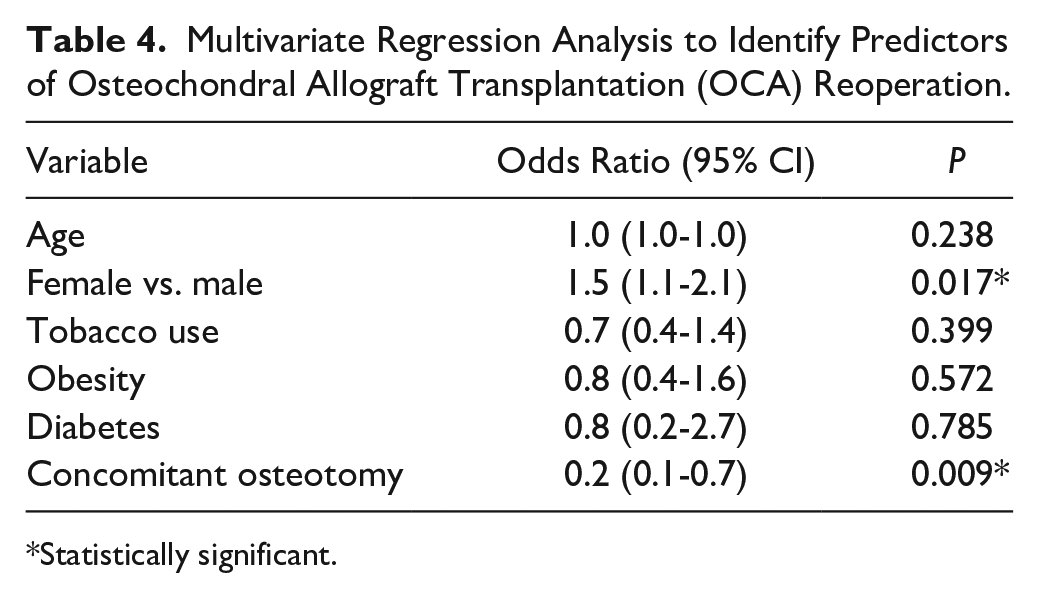
Statistically significant.
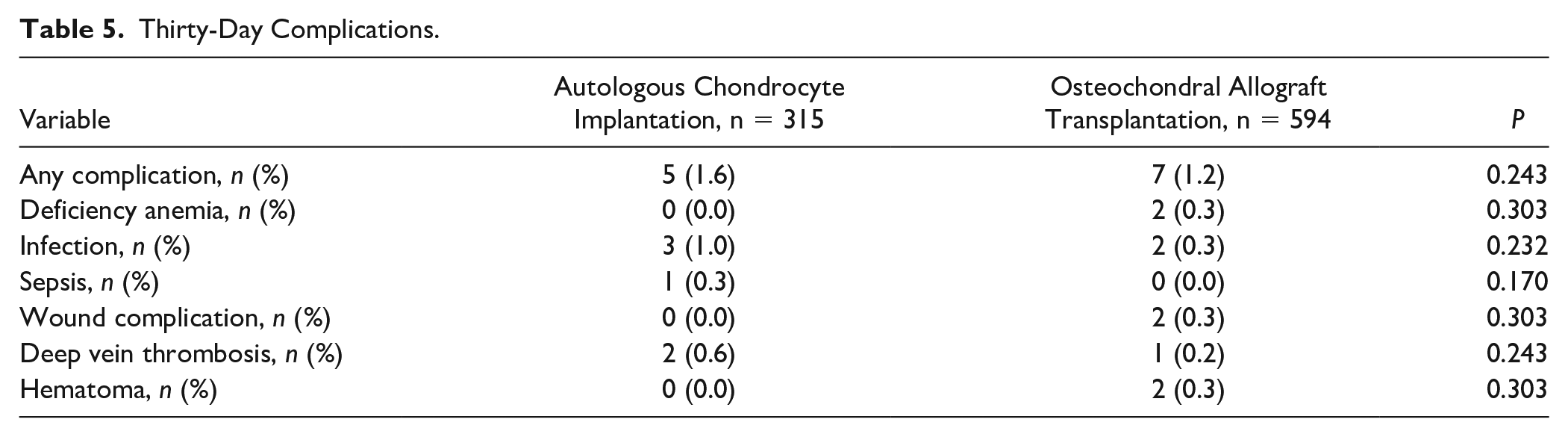
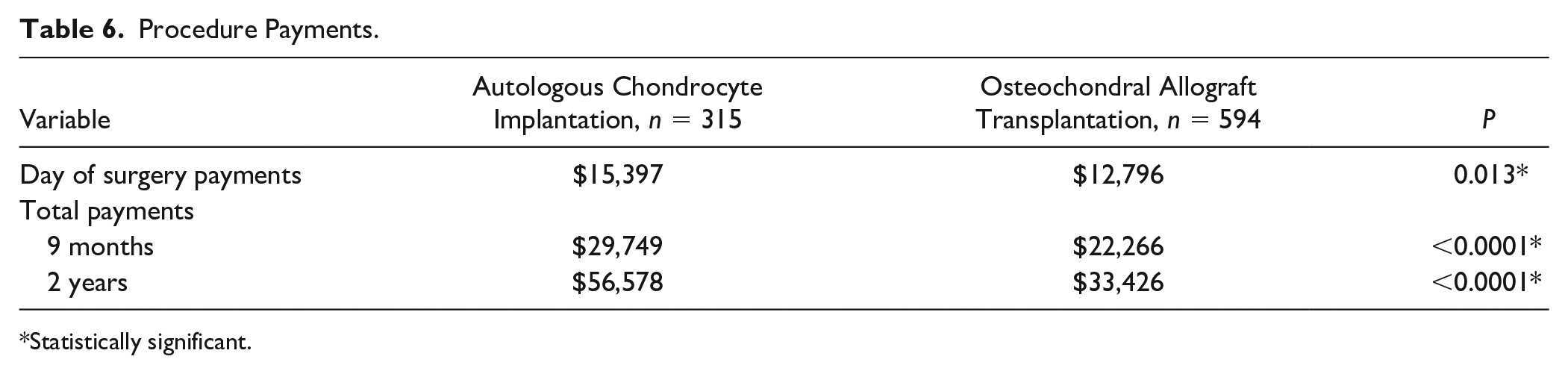
The overall complication rates were similar between the ACI (1.6%) and OCA (1.2%) groups (P = 0.24) ( Table 5 ). The total day of surgery payments was significantly higher in the ACI group compared with OCA ($15,397 vs. $12,796, P = 0.013) ( Table 6 ). This trend occurred at all time points in the study with a total 2-year cost of ACI at $56,578 compared with the 2-year cost of OCA of $33,426 including reoperations (P < 0.0001).
Thirty-Day Complications.
Procedure Payments.
Statistically significant.
Discussion
Autologous chondrocyte implantation results in significantly higher reoperation rates, similar complication rates, and significantly higher cost compared to osteochondral allograft transplantation of the knee with concomitant osteotomy significantly reducing the risk for reoperation in both groups in a large insurance database.
Subjects undergoing autologous chondrocyte implantation as the index procedure had a significantly higher reoperation rate (67.6%) compared with those undergoing osteochondral allograft (40.4%) at final follow-up. The current study has significantly higher failure rates than previously reported in the literature for both the ACI and OCA groups. Previous studies have determined that ACI and OCA survivorship free from reoperation ranges from 71.0% to 87.5% and 76.0% to 91.0% at up to 10 years following surgery, respectively.15-24
This higher reoperation rate seen in both groups is likely multifactorial. In previous studies, graft failure was defined differently with the most commonly used definitions consisting of reoperation, revision surgery, need for knee arthroplasty, and failure to improve from baseline on patient reported outcomes scores postoperatively. As such, reoperation depends on the definition used. However, the study was able to perform an adequate comparison between cohorts by using the same definition of reoperation for subjects undergoing ACI and OCA treatments. This would seem to control for the varying definitions of failure seen in other studies.
Additionally, most of the peer-reviewed literature is from knee reconstruction experts with high-volume experience, usually of longer duration, and potentially greater familiarity with the procedures than the average orthopedic surgeon. As such, the current literature may underestimate the true reoperation rate in the general orthopedic surgeon population. 25 This becomes increasingly more evident after review of the present study with higher reoperation rates compared to the literature. Therefore, it is the opinion of the current authors that these surgeries be performed by high-volume surgeons with extensive experience in cartilage restoration in order to limit adverse outcomes and high reoperations.
Several patient demographic and anatomical factors have been identified that can affect the outcomes of ACI and OCA surgery. There were no independent predictors of reoperation in the current study utilizing multivariate logistic regression models for subjects undergoing autologous chondrocyte implantation. This is similar to a previous study by Jungmann et al. in which age, body mass index, smoking history, defect number, defect size, and defect location were not identified to be predictors of failure. 26 Two previous studies by Jaiswal et al.,27,28 however, did identify elevated body mass index and tobacco use as predictors of worse outcomes. However, this was based on patient-reported outcome scores and not failure or reoperation rates.
One potential explanation for the higher reoperation rate following ACI is the inclusion of multiple generations of ACI treatments. Although studies have shown similar clinical outcomes between the generations at two years, graft hypertrophy is significantly higher following ACI with periosteal patch (22%) compared to the using a membrane (6%), leading to higher reoperations.26,29-31 It is possible that the ACI cohort had a higher number of subjects that underwent use of periosteal patch resulting in reoperation compared to previous studies. As such, if subjects that underwent the older generation of ACI were excluded, the reoperation rate may more closely resemble that of the OCA cohort. However, this could not be reliably determined in the current study.
It is also possible that ACI was more frequently used in the patellofemoral joint. However, this is difficult to discern from the database. If that is the case, the reoperation rate in the current study would be more similar to that seen in the literature for patella ACI of 60% at up to 14 years postoperatively. 32
Multivariate logistic regression models in the osteochondral allograft cohort identified female gender as a predictor of reoperation. Previous studies had similar results with age, tobacco use, and obesity having no significant effect on reoperation rates.33-35 There are conflicting results with regards to the relationship between sex and graft failure in the literature, however. Frank et al. 33 demonstrated that males and females had similar outcomes following osteochondral allograft. This differs from the current study that demonstrated females to be predictive of reoperation. It is possible that the difference is due the study by Frank et al. 33 being underpowered to detect such a difference with only 170 subjects included compared with 594 in the present study.
Concomitant osteotomy was identified as an independent predictor of reduced reoperation in both the ACI and OCA cohorts in the present study. This confirms the results of several previous publications in the literature. With regard to ACI, several studies have found that concomitant osteotomy (distal femoral, high tibial, or tibial tubercle) results in improved clinical outcomes and graft survivorship.36-39 This same trend was also seen in patients following osteochondral allograft as residual malalignment was identified as a predictor for failure.40,41 Concomitant osteotomy unloads the affected compartment leading to reduced contact pressures on the implanted graft which likely leads to improved graft survival and outcomes.42-45
Despite the increased reoperation rate following ACI compared with OCA, both cohorts had similar complication rates (1.6% vs. 1.2%, respectively, P = 0.24). These rates are similar to the previously reported complications following ACI and OCA.15-24 However, it is possible that this complication rate may be underestimated. This is due to the presence of graft hypertrophy, which has been shown to occur in up to 22% of subjects following ACI with periosteal patch. 30 However, this is not a trackable code and may not have been identified in the present study other than potentially using postoperative chondroplasty as a surrogate for this risk factor for reoperation. This is important to note as periosteal patch is an independent predictor of reoperation following ACI. 26
The total day of surgery payments was significantly higher in the ACI group compared with OCA. The initial higher cost in the ACI group is likely due to initial differences in implant cost. However, this can be institution dependent with a prior study by Everhart et al. 46 demonstrating OCA to have a higher cost compared to ACI at a single academic institution. The same trend continued at 9 months and 2 years with the ACI group having a higher payout compared to the OCA cohort. At these later time points, the increased cost is likely due to the increased reoperation rate seen in the present study following ACI compared with OCA. The autologous chondrocyte implantation was used as the index surgery date with the initial cartilage biopsy not included in cost analysis. Additionally, prior to OCA implantation, many surgeons perform a staging arthroscopy that would not be included in the cost analysis. Therefore, the total cost of both procedures would likely be even higher than reported in the present study, but the cost differences would likely remain the same.
Despite excellent outcomes and improved reoperation rates compared with ACI, the availability of osteochondral allografts internationally remains a concern. 47 This is likely due to cultural and educational differences among the populations with some countries reporting donor rates of only 1.1 per million people. 47 As such, the scarcity of fresh osteochondral allografts in some parts of the world may lead to osteochondral allografts having a higher cost compared with ACI or other cell-based cartilage restoration techniques.
It is important to note that despite the high cost of ACI and OCA, both remain a cost-effective option for the majority of subjects up to 10 years following the index procedure due to significant improvements in patient reported outcome scores. 46 This would continue to hold true even with a 50% increase in the cost of the procedures. 46 However, there is a point in which high reoperation rates make the procedure cost ineffective. Therefore, future research should continue to focus on the risk factors and potential causes of reoperations following ACI and OCA so that surgeons can mitigate this effect.
There are some limitations to this study inherent to all studies that use large databases. The analysis is dependent on the accuracy of the ICD and CPT codes reported. As such, inaccuracies, miscoding, or noncoding by physicians is a potential source of error. Additionally, patients can change insurances and therefore, leave the database. However, this was controlled for through inclusion of subjects with minimum 2-year follow-up. It is also possible that the database is not a true representation of the health care population in the United States. Additionally, the database only included records during a 9-year period from January 1, 2007 to December 31, 2016 so procedures (index or reoperation) that occurred outside that timeframe may have been missed. The current study also only identified complications that occurred within 30 days from the index procedure to increase the likelihood that the complications identified were related to the postoperative course following ACI and OCA and not another medical condition that arose. Thus, late complications that occurred outside the 30-day window were not captured in the present study. Cost analysis is based on the average, per patient total insurer payout per diagnosis at the time of surgery and follow-up time points including reoperations. This may not be representative of all institutions. There is also the limitation of not performing a formal chart review. Inherent to this type of study, there are multiple unknown confounding variables such no direct physical contact, patient reported outcomes, or medical records access to determine diagnosis, prior procedures, meniscus status, chondral defect size, chondral defect location, alignment, and all concomitant procedures.
In conclusion, ACI had significantly higher reoperation rates and cost with similar complication rates compared to OCA. Concomitant osteotomy significantly reduced the risk for reoperation in both groups.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Marc R. Safran has the following disclosures: American Journal of Sports Medicine: Editorial or governing board; Biomimedica: Stock or stock Options; Unpaid consultant; DJ Orthopaedics: IP royalties; International Society for Hip Arthroscopy: Board or committee member; International Society of Arthroscopy, Knee Surgery, and Orthopaedic Sports Medicine: Board or committee member; JISAKOS: Editorial or governing board; Journal of Hip Preservation Surgery: Editorial or governing board; Medacta: Paid consultant; Paid presenter or speaker; Saunders/Mosby-Elsevier: Publishing royalties, financial or material support; Smith & Nephew: IP royalties; Paid presenter or speaker; Research support; paid consultant; Stryker: IP royalties; Wolters Kluwer Health–Lippincott Williams & Wilkins: Publishing royalties, financial or material support; consulting fees from Anika Therapeutics, Linvatec; Linvatec: paid speaker. Geoffrey D. Abrams has the following disclosures: AAOS: Board or committee member; American Orthopaedic Society for Sports Medicine: Board or committee member; Arthrex, Inc: Other financial or material support, educational support; Cytonics Inc.: Paid consultant; Stock or stock Options; Fidia Pharma: Paid consultant; International Society of Arthroscopy, Knee Surgery, and Orthopaedic Sports Medicine: Board or committee member; RubiconMD: Paid consultant; Sideline Sports Doc: Paid consultant; Stryker: educational support; TeachAIDS: Unpaid consultant; Evolution Surgical: educational support; Consulting fees from Cytonics, Fidia Pharma, RubiconMD, and Sideline Sports Doc. Joseph Donahue has the following disclosures: Stabilynx: Stock or stock options; educational support from Arthrex, consulting fees from DePuy Synthes and Medical Device Business Systems, hospitality payments from Evolution Surgical. Constance Chu has the following disclosures: Honoraria from Fidia Pharma. Seth L. Sherman has the following disclosures: ACL Study Group: Board or committee member; American Journal of Orthopedics: Editorial or governing board; American Orthopaedic Society for Sports Medicine: Board or committee member; Arthrex, Inc: Paid consultant, nonconsulting fees; Research support; Arthroscopy: Editorial or governing board; Arthroscopy Association of North America: Board or committee member; Ceterix Orthopaedics: Paid consultant; CONMED Linvatec: Paid consultant; Flexion Therapeutics: Paid consultant; GLG Consulting: Paid consultant; International Cartilage Regeneration & Joint Preservation Society: Board or committee member; International Society of Arthroscopy, Knee Surgery, and Orthopaedic Sports Medicine: Board or committee member; JRF Ortho: Paid consultant; Moximed: Paid consultant; Olympus: Paid consultant; Vericel: Paid consultant, nonconsulting fees, honoraria; RTI surgical: Paid consultant; DJO: grant; Elite Orthopedics: Educational support. Kyle R. Sochacki, Kunal Varshneya, and Jacob G. Calcei declare no potential conflicts of interest.