
Abstract
Objective
The purpose of this study is to systematically review the literature and to evaluate the reported rehabilitation protocols, return-to-play guidelines, and subsequent rates of return to play following cartilage restoration procedures in the knee.
Design
MEDLINE, EMBASE, and the Cochrane Library were searched according to the PRISMA guidelines to find studies on cartilage restoration procedures in the knee, including (1) microfracture (Mfx), (2) osteochondral autograft transfer (AOT), (3) osteochondral allograft implantation (OCA), and (4) autologous chondrocyte implantation (ACI). Studies were included if they reported return-to-play data or rehabilitation protocols.
Results
Overall, 179 studies fit our inclusion criteria, with 48 on Mfx, 34 on AOT, 54 on OCA, and 51 on ACI. The rate of return to play was reported as high as 88.2% with AOT, and as low as 77.2% following OCA, with rates of return to play at the same/higher level as high as 79.3% with AOT, and as low as 57.3% following ACI. The average reported time of return to play was as low as 4.9 months with AOT, and as high as 11.6 months following ACI.
Conclusions
The majority of patients are able to return to play following cartilage restoration procedures in the knee, regardless of surgical procedure utilized. However, while the rate of return to play at the same level was similar to the overall rate of return following AOT, there was a large number of patients unable to return to the same level following Mfx, OCA, and ACI. Additionally, there is wide variety in the rehabilitation protocols, and scant literature on return-to-play protocols.
Keywords
Introduction
Cartilage defects can be debilitating for athletes, causing pain and limiting their ability to participate in high-impact activities, thus leading to unwanted lifestyle modifications. These defects have also been implicated in the progression of early osteoarthritis. 1 While cartilage injuries can initially be treated conservatively, their low potential for healing often necessitates operative management. 2 Options for surgical intervention include simple debridement/chondroplasty, microfracture (Mfx), osteochondral autograft transfer (AOT), osteochondral allograft implantation (OCA), and autologous chondrocyte implantation (ACI), with no current gold standard of treatment.3-6 Surgeons utilize a variety of factors, including the size, location, and chronicity of the chondral defect to select the most appropriate management strategy.
One of the most common questions asked by patients regarding surgery is their ability to return to athletic activities. Multiple studies have reported excellent rates of return to play—a case series by Krych et al. 7 found 88% of athletes to return to sport following OCA; another case series by Mithofer et al. 8 found 96% of adolescents who underwent ACI to return to high-impact sports; a prospective randomized study by Gudas et al. 9 found 93% of athletes who underwent AOT to return to sports; a cohort study by Harris et al. 10 found 83% of professional basketball players to return to play following Mfx. However, there are still gaps in the literature on postoperative outcomes following cartilage restoration procedures. Despite strong evidence suggesting that athletes are able to return to play following cartilage restoration procedures, the optimal postoperative rehabilitation protocol (e.g., commencement of range of motion [ROM], progression of weightbearing [WB] status) or the level of activity that an athlete can ultimately regain remains unclear. Similarly, there are no consensus guidelines or criteria on how to allow for safe return to play.
Therefore, the purpose of this study is to systematically review the literature and evaluate the reported rehabilitation protocols, return-to-play guidelines, and subsequent rates of return to play following cartilage restoration procedures in the knee. We hypothesized that there would be a high rate of return to play following cartilage restoration procedures in the knee, but there would only be moderate rates of return at the same level, and wide variations in rehabilitation and return-to-play criteria.
Methods
Search Strategy and Study Selection
A systematic review was performed—according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines—to summate all existing evidence related to return to play following cartilage restoration procedures along with their respective rehabilitation protocols. Eligibility criteria for this review included all available full-text, peer-reviewed clinical studies of patients undergoing cartilage restoration procedures of the knee in which rehabilitation protocols and/or return-to-play data were reported. Exclusion criteria included non-English studies, review articles, case reports, surgical technique articles, biomechanical studies, and studies involving concomitant procedures that explicitly influenced the rehabilitation protocol.
Screening, eligibility, and inclusion were determined by 2 independent reviewers. The MEDLINE, EMBASE, and Cochrane Library databases were searched from their inception to June 2019 using the following algorithm: ((knee) and ((microfracture or micro fracture or mfx) or (osteochondral autograft or oats or aot or autologous osteochondral) or (osteochondral allograft or oca) or (autologous chondrocyte or aci))). The titles and abstracts of returned results were screened according to the described eligibility criteria. Potentially relevant studies were identified, and the associated full text was reviewed. The reference lists of all relevant studies were screened for any articles that were not identified through the database search. Studies were included based on agreement of both independent reviewers. Any instances of disagreement were resolved through consultation with the senior author.
Assessment of Level and Quality of Evidence
All included studies were evaluated based on criteria outlined by The Oxford Centre for Evidence-Based Medicine, for level of evidence (LOE). 11 The methodological quality of return-to-play guidelines described in each study was assessed based on the criteria outlined by Zaman et al. 12 Each study was evaluated based on a scale from 0 to 4 points. Zero points indicated that the article did not include return-to-play criteria, and 4 points signified well-defined return-to-play guidelines. Studies received 1 point for inclusion of each of the following: a rehabilitation protocol, specific measurements guiding safe return to activity, a timeline for return to full sport or athletic activity, and any objective or subjective conditional criteria that needed to be met before returning to full activity. Instances of scoring discrepancy were resolved through consultation with the senior author.
Data Extraction
Two reviewers independently extracted data in duplicate from the included studies using a predesigned data collection form. Studies were screened and expunged of duplicate patient records. A number of demographic variables (total number of patients, patient age, gender ratio, follow-up time) were recorded when available. Variables related to rehabilitation protocol (time to achieve full ROM, partial WB, and full WB) were also recorded. Finally, variables related to return-to-play (patient-reported timing of return to athletic activity, surgeon-recommended guidelines for allowing athletes to return to full activity, percentage of patients returning to sport or play) were recorded.
Statistical Analysis
Statistical analysis was performed using SPSS (IBM Corp. Released 2013. IBM SPSS Statistics for Macintosh, Version 22.0. Armonk, NY).
Results
Initially, 6579 studies were identified. After removal of duplicates, 3073 studies were further analyzed. After application of inclusion/exclusion criteria, 179 studies were included in the final analysis ( Fig. 1 ).
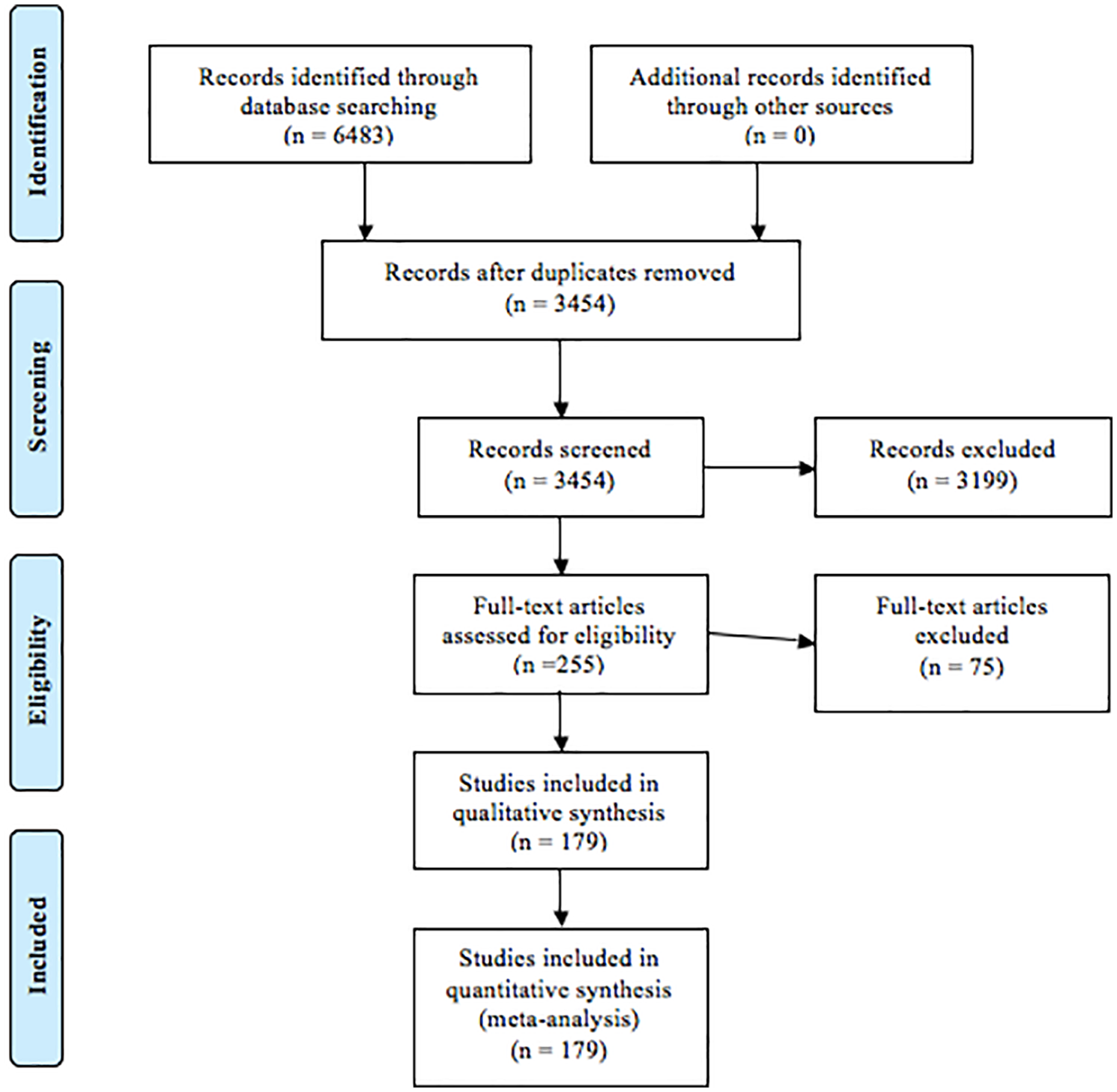
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) figure.
Study Characteristics
Overall, 179 studies (LOE I, 18; LOE II, 14; LOE III, 31; LOE IV, 116) fit our inclusion criteria, with 48 on Mfx, 34 on AOT, 54 on OCA, and 51 on ACI.
Rate and Time of Return to Play
Overall, return to play was reported in 31 studies with 894 patients, and return to play at the same/higher level in 28 studies with 895 patients. The rate of return-to-play was reported as high as 88.2% with AOT, and low as 77.2% following OCA ( Table 1 ). The rate of return to play at the same/higher level was reported as high as 79.3% with AOT, and low as 57.3% following ACI. Timing of return-to-play was reported in 13 studies. The average reported time of return-to-play was as low as 4.9 months with AOT, and as high as 11.6 months following ACI.
Rate and Time of Return-to-Play.
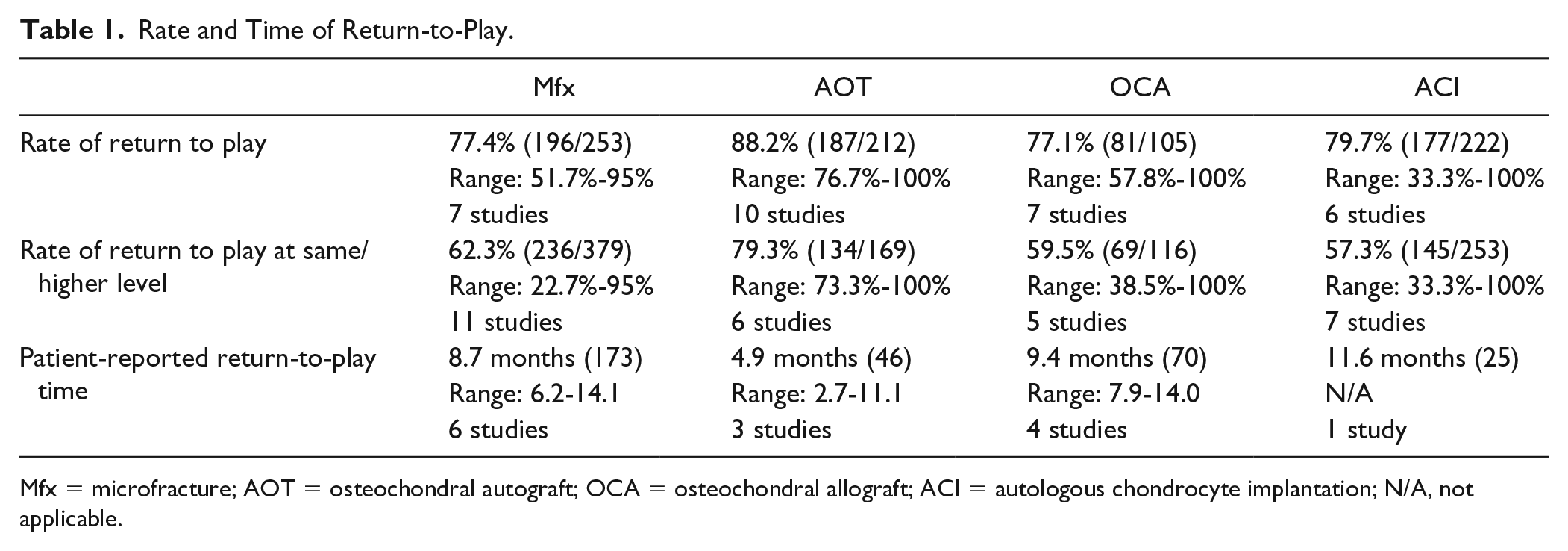
Mfx = microfracture; AOT = osteochondral autograft; OCA = osteochondral allograft; ACI = autologous chondrocyte implantation; N/A, not applicable.
Range of Motion Protocols
The time to commencing ROM was reported in 81.3%-97.1% of studies. The most commonly reported time of commencing ROM was within the first week across all procedures (79.2%-100%), with all procedures apart from OCA having all studies reporting commencing ROM in the first 2 weeks ( Table 2 ).
Range of Motion Protocols.
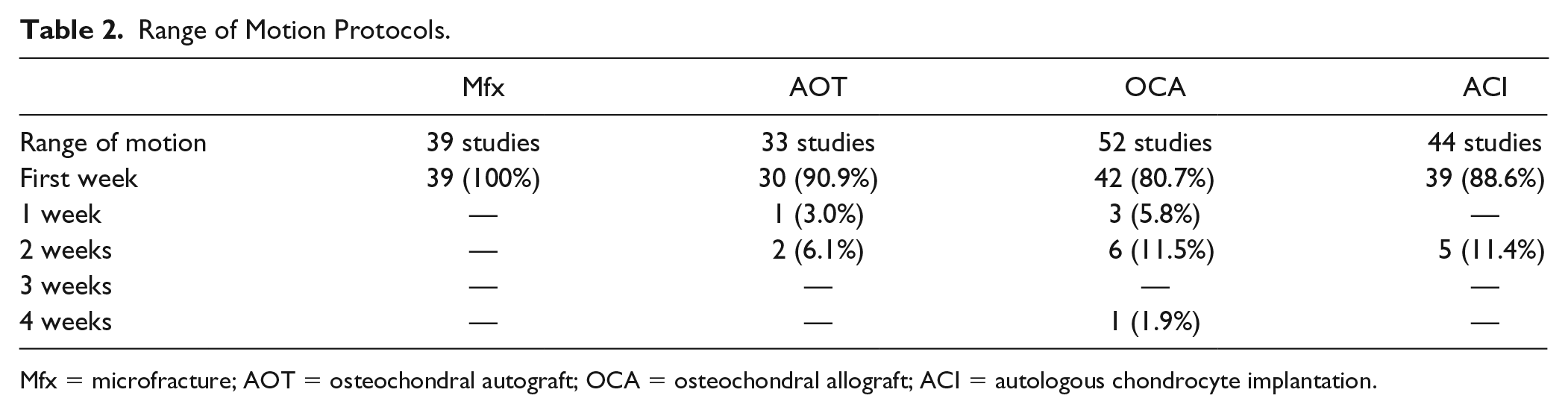
Mfx = microfracture; AOT = osteochondral autograft; OCA = osteochondral allograft; ACI = autologous chondrocyte implantation.
Weightbearing Protocols
The time to WB was reported in 82.4% to 97.9% of studies. The most commonly reported time of commencing partial WB was the first week for Mfx (55.3%) and ACI (40.5%), but 6 weeks for AOT (37.5%) and OCA (31.4%) ( Table 3 ). The most commonly reported time of commencing full WB was 6 weeks postoperatively following all procedures (25%-53.5%), with wide variation in reporting. The majority of studies on AOT (56.7%) and OCA (56.8%) reported no time difference between partial and complete weightbearing, but 6 weeks for Mfx (32.6%) and ACI (39.4%).
Weightbearing Protocols.
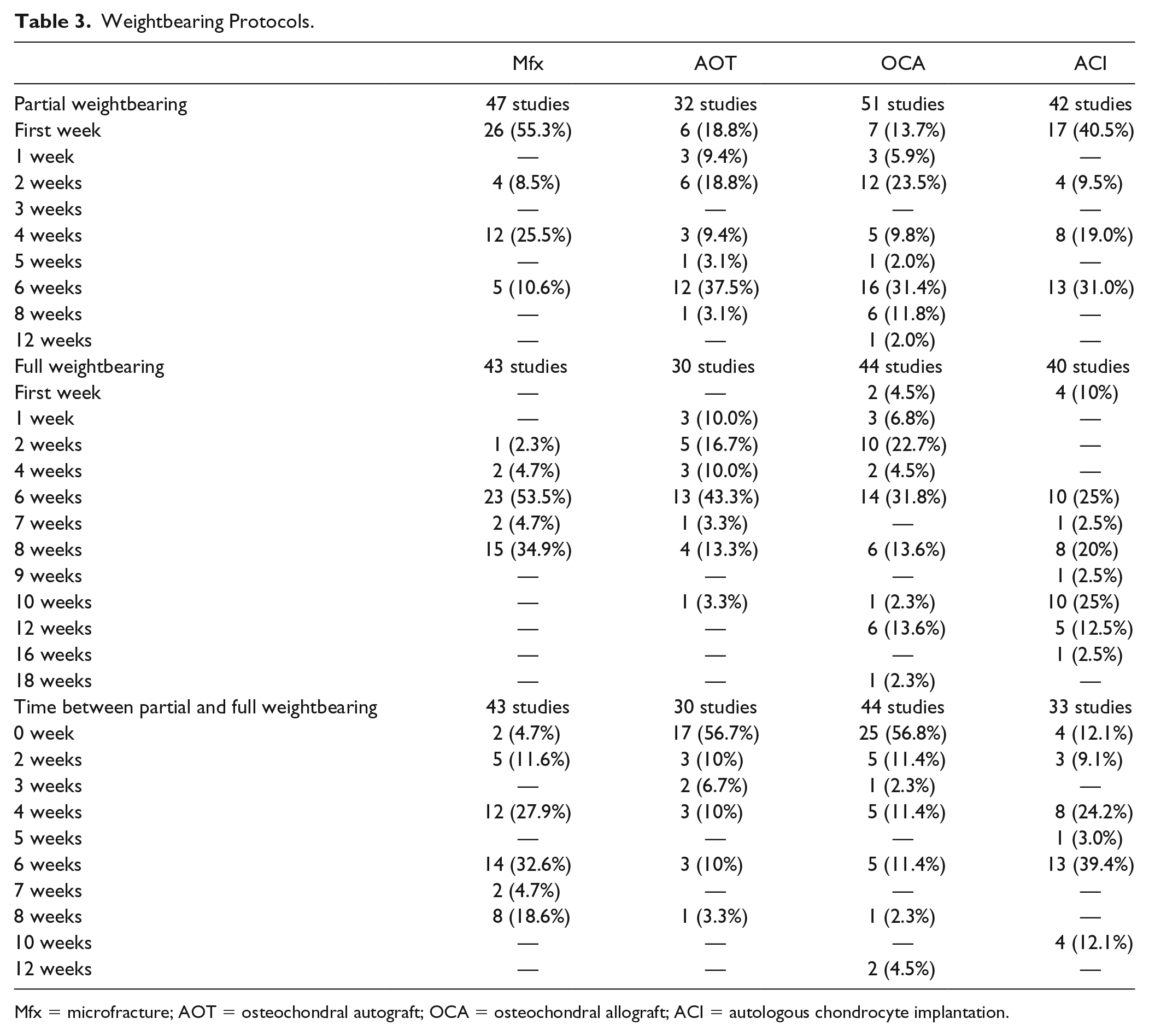
Mfx = microfracture; AOT = osteochondral autograft; OCA = osteochondral allograft; ACI = autologous chondrocyte implantation.
Surgeon Guidelines and Criteria for Return to Play
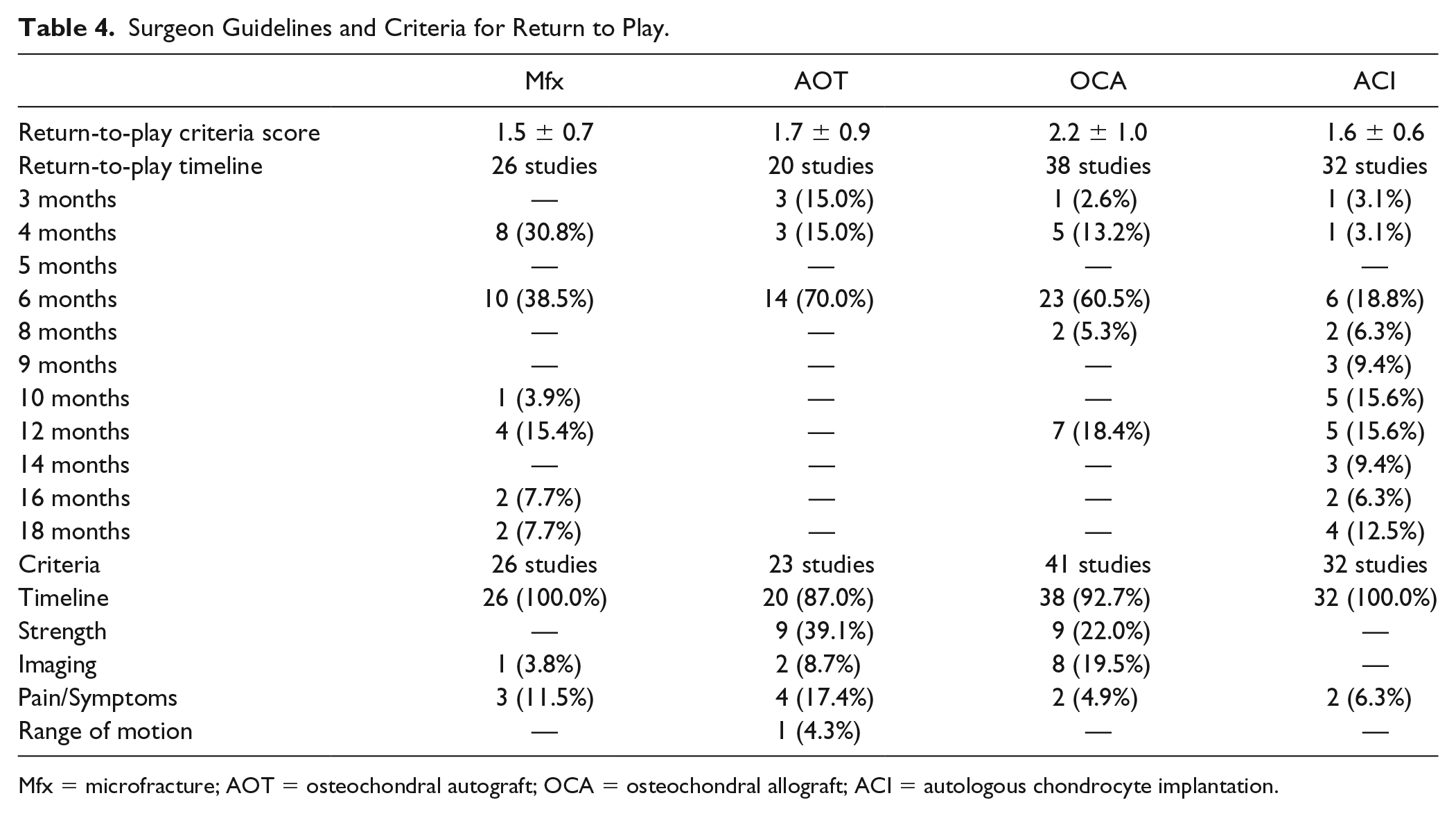
The surgeon guidelines for return to play were reported in 44.8% to 75.9% of studies. The most commonly reported time of surgeons allowing return to full activity was 6 months postoperatively with all procedures, but there is variability on either side of this time point, particularly with ACI. The mean quality of return-to-play criteria score was between 1.5 and 2.2 ( Table 4 ). The other identified criteria for safe return to play were strength, imaging, pain/symptoms, and ROM. The only conditional criteria with objective measures were radiological findings with graft/host integration healing following AOT/OCA.
Surgeon Guidelines and Criteria for Return to Play.
Mfx = microfracture; AOT = osteochondral autograft; OCA = osteochondral allograft; ACI = autologous chondrocyte implantation.
Discussion
The most important finding in our study was that the majority of patients were able to return to play following cartilage restoration procedures in the knee, regardless of surgical procedure utilized. However, when comparing the 4 procedures, there was a discrepancy in patients’ abilities to return to play at their preinjury level of activity. While the majority of patients who returned to play following AOT were also able to achieve their preinjury level of activity, a large number of patients who underwent Mfx, OCA, and ACI were not able to do so. An additional important finding was the extensive heterogeneity among rehabilitation protocols across studies, with scant literature on return-to-play protocols.
Overall, there was a high rate of return to play following cartilage restoration procedures in the knee. Approximately 75% to 90% of patients who underwent a cartilage restoration procedure were able to return to play, with the highest overall rate of return and return to preinjury level of activity following AOT. The rate of return to play at the same level was low following Mfx, OCA and ACI. A cross-sport study by Schallmo et al. 13 found that 78.4% of professional athletes (from the MLB [Major League Baseball], NBA [National Basketball Association], NFL [National Football League], and NHL [National Hockey League]) who underwent Mfx were able to return to professional-level athletic activity, indicating that it is possible for athletes to return to competitive sports following Mfx. 13 Although some of the included studies report high levels of return to preinjury level of activity following OCA and ACI, the cumulative rate is low. It is unclear why these athletes are unable to return—reasons may range from residual symptoms, to a fear of reinjury/prolonged rehabilitation process, to other lifestyle factors. The mean time of return to play ranged between 5 and 12 months, with almost half of the studies allowing patients to return at 6 months (per their protocols). Thus, while patients may have been cleared to play early on, they may require additional time to fully rehabilitate before returning. Furthermore, the longevity of an athlete’s career following return to play, along with the impact of returning to play on the athlete’s knees, remains to be elucidated. However, there is still a concern that resumption of high-intensity activity may negatively affect the cartilage repair tissue, and that this still may prevent the athlete from having a long career on returning. Following MFx, this is of particular concern given the fibrocartilage nature of the repair tissue, as there is evidence that this naturally degenerates over time. 14
The vast majority of studies allowed for the onset of ROM exercises within the first week postoperatively using continuous passive motion, and only 1 study following OCA preventing mobilization within the first 2 weeks. 15 Basic science studies support early resumption of ROM for improved cartilage healing.16-19 For instance, animal studies using continuous passive have shown earlier resumption of ROM results in improved chondrogenesis, proteoglycan and glycosaminogen synthesis in cartilage as well as decreasing collagen breakdown.17,20,21 Additionally, early ROM prevents disuse atrophy and prevents knee stiffness, which improve early postoperative outcomes. 22 However, it remains to be seen clinically whether early resumption of ROM is superior to providing a limited-flexion brace, which is claimed to prevent shear forces in the early postoperative phase. It is also unclear if ROM protocols should differ based on the location of the cartilage lesion (i.e., femoral condyle, trochlea, patella).
There was significant heterogeneity among WB protocols used across the studies, with most allowing some partial WB within the first month. Early WB can be psychologically advantageous following surgery, as it allows for earlier resumption of normal daily activity and encourages progressively increased levels of activity. 23 However, this potential benefit needs to be balanced with protecting the cartilage restoration site as earlier WB may put undue strain on the site and may cause early failure. Based on the analyzed studies, it is still unclear which time point is safest to allow full WB. Interestingly, across all procedures the most common time for full WB was 6 weeks, with the majority of Mfx and ACI studies allowing protected weightbearing initially, but the AOT and OCA studies allowing for rapid progression to full WB at 6-weeks without a period of protected weightbearing. The studies on ACI do, however, report longer wait times before resumption of full WB status. However, Ebert et al. 24 found in a randomized controlled trial that it was safe to resume full WB at 6 weeks compared with at 8 weeks. They used this as the literature standard and found no significant difference at 2-year follow-up. Similar to before, it remains to be seen whether WB protocols should differ based on the location of the cartilage lesion.
There was significant heterogeneity in the return-to-play protocols and criteria following cartilage restoration procedures in the knee, as the majority of studies only utilized time-based criteria for allowing return to play. There was also wide variety in when athletes were allowed to fully return, with a quarter of studies preventing return to play within a year, and approximately two-thirds of studies allowing return within 6 months. While time-based criteria may be useful in determining time taken for healing to occur and/or sufficient rehabilitation to take place, rehabilitation itself is variable and is often patient-dependent. Individualized criteria should be utilized in determining when an athlete is safe to return, similar to guidelines released by The American Academy of Orthopaedic Surgeons regarding anterior cruciate ligament reconstruction rehabilitation. 25 Individualized criteria should include measures such as presence of pain, restoration of full ROM, return of functional strength, ability to perform sport-specific movement, and perhaps radiographic evidence of tissue healing at the site of restoration. Magnetic resonance imaging with T2-mapping and T1-rho may be a useful objective measurement to establish whether the quality of the cartilage healing was sufficiently robust to allow for return to play. 26 Furthermore, magnetic resonance imaging also may assess graft hypertrophy after ACI and its associated potential for graft delamination, which may cause substantial morbidity and revision surgery. Assessment and evaluation of these criteria for safe return to play could have the potential to improve outcomes and patient satisfaction with decreased failure rates.
Limitations
There are limitations inherent to all systematic reviews, including potential biases in the included studies. The majority of the studies having low level of evidence, and retrospective design limit the conclusions that can be drawn from this analysis. It should be noted that technique specific, patient specific, and sport-specific rehabilitation are based on the biology of the cartilage repair procedure are used to guide the clinicians on the rehabilitation protocol, but nuances and variations between patients are not discussed in depth in the included studies. Additionally, there was inconsistent reporting of return-to-play data in the included studies as only 18% of studies reported this. Furthermore, rate and timing of return to play may be influenced by the individuals sport and level of play, thus, the heterogeneity among activities in the included studies likely impairs the ability to generalize the results to all sports. Additionally, it was not possible to assess the impact of location size and lesion on the rate of return to play, due to heterogeneity in reporting. While we were able to exclude studies in which concomitant procedures explicitly affected the rehabilitation protocol, it was not possible to evaluate whether concomitant procedures had an effect on the rate of return to play as some studies underreported concomitant procedures such as treating meniscal pathology or osteotomies.
Conclusion
The majority of patients are able to return to play following cartilage repair procedures in the knee, regardless of surgical procedure utilized. However, while the rate of return to play at the same level was similar to the overall rate of return following AOT, there was a large number of patients unable to return to the same level following Mfx, OCA, and ACI. Additionally, there is wide variety in the rehabilitation protocols, and scant literature on return-to-play protocols.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.