
Abstract
Objective
To investigate intermediate-term clinical results in patients with concomitant anterior cruciate ligament (ACL) reconstruction and chondral defect treated with high-density autologous chondrocyte implantation (HD-ACI) compared to patients without ACL tear but with a chondral lesion and HD-ACI treatment.
Design
Forty-eight patients with focal chondral lesions underwent HD-ACI (24 with ACL reconstruction after an ACL injury and 24 with an intact ACL). Follow-up assessments occurred at 6, 12, and 24 months. Patient-reported knee function and symptoms were assessed using the International Knee Documentation Committee (IKDC) questionnaire, pain was measured using the Visual Analog Scale (VAS), and adverse events were monitored. Physical activity was assessed using the Tegner Activity Level Scale, and cartilage healing was evaluated with the Magnetic Resonance Observation of Cartilage Repair Tissue (MOCART) score.
Results
No significant adverse events occurred during follow-up. Both groups showed significant improvements at 2 years compared to baseline (VAS: 8.0 ± 1.3 to 1.4 ± 2.0 [normal ACL]; 7.4 ± 2.3 to 2.1 ± 2.3 [ACL reconstruction]; IKDC: 39.2 ± 10.6 to 76.1 ± 22.0 [intact ACL]; 35.6 ± 12.1 to 74.6 ± 20.9 [ACL reconstruction]). Patients in both groups exceeded the minimal clinically important difference (MCID) for IKDC scores. The Tegner Activity Level Scale decreased immediately after surgery and increased after 2 years, with 70.6% (normal ACL) and 89.5% (ACL reconstruction) returning to their preinjury activity levels. No significant differences in the MOCART score were observed between the groups.
Conclusions
ACL reconstruction does not appear to reduce the outcomes (at 2 years) of HD-ACI.
Keywords
Introduction
Anterior cruciate ligament (ACL) rupture commonly affects young patients and may lead to functional impairment and instability that will progress to osteoarthritis in the long term.1,2 Usually the injury mechanism of this lesion is knee valgus combined with pivoting moments leading to high shear that will be associated with traumatic chondral injuries in 16%-46%.3,4
Articular cartilage primarily composed of type II collagen fibers possesses a limited ability to repair when damaged. Consequently, when injuries occur, the healing process often leads to the formation of fibrocartilage primarily composed of type I collagen.5,6 This fibrocartilage lacks the biomechanical load-bearing properties inherent in hyaline cartilage. This disparity is correlated to worse outcomes when associated with ACL ruptures, exhibiting a worse prognosis when associated with grade III and IV cartilage injuries.7,8 Management of articular cartilage injuries in the context of ACL insufficiency remains uncertain. 1 While early ligament reconstruction is advised to provide stability and minimize the risk of progression of cartilage injury, the optimal treatment approach for existing chondral pathology remains unclear in these patients. 9 In addition, the outcomes following combined ACL reconstruction and cartilage repair have not been extensively investigated. 4
Treatment for osteochondral defects of the knee includes a wide range of options. 10 This will depend on various factors including the size, location, and severity of the osteochondral defect, as well as the patient’s age, activity level, and overall joint health. 6 Reported management options for osteochondral defects also include nonsurgical approaches such as physiotherapy, which aims to improve joint function and alleviate symptoms.8,10 In addition, fibrocartilage-forming techniques like debridement, curettage, bone drilling, abrasion chondroplasty, and microfracture are used to stimulate the formation of fibrocartilage within the defect, which might progress to future osteoarthritis. 6 Allograft transplantation, autograft transplantation, and (matrix-induced) autologous chondrocyte implantation (ACI) are cartilage-restoration techniques that pretend to give a better outcome to the patient when associated with large chondral defects; however, there are limited data directly comparing each techniques.11,12
ACI has been shown in high-level studies to be an effective and reliable long-term surgical option for articular cartilage regeneration in the knee joint.13,14 Initially, cultured chondrocytes suspended in a liquid medium were injected on the cartilage defect covered by a periosteal flap. Subsequently, a technique named matrix-induced autologous chondrocyte implantation (MACI) was documented. This innovation marked a significant advancement in the realm of orthopedic surgery, introducing a promising avenue for individuals grappling with cartilage injuries. MACI encompassed the process of transplanting cultured chondrocytes onto a specialized matrix, followed by implantation into the affected region of the joint. 4 The results of several studies indicate that MACI can lead to better clinical outcomes and improved knee function compared to microfracture. 4 Furthermore, in specific populations such as professional athletes, treatment with MACI has yielded favorable results. Football players reported good to excellent outcomes after undergoing these procedures, with significant improvements in activity scores and clinical knee and ankle scores following surgery. 15 The findings from these studies highlight the effectiveness and potential superiority of MACI over other treatments in terms of clinical outcomes, structural repair, and improved knee function.
High-density autologous chondrocyte implantation (HD-ACI) is an innovative surgical technique designed to address cartilage defects and promote regenerative healing within damaged joints. 16 The technique involves obtainment of a biopsy of the damaged joint through arthroscopic surgery. The sample is then sent to the cell culture laboratory, where the chondrocytes are cultured for 4-6 weeks and multiplied until reaching 5 million chondrocytes per cm2 of cartilage lesion, after 3 passages. When the culture is ready, a second surgery for implantation is carried out. In this operation, after accessing the knee and exposing the lesion, the latter is carefully cleaned, leaving lesion margins with healthy cartilage. The cells are seeded on a type I/III collagen membrane of porcine origin, previously cut according the shape and size of the defect. The membrane with the cells is placed in the lesion and sutured to the healthy adjacent cartilage. 14
The objective of this study was to investigate the intermediate-term clinical results regarding pain and knee function among patients presenting simultaneous ACL rupture with ACL reconstruction and chondral lesion treated with HD-ACI. This cohort will be compared to patients with normal ACL who underwent HD-ACI after a chondral lesion to assess the differences in outcomes.
Methods
Study Design
This prospective cohort study was designed to compare the clinical outcomes of HD-ACI treatment in patients with or without ACL injury over a 2-year follow-up period. A total of 48 patients were included, with 24 patients in each group. The study received ethical approval from the institution’s ethics committee (Clinica CEMTRO’s Teaching and Research Commission, approval number: 021/19).
Study Participants
To participate in this study, patients should fulfill the following inclusion criteria: (1) to sign a written informed consent, (2) male or female from 18 to 55 years, (3) grade III/IV Outerbridge chondral lesion in the knee diagnosed by an imaging test, (4) 1-3 lesions from 1 to 5 cm2 in size. The exclusion criteria of the study were (1) osteoarthritis, (2) specular lesions on the same side of the femoral condyle and tibial plateau, (3) limb misalignment beyond 10° varus or valgus, (4) allergies to penicillin and/or streptomycin, (5) hypersensitivity to products derived from porcine sources, (6) ongoing infections, tumoral conditions, and systemic diseases like rheumatoid arthritis or other autoimmune disorders affecting the joints. The study enrolled 48 patients who had a chondral lesion and underwent autologous chondrocyte implantation (HD-ACI) for cartilage repair. The ACL injury group comprised 24 patients with both ACL injury and cartilage defects, while the non-ACL injury group consisted of 24 patients with cartilage defects but without an ACL injury.
Surgical Procedure
HD-ACI was performed as previously described.14,17 Briefly, this is a 2-step surgical procedure: The first surgery involves arthroscopy of the knee to assess the chondral lesion and determine its suitability for the chondrocyte implantation technique. Additional procedures such as ACL reconstruction, total or partial meniscectomies, or meniscal suture were performed as needed. All patients with ACL rupture underwent autograft ACL reconstruction with harmstring tendons. During this surgery, a non-weight-bearing area of healthy cartilage was selected to obtain the biopsy (similar to 3-4 rice grain–sized fragments). The biopsy was placed in a sterile tube containing Dulbecco’s Modified Eagle Medium (DMEM) and promptly sent to the laboratory. In the laboratory, the chondrocytes were isolated from the cartilage sample and cultured. After 3 cell passages, which lasted 4-6 weeks, depending on the size of the cartilage defect, the culture reached the adequate number of cells (5 million cells per cm2 of lesion) and was ready for implantation.14,17 The cultured chondrocytes were implanted in a second surgery. During this surgery, access to the lesion was achieved by a paramedical, or a minimally invasive joint incision was made, allowing access to the lesion. The damaged cartilage was cleaned using curettes, and the lesion was debrided, leaving healthy and exposed subchondral bone. The dry type I/III collagen membrane from porcine origin (Chondro-Gide, Geistlich Biomaterials, Wolhusen, Switzerland) was trimmed to the size and shape of the lesion, and the cultured chondrocytes were seeded on the membrane using a sterile pipette, ensuring even distribution over the entire surface. The membrane was placed in the lesion, and the margins were sutured to the healthy cartilage using Vicryl® 5/0 (Ethicon LLC, Puerto Rico, USA). The fixation was reinforced by sealing between the stitches with Tisseel (Baxter S.L., Valencia, Spain). The joint was mobilized to check the stability of the membrane.
Postsurgical Rehabilitation Protocol
Postoperatively, all patients were subjected to a standardized rehabilitation protocol. Patients initiated the treatment with a period of non-weight-bearing lasting 2 months, followed by a phase of functional recovery. Starting at the 4-month mark, they were allowed to participate in weight-bearing activities like cycling and swimming. From 9 to 10 months, low-impact physical activities were permissible, encompassing elliptical training, gym workouts, and walking. By the 12 month of milestone, they were engaged in general physical conditioning and gradually reintegrated into their regular activities based on individual tolerance levels.
Patient’s Follow-Up
Regular follow-up evaluations were conducted at 6, 12, and 24 months after the HD-ACI procedure. During each follow-up visit, the following assessments were performed: (1) subjective perception of knee function and symptoms with the International Knee Documentation Committee (IKDC) questionnaire, (2) pain with Visual Analog Scale (VAS), and (3) adverse effects, such as infections, graft failure, or other complications, that were carefully monitored and documented at 2, 6, 12, and 24 months after surgery. The Tegner Activity Level Scale was employed to evaluate the individual’s physical activity and functional status at several time points: prior to the chondral and/or ACL lesion, at the time of the injury, as well as at 1 and 2 years following the operation. Assessment of cartilage healing at 12- and 24-month follow-ups involved using the Magnetic Resonance Observation of Cartilage Repair Tissue (MOCART) score. To ensure impartiality, the evaluations and monitoring of patients were consistently conducted by the same physician and radiologist.
Statistical Analysis
Because of the limited number of patients who had both ACL rupture and chondral lesions treated with HD-ACI, a convenience sample was employed for this study. This sample encompassed all patients with the mentioned characteristics who underwent a 2-year follow-up. This group consisted of 24 patients, and they were contrasted with an additional 24 patients who solely had chondral lesions treated with HD-ACI. Conversely, with sufficient patients having a chondral lesion without ACL rupture, meeting the required sample size, we randomized eligible participants based on the criteria into two groups: one invited to participate and the other not. Ensuring randomness, we used simple randomization, until reaching 24 patients. Statistical analysis was conducted using IBM® SPSS® Statistics Version 22 (Armonk, NY), and a post-hoc power estimation was carried out with the G*Power 3.1.9.2 software. Continuous variables were summarized as the mean ± standard deviation for normally-distributed variables or as the median for the central tendency measure along with the minimum and maximum values for non-normally-distributed variables. The normality was assessed using the Kolmogorov-Smirnov test. Univariate comparisons were carried out utilizing the Student’s t test for variables with a normal distribution and the Mann-Whitney U test for variables with a non-normal distribution. A repeated-measures analysis of variance (ANOVA) was conducted to examine the changes in pain and IKDC over time, as well as the impact of other factors. Categorical variables were expressed as counts and/or percentages and analyzed in contingency tables using the Fisher’s Exact (2 × 2 tables) or χ2 (remaining tables) tests. A P-value of less than 0.05 was considered statistically significant.
Results
The present study aimed to investigate the outcomes of ACI combined with ACL reconstruction, specifically comparing it to isolated cartilage repair in ligament-intact joints. Table 1 illustrates the fundamental traits of patients from both patient groups. There were no significant variations in terms of age, dominance, laterality, level of sports engagement, or grade of chondral lesion between the two groups. The only statistically significant distinction laid in the distribution of genders, with the proportion of male patients being greater in the reconstructed-ACL group than that in the group with normal ligament (21 vs. 13; P = 0.024; power = 95.2%).
Baseline Characteristics of the 48 Patients Included in This Study Who Underwent HD-ACI Treatment.
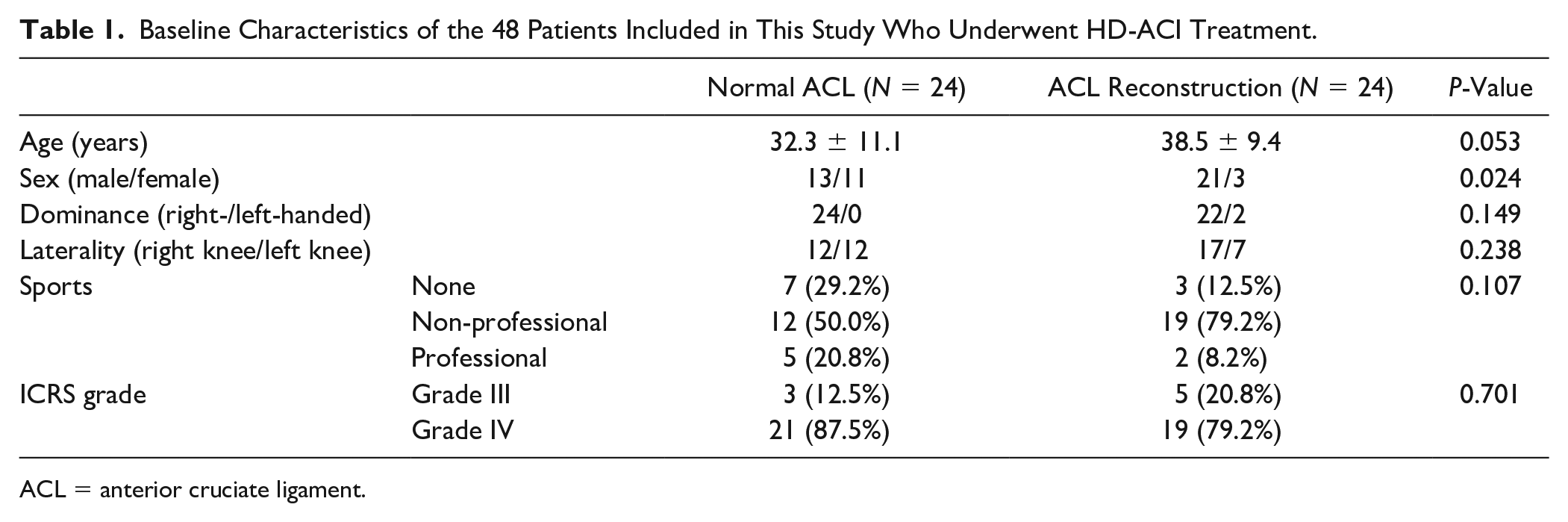
ACL = anterior cruciate ligament.
In the group of patients with ACL reconstruction, 19 individuals exhibited a concomitant meniscus injury, whereas none of the patients without an ACL rupture had this condition. Among those with a meniscus injury, 4 individuals had damage in the lateral meniscus, 10 in the medial meniscus, and 5 in both menisci.
No significant differences were observed in the percentage of patients who had undergone prior cartilage treatment or in the type of treatment received when comparing patients with or without ACL reconstruction (Table 2).
Previous Treatment for Cartilage Lesions Received by Patients From Both Groups, Showing No Significant Differences Between the Two Groups (P = 0.453).
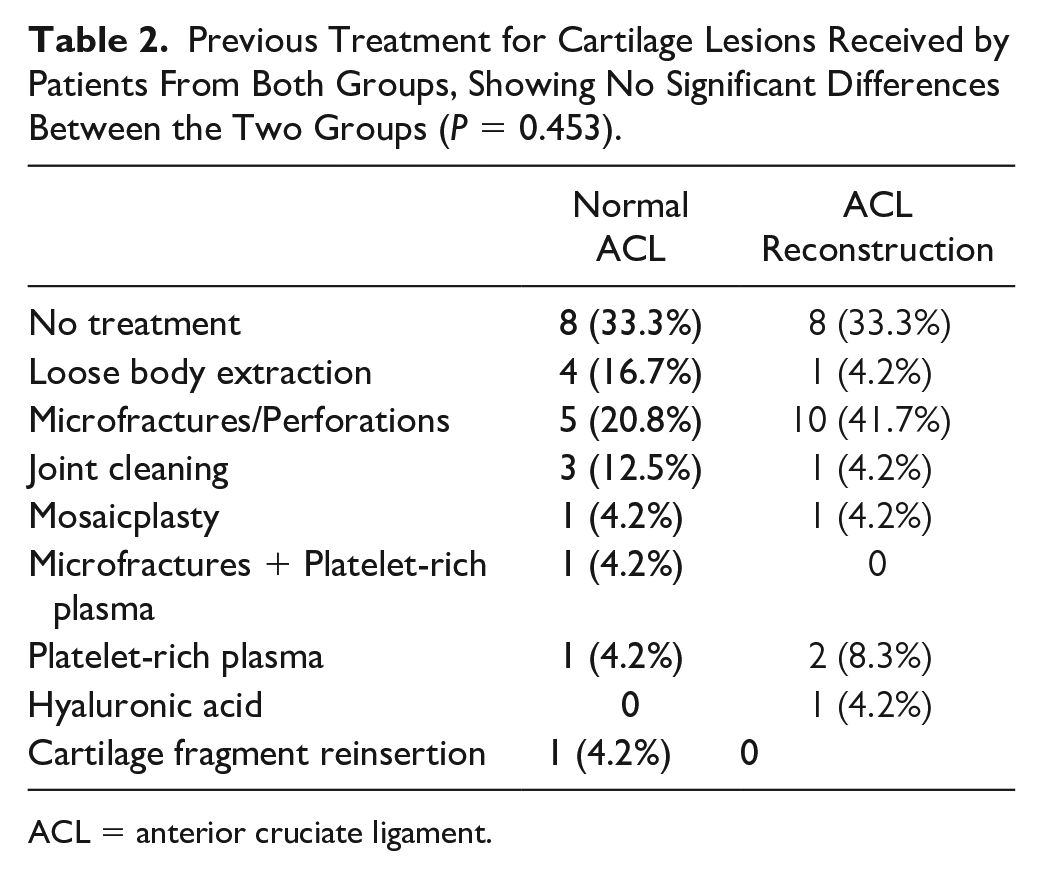
ACL = anterior cruciate ligament.
No significant adverse events were detected throughout the follow-up period, as indicated in Table 3. It is noteworthy swelling emerged as the most common complication observed 2 months after the surgery in both cohorts. While the majority of complications were concentrated in the patient group with concomitant ACL reconstruction, none of the incidents necessitated major interventions; they progressed naturally without the requirement for exceptional measures.
Adverse Events Within Both Cohorts Over the Course of the Follow-Up Period.
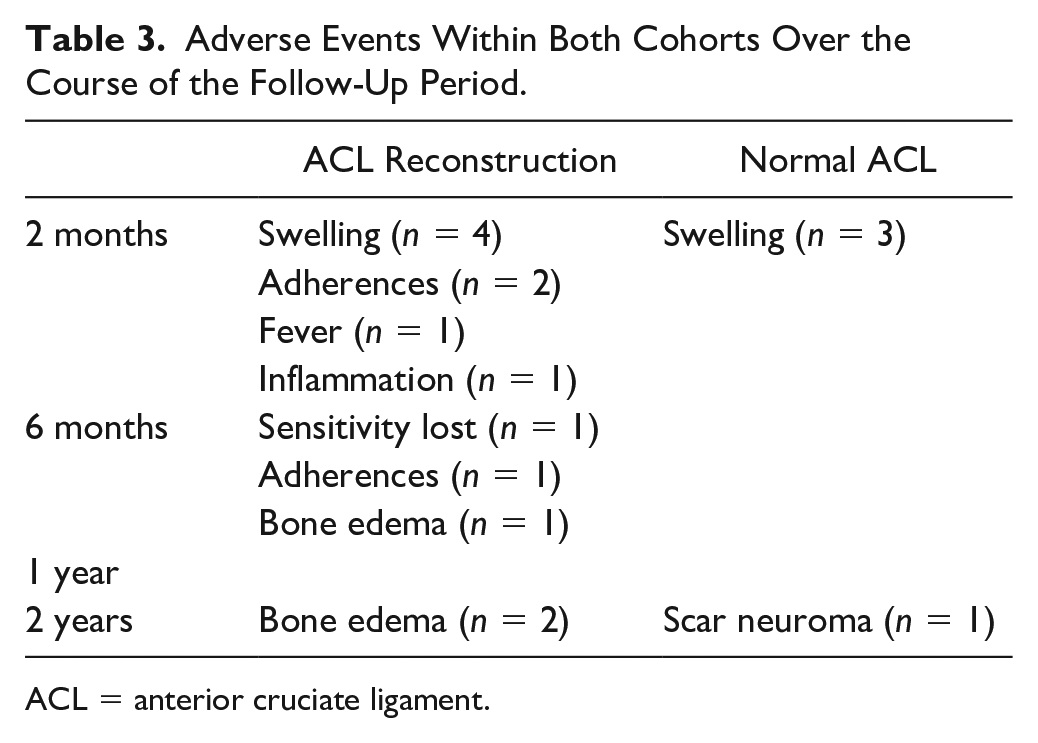
ACL = anterior cruciate ligament.
There were no statistically significant differences in the number of chondral lesions between patients with normal ACL and those with ACL reconstruction (P = 0.550, power = 98.5%): 34 patients had a single chondral lesion (16 patients with ACL reconstruction and 18 with normal ACL), 15 had 2 lesions (7 and 6 patients with or without ACL reconstruction, respectively), and 1 patient with ACL reconstruction had 3 lesions. No differences in lesion size were detected between the two groups either (4.9 ± 1.3 cm² vs. 3.0 ± 1.3 cm², P = 0.181; power = 99.9%, in patients with ACL reconstruction or with normal ACL, respectively). Figure 1 illustrates the distribution of anatomical locations of chondral lesions in the knee among patients with ACL reconstruction and normal ACL. Upon comparison of both groups, no statistically significant differences were detected in terms of anatomical location (P = 0.567; power = 89.1%).
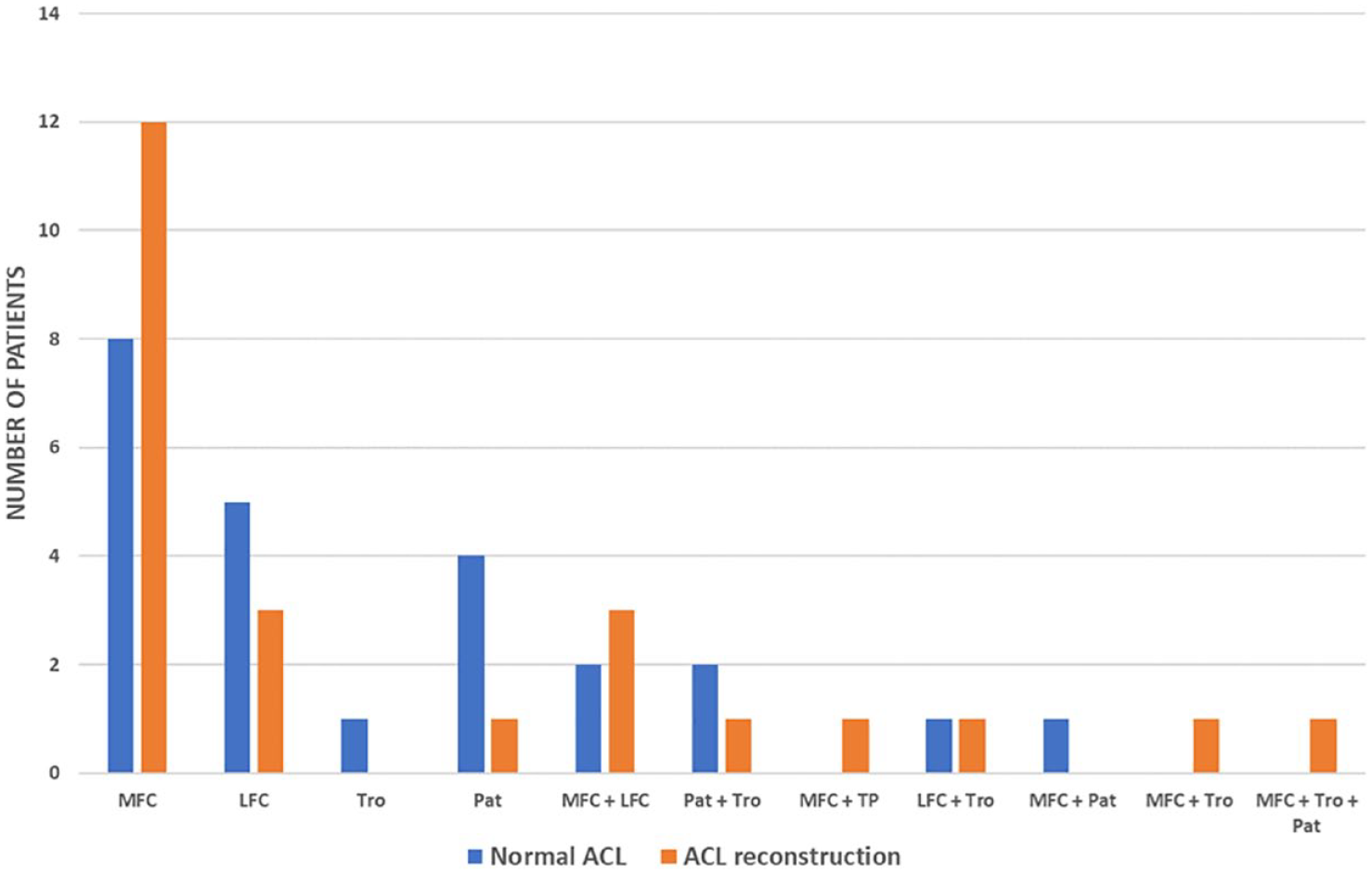
Anatomical location of chondral lesions in both groups of patients. MFC = medial femoral condyle; LFC = lateral femoral condyle; Tro = trochlea; Pat = patella.
Pain, assessed with VAS, exhibited a significant improvement from the baseline value during the follow-up period in both groups (P < 0.001; power = 99.9%). Furthermore, no significant differences between the two groups were identified; neither at baseline nor at 6 months, 1 year, or 2 years ( Fig. 2A ). Conversely, the IKDC value displayed a noteworthy increase from the baseline value throughout the follow-up period (P < 0.001; power = 99.8%). Similar to the VAS results, no statistical differences were observed at baseline, 6 months, 1 year, or 2 years when comparing patients with ACL reconstruction or with normal ACL ( Fig. 2B ). Significantly, the presence of a meniscal lesion had no impact on the patients’ outcomes, either in terms of VAS or IKDC values.
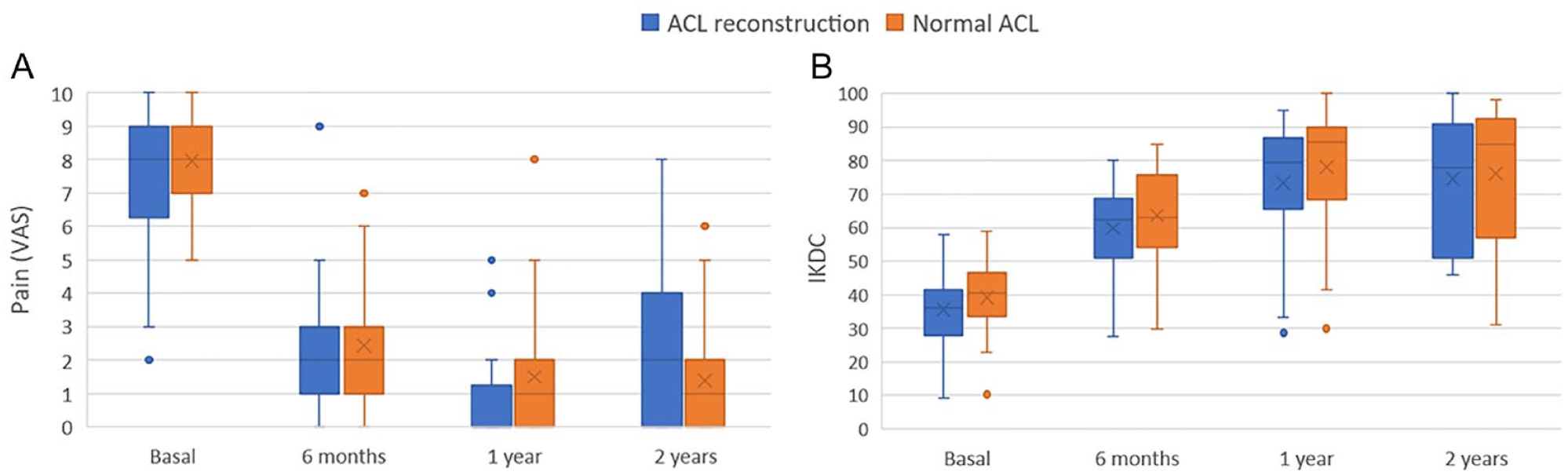
Box plots depicting pain assessed using the Visual Analog Scale (VAS) (
In both groups, patients showed noteworthy improvements in IKDC scores during the 2-year follow-up, surpassing the established minimal clinically important difference (MCID) for this measure. However, there were no statistically significant distinctions observed between patients with normal ACL and those with ACL reconstruction. This observation is depicted in Figure 3 , which illustrates that at all time points (6 months, 1 year, and 2 years), the distribution of IKDC score differences from baseline was significantly higher in both cohorts than the MCID value of 16.7 for IKDC.
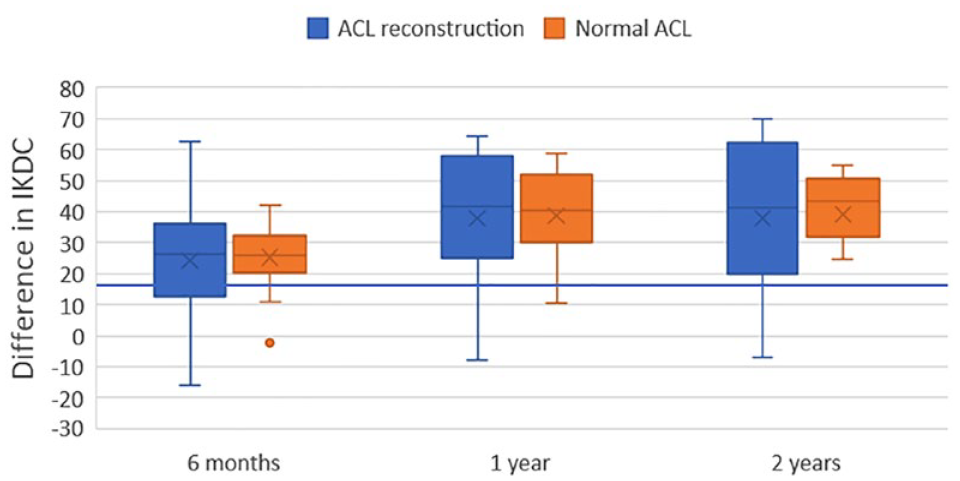
Box plot displaying the difference in IKDC values at 6 months, 1 year, and 2 years relative to the baseline score. A horizontal blue line represents the minimal clinically important difference (MCID) value of 16.7.
Mobility throughout the follow-up period was also studied ( Fig. 4 ). There were no statistically significant distinctions observed between the two groups in terms of extension ( Fig. 4A ) and flexion ( Fig. 4B ). While patients without complete extension displayed minimal fluctuations in both cohorts, the proportion of patients with complete flexion slightly increased over time, albeit without statistical significance.
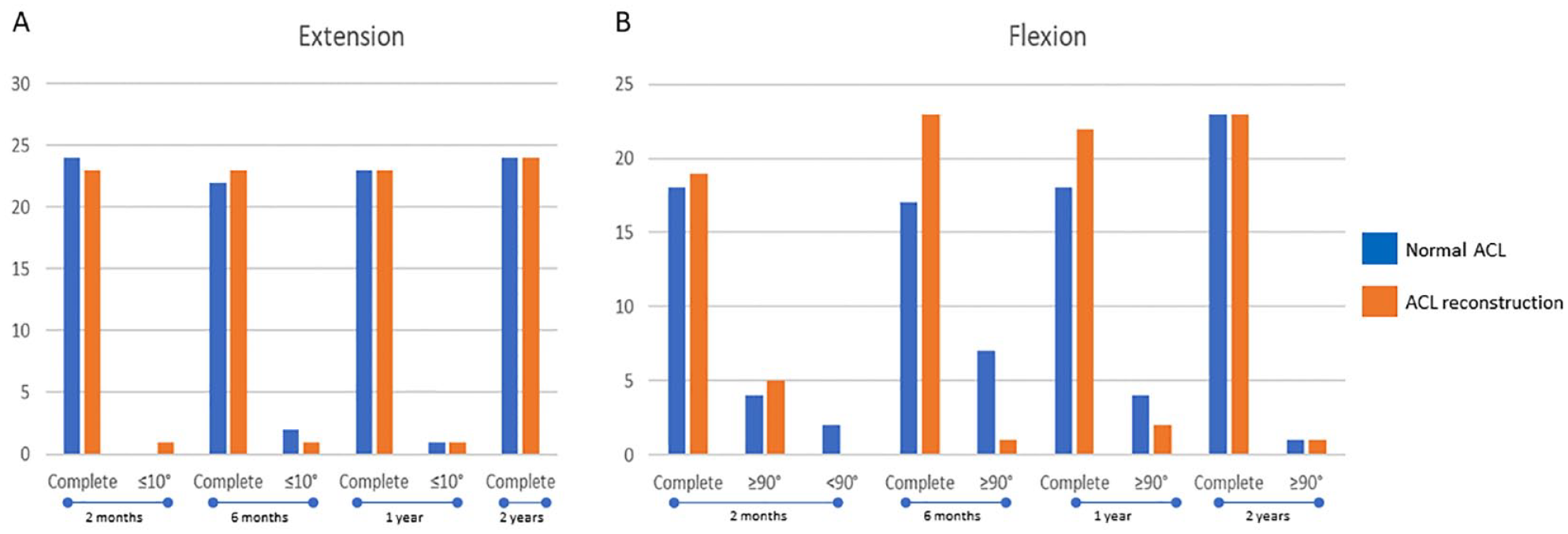
Bar charts depicting the count of patients with varying degrees of extension (
The Tegner Activity Level Scale exhibited a decrease in median values, transitioning from 7.5 to 2.5 for patients with normal ACL and from 6.5 to 3.0 for those with ACL reconstruction, both at the time of surgery ( Fig. 5 ). Figure 5 shows that 1 and 2 years after surgery, nearly all patients returned to Tegner values very similar to their initial ones. Notably, the behavior of this parameter in patients with normal ACL closely paralleled that of those with ACL reconstruction, resulting in no statistically significant differences between the two groups (P = 0.395, power = 99.8%, before the injury; P = 0.766, power = 74.2% at the time of injury; P = 0.471, power = 75.4%, 1 year after surgery; and P = 0.391; power = 81.3%, 2 years after surgery; Fig. 5 ).
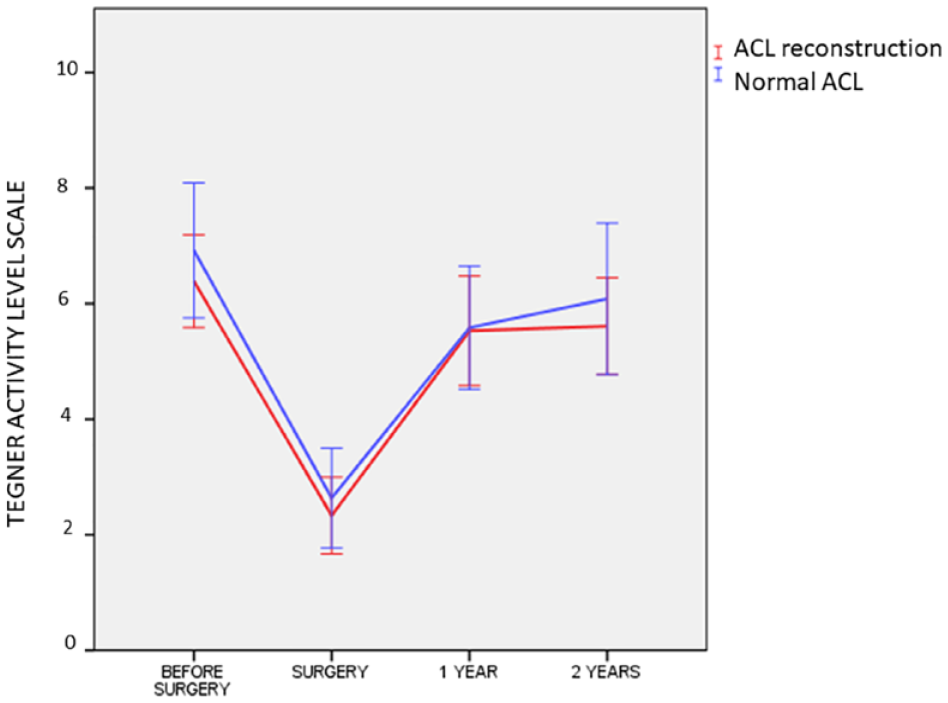
Line chart showing the evolution of the Tegner Activity Level. No statistical differences were found between both cohorts.
Concerning involvement in sports, 17 individuals with normal ACL and 21 with ACL reconstruction regularly engaged in sports at amateur or professional levels prior to experiencing ACL and/or chondral injuries. Table 4 displays the breakdown of patients’ previous sports activity levels and their levels 2 years after surgery. Among the group of patients with normal ACL, 12 out of 17 (70.6%) individuals who participated in sports before the injuries were able to return to sports at the same level. In contrast, this was the case for 17 out of 19 (89.5%) patients with ACL reconstruction, without statistical differences when comparing with the other cohort of patients (P = 0.140; power = 96.4%).
Comparison of Patients’ Sports Levels Before the Injuries With Their Levels 2 Years After Surgery.
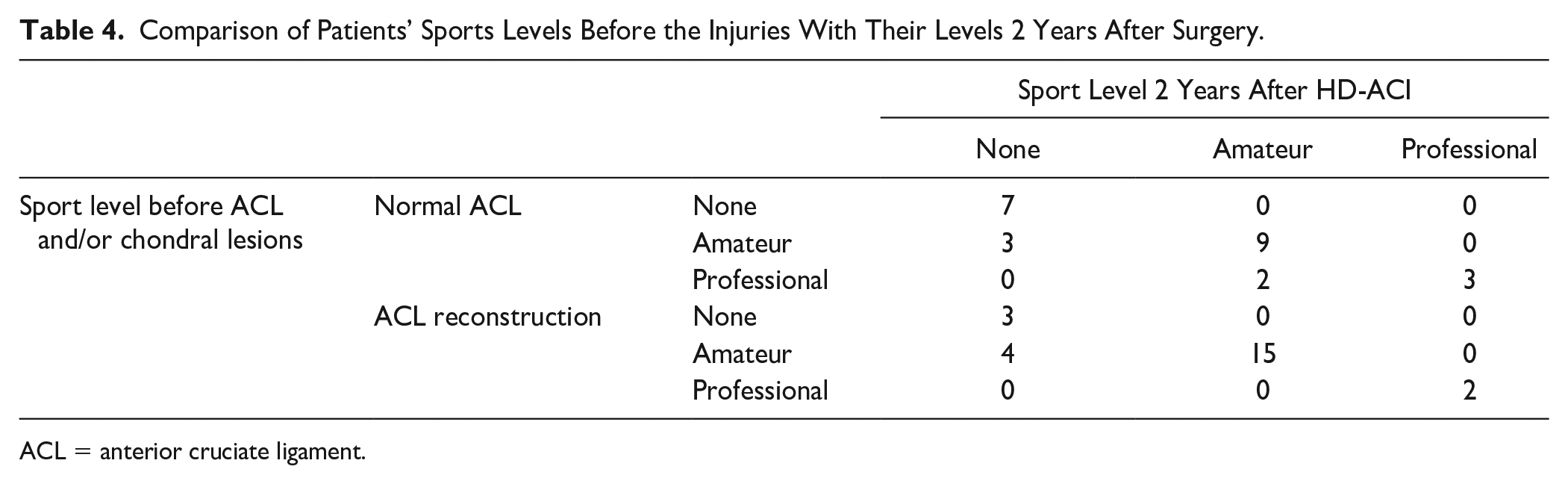
ACL = anterior cruciate ligament.
Regarding the assessment of cartilage repair using MRI analysis, there were no statistically significant differences in the MOCART score. This was observed both when comparing the 1-year and 2-year values and when comparing the two patient cohorts ( Fig. 6 ).
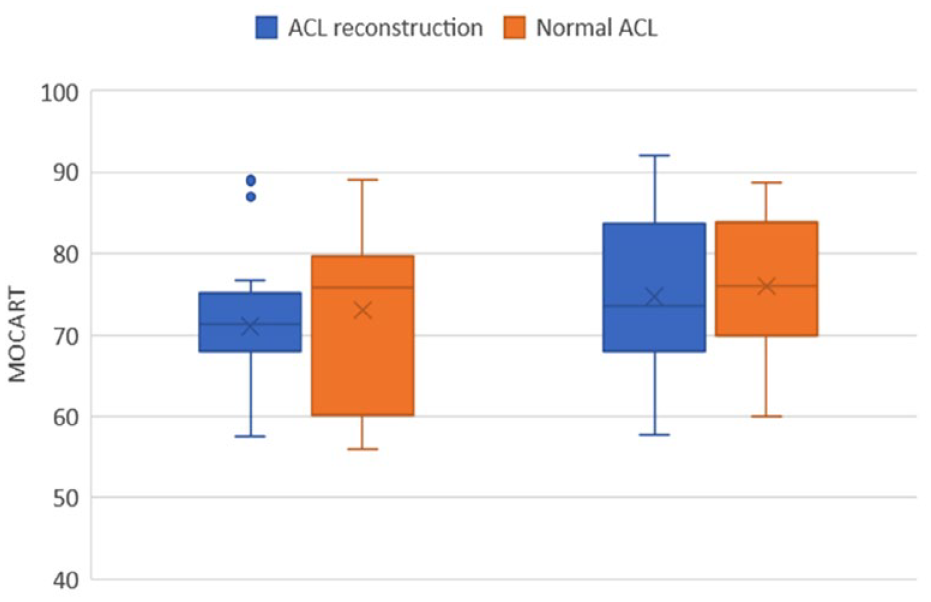
Box plots of MOCART = Magnetic Resonance Observation of Cartilage Repair Tissue score at 1 and 2 years. No statistical differences were found between both cohorts.
Discussion
The present study aimed to investigate the efficacy and safety of HD-ACI for the treatment of articular cartilage lesions in the knee, specifically evaluating the impact of concomitant ACL reconstruction. The findings shed light on the outcomes of HD-ACI in patients with and without ACL tears, providing valuable insights into the effectiveness of this treatment approach. In line with previous research reported by Mehl et al. 4 our results demonstrate a higher percentage of patients with meniscal injury in the group of patients with ACL injury. The coexistence of a chondral lesion with an ACL tear and a meniscus tear within the knee joint is a complex clinical scenario that poses substantial challenges to both patients and healthcare providers. These injuries frequently occur together and need comprehensive evaluation and management to optimize outcomes.9,18-20 This observation underscores the significance of acknowledging the potential presence of simultaneous meniscal injuries and their relevance in the pathophysiological context when devising treatment approaches for ACL tears in the presence of a chondral lesion. However, it is noteworthy that, in our specific case, we did not discover an elevated risk associated with meniscus tears in these patients.
In our study, when comparing patients with and without ACL tears, no statistically significant differences were found in various factors, including the type of previous treatment for cartilage, Outerbridge grade, laterality, anatomical location, number, and size of lesions according with the data presented by Dhinsa et al. 8 This suggests that HD-ACI can be equally effective in patients regardless of the presence of an ACL tear and a subsequent reconstruction. Our study also assessed pain and functionality outcomes using the VAS and IKDC scores. Notably, pain, as measured by VAS, decreased significantly at 2 years in both groups, with no statistically significant difference between patients with and those without ACL tears. This finding indicates that HD-ACI can effectively alleviate pain in patients with articular cartilage lesions, irrespective of ACL tear status and reconstruction. Similar trends were observed in IKDC scores, where both patient groups experienced a significant improvement at 2 years, without significant differences between them. Moreover, the observed improvement surpassed the published MCID for IKDC scores, highlighting the perceived clinical relevance of the improvements achieved with HD-ACI.
Regarding mobility, the proportion of patients with complete mobility (extension and flexion) increased significantly throughout the follow-up period, with no significant differences between both cohorts. As was also found by other authors, this fact suggests that HD-ACI can lead to improved mobility outcomes in both groups, reinforcing its efficacy in restoring joint function. 8
The Tegner Activity Scale holds particular significance in cases involving both ACL and chondral lesions. Research indicates that patients with concurrent injuries typically exhibit lower Tegner scores than those with isolated ACL injuries. 21 This scale serves as a valuable tool for clinicians in evaluating a patient’s potential to return to their preinjury activity level. In the context of this study, the Tegner values exhibited a remarkably consistent pattern, regardless of the presence or absence of an ACL injury. On average, all patients reached Tegner values slightly lower but in close proximity to their baseline levels. This suggests that nearly all patients were able to regain the activity level they had before the injuries and subsequent surgical interventions. Consequently, our findings imply that an ACL lesion does not significantly impact patient recovery and outcomes. To our knowledge, there are no existing studies that track changes in Tegner scores over time to provide insights into the long-term outcomes of individuals with concomitant ACL reconstruction and chondral lesions.
In the present study, a noteworthy proportion of patients from both cohorts successfully returned to sports at their preinjury levels. Interestingly, only 2 professional athletes with normal ACL faced challenges in resuming professional sports participation. The process of returning to sports, whether following a chondral lesion alone or in conjunction with an ACL injury, represents a multifaceted challenge within the realm of sports medicine. Surgical intervention is often considered for individuals with concurrent chondral and ACL injuries, with the choice of surgical approach, whether it involves ACL reconstruction alone or combined procedures addressing chondral lesions, potentially exerting a substantial impact on the ultimate outcomes. 22
Postsurgery rehabilitation, particularly among professional athletes, assumes a pivotal role in facilitating a successful return to sports. Customized rehabilitation programs, encompassing a spectrum of exercises that target range of motion, strength enhancement, and neuromuscular re-education, prove indispensable in achieving favorable results. 23 The decision-making process regarding the return to sports should adhere to well-defined, objective criteria. In addition, psychosocial factors, including apprehension regarding re-injury and the confidence level in the rehabilitated knee, can exert considerable influence on the timeline for resuming sports activities. Consequently, these psychosocial factors should not be underestimated during the recovery process.21,24
Importantly, the HD-ACI safety profile was assessed in our study, revealing that it is a safe technique for the treatment of articular cartilage lesions in the knee, regardless of the presence of reconstruction ACL. No significant differences were observed in the occurrence of serious adverse events between the two groups, further supporting the safety and feasibility of HD-ACI.
In light of these findings, for patients treated with HD-ACI for chondral lesions, the presence of prior ACL reconstruction does not appear to diminish outcomes at the 2-year mark when compared to knees with intact ACLs. As has been also highlighted by other authors, the efficacy and safety of ACI were comparable between patients with an ACL tear followed by ACL reconstruction and those with an intact ACL.1,2,6,25
Overall, our study adds to the growing body of evidence supporting the use of ACI as a viable treatment modality for articular cartilage lesions in the knee. The findings suggest that the presence of an ACL tear and subsequent reconstruction does not significantly impact the outcomes of HD-ACI. Therefore, ACI and particularly HD-ACI can serve as a valuable treatment option, for patients with multiple single or multiple cartilage lesions.
It is important to acknowledge the limitations of our study, such as the relatively small sample size and the lack of long-term follow-up. Post-hoc power estimation for all statistical comparisons indicated a sufficiently high level to ensure the robustness of our findings. However, further research with larger cohorts and extended observation periods is warranted to validate these findings and provide more comprehensive insights into the long-term efficacy and safety of HD-ACI in patients with ACL tear. Another limitation of our study stems from the uniform application of the rehabilitation protocol to all patients, making it difficult to separate its effects from those of the surgical interventions. Moreover, the absence of a control group undergoing only the rehabilitation protocol without surgery hinders the assessment of surgery versus rehabilitation contributions to outcomes. Future research will aim to elucidate the specific impact of the rehabilitation program on clinical outcomes.
In conclusion, for patients with chondral lesions undergoing HD-ACI, the presence of prior ACL reconstruction does not appear to negatively impact outcomes at the 2-year mark when compared to knees with intact ACLs. HD-ACI provides relief from pain, enhances functionality, improves mobility, and yields positive clinical results, particularly in the context of regaining preinjury activity levels and returning to sports. These results underscore the practical value of HD-ACI in healthcare, highlighting its capacity to enhance the quality of life for individuals dealing with knee articular cartilage injuries.
Footnotes
Acknowledgment and Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work has been supported by a grant from Fundación Dr. Pedro Guillén.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.