
Abstract
Objective
The purpose of this study was to evaluate changes in the synovial fluid proteome following acute anterior cruciate ligament (ACL) injury.
Design
This study represents a secondary analysis of synovial fluid samples collected from the placebo group of a previous randomized trial. Arthrocentesis was performed twice on 6 patients with an isolated acute ACL tear at a mean of 6 and 14 days postinjury. Synovial fluid was analyzed by a highly multiplexed assay of 1129 proteins (SOMAscan version 3, SomaLogic, Inc., Boulder, CO). Pathway analysis using DAVID was performed; genes included met 3 criteria: significant change between the 2 study time points using a paired t test, significant change between the 2 study time points using a Mann-Whitney nonparametric test, and significant Benjamini post hoc analysis.
Results
Fifteen analytes demonstrated significant increases between time points. Five of the 15 have been previously associated with the onset and/or severity of rheumatoid arthritis, including apoliopoprotein E and isoform E3, vascular cell adhesion protein 1, interleukin-34, and cell surface glycoprotein CD200 receptor 1. Chondrodegenerative enzymes and products of cartilage degeneration all increased over time following injury: MMP-1 (P = 0.08, standardized response mean [SRM] = 1.00), MMP-3 (P = 0.05, SRM = 0.90), ADAM12 (P = 0.03, SRM = 1.31), aggrecan (P = 0.08, SRM = 1.13), and CTX-II (P = 0.07, SRM = 0.56). Notable pathways that were differentially expressed following injury were the cytokine-cytokine receptor interaction and osteoclast differentiation pathways.
Conclusions
The proteomic results and pathway analysis demonstrated a pattern of cartilage degeneration, not only consistent with previous findings but also changes consistent with an inflammatory arthritogenic process post-ACL injury.
Introduction
Posttraumatic osteoarthritis (OA) is considered to be the consequence of an initial mechanical disruption or injury. The initial acute damage to the joint includes mechanical damage to the tissue itself with elevated expression of catabolic enzymes 1 and inflammatory cytokines and ultimately death of chondrocytes.2-5 The hemarthrosis following anterior cruciate ligament (ACL) injury 6 can further affect cartilage stability and viability. Recently, there has been a renewed focus on the inflammatory milieu and its effects on the ability to repair or restore cartilage after acute traumatic injury. Increased markers of type II collagen turnover and inflammatory cytokines have been detected in the acute phase after injury.7-13
Historically, the principal evidence for the onset of posttraumatic OA has been radiographic joint space narrowing. However, joint space narrowing often takes years to manifest. 14 To better understand the etiology and evolution of posttraumatic OA, a new emphasis has been placed on identifying biomarkers that could be used as objective indicators of the key pathogenic processes or responses to therapeutic interventions. 15 Lattermann et al. 13 recently evaluated the potential to alter chondral breakdown following acute ACL injury through the use of a corticosteroid injection within the first week after injury. Monitoring of the progression of soluble analytes associated with chondral breakdown demonstrated early potentially irreversible cartilage changes after injury (as demonstrated by loss of type II collagen fragments from cartilage within the first 2 weeks after injury). However, as observed for established OA, 16 Lattermann et al. 13 also observed variability in responses to anti-inflammatory treatment after ACL injury. This experience underscores the need to continue to explore potential therapeutic agents to lessen chondrodegeneration following ACL injury and the need to define patient phenotypes that may or may not respond to specific interventions. 15 With this in mind, our long-term goal is to identify potential ACL patient phenotypes that either do or do not respond to early anti-inflammatory treatment. However, to both determine if different patient phenotypes exist and to potentially identify additional therapeutic targets, the proteomic response to acute ACL injury must first be quantified. Proteomic analyses of synovial fluid from patients with idiopathic knee OA have been performed 17 ; however, to our knowledge, the proteomic response after acute ACL injury has not been performed. As such, the purpose of this study was to explore synovial fluid proteome changes to potentially provide insights into mediators of the cartilage degradative process following acute joint injury. We hypothesized that analytes previously associated with idiopathic OA would be differentially expressed following acute ACL injury.
Methods
Study Design
This study represents a secondary analysis of patients with acute ACL tears who participated in an institutional review board (IRB)–approved randomized clinical trial (clinicaltrials.gov: NCT01692756) to assess the efficacy of early anti-inflammatory treatment following ACL injury. 13 The procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000.
While this IRB-approved randomized controlled trial did evaluate the effect of intra-articular triamcinolone acetonide, none of the patients from the treatment group were analyzed for this study. Samples for the current proteomic analysis were selected from among the placebo-treated group who underwent direct joint aspirations and subsequent small volume (10 mL) intra-articular saline injections. Arthrocentesis to dryness was performed on the day of initial presentation (mean = 6 days postinjury, range = 2-8 days) and at a second time point between 6 and 12 days after the initial visit (mean = 14 days postinjury, range = 8-20 days). After arthrocentesis, patients administered 10 mL of normal saline (placebo) at both of the 2 study visits were included in this analysis.
Patient Characteristics
This study involved a subset of 6 patients (3 females, 3 males; mean age 17.5 years, range 16.4-20.4 years; mean body mass index 22.8 kg/m2, range 20-24.4 kg/m2) with acute ACL tears. Study inclusion criteria included the following: isolated ACL injury as determined via clinical exam (positive Lachman test with intra-articular effusion) and validated using magnetic resonance imaging (MRI) examination, age 14 years or older with closed growth plates as visualized on plain knee radiographs, no history of previous traumatic ipsilateral knee injury, occurrence of the ACL injury during sports activity, no clinical evidence of posterior cruciate ligament injury, and no more than grade 1 medial or lateral collateral ligament injury. Exclusion criteria included: onset of injury more than 8 days prior to enrollment, previous ipsilateral knee surgery, intra-articular cortisone injection into either knee within 3 months of injury, or a history of any inflammatory disease.
Preoperative MRI of the knee was used to confirm the absence of concomitant injury as suggested by the clinical exam, and an ACL injury was confirmed intraoperatively at the time of ACL reconstruction. Patients were instructed to avoid any prescription or over-the-counter nonsteroidal anti-inflammatory medications but were encouraged to rest, ice, and elevate the involved knee to control inflammation. All patients had similar self-directed, home-based preoperative rehabilitation, which included quadriceps initiation exercises and passive range of motion.
Proteomic Analyses
Proteomic analysis of the synovial fluid biospecimens was performed using a high throughput and highly multiplexed assay (SOMAscan version 3, SomaLogic, Inc., Boulder, CO). 18 SOMAscan uses aptamers, chemically modified oligonucleotides that recognize the 3 dimensional structure of proteins with high specificity and high sensitivity. Each aptamer, recognizing a specific protein, was tagged with a short DNA sequence enabling quantification using a custom hybridization array. The assay transformed the measurement of proteins into the measurement of the corresponding DNA via hybridization to an antisense probe array using a hybridization gasket slide with 8 microarrays per slide. Data were recorded for each protein as relative fluorescent units (RFU). The median coefficient of variation for the SOMAscan Assay is 5% (somalogic.com/somascan-assay-faqs).
We also assessed changes in specific analytes, measured by the SOMAscan Assay, that have been previously linked to OA: aggrecan, disintegrin and metalloproteinase domain-containing protein 12 (ADAM12), metalloproteinase inhibitor-1 (TIMP-1), and matrix metalloproteinases 1, 3, and 9 (MMP-1, MMP-3, and MMP-9, respectively).19-23 With the exception of TIMP-1 for which decreasing values have been associated with OA changes, increasing values of these proteins would be indicative of greater cartilage breakdown. Lower values of TIMP-1 would also be consistent with a chondrodegenerative process as it has been identified as the primary inhibitor of MMP-1 and -3.
Statistical Analyses
The chondrodegenerative process following acute ACL injury was quantified by comparing biomarker values at the 2 study time points using paired t tests. However, because of the small sample size, we also calculated standardized response means (SRMs) to determine if potentially meaningful trends could be identified. SRM is the pre- to postoperative change divided by the standard deviation of the change scores for that particular variable, with values >0.8 considered large.24-26
Pathway analysis was performed using the Database for Annotation, Visualization, and Integrated Discovery (DAVID Bioinformatics Resources 6.8, National Institute of Allergy and Infectious Diseases, NIH). Genes included in the pathway analyses were those that met all 3 of the following criteria: significant change between the 2 study time points using a paired t test, significant change between the 2 study time points using a Mann-Whitney nonparametric test, and significant Benjamini post hoc analysis. The Gene Functional Analysis Tool was used to identify pathways that were differentially expressed, with Benjamini post hoc analyses performed to account for multiple comparisons.27,28
Results
Analytes Demonstrating Greatest Increases
From among the 1,129 analytes measured (Supplemental Table S1, available in the online version of the article), we identified the 30 proteins that demonstrated the largest change during the first 2 weeks after ACL injury ( Table 1 ). While likely due to the small sample size of this pilot work, large variation in analyte concentrations were observed during the first 2 weeks following ACL injury (SRMs ranged from 1.22 to 4.22); 15 proteins from among these 30 were statistically significantly changed during the first 2 weeks after ACL injury (based on P < 0.05). Interestingly, 5 of the 15 analytes (33%) that significantly increased after ACL injury have been previously associated with the onset and/or severity of rheumatoid arthritis (RA), including apoliopoprotein E and isoform E3, vascular cell adhesion protein 1, interleukin-34, and cell surface glycoprotein CD200 receptor 1 ( Table 1 ). In contrast, only 1 of the 15 significant analytes (ADAM12) has been previously associated with idiopathic OA ( Table 1 ). 29
Thirty Proteins That Demonstrated the Largest SRMs between the 2 Study Time Points Following Acute Anterior Cruciate Ligament Injury. a
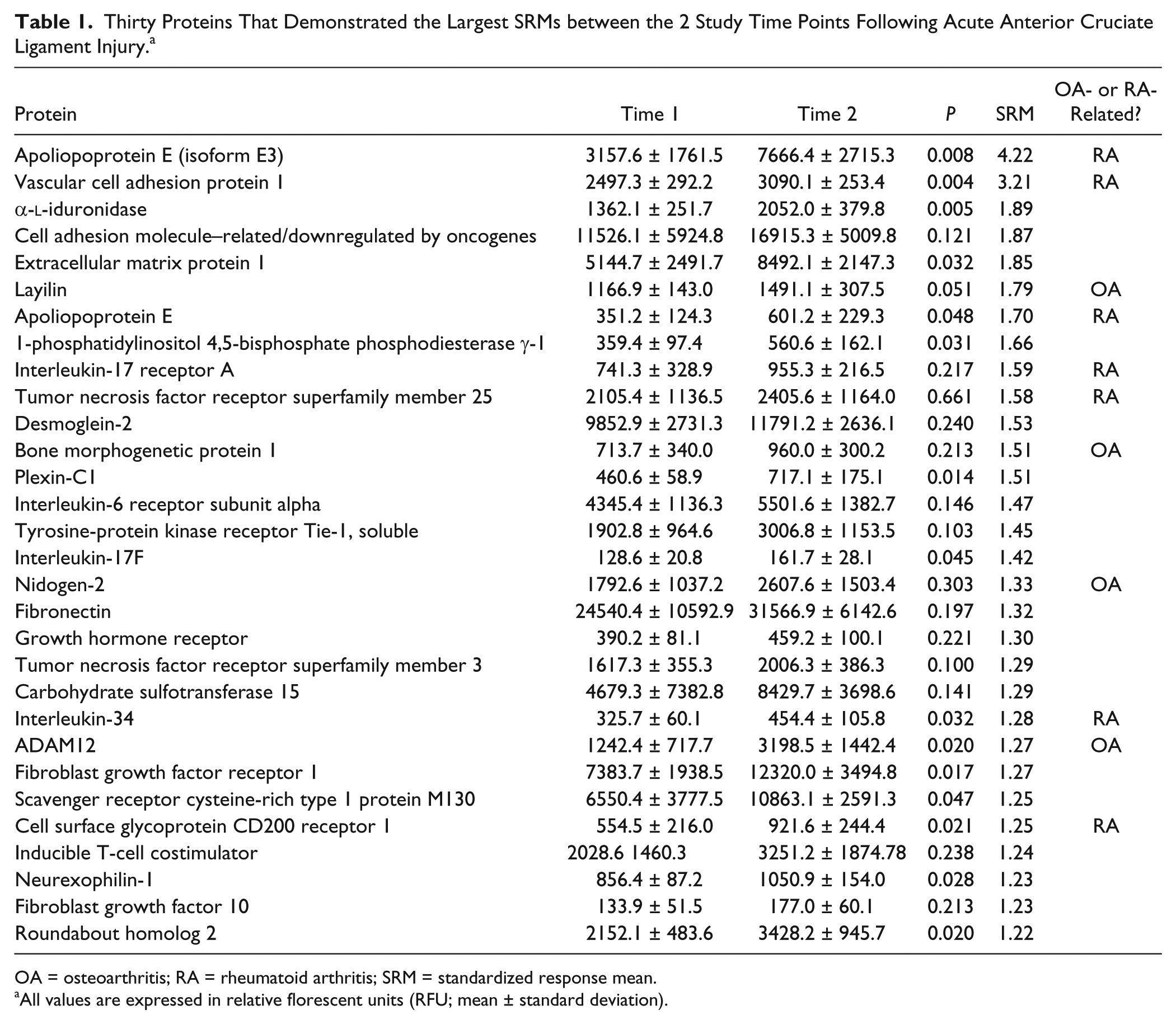
OA = osteoarthritis; RA = rheumatoid arthritis; SRM = standardized response mean.
All values are expressed in relative florescent units (RFU; mean ± standard deviation).
Pathway Analysis
Of the full list of 1,129 protein analytes that were assessed, 83 met the criteria for inclusion in the pathway analysis. The pathway analysis identified the following 8 pathways that were differentially expressed: cytokine-cytokine receptor interaction pathway (P = 0.005, 7 analytes identified in this pathway), phagosome pathway (P = 0.004; 6 analytes identified), hematopoietic cell lineage pathway (P = 0.003; 5 analytes identified), extracellular matrix receptor interaction pathway (P = 0.003; 5 analytes identified), osteoclast differentiation pathway (P = 0.01; 5 analytes identified), natural killer cell–mediated toxicity pathway (P = 0.01; 5 analytes identified), hypoxia-inducible factor 1 (HIF-1) signaling pathway (P = 0.03; 4 analytes identified), and T cell receptor signaling pathway (P = 0.03; 4 analytes identified). Specific analytes associated with each pathway are presented in Table 2 .
Analytes Identified for Each of the Significant Pathways.
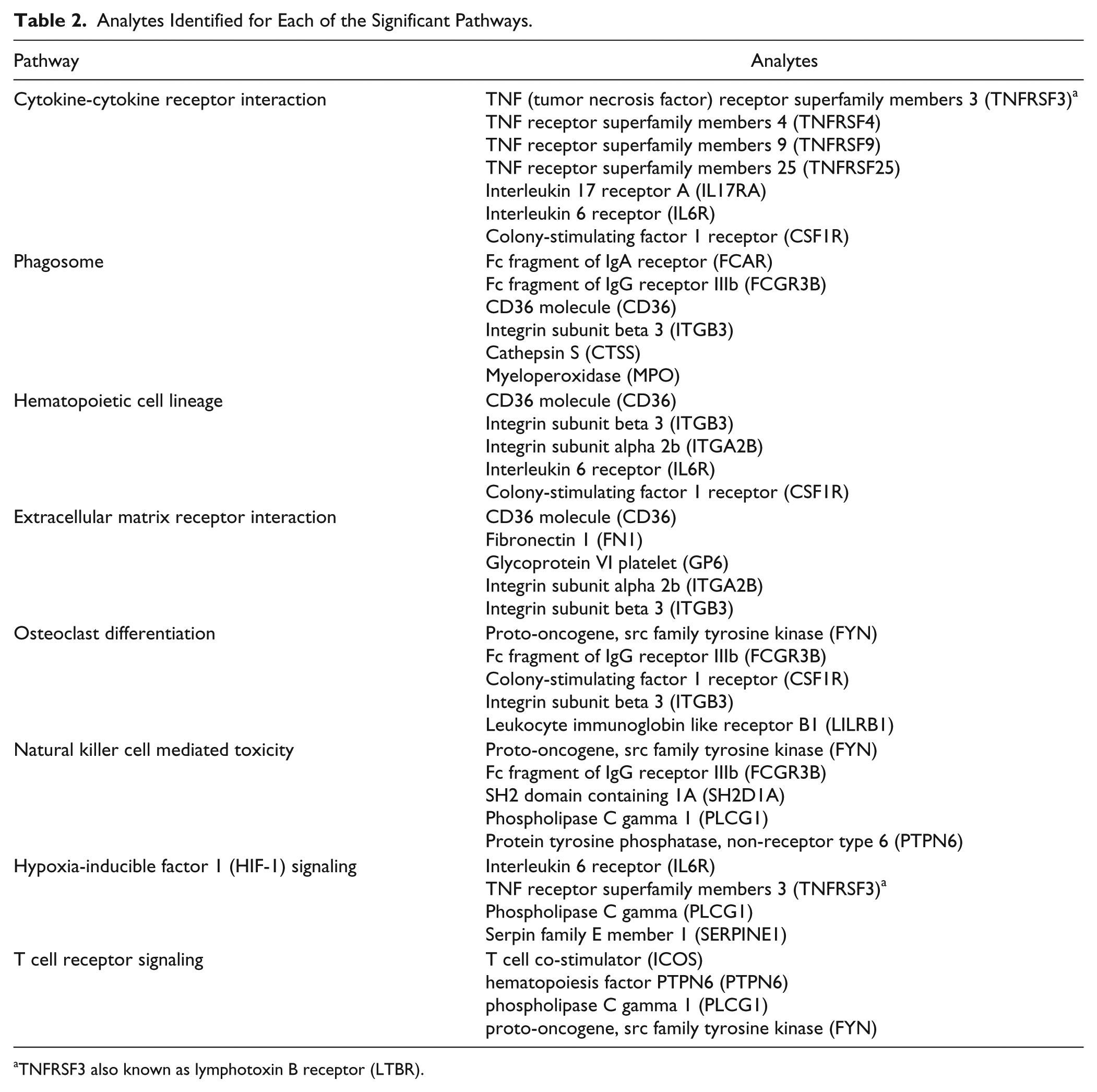
TNFRSF3 also known as lymphotoxin B receptor (LTBR).
Analytes Previously Linked to Osteoarthritis
In addition to the 30 proteins that demonstrated the largest change during the first 2 weeks after ACL injury, we also evaluated 6 biomarkers previously linked to OA ( Table 2 ). TIMP-1, the primary inhibitor of MMP-1 and MMP-3, tended to be downregulated in the first 2 weeks after ACL injury (P = 0.09, SRM = −0.89, Table 3 ). In contrast, chondrodegenerative enzymes and products of cartilage degeneration all tended to increase: MMP-1 (P = 0.08, SRM = 0.88), MMP-3 (P = 0.12, SRM = 1.04), ADAM12 (P = 0.02, SRM = 1.27), and aggrecan (P = 0.06, SRM = 0.89). Interestingly, MMP-9, previously shown to decrease with OA, tended to decrease over the first 2 weeks after ACL injury (P = 0.24, SRM = −0.84).
Osteoarthritis-Related Proteomic Changes Occurring between 1 and 2 Weeks Following Acute Anterior Cruciate Ligament Injury.
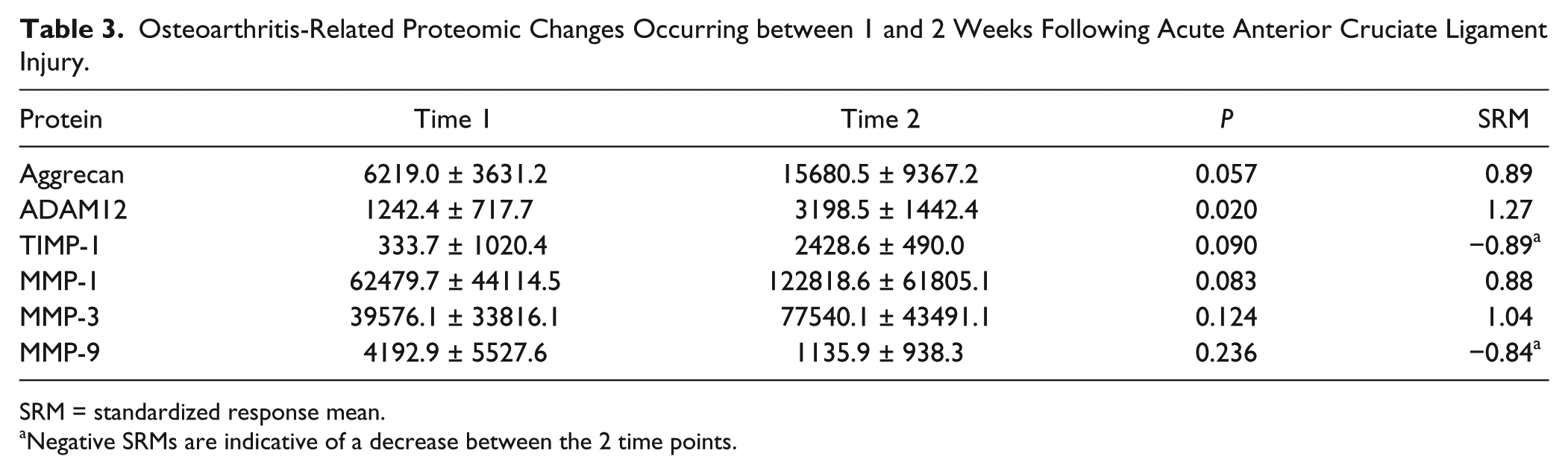
SRM = standardized response mean.
Negative SRMs are indicative of a decrease between the 2 time points.
Discussion
An acute ACL tear has been established as a risk factor for the development of posttraumatic knee OA. Greater than 50% of patients will develop radiographic evidence of posttraumatic OA within 10 to 20 years following ACL injury.30,31 While surgical stabilization of the knee can normalize biomechanics, it does not alone reduce the risk of progressive cartilage degeneration. A critical response to joint injury involves activation of inflammatory pathways; however, prolonged activation of these pathways results in increased biomarkers associated with progressive cartilage breakdown and matrix catabolism.32-34 Elevated inflammatory markers and cytokine concentrations at the time of ACL reconstruction have been reported to be predictive of cartilage matrix composition 3 years after surgery, 35 and biomarker concentrations on the day of surgery may be predictive of patient-reported outcomes 2 years following surgery for female patients. 36
The changes we observed in markers previously associated with cartilage degradation and OA were consistent with prior studies, namely increased synovial fluid aggrecan fragments, MMP-1, MMP-3, and ADAM12 following knee injuries and in early stage OA.32,37 In addition to these results, we were intrigued by the number of RA-related markers that were upregulated following acute ACL injury suggesting that the initial response to injury may have distinct biological pathways in common with RA. Proteins upregulated acutely after ACL injury included apoliopoprotein E and isoform E3, vascular cell adhesion protein 1, interleukin-34, and cell surface glycoprotein CD200 receptor 1. This is perhaps suggestive of chondral breakdown driven by an inflammatory process, not unlike what is seen in the early stages of RA. Others have noted the similarity of early stages of posttraumatic OA and early stages of RA. 38 Both are associated with synovial membrane inflammation with increases in inflammatory cytokines with no radiographic evidence of OA. In RA, this initial response ultimately leads to T and B cell proliferation in the synovium that is not present in OA.
The similarities of RA and posttraumatic OA processes do not extend to the features of stage III RA that include development of a pannus. However, while the B and T cell response and subsequent pannus development are clearly not a part of the posttraumatic OA progression, we have anecdotally noted the presence of an intra-articular film-like membrane during second-look arthroscopy of knees with persistent pain and synovitis that may be suggestive of a persistent inflammatory response following acute ACL injury consistent with a central role of inflammation long after the initial injury ( Fig. 1 ). Taken together, the results of the current study lend further support to the concept of controlling the early inflammatory response to joint injury as a potential chondroprotective strategy.

Second look arthroscopy of a patient not involved in the current study performed 4 weeks after anterior cruciate ligament (ACL) reconstruction. After ACL injury, the patient showed a subacute inflammatory response in the surrounding synovium that can be strictly localized as shown in (
Exploratory Pathway Analyses
Eight pathways were noted to be differentially upregulated. Several pathways, such as the phagosome, hematopoietic cell lineage, extracellular matrix receptor interaction, natural killer cell–mediated toxicity, hypoxia-inducible factor 1 signaling, and T cell receptor signaling pathways, are to be expected as a result of the acute inflammatory response after ACL injury. However, 2 pathways, the cytokine-cytokine receptor interaction and osteoclast differentiation pathways, may have implications for the observed RA-like response and progressive cartilage degradation following ACL injury.
Cytokine-Cytokine Receptor Interaction Pathway
It is not surprising that the cytokine-cytokine receptor interaction pathway is upregulated following acute ACL injury as cytokines play a crucial role in both innate and adaptive inflammatory host defenses, and development and repair processes aimed at the restoration of homeostasis. However, this pathway has been previously linked to many diseases, including juvenile idiopathic arthritis suggesting a role in cartilage degradation and not solely a response to acute injury. 29 Four of the seven analytes belong to the tumor necrosis factor (TNF) family and include TNF receptor superfamily members 3, (TNFRSF3), 4 (TNFRSF4), 9 (TNFRSF9), and 25 (TNFRSF25). Interleukin 17 receptor A (IL17RA) was also upregulated and is involved in the pathogenesis of inflammatory and autoimmune diseases including RA. 29
Cytokine concentrations in the synovial fluid early after ACL injury have been associated with degenerative cartilage changes over the ensuing three years. 35 OA is a chronic, inflammatory condition with monocytes and macrophages acting as mediators in the cycle of cartilage degradation in knee OA.39,40 Synovial macrophages activated by proinflammatory cytokines as a result of cartilage breakdown produce proinflammatory cytokines, which then activate chondrocytes and production of MMPs, thereby creating a cyclical process of cartilage degradation. 39
As such, it is particularly noteworthy that four protein analytes in the TNF family were upregulated following acute ACL injury. Genes in the TNF family have been previously associated with both RA and OA,41,42 and this may be a potential therapeutic target. Corticosteroids have been demonstrated to reduce markers of type II collagen breakdown following acute ACL injury 13 ; and it may be the underlying ability of corticosteroids to modulate macrophage function that is causing the reduction in collagen breakdown. Acute injury initiates a cascade of activity, including activation of synovial macrophages and increased concentrations of TNF-α and other proinflammatory cytokines, which thereby results in increased markers of type II collagen turnover in the acute phase after injury.7-13 Intra-articular corticosteroids have demonstrated the ability to disrupt this cycle by lessening TNF and cytokine concentrations in chronic arthritis, 43 albeit transiently.
Osteoclast Differentiation Pathway
While OA progression has been linked to the innate immunologic response, OA progression is also potentially affected by cross-talk between the cartilage (chondrocytes) and subchondral bone (osteoclasts and osteoblasts). 44 Not only does ACL injury result in an intraarticular inflammatory response, there is also substantial injury to the subchondral bone. So-called “bone bruises” in the proximal tibia and distal femur are commonly found in combination with ACL injury.45-47 There are conflicting reports as to whether these bone bruises resolve over time,46,47 but other characteristics, including bone mineral density, bone mass, and bone content, are all altered after ACL injury and do not return to preinjury status even years after injury.48,49 Furthermore, bone bruise volume in the lateral compartment shortly after ACL injury has been associated with cartilage degradation during the first 2 to 3 years after injury. 46
In our study, colony-stimulating factor 1 receptor (CSF1R) was upregulated after ACL injury (P = 0.04, SRM = 1.16). Bone bruises were present on preoperative MRIs for all 6 patients and, while not statistically significant because of the small sample size (P = 0.16), there was a positive correlation between the volume of preoperative bone bruises in the lateral compartment and the change in CSF1R between the 2 study time points (Spearman’s ρ = 0.66). CSF1R is involved with both the cytokine-cytokine receptor interaction and osteoclast differentiation pathways. CSF1R is a cytokine that controls the production, differentiation and function of macrophages and osteoclasts. 35 Importantly, CSF1R has been known to be involved in transmembrane signaling in both bone marrow and blood mononuclear cells and as such, could potentially play a role in both innate immunologic and subchondral bone mechanisms of OA progression. 35 Synovial CSF1 expression has been demonstrated to be significantly greater for both RA and OA patients that controls. 50 CSF1R is expressed by synovial macrophages activated by TNF; CSF1R also differentially regulates MMP expression, osteoclast differentiation, and TNF-induced osteolysis, and thereby appears to have an essential role in cartilage degradation.50-52 Recent animal model results suggest that blockade of CSF1R may suppress the synovial inflammatory response 50 ; this highlights the need for future studies to aid in determining optimal early interventions for minimizing cartilage degeneration, and hopefully the incidence of PTOA following acute knee injuries.
This preliminary study was exploratory in design and thus, not without limitations. An a priori power analysis was not used to justify the sample size. The sample size was small consisting of only 6 relatively young patients (mean age of 17.5 years) thereby limiting the conclusions that can be drawn and whether the results can be generalized to older patient populations. The development of OA and the progression of articular cartilage damage after ACL injury and reconstruction are undoubtedly multifactorial in nature. Several factors, including patient age, body mass index, and treatment of the menisci, have been associated with progressive articular cartilage changes. 53 While the onset and progression of posttraumatic OA after ACL injury are multifactorial, elevated inflammatory markers and cytokine concentrations at the time of ACL reconstruction have been reported to be predictive of cartilage matrix composition 3 years after surgery, 35 and biomarker concentrations on the day of surgery are predictive of patient-reported outcomes 2 years following surgery for female patients. 36 The current analyses address the biologic factors potentially associated with posttraumatic OA progression. The samples subjected to proteomic analysis were limited to 2 very early time points, but nevertheless demonstrate the feasibility and utility of proteomic analyses of synovial fluid. The combination of our current proteomic results and previously reported synovial fluid biomarker results highlight the need for additional studies to determine if progression of posttraumatic OA after ACL injury is driven by an inflammatory process represented by the autoimmune arthropathy as in rheumatoid arthritis, or switches to a subacute innate immune inflammatory arthropathy represented by idiopathic OA. A better understanding of the underlying mechanisms of posttraumatic OA progression may then yield novel treatments to lessen the burden of posttraumatic OA after acute ACL injury. These data may also contribute to identification of pharmacodynamic biomarkers to quantify treatment efficacy, and data with which to estimate adequate power in future studies.
Conclusions
In conclusion, the proteomic results demonstrate a pattern of biomarker expression following ACL injury that was indicative of articular cartilage degeneration. To our knowledge, this is the first clinical study to assess proteomic changes following acute ACL injury. We found that the protein responses postinjury were similar in direction to those previously reported with knee OA. The proteomic analysis also revealed large post-injury increases in RA associated markers, and differential upregulation of the cytokine-cytokine receptor interaction pathway that is closely associated with inflammation. These results not only concur with other recent studies that have reported that the chondrodegenerative process begins early after acute ACL injury12,13,54 but also provide unique insights into potential therapeutic targets.
Supplemental Material
Additional_File_1 – Supplemental material for Joint Fluid Proteome after Anterior Cruciate Ligament Rupture Reflects an Acute Posttraumatic Inflammatory and Chondrodegenerative State
Supplemental material, Additional_File_1 for Joint Fluid Proteome after Anterior Cruciate Ligament Rupture Reflects an Acute Posttraumatic Inflammatory and Chondrodegenerative State by John D. King, Grant Rowland, Alejandro G. Villasante Tezanos, James Warwick, Virginia B. Kraus, Christian Lattermann and Cale A. Jacobs in CARTILAGE
Footnotes
Acknowledgments and Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received funding from The Arthritis Foundation of America. Research reported in this publication was supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases of the National Institutes of Health under Award Number 5K23AR060275 and was supported in part by pilot awards from NIH NICHD National Center for Medical Rehabilitation Research (R24HD050846), and the Clark Charitable Foundation. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. Data collection and study administration was supported by the University of Kentucky CTSA award (UL1TR000117).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the University of Kentucky Institutional Review Board (Protocol #12-0706).
Informed Consent
all subjects consented prior to study participation.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.