
Abstract
Objective
This study aimed to assess the clinical and radiographic outcomes of juvenile patients who suffered from stage II or III osteochondritis dissecans (OCD) of the knee and underwent arthroscopic retrograde drilling and internal fixation with bioabsorbable pins.
Design
Medical and radiological records from patients aged 11 to 16 years, who underwent arthroscopic treatment for OCD lesions of the knee in 2 tertiary hospitals, were retrospectively reviewed. The procedure was indicated by persistent pain and by magnetic resonance imaging (MRI). All patients underwent retrograde drilling and arthroscopic fixation of the lesion with bioabsorbable pins. MRI was conducted at least 1 year postoperative in all patients to evaluate healing. Functional outcomes were evaluated through the Visual Analogue Scale (VAS) for pain, Lysholm, and IKDC (International Knee Documentation Committee) scores.
Results
A total of 40 patients, with an average age of 13.1 years (range = 11-16 years) and an average follow-up of 6.6 years (range = 3-13 years) were reviewed. MRI findings confirmed the healing of the lesion in 36 out of the 40 (90%) patients. In particular, the healing rate was 95% (20/21) and 84% (16/19) for stage II and stage III, respectively. Lysholm, IKDC, and VAS scores revealed a statistically significant improvement (P < 0.05) at final follow-up in comparison to preoperative status. No infection, knee stiffness, or other complication was recorded.
Conclusions
Retrograde drilling combined with internal fixation with bioabsorbable pins, of stages II and III OCD lesions of the knee provides good to excellent outcomes to juvenile patients, with a high healing rate.
Introduction
Osteochondritis dissecans (OCD) of the knee is an idiopathic pathologic process characterized by a focal alteration of subchondral bone structure that causes knee pain and dysfunction. Its prevalence is estimated to be 15 to 29 per 100,000 population.1-3 Young athletes are usually affected, while boys are at 3.8 times higher risk for developing OCD.4,5 The most common site of the injury is the medial femoral condyle, on its posterior aspect.6,7 Pain on weight bearing is the predominant symptom in around 80% of the cases. 8 Following clinical evaluation, magnetic resonance imaging (MRI) is the most useful investigation in OCD.9-11 Prognosis of the disease is highly dependent on the skeletal maturity of the patient. However, early diagnosis and treatment are essential for every patient to prevent further cartilage destruction and knee function.
Treatment options vary and include both operative and nonoperative treatment. Conservative treatment is the preferred means of treatment for stable lesions in juvenile patients.12,13 Surgical management is reserved for cases with severe lesions, such as grades III and IV, and for those that fail conservative treatment. Antegrade and retrograde drilling, microfracture methods, loose body and fragment removal, and internal fixation are some of the operative techniques used.14-17 Autologous chondrocyte implantation is mainly used for unsalvageable fragments.18,19 When stability is in doubt, then fixation is necessary. Historically, these lesions were treated with fixation with metallic, nonabsorbable implants, such as Herbert screws and cannulated screws.20-23 However, the use of these implants has been associated with complications, such as implant migration or breakage. 14 Subsequently, fixation with bioabsorbable screws is gaining attention during recent years. Nevertheless, there are few studies available in the literature evaluating clinical and radiological outcomes after fixation with absorbable pins.17,24 Furthermore, comparative studies between different stages of OCD using this type of fixation have not been reported yet.
The purpose of the present study was to assess the clinical and radiographic outcomes of juvenile patients who underwent retrograde drilling and internal fixation with bioabsorbable pins of stage II and stage III (based on Guhl classification) OCD of the knee, and evaluate if this method is effective in these both types of OCD. Our hypothesis was that retrograde drilling and arthroscopic fixation with bioabsorbable pins could result in a high healing rate along with satisfactory clinical and radiological results and therefore could be successfully applied in these patients.
Methods
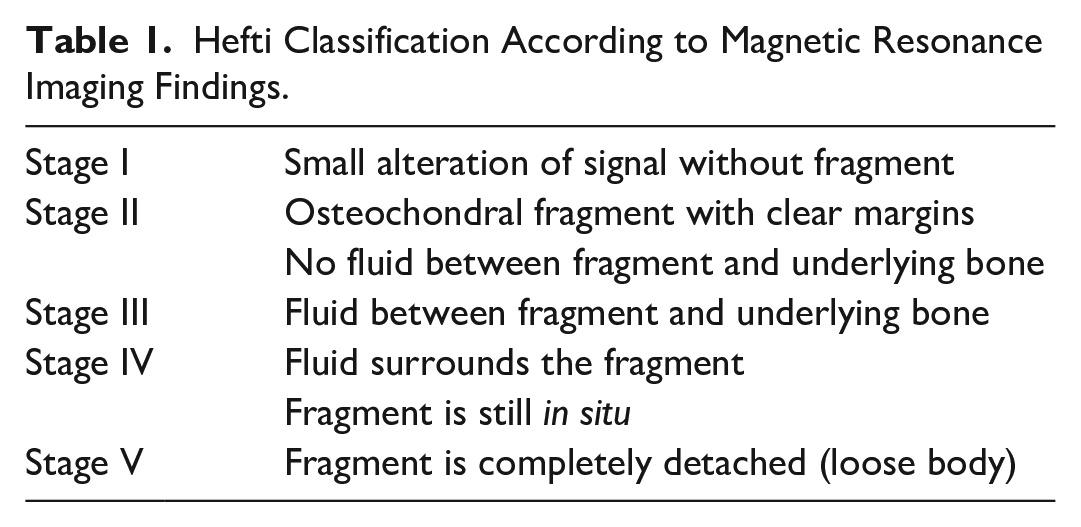
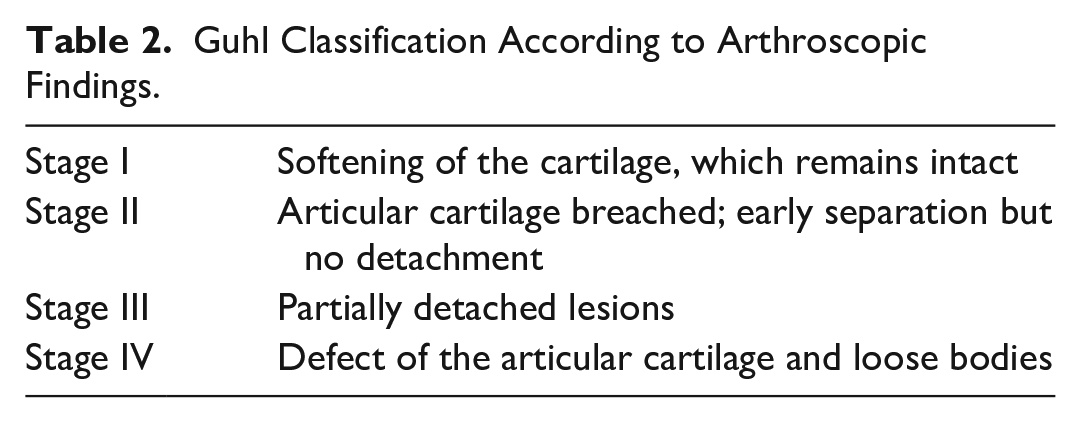
After obtaining institutional review board approval, all the patients who were diagnosed with OCD of the knee and underwent arthroscopic operative treatment were identified and reviewed. The study included patients operated between 2004 and 2016 in 2 tertiary hospitals, by 2 surgeons (MH and MI) who applied the same technique in this particular disease. The absolute indication for operation was failure of nonoperative management with persistent pain, besides the other clinical and radiological findings. No operative treatment was offered to asymptomatic patients. The patients were classified depending on the stage of OCD, which was assessed with MRI and then confirmed during the arthroscopy. In the literature, several classification systems have been proposed. Hefti and Guhl classifications were utilized, in an attempt to combine a radiological and arthroscopic classification system that can be correlated to each other. In the preoperative setting, the Hefti classification was used, which is based on MRI findings ( Table 1 ). 5 After evaluating the MRI, the diagnosis was set and the classification was made by the 2 principal surgeons (MH and MI). The interobserver reliability was excellent (0.921). However, each lesion was eventually classified during the arthroscopic procedure and utilizing the Guhl classification 25 ( Table 2 ).
Hefti Classification According to Magnetic Resonance Imaging Findings.
Guhl Classification According to Arthroscopic Findings.
All operating reports with the diagnosis of OCD were manually reviewed. Only juvenile patients who were followed for a minimum of 2 years were included. Furthermore, only those who had conducted an MRI study before and after the operation were included. Exclusion criteria were stage other than II or III, age older than 16, or closed distal femoral physes, and patients with a concomitant injury along with OCD. In total, 10 cases were excluded from the final evaluation (see flowchart in Fig. 1). In particular, 3 cases were patients over 16 years old (range = 18-28), 3 cases were classified as grade IV, while 4 patients were not available to undergo a postoperative MRI.
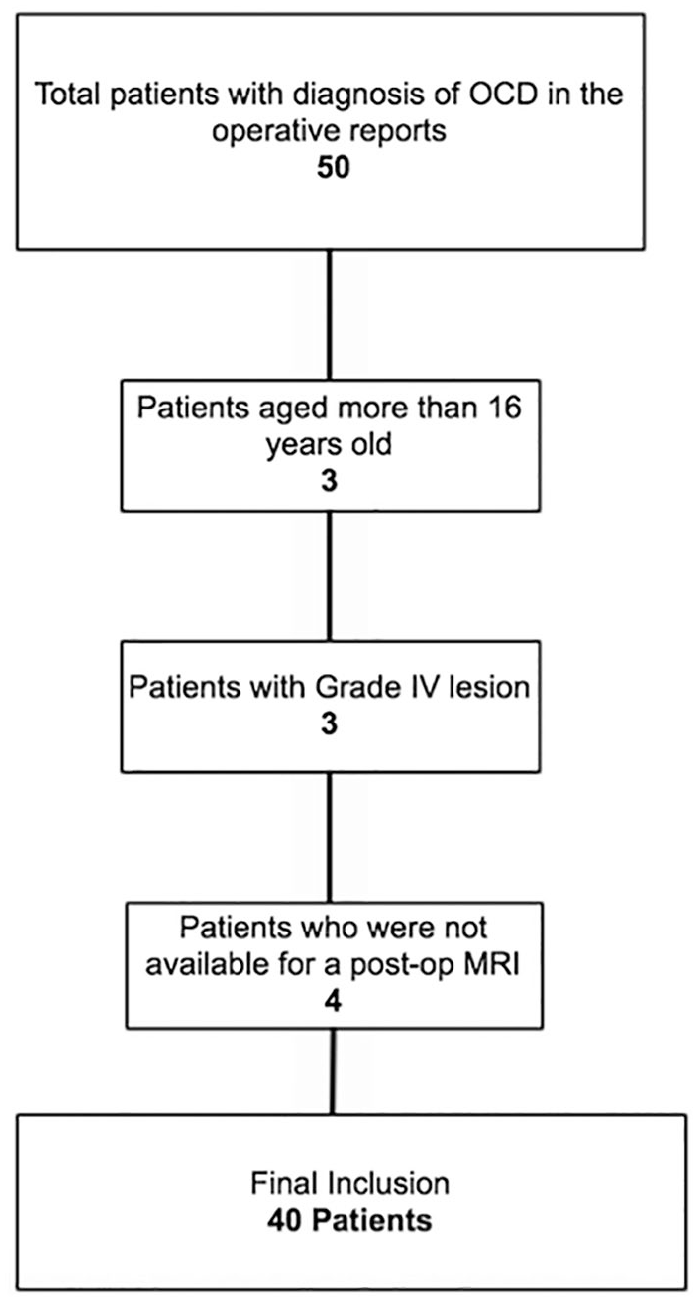
Flowchart of the patients finally included in the study.
In all patients nonoperative treatment was applied for at least 6 months before surgery. Although there are published data that report high failure rates with conservative treatment in grade III lesions, 26 we decided to apply nonoperative treatment to all patients since all patients accepted to be treated initially with nonoperative, functional treatment. Besides, there are studies that demonstrate that less severe cases can heal within 6 to 18 months with conservative treatment.27,28 This consisted of limited weight bearing for 6 weeks and restriction in sports activity for 4 to 6 months.
Patient demographics, surgical variables, imaging studies, and postoperative complications were recorded. Demographic data included age, sex, and dominant knee affected. Surgical variables, such as the number of implants used, were obtained, while the size of the lesion was also recorded by measuring the maximum diameter of each ( Table 3 ). Early postoperative complications were defined as severe hemarthrosis or synovitis, acute infection, and neurovascular complication and late ones as knee stiffness or another surgery for implant removal.
All Cases Included in the Study.

These were the nonhealed cases.
Patients were assessed preoperatively and at the final follow-up with the International Knee Documentation Committee (IKDC) subjective knee score and the Lysholm score. Additionally, the Visual Analogue Pain Scale (VAS; 0-10, 10 being worst) was used to measure the subjective improvement in symptoms. MRI was conducted at least 1 year after the surgery in all patients to evaluate the status of the lesion. Healing was defined as the radiological sign of union in MRI and elimination of the symptoms, especially regarding pain. Failure was defined patient’s complaint about persistent pain at final follow-up, along with MRI findings suggestive for a nonhealed lesion, such as high-intensity signal at the interface between the fragment and the adjacent bone, or presence of edema around the lesion, or joint fluid around the fragment indicating a complete detachment.
Surgical Technique
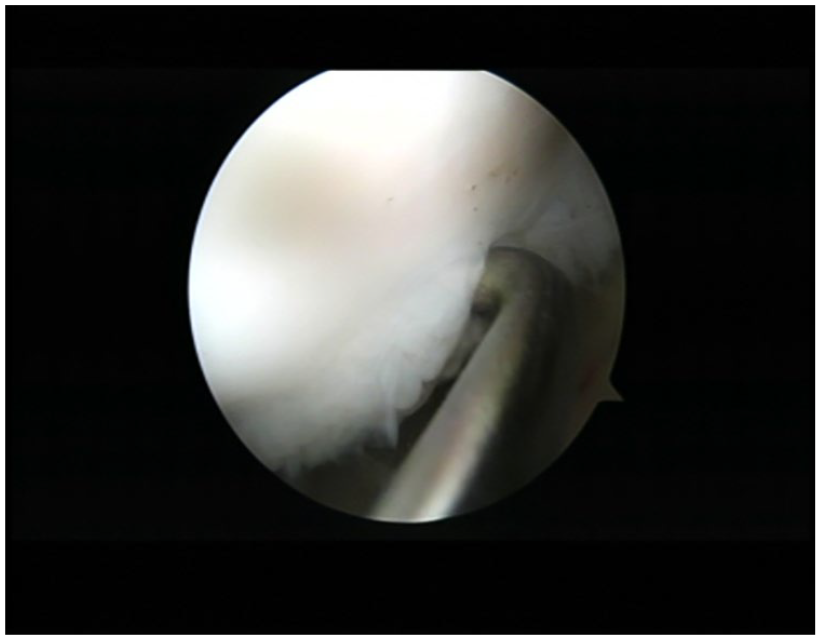
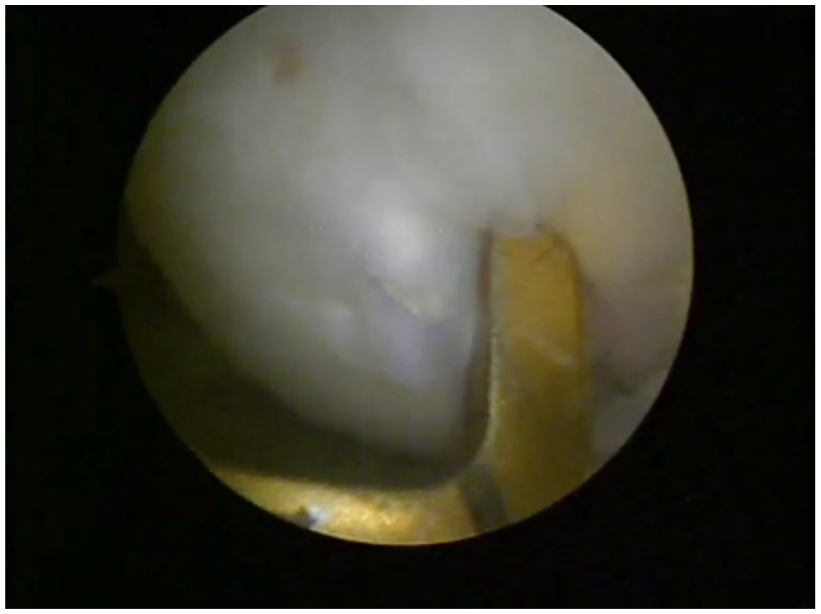
All procedures were performed under general or regional anesthesia and with the use of a tourniquet. Initially, a complete diagnostic arthroscopy of the knee was performed to identify any concomitant lesions. Cartilage was evaluated with the use of the probe, and confirmation of the stage of the lesion according to Guhl classification was made intraoperatively ( Figs. 2 and 3 ). Using an anterior cruciate ligament tibia tunnel guide, retrograde drilling of the lesion in situ was performed (without any manipulation of the affected cartilage) to stimulate healing via release of growth factors from the surrounding healthy cancellous bone ( Fig. 4 ). Finally, arthroscopic fixation of the lesion with bioabsorbable pins (Smart nails-CONMED, Linvatec, Edison, NY) was performed.
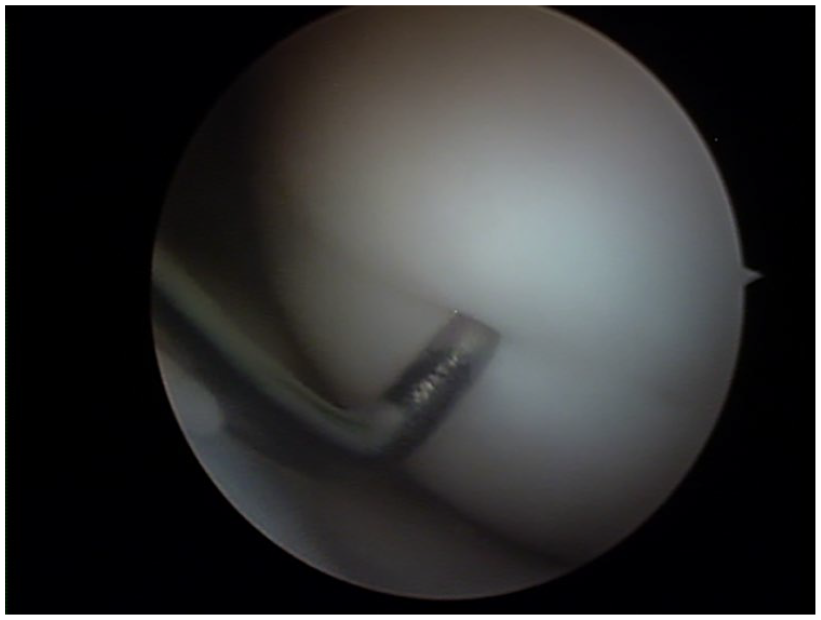
Probing of a stable osteochondritis dissecans lesion during the arthroscopy.
Probing of an unstable osteochondritis dissecans lesion during the arthroscopy.
Retrograde drilling of the lesion in situ with the use of an anterior cruciate ligament tibia tunnel aimer.
Rehabilitation Protocol
Postoperative rehabilitation included partial weight bearing and avoidance of knee flexion beyond 90° for 6 weeks, followed by physical therapy, and exclusion from sports activities for at least 8 months.
Statistical Analysis
Categorical data were compared between 2 groups using the Fisher exact test, and a nonpaired t test was used for continuous variables, such as the comparison between preoperative and postoperative scores. In an attempt to identify differences in the final outcome between the 2 groups (stages II and III), a statistical analysis of demographic data and surgical variables, such as the number of pins implanted, was performed. Significance was set at P < 0.05.
Results
Overall, 40 cases that fulfilled the inclusion criteria were recorded. Twenty-eight lesions were treated in males (70%) and 12 (30%) in females. The average age was 13.1 (range = 11-16). Medial femoral condyle was affected in the majority of the cases (33/40, 82.5%). According to the MRI findings, 21 patients (52.5%) were classified as Hefti ΙΙ and 19 (47,5%) as Hefti ΙΙΙ. As aforementioned, the definite classification was made based on arthroscopic findings. This was eventually in absolute accordance with the initial one. Subsequently, 21 patients (52.5%) were classified as Guhl ΙΙ and 19 (47.5%) as Guhl ΙΙΙ. The average lesion size was 18.5 mm (range = 14-26 mm) and 20.3 mm (range = 14-28 mm), for stages II and III, respectively. All patients were observed postoperatively for a minimum follow-up period of 2 years (range 3-13 years, average 6.6 years). Overall, the healing rate was 90% (36/40). In particular, the healing rate was 95% (20/21) for stage II and 84% (16/19) for stage III ( Table 4 ).
Comparison of Demographic Data and Healing Rate between Groups.

The average amount of absorbable pins used for fixation was 2.3 (range = 1 to 4). There was no statistical difference between the 2 groups (stages II and III) neither regarding the demographic data, age, and gender, nor the surgical variables (amount of pins used). Furthermore, there was no significant difference in healing rate between the 2 lesion stages (II and III; Table 4 ). Additionally, the size of the lesion and the number of used pins were not statistically correlated to success or failure.
Regarding the functional outcome scores, applied to the whole population, all of them revealed a statistically significant improvement (P < 0.05) in comparison to preoperative status. More specifically, the mean postoperative IKDC score increased to 86.46 from 50.36 preoperatively, while the Lysholm score increased to 95.1 from 70.4, and the VAS score decreased to 1.8 from 7.3 ( Table 5 ). Similarly to overall outcomes, there was again a statistically significant improvement of IKDC score, Lysholm score, and VAS score when groups were separately evaluated (P < 0.05) ( Table 5 ).
IKDC, Lysholm, and VAS Scores Preoperatively and Postoperatively.

IKDC = International Knee Documentation Committee; VAS = Visual Analogue Scale.
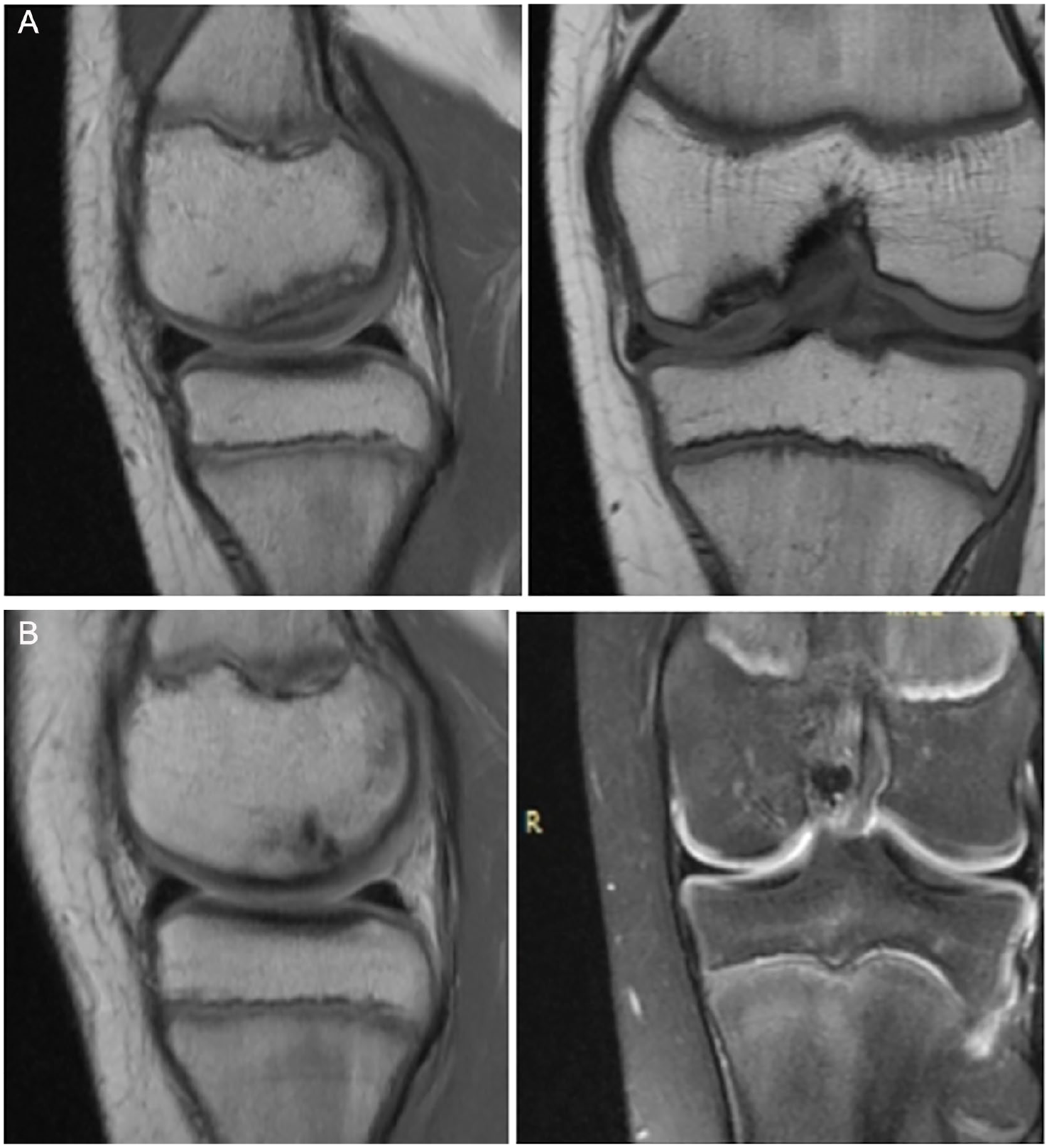
All patients underwent preoperatively MRI to set the diagnosis along with the clinical findings, and postoperatively in an attempt to evaluate the healing process ( Figs. 5 and 6 ). There was complete healing of the lesion seen in the MRI, in 36 patients, with subchondral bone showing normal, homogeneous signal intensity with no demarcation line and no presence of fluid ( Fig. 5B ).
(
Coronal (
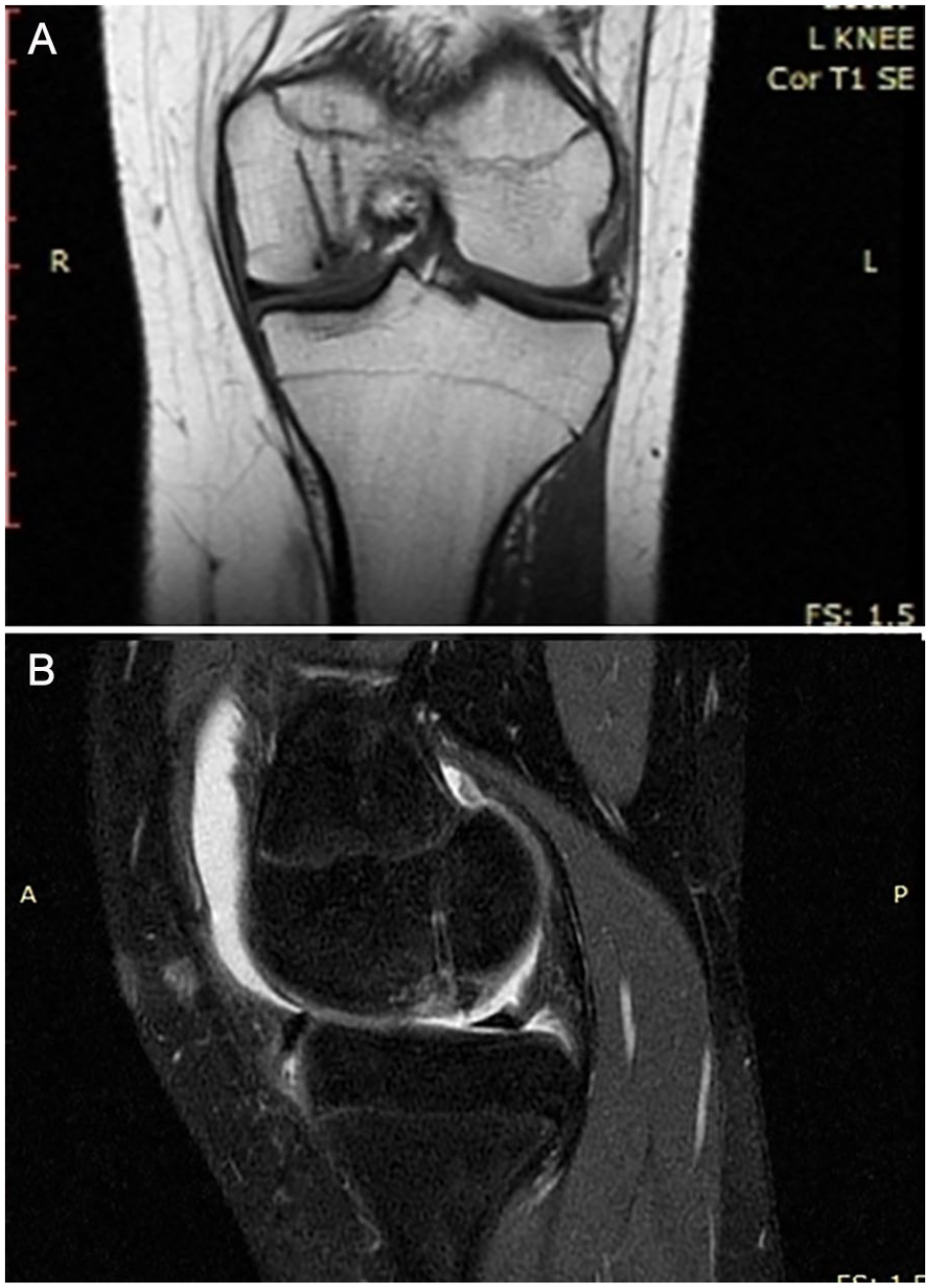
Four patients were considered failures in our study. All these patients experienced mild to moderate pain during follow-up time, and the MRI revealed a nonhealed lesion ( Fig. 6 ). Although the symptoms were meliorated, the persistence of mild pain led them to request further intervention. The patient from stage II group with a nonhealed lesion underwent a second procedure with autologous bone grafting of the lesion plus sealing of the defect with a hyaluronic acid scaffold. In the 3 patients from stage III group who continued to experience pain, a further intervention was performed with autologous chondrocyte implantation.
No intraoperative or perioperative complications occurred. No infection, synovitis, neurovascular complication, or knee stiffness was recorded and no further operation for implant failure and removal was needed. Six weeks postoperative, all patients were able to walk with full weight bearing, without complaints. Patients with healed lesions were able to initiate sports activities at 8 months. All of them reported at the final follow-up that they were able to continue their previous sport activities without any restrictions.
Discussion
The most important finding of this study is that internal fixation of stage II and stage III OCD lesions of the knee with bioabsorbable pins can result in good to excellent radiological and clinical outcome in the vast majority of juvenile patients. The healing rate in our series was 90% (36/40) at a mean follow-up of 6.6 years. Pain, which was the predominant symptom among the patients, was completely resolved in 36 of them. All these patients returned to their previous sport activities without any further complaints.
For juvenile patients with OCD lesions where nonoperative management fails or for those with unstable lesions, internal fixation of the fragment has been proven to be effective29,30; early cartilage separation, partial detachment, and, even worse, loose bodies are typically treated operatively. In this study’s cohort, internal fixation apart from its use in partially detached lesions was also applied for the treatment of stable, early separated lesions with persistent symptoms, resulting in extremely favorable results. A high healing rate with excellent functional outcome was achieved for internal fixation of stage II and stage III juvenile OCD lesions of the knee. Although there was a trend for a higher healing rate in the stage II group (95%), in comparison to stage III (84%), no statistically significant difference in healing rate by lesion grade was observed. However, this could be due to the relatively low number of patients in each group, which subsequently could lead to a type B error.
Several factors may lead to this lower healing rate of grade III lesions, such as divergent demographic data among the patients or the nature of the lesion itself. Nevertheless, the size of the lesion was not proved to be a predisposing factor for failure in our series. Noteworthy, there are conflicting previously published data regarding the impact of lesion stability and size on the final outcome. There are studies that demonstrated no difference in healing rate by lesion grade, 29 and others that correlated failed cases with unstable lesions in MRI and large lesion sizes. 31
The performed surgical technique includes retrograde drilling of the lesions. Arthroscopic drilling of juvenile OCD lesions has been well documented in the literature, but especially for stable, intact articular surfaces. Kocher et al. 32 evaluated the functional and radiographic outcomes after transarticular arthroscopic drilling in 30 knees of 23 skeletally immature patients. Healing, seen on plain radiographs, was achieved in all patients at a mean of 4.4 months after drilling with significant improvement in the mean Lysholm score. Antegrade drilling was effective in skeletally immature patients and curative in 83% in another study by Anderson et al. in 24 patients. 33
Of note, there is no gold standard on treating OCD lesions. A systematic review by Abouassaly et al. 34 highlighted the wide variety and the high heterogeneity of surgical methods used for stable but especially unstable lesions. They concluded that no particular techniques have been shown to be superior through high-quality studies. As aforementioned, many studies have evaluated the isolated application of suchondral drilling, either transarticular or retrograde, but mainly in stable lesions. Retrograde drilling was performed in this study, which is technically demanding, but straightforward and can aid in stimulating the subchondral bone, without damaging the cartilage. Our technique with the use of anterior cruciate ligament tibia aimer allows us to penetrate the subchondral bone and enhance vascularization. The main limitation of this technique based on published data is its use in patients with closed physes. 33
The first implants used for internal fixation were metallic ones, such as cannulated screws, Herbert screws, and metal staples. 35 Arthroscopic fixation with different forms of cannulated screws for unstable lesions is considered an effective option in patients with Guhl stages II and III osteochondral lesions. 21 Cugat et al. 21 demonstrated excellent results in 12 of the 15 patients managed arthroscopically with cannulated screws, while Guhl 25 found good to excellent results in 40 of his 46 patients. Despite promising results, these implants have been associated with severe drawbacks, including MRI interference and postoperative complications, such as migration or breakage, which usually lead to a second intervention.14,21,25 Subsequently, these distinct disadvantages resulted gradually in dominance of the use of bioabsorbable materials.
The use of bioabsorbable pins compared with metal screws has the added benefit that no further procedure is necessary for implant removal, while no interference is provoked on the postoperative MRI scan. 24 On the other hand, use of bioabsorbable implants is not without drawbacks. Among others, the most important and frequently reported one is synovitis. Synovitis is most likely related to biodegradation of polymers and to the host response.36,37 Several studies have highlighted synovitis as a significant complication after this procedure.38-40 Other complications reported include sterile abscess formation and loss of fixation. 2 It is worth noting that in the present case series, no direct implant-related complications have been experienced. Some may also argue that bioabsorbable pins result in a less rigid fixation, which may eventually lead to nonunion. This may be one of the reasons for failure in the 4 cases of our cohort.
Perelli et al. 41 attempted to evaluate the use of different devices, such as Herbert screws, cannulated screws, and bioabsorbable nails, and found no difference between them with regard to clinical and radiological outcomes. However, their study evaluated only mature patients. Of note, few studies have evaluated the clinical and radiological outcomes after fixation with absorbable pins. Furthermore, most of these studies are characterized by heterogeneity, regarding the implanted devices, the lesions, and the population. Kocher et al. 29 reported a high healing rate of 84.6%. However, their study was highly heterogeneous, including 26 lesions of stages II, III, and IV, treated with 4 different fixation methods. Dines et al. 42 investigated the outcomes following the use of SmartNail in osteochondral lesions, with a mean MRI follow-up of 33 months. Nevertheless, their cohort was relatively small, with only 9 knees. They reported excellent outcomes in 7 patients, good in 1, and fair in 1. Tabaddor et al. 17 showed a healing rate of 91.7% in unstable lesions of 24 knees, treated either arthroscopically or with arthrotomy in both mature and immature patients. Moreover, in one of the very few studies targeted on juvenile patients, Adachi et al. 24 reported a high healing rate of 97% in 33 lesions, treated either arthroscopically or with arthrotomy.
This study is not without limitations. First, it has the inherent disadvantages of its retrospective nature. In addition, no control group or group treated with a different method was available, which does not allow us to conclude the superiority of the proposed fixation over other fixation methods. Furthermore, as aforementioned, we lack detailed information about conservatively treated patients. This fact does not allow as deriving conclusions about the patients who are the best candidates for surgical treatment. Besides, the first and foremost strength of this cohort is its homogeneity. Patients were categorized into 2 highly homogenous groups and were all treated arthroscopically with the same surgical procedure following the same rehabilitation protocol.
Conclusion
Based on the present study’s results, internal fixation of stage II and stage III OCD lesions of the knee with bioabsorbable pins represent a surgical option providing good to excellent results in juvenile patients in midterm to long-term follow-up. Optimal staging according to MRI classification systems and final evaluation in the operating theater, proper patient selection, as well as advanced acquired arthroscopic skills are essential for the desired outcome.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was obtained from General University Hospital of Larissa Protocol No 86382/23-1-2019.
Informed Consent
Written informed consent was obtained from all subjects before the study.