
Abstract
Objective
This study aimed to examine the midterm clinical outcomes of autologous osteochondral grafts (AOG) that were performed in the femoral condyle without treating the tibial plateau with subchondral bone exposed, and to compare these outcomes with those of AOG used in patients with osteoarthritis (lateral type or medial type) or osteonecrosis.
Design
The study included 6 men and 16 women and 11 right knees and 11 left knees. The mean operative age was 56.0 years (range, 21-76 years), and the mean follow-up period was 98.4 months (range, 60-164 months). Six patients had lateral type osteoarthritis (OAL), 7 had medial type osteoarthritis (OAM), and 9 had osteonecrosis (ON). The patients’ knee symptoms as their clinical outcome were evaluated using the knee scoring system of the Japanese Orthopedic Association (JOA), and the International Knee Documentation Committee (IKDC) subjective score.
Results
The postoperative clinical outcomes of the OAL and ON group were significantly better than their preoperative clinical scores and remained the same until the final follow-up. However, the clinical outcomes of OAM improved 2 years after AOG, but eventually decreased thereafter. The number of worse cases in the OAM group was significantly larger than those in the OAL and ON groups.
Conclusion
In these procedures, the postoperative clinical outcomes of the OAL and ON groups were significantly better than their preoperative clinical scores and were maintained for about 8 years. However, the clinical outcomes of OAM improved until 2 years after AOG, but eventually decreased thereafter.
Introduction
Since Matsusue et al. 1 first reported autologous osteochondral grafts (AOG) in 1993, AOG is increasingly used in the treatment of small, isolated, well-contained, articular cartilage defects.2 -6 In osteochondral diseases such as osteonecrosis and osteochondritis dissecans, the technique has been reported to have a good clinical outcome.7,8 The long-term clinical outcome after mosaicplasty for a symptomatic osteochondral defect in the knee is good, but varies greatly depending on age, sex, and the size of the lesion.9,10
In most young patients, their recipient sites were only their femoral condyle or tibial plateau. However, in patients aged older than 40 years, their recipient sites were both femoral condyle and tibial plateau. 11 We previously described the good clinical outcomes of AOG for osteonecrosis12,13 or osteoarthritis. 14 Even if the recipient sites were the femoral condyle and tibial plateau, most of the AOGs were applied only in the femoral condyle due to the limited donor area. To date, only a few studies reported the midterm clinical outcomes of AOG applied only in the femoral condyle with no procedure in exposed subchondral bone of tibia. 15
Therefore, this study aimed to examine the midterm clinical outcomes of AOGs applied only in the femoral condyle with no procedure in exposed subchondral bone of tibia, and to examine these outcomes with those of AOGs used in patients with osteoarthritis (lateral type or medial type) or osteonecrosis. The clinical outcomes at 2 years after AOG as short-term results and the clinical outcomes at 5 years after AOG and final follow-up were also examined.
Materials and Methods
In our treatment protocol for osteochondral diseases in the knee joints, if the femorotibial angle is more than 180°, high tibial osteotomy with AOG is performed. If the femorotibial angle is less than 168°, distal femoral varus osteotomy with AOG is performed. Therefore, if the femorotibial angle is between 168° (valgus deformity) and 180° (varus deformity), we perform AOG alone. When the patient has an insufficient donor area, AOG is only performed in the femoral condyle if the recipient area in the femoral condyle is larger than that in the tibial plateau. AOG is only performed in the tibial plateau if the recipient area in the femoral condyle is smaller than that in the tibial plateau. And, we have no treatment procedure in exposing subchondral bone of the opposing articular surface.
In this study, AOG was performed as treatment for osteochondral diseases if the conservative treatment for more than 3 months had no effect. Patients who had AOG in the femoral condyle as treatment for osteochondral diseases and had more than 5 years of follow-up were included in the study. Their tibial subchondral bone was exposed as their opposing articular surface, and no surgical procedures were performed. The permitted combined operations were partial menisectomy or ligament reconstruction. Meanwhile, patients underwent osteotomy to improve their knee alignment were excluded. A total of 22 patients (6 men and 16 women) and 22 knees (11 right knees and 11 left knees) were examined from September 2001 to November 2012 in this series. The follow-up ratio was 84.6% at 5 years after AOG. All procedures were reviewed and approved by the research ethics committee of our hospital, and this study was carried out in accordance with the World Medical Association’s Declaration of Helsinki. Their mean operative age was 56.0 years (range, 21-76 years), and the mean follow-up period was 98.4 months (range, 60-164 months). Two patients had arthroscopic partial lateral menisectomy, 1 had arthroscopic anterior cruciate ligament reconstruction, and another had arthroscopic posterior cruciate ligament reconstruction. The postoperative rehabilitation program was as follows: range of motion exercise was initiated in day 3 after AOG, and partial weight-bearing gait started in week 3 or 4 and full weightbearing gait in week 6 or 7. The patient’s donor site was either the lateral or medial side of the femoral trochlea, and one patient had their contralateral knee as the donor site.
With regard to basic diseases, 6 patients had lateral-type osteoarthritis (OAL) whose recipient sites were lateral femoral condyle, 7 had medial-type osteoarthritis (OAM) whose recipient sites were medial femoral condyle, and 9 had osteonecrosis (ON) whose recipient sites were lateral femoral condyle (2) and medial femoral condyle (7). During AOG, 2 patients with OAL had less than one-third lateral meniscus, and the other 20 patients had more than one-third meniscus of the same compartment.
The patients’ knee symptoms as their clinical outcome were evaluated according to the following criteria: the knee scoring system of the Japanese Orthopedic Association (JOA), 16 and the International Knee Documentation Committee subjective score (IKDC). 17 The JOA scale evaluates the following four items: ability to walk (30 points), ability to climb up and down the stairs (25 points), range of motion (35 points), and joint swelling (10 points). Each knee joint can achieve a maximum score of 100 points on the JOA scale. We evaluated the clinical outcomes at preoperative period, 2 years after AOG, 5 years after AOG and at final follow-up. Twenty patients had more than 72 months of follow-up, 1 with OAM had a 60-month follow-up, and another with OAM had a 61-month follow-up. Data on the 2 patients’ scores at preoperative period, 2 years after AOG, and 5 years after AOG were obtained, but their final scores were not obtained.
We also examined the changes of Kellgren-Lawrence (KL) classification in plain anteroposterior radiographies. As the KL classification can be used to examine each compartment of the same knee separately, the patients were divided into 3 groups: OAL, OAM, and ON. Preoperative KL classifications among 3 groups were shown in Table 1 .
Preoperative Items in 3 Groups. a
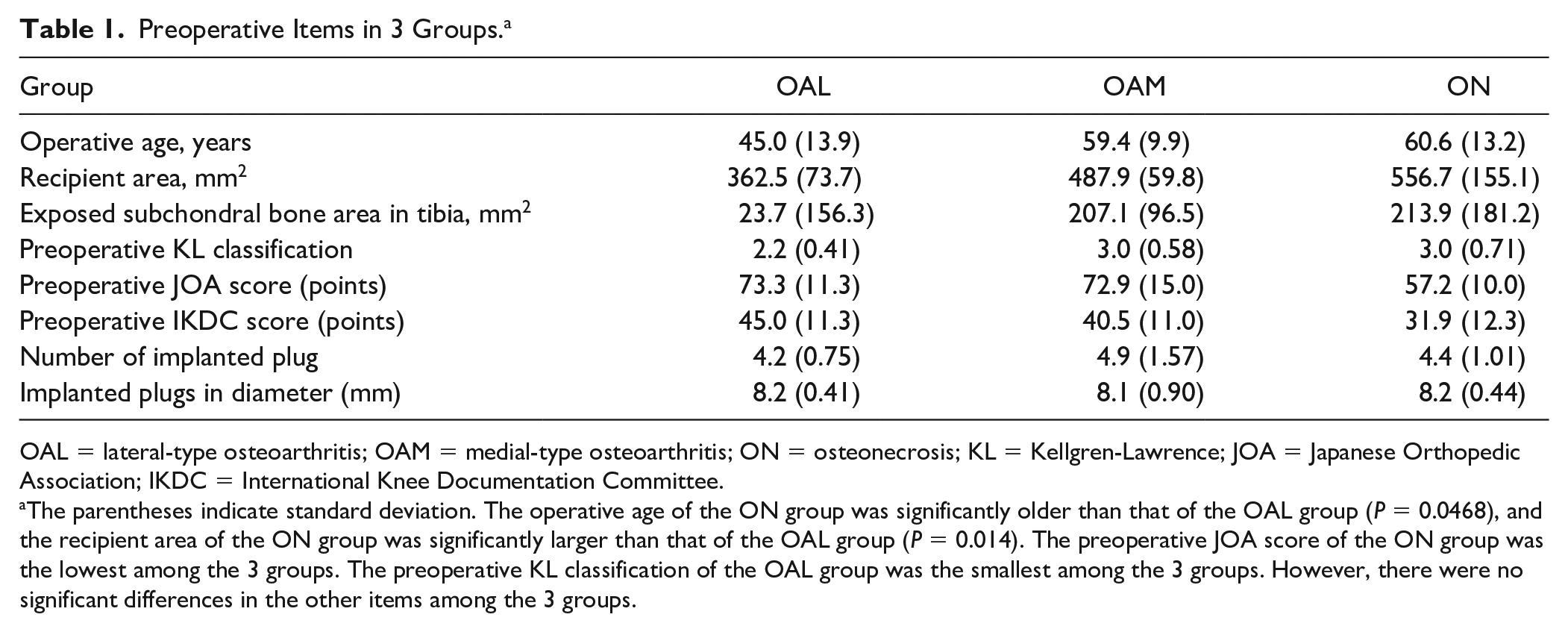
OAL = lateral-type osteoarthritis; OAM = medial-type osteoarthritis; ON = osteonecrosis; KL = Kellgren-Lawrence; JOA = Japanese Orthopedic Association; IKDC = International Knee Documentation Committee.
The parentheses indicate standard deviation. The operative age of the ON group was significantly older than that of the OAL group (P = 0.0468), and the recipient area of the ON group was significantly larger than that of the OAL group (P = 0.014). The preoperative JOA score of the ON group was the lowest among the 3 groups. The preoperative KL classification of the OAL group was the smallest among the 3 groups. However, there were no significant differences in the other items among the 3 groups.
Their postoperative clinical outcomes were compared with their preoperative clinical scores. We also assessed the operative age, follow-up periods, the recipient area, the subchondral bone exposing area in their tibia of same compartment, the number of implanted plugs and the diameter of implanted plugs.
About 1 year after primary AOG, second-look arthroscopy was planned to examine the grafted articular cartilage. Of the 12 patients who underwent second-look arthroscopy, 4 were assigned in the OAL group, 5 in the OAM group, and 3 in the ON group. The mean time from AOG to the second-look arthroscopy was 19.1 months (range, 3-84 months). The recipient site was evaluated using the ICRS (International Cartilage Repair Society) cartilage repair assessment score.
The Mann-Whitney U test and chi-square test were used to perform the statistical analysis of various scores. The level of statistical significance was set at P < 0.05.
Results
In the total cases, the operative age, follow-up periods, the recipient area, the area of exposed subchondral bone in the ipsilateral tibial plateau, the number of implanted plugs, and the diameter of implanted plugs were 56.0 years (range, 21-76 years), 98.4 months (range, 60-164 months), 481.8 mm2 (range, 300-800 mm2), 212.5 mm2 (range, 25-600 mm2), 4.7 plugs (range, 3-8 plugs), and 7.5 mm (range, 4.5-9 mm), respectively. In terms of clinical outcomes, the chronological changes of JOA and IKDC are shown in Fig. 1 . In JOA and IKDC, the scores at 2 years after AOG were significantly the highest of all time periods. The scores at 5 years and final follow-up after AOG were significantly higher than those in the preoperative periods.
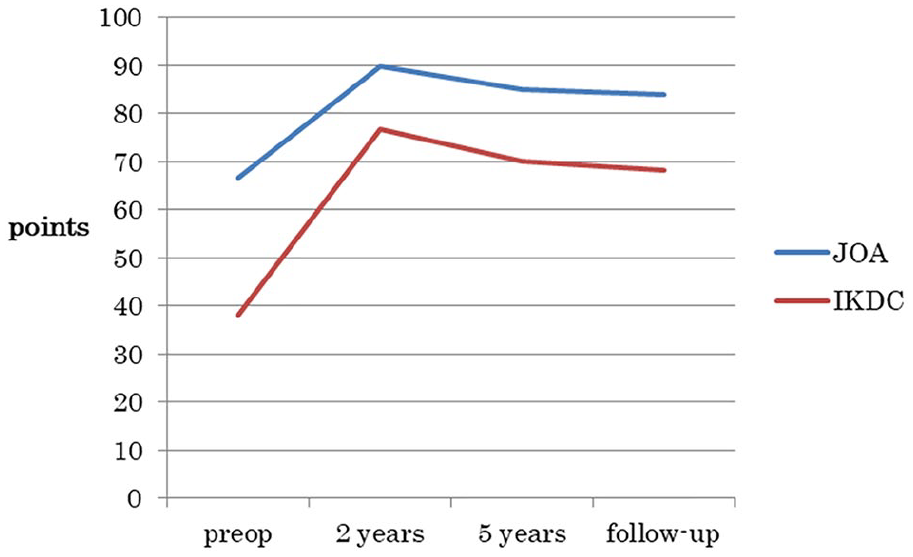
Chronological changes of JOA and IKDC subjective scores in all cases. In JOA and IKDC, the scores at 2 years after AOG were significantly higher in all periods. The scores at 5 years and final follow-up after AOG were significantly higher than those in the preoperative periods. AOG, autologous osteochondral graft; JOA, Japanese Orthopedic Association; IKDC, International Knee DOcumentation Committee.
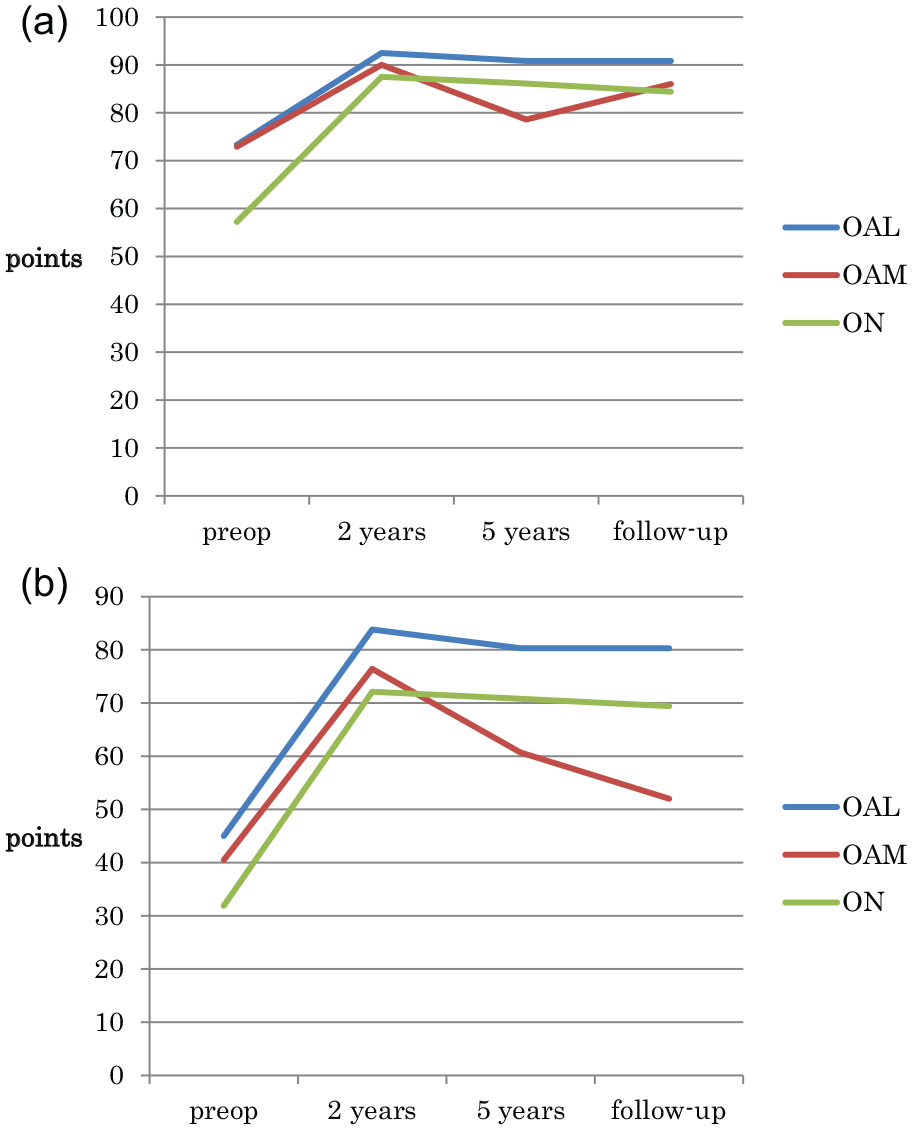
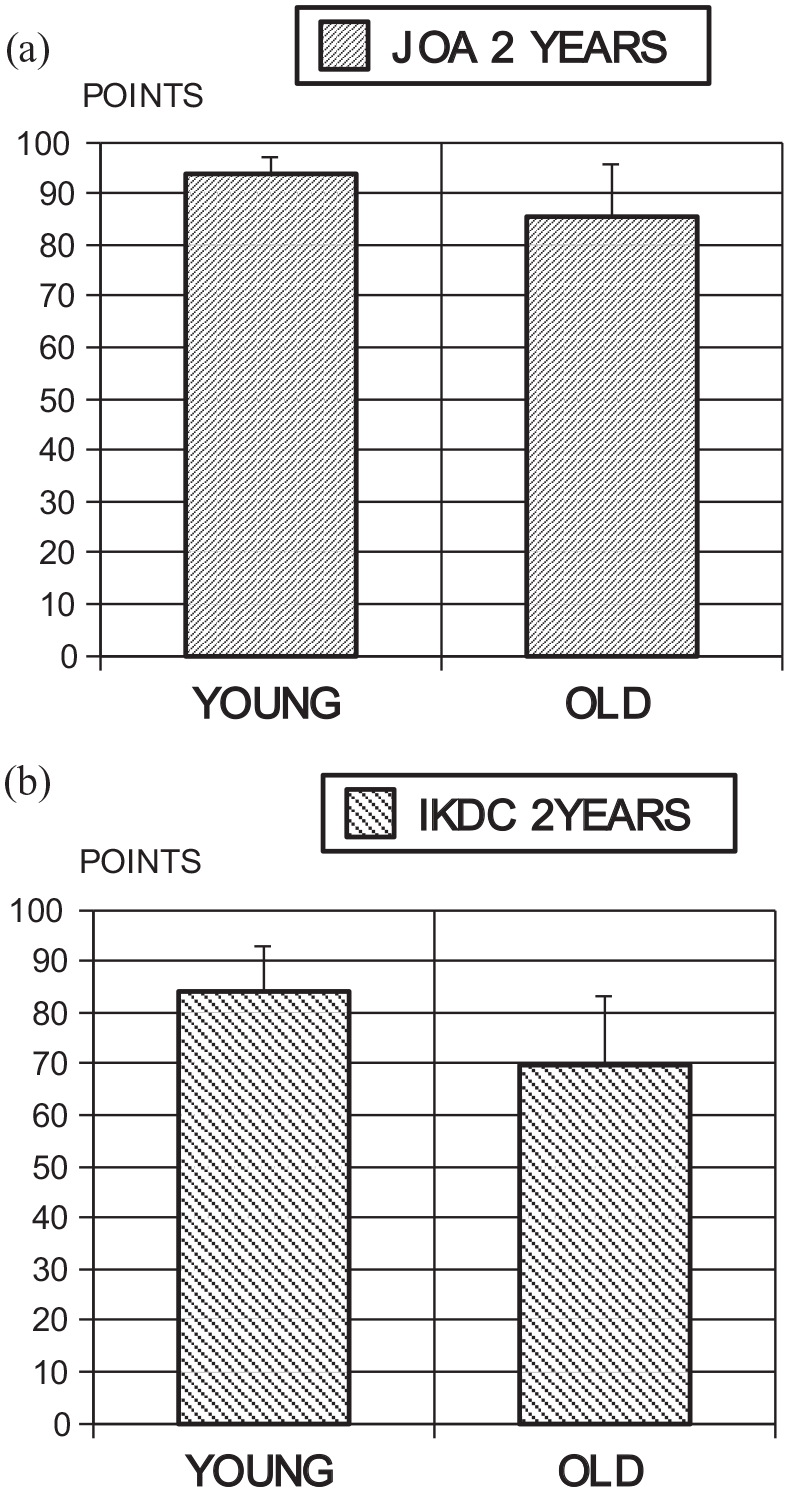
Next, the preoperative items in the OAL, OAM, and ON groups are shown in Table 1 . The operative age of the ON group was significantly older than that of the OAL group, and the recipient area of the ON group was significantly larger than that of the OAL group. The preoperative JOA score of the ON group was the lowest among the 3 groups. The preoperative KL classification of the OAL group was the smallest among the 3 groups. However, there were no significant differences in the other items among the 3 groups. The chronological changes of JOA and IKDC in 3 groups are shown in Figure 2 . The JOA scores at 2 years after AOG of the 3 groups were significantly higher than those in the preoperative period. The scores at 5 years and at final follow-up in OAL and ON were significantly higher than those during the preoperative period, but the scores at 5 years and final follow-up in OAM were not significant ( Fig. 2a ). At final follow-up, the JOA score of the OAL group was significantly higher than those of the OAM group (P = 0.0476). In IKDC, the scores at 2 years and 5 years after AOG of the 3 groups were significantly higher than those during the preoperative period. The scores at final follow-up in OAL and ON were significantly higher than those during the preoperative period, but the scores at final follow-up in OAM were not significant ( Fig. 2b ). At final follow-up, the IKDC score of the OAL group was significantly higher than those of the OAM group (P = 0.0142), and the ON group had a higher IKDC score than the OAM group (P = 0.0517). Therefore, the postoperative clinical outcomes of the OAL and ON groups were significantly better than their preoperative clinical scores and remained the same until the final follow-up. However, the clinical outcome of the OAM group improved until 2 years after AOG, but eventually decreased thereafter.
(
Table 2 summarizes the patients’ clinical outcomes and their preoperative clinical scores. The OAM group had significantly more worse cases than the OAL and ON groups. Two patients from the OAM group had total knee arthroplasty at 61 months and 123 months after AOG, 1 had high tibial osteotomy at 96 months after AOG, and 1 patient had no additional operation.
The Worse Cases Comparing the Follow-up Scores with Their Preoperative Scores.
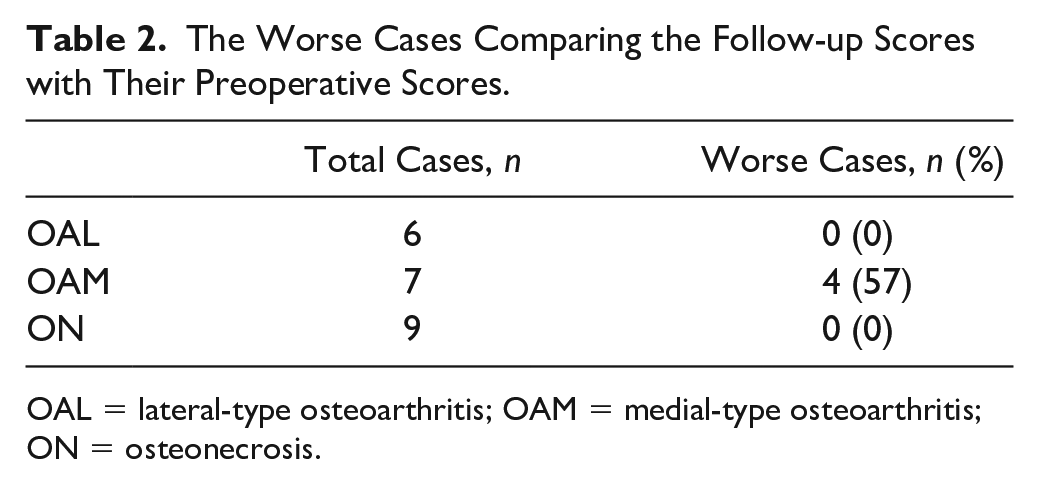
OAL = lateral-type osteoarthritis; OAM = medial-type osteoarthritis; ON = osteonecrosis.
At final follow-up, 10 patients received no treatment, including 3 from the OAL group, 2 from the OAM group, and 5 from the ON group. Except 3 patients who underwent revision operations, the other treatments performed were as follows. In the OAL group, 1 received hyaluronic acid injection, while 2 were occasionally treated with nonsteroidal anti-inflammatory drugs (NSAIDS). In the OAM group, 1 was occasionally treated with NSAIDS, and 1 received ointment therapy. In the ON group, 3 occasionally received hyaluronic acid injection, and 1 was given a pain patch.
The risk factor for the clinical outcomes was older age at 2 years after AOG in the JOA ( Fig. 3a ) and IKDC ( Fig. 3b ) and at 5 years in the JOA. There were no significant differences in the other factors.
(
The KL grade of all 6 patients from the OAL group remained unchanged from the preoperative period to follow-up period. Five patients had grade 2 and 1 had grade 3. In the OAM group, the KL grade in 1 patient improved (grade 3 to 2), that in 3 patients worsened (grade 3 to 4), and that in another 3 patients remained unchanged (1 grade 2; 1 grade 3; and 1 grade 4). In the ON group, the KL grade in 3 patients improved (1 grade 3 to 2; 1 grade 4 to 2), that in 1 worsened (grade 2 to 3), and that in 5 remained unchanged (1 grade 2; 1 grade 4; 3 grade 3).
Twelve patients underwent a second-look arthroscopy. The mean period from AOG to the performance of second-look arthroscopy was 19.1 months (range, 3-84 months). In ICRS cartilage repair assessment during the second-look arthroscopy, the mean scores were 10.25 points (range, 9-11; 4 patients) in the OAL group, 10.4 points (range, 10-11; 5 patients) in the OAM group, and 10.7 points (range, 9-12; 3 patients) in the ON group. Results of the second-look arthroscopy showed that the recipient and opposing articular surfaces in the 3 groups did not worsen.
The following are 2 case reports. Patient 1 was included in the OAL group. This 48-year-old woman had an AOG in her left femoral condyle with left anterior cruciate ligament reconstruction. Her preoperative radiogram showed KL grade 2 and her preoperative femorotibial angle was 170° ( Fig. 4a ). Her preoperative JOA and IKDC scores were 60 points and 44.2 points, respectively. The recipient area (left lateral femoral condyle) measured 450 mm2 ( Fig. 4b ), while her opposing articular surface (left lateral tibia) measured 225 mm2, when her subchondral bone was exposed ( Fig. 4c ). Two osteochondral plugs 7 mm in diameter and 3 plugs 8 mm in diameter were implanted into the recipient sites ( Fig. 4d ), and no procedure was performed in her opposing articular surface. At 13 months after AOG, a second-look arthroscopy was performed. Her ICRS cartilage repair assessment score was 11 points ( Fig. 4e ). At 95 months after the AOG, anteroposterior knee radiography was performed. The patient had KL grade 2 at preoperative period and had the same KL grade until the follow-up period ( Fig. 4f ). Her JOA and IKDC subjective scores were 95.0 point and 89.6 point, respectively, at the final follow-up period.
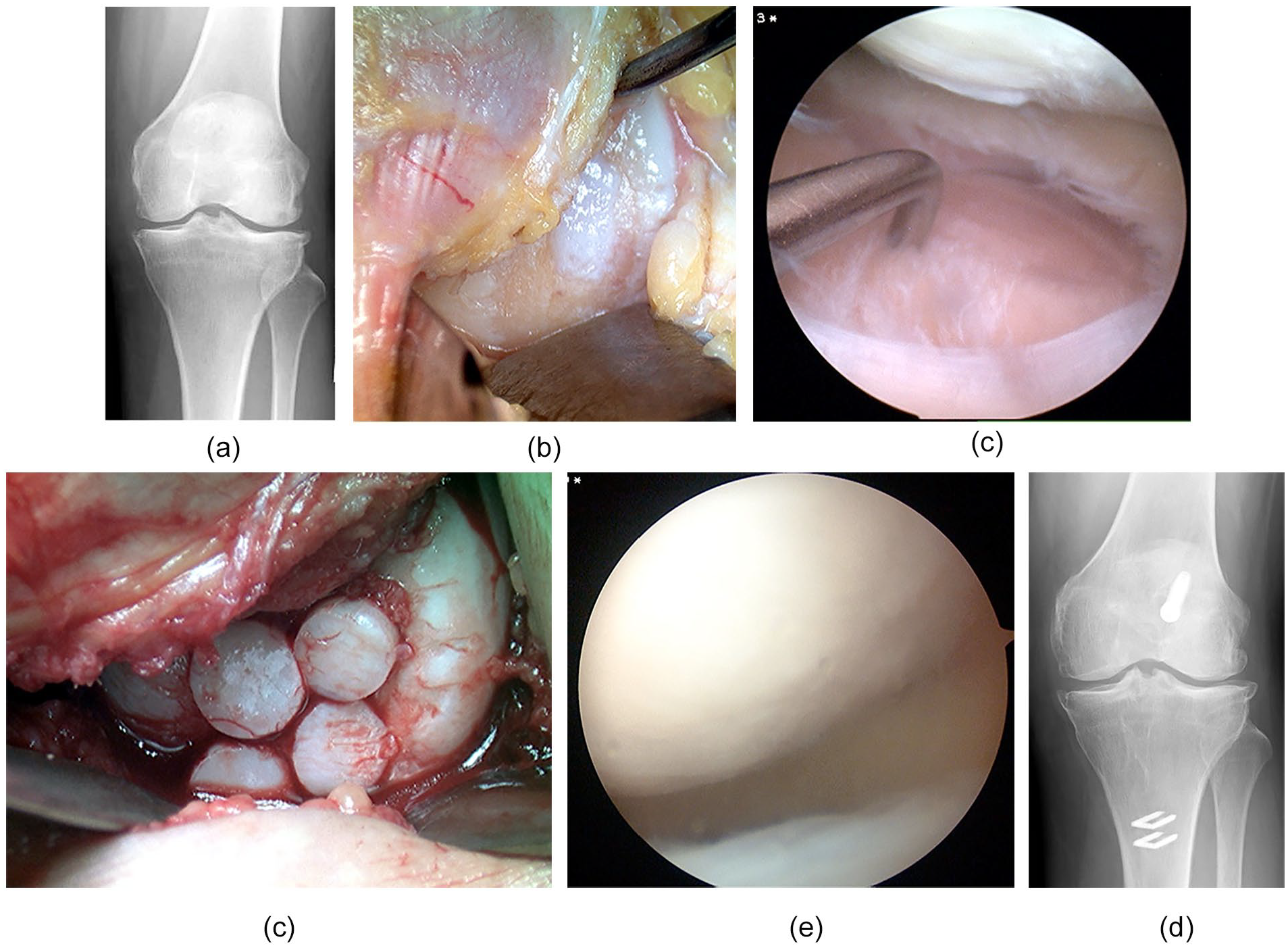
Case presentation in the OAL group. A 48-year-old woman: (
Patient 2 was included in the OAM group. This 49-year-old man had AOG in his left medial femoral condyle. His preoperative radiogram showed KL grade 4 and his preoperative femorotibial angle was 178° ( Fig. 5a ). His preoperative JOA and IKDC scores were 70 points and 42.9 points, respectively. The recipient area (left medial femoral condyle) measured 400 mm2 ( Fig. 5b ), while opposing articular surface (left medial tibia) measured 225 mm2, when the subchondral bone was exposed ( Fig. 5c ). Four osteochondral plugs at 9 mm in diameter were implanted into the recipient sites ( Fig. 5d ), and no procedure was performed in his opposing articular surface. At 13 months after AOG, a second-look arthroscopy was performed. His ICRS cartilage repair assessment score was 10 points ( Fig. 5e ), and no changes were noted in his opposing articular surface ( Fig. 5f ). At 96 months after his AOG, his left knee pain increased, and anteroposterior knee radiography was performed ( Fig. 5g ). The patient’s KL grade was 4 at preoperative period and remained the same until the follow-up period. His JOA and IKDC subjective scores were 60.0 points and 22.4 points, respectively. Therefore, we performed his left high tibial osteotomy. His left knee radiogram was performed 1 year after his osteotomy ( Fig. 5h ). His left knee pain disappeared.
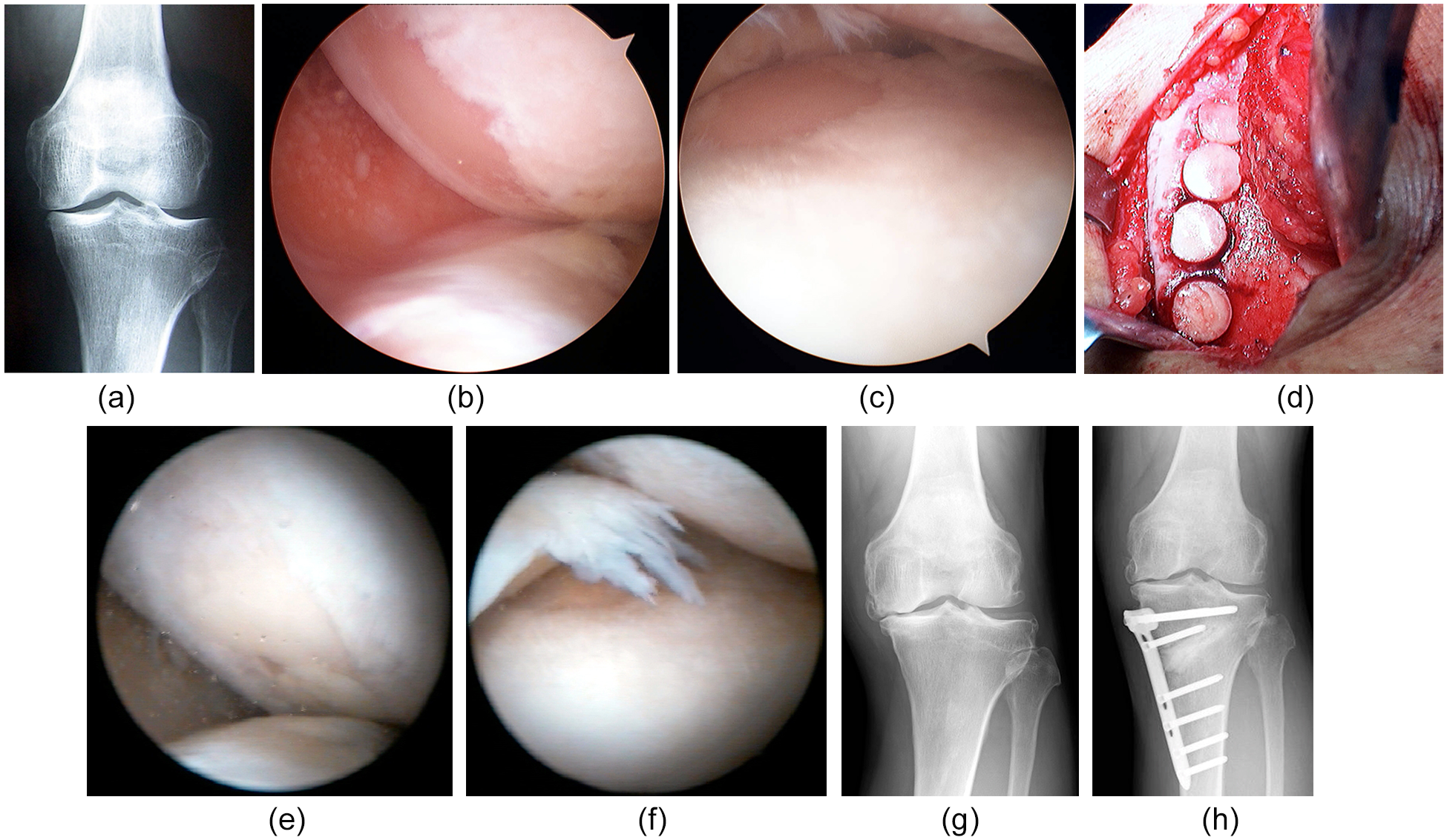
Case presentation in the OAM group. A 49-year-old man: (
Discussion
In this study, if AOG was only performed in the femoral condyle with no procedure in exposed subchondral bone of tibia, the JOA scores at 2 years after AOG in the 3 groups were significantly higher than those in the preoperative period. The scores at 5 years and final follow-up in the OAL and ON groups were significantly higher than those in the preoperative period, but the scores at 5 years and final follow-up in the OAM group were not significant. IKDC scores at 2 years and 5 years after AOG in the 3 groups were significantly higher than those in the preoperative period. The scores at final follow-up in the OAL and ON groups were significantly higher than those in the preoperative period, but the scores at final follow-up in the OAM group were not significant. The number of worse cases in the OAM group was significantly larger than those in the OAL and ON groups. Therefore, the postoperative clinical outcomes of the OAL and ON groups were significantly better than their preoperative clinical scores and remained the same until the final follow-up. However, the clinical outcome of the OAM group improved until 2 years after AOG, but eventually decreased thereafter. Among the preoperative status in 3 groups, some items had significant differences in the following: The operative age of the ON group was significantly older than that of the OAL group, and the recipient area of the ON group was significantly larger than that of the OAL group. The preoperative JOA score of the ON group was the smallest among the 3 groups. The preoperative KL classification of the OAL group was the smallest among the 3 groups. These differences might affect the above different results among the 3 groups. However, we think the disease characteristic of OAM may be different with these of OAL and ON.
In the previous study, Nakagawa et al. 15 reported that the outcome of AOG only in the femoral condyle with no procedure in exposed subchondral bone of tibia was good. The study included 17 patients and 18 knees and had a mean follow-up of 30 months. 15 The difference between the above study and our present study was follow-up period. Laursen 18 reported the outcome of femoral resurfacing using the UniCAP implant without tibial component. In this study, patients younger than 35 years or older than 65 years with a valgus or varus malalignment exceeding 5° were not offered treatment. Their indications were almost the same as those in our study. Approximately 47% of the implants were revised within 7 years to arthroplasty due to the progression of cartilage lesions. 18 Its outcome was the same as that in the OAM group in our study. Heir proposed that patients with focal cartilage lesions have major problems with pain and functional impairment. 19 In our study, the OAL and ON groups had focal cartilage lesions in their tibia, but their midterm outcomes remained good.
Several studies reported good midterm outcomes of mosaicplasty. Solheim et al. 20 proposed that mosaicplasty in a single cartilage defect size of 1-5 cm2 of the femoral condyle resulted in a better outcome than microfracture within a 10-years follow-up. Gudas et al. 21 reported that mosaicplasty-treated patients had significantly higher ICRS and Tegner scores than the microfracture-treated patients at a mean follow-up of 10.4 years. Krych et al. 22 insisted that patients treated with AOG maintained a superior level of athletic activity compared with those treated with microfracture. Ebert et al. reported that patient who had mosaicplasty had a good clinical outcome within a follow-up of 9.8 years in terms of Lysholm score, KOOS, isokinetic muscle strength or radiographic osteoarthritis. 23 Matrix-induced autologous chondrocyte implantation provided high satisfaction levels and tissue durability beyond 10 years. 24 In our study, the clinical outcomes of OAL and ON groups remained good at a mean follow-up of 98.4 months.
Hangody et al. 3 and Jakob et al. 4 reported that the clinical outcome of AOG in femoral condyle was better than that of the AOG in the patellofemoral joint, but no significant differences existed between the lateral and medial femoral condyle. However, in our study, the clinical outcome of the OAL group was significantly better than that of the OAM group at a follow-up of more than 5 year. With regard to AOG for knee osteonecrosis, Kumagai et al. 24 and Nakagawa et al. 12 insisted that good clinical outcomes were obtained. Because the generally accepted indication for AOG is focal chondral defects, not bipolar OA, as in our group, the comparison with other studies is difficult. However, in our study, the clinical outcomes of the ON group remained good at a mean follow-up of 98.4 months.
Lamplot et al. 25 reported that only a few studies investigated the outcomes of revision surgery after a failed attempt at cartilage repair or reconstruction, while several studies have reported outcomes following a variety of cartilage restoration procedures. Lesions frequently occurred in the medial femoral condyle, and the same finding was reported in our study. Minas et al. 26 reported that a relatively high proportion of patients underwent realignment osteotomies concurrently with revision cartilage restoration. In our study, 3 patients underwent revision surgery. In the OAM group, one had total knee arthroplasty at 61 months (operative age, 76 years) and another had total knee arthroplasty at 123 months (operative age, 70 years) after AOG, 1 had high tibial osteotomy at 96 months (operative age, 49 years) after AOG.
After exposing the tibial subchondral bone, at second-look arthroscopy (19 months after AOG), the recipient and opposing articular surfaces of the patients in this study did not worsen. Bowland et al. 27 stressed that the effects of osteochondral defects on the contact stress of the surrounding articular cartilage had been studied experimentally. Elevated contact stress had been shown to occur in the rim of osteochondral defects with peak stresses and increased contact stress gradients also occurring in the cartilage surrounding the defect. Nosewicz et al. 28 indicated that when grafts decrease to less than 1 mm below congruency, cartilage thickening may occur, in order to compensate for the difference between the surface profiles of the graft and host cartilage. In clinical cases, Nakagawa et al. 29 reported that an isolated osteochondral plug depression of not greater than 1 mm could still promote acceptable cartilage healing leading to good clinical outcomes. However, plug protuberance at mosaicplasty should always be avoided. 29 Moreover, Johnson and LaPrade 30 suggested preventing the placement of a proud autograft. If a smooth surface was seen in the recipient site during second-look arthroscopy, the cartilage degeneration in its opposing articular surface did not become worse after mosaicplasty. 12 Therefore, no procedures were performed in the exposed tibial subchondral bone area in the OAL and ON groups, and this did not affect the clinical outcome.
The limitations of our study were as follows: small samples (22 patients and 22 knees) and midterm follow-up (mean follow-up of 98.4 months). There were preoperative differences between patients in the 3 groups, when considering age, recipient area, JOA score, and degree of osteoarthritis according to the Kellgren-Lawrence classification.
In conclusion, we examined the midterm clinical outcomes of AOG only in the femoral condyle without treating the tibial plateau with subchondral bone exposed, in 22 patients and 22 knees, and the mean follow-up period was 98.4 months. The postoperative clinical outcomes of the OAL and ON groups were significantly better than their preoperative clinical scores, and remained the same for about 8 years. However, the clinical outcome of the OAM group improved until 2 years after AOG, but eventually decreased thereafter.
Supplemental Material
Enago-Certificate-YASLKJ-3. – Supplemental material for Midterm Outcomes of Autologous Osteochondral Graft Transplantation Only in the Femoral Condyle without Treating the Tibial Plateau with Subchondral Bone Exposed
Supplemental material, Enago-Certificate-YASLKJ-3. for Midterm Outcomes of Autologous Osteochondral Graft Transplantation Only in the Femoral Condyle without Treating the Tibial Plateau with Subchondral Bone Exposed by Yasuaki Nakagawa, Shogo Mukai, Takahiro Maeda, Shota Akamatsu, Kentaro Satomi and Ryota Nakamura in CARTILAGE
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was obtained from the institutional review board (13-20).
Informed Consent
Written informed consent was obtained from all subjects before conducting this study.
Trial Registration
Not applicable.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.