
Abstract
This review presents the current understanding of the etiology, pathogenesis, and how to diagnose and treat osteochondritis dissecans (OCD) at the elbow joint followed by an analysis of particular characteristics and outcomes of the treatment. OCD is seen in patients with open growth plates (juvenile OCD [JOCD] and in adults [AOCD] with closed growth plates [adult OCD). The etiology at smaller joints remains as unclear as for the knee. Mechanical factors (throwing activities [capitulum] seem to play an important role. Clinical symptoms are unspecific. Thus, imaging techniques are most important for the diagnosis. In low-grade and stable lesions, treatment involves rest and different degrees of immobilization until healing. When surgery is necessary, the procedure depends on the OCD stage and on the state of the cartilage. With intact cartilage, retrograde procedures are favorable while with damaged cartilage, several techniques are used. Techniques such as drilling and microfracturing produce a reparative cartilage while other techniques reconstruct the defect with osteochondral grafts or cell-based procedures such as chondrocyte implantation. There is a tendency toward better results when reconstructive procedures for both the bone and cartilage are used. In addition, comorbidities at the joint have to be treated. Severe grades of osteoarthritis are rare.
Keywords
Introduction
In a recent article on osteochondritis dissecans (OCD), 1 the etiology, pathogenesis, histology, and diagnostics have been thoroughly discussed with a special focus on the knee. A retrospective study 2 showed that the knee joint (61.7%) is the most often involved joint followed by the ankle joint (25%) and the elbow joint (2%-12%). The shoulder (0.6%) and the foot (0.3%) are rarely involved.2,3
In this article, we will focus on OCD in the elbow joint. The most common type of lesion is the capitellar osteochondritis dissecans (OCD), and it is a condition that can be a significant problem in adolescents especially in athletes. The aim of this article is to provide a review of the current literature and present how to best make the diagnosis and the possible available treatment of elbow osteochondritis dissecans with published outcomes.
Etiology and Epidemiology
At the elbow joint, a possible mechanical traumatic or repetitive microtraumatic etiology is proved by the fact that those OCD lesions are usually located at the capitulum humeri, either centrally or laterally and occur in almost all patients predominantly in the dominant arm. Patients are mostly males who indulge in an activity that involves throwing and/or manual work or gymnastics (in females).4-21 Only a few cases are located at the trochlea humeri and are most often seen in combination with a cubitus varus or are rarely located at the radial head probably accompanied with radial head instability.7,16,21 -26 However, Klekamp et al. 27 reported that capitellar OCD may produce radial head instability and Wu et al. 28 described concomitant lesions at the radial head in cases of capitellar OCD. Furthermore, it is still unclear whether an enlargement of the radial head is also an etiological factor or a sequela of the lesion occurring in the capitulum humeri.7,15
Regarding the load transmission, the radio-capitellar joint provides axial stability to the elbow with the capitellum transmitting approximately 60% of compressive forces across the joint.20,21,23,29
There are several biomechanical studies on the elbow joint with data contributing toward a biomechanical etiology of OCD lesions in elbow joints. A study in cadaveric elbows testing biomechanical properties of the radio-capitellar articular surface 30 showed that the medial portions of the radial head are the softest of all tested radio-capitellar segments. The central radial head is significantly stiffer than the lateral capitellum and at the capitellum there is a trend of decreased stiffness from medial to lateral. No significant difference between the stiffness of the radial head sites and the medial capitellum were found. It was supposed that the disparity of the stiffness might be an etiological factor in the development of a capitellar OCD. Another biomechanical study using fresh-frozen cadaveric upper limbs exhibited that valgus torque increases the contact pressure in the radio-capitellar joint. 31 Capitellar osteochondral defects increase elbow valgus laxity and contact pressure without increasing ulnar collateral ligament strain. When valgus torque is applied, contact pressure in the radio-capitellar joint is greater with a lateral than with a central defect. 31 Measurements of the bone density in different parts of the elbow joint assessed by computed tomography osteo-absorptiometry showed that the actual stress across the elbow is concentrated in the posterior part of the trochlea in humans.
Baseball pitching may produce excessive or repetitive stress against not only this part but also the anterior part of the capitellum. The majority of OCD lesions affecting the elbow are found in the anterior part of the capitellum in throwing athletes. 17 The results may support an important role of mechanical conditions in the cause of elbow OCD. 17 Clinically, bone bruises seen at the capitellum may be the precursor of an OCD lesion, for example, at the elbow. 32
Injuries of the ulnar collateral ligament (UCL) seem to play an important etiological factor in the development of elbow OCD. 33 In a radiographic examination 34 using magnetic resonance imaging (MRI) and normal radiographs (anterior-posterior and lateral view) adolescent patients suffering from capitellar OCD lesion (n = 19; mean age, 13.5 years, or patients with a tear of the ulnar collateral ligament (UCL) (n = 9, mean age 16.9 years, mean age) were controlled compared with normal controls (16, mean age 14.6 years). Interestingly, they found in the OCD and UCL group a significantly reduced carrying angle in comparison to the controls. In contrast, the distal humeral articular surface angle was significantly increased in OCD and UCL patients with an increased valgus at the distal humeral articular surface. No differences were found in the radial neck-shaft angle or anterior angulation of the articular surface at the distal humerus.
Regarding radial instability, there are only 2 reports on radial head subluxation or radial head dislocation accompanied with OCD lesions at the capitellum 35 or with a very rare OCD lesion at the radial head. 25 In contrast to these aforementioned biomechanically orientated studies in recent publication no greater analyses on other etiological factors such as genetics, blood supply to the elbow joint, for example, the capitellum for initiation of an OCD in the elbow joint are available.
Regarding the epidemiology of OCD lesions in the elbow joint different statements are made: It is of interest to note that the incidence of such lesions is reported to be high among young baseball players4,11 and the male to female ratio is reported to be 42:4 5 and 35:3 37 . Weiss et al. 2 studied the general incidence of OCD lesions in 317 patients with 334 involved joints. The majority of lesions (61.7%) were seen in the knee, followed by the ankle (25.4%) and the elbow (12%). The percentage of all lesions progressing to surgery was 35.3%; surgical progression for knee, ankle, and elbow joints was 33.5%, 31.8%, and 55.0%, respectively. Patients aged 12 to 19 years had a 7.4 times greater risk of progression to surgery for knee OCD lesions than 6- to 11-year-olds. 2
Diagnostics
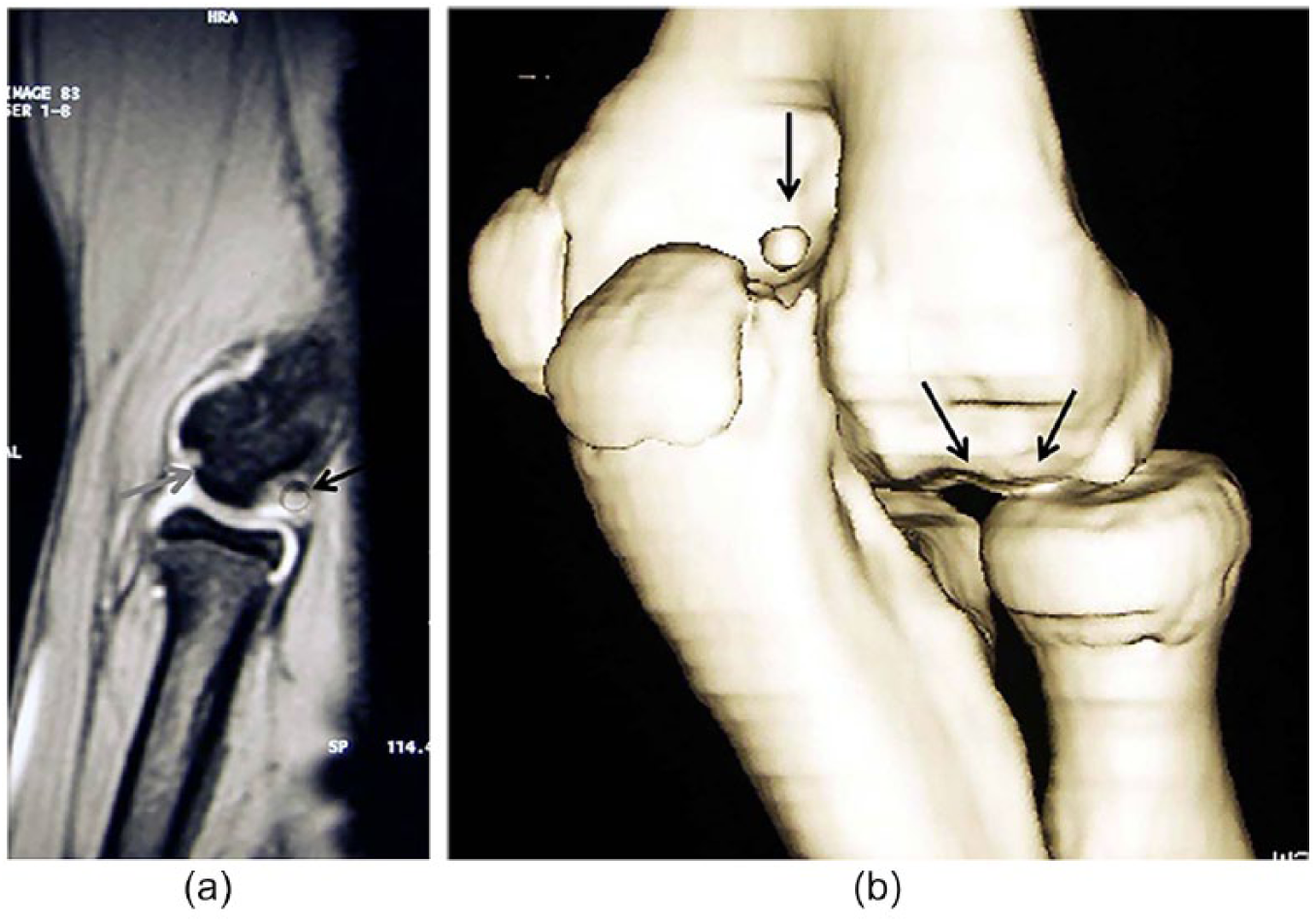
Conventional X-rays and MRI are the most important imaging tools also in OCD lesions of the elbow (Fig. 1).1,16,23,24,36,37 There are divergent data regarding the predictive value whether a lesion is a stable one or is unstable, which is important for the decision whether the treatment should be conservatively or surgical. Iwasaki et al. 38 found in a retrospective analysis that fragment stability is difficult to determine with an unsatisfactory low sensitivity (89%) and specificity (44%). Positive predictive value (PPV), and negative predictive value (NPV) were determined for fragment instability as evaluated by MRI. The PPV and NPV for fragment instability were 76% and 67% using the De Smet et al. criteria 39 and 75% and 57% according to the Dipaola et al. 40 staging. They also found a rather low PPV (76%, 75%) and NPV (67%, 57%).39,40 However, contrarily, Itsobu et al. 41 found that the stability evaluation with MRI staging of OCD lesions at the capitellum was correct in 94% of the patients when compared with the intraoperative findings, for example, ICRS (International Cartilage Repair Society) grading. They also found a sensitivity of 100% and a specificity of 80%. The positive predictive value and the negative predictive value were 93% and 100%, respectively, for diagnosing of lesion instability and the interrater reliability was rather high. 41 In another recent study, ultrasound has been used for preoperative determination of the fragment instability and has been compared with MRI. Surprisingly, ultrasound achieved superior results than MRI. 42 Further studies on the use of ultrasound diagnostic are needed to confirm these findings in a larger group of patients.
(
Regarding staging or classification of OCD lesions in the elbow joint, several systems have been used ( Table 1 ) . However, there are 3 systems particularly for staging elbow lesion1,36,48,101,102 that are most often used.
Staging systems used for classification/staging of capitellar OCD-lesions.
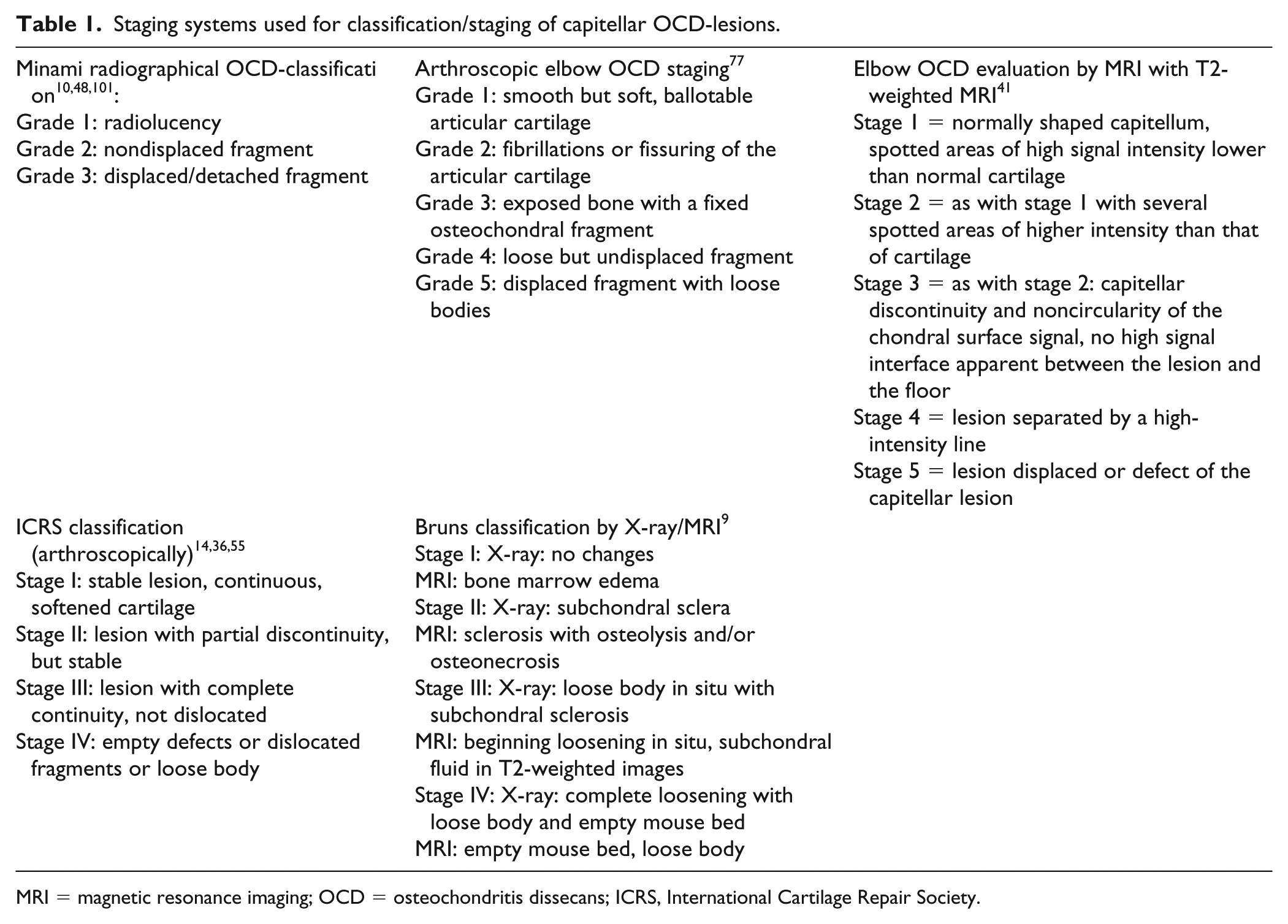
MRI = magnetic resonance imaging; OCD = osteochondritis dissecans; ICRS, International Cartilage Repair Society.
Treatment Options and Results
The general scientific problem as in other OCD lesions such as the knee joint is that no controlled prospective studies exist describing standardized procedures which take into account the stages of the lesions, the stages of the physes or standardized therapeutically regimes.43 -45 Furthermore, the different outcome scoring systems not being consistent makes scientific comparison even more difficult. It has been suggested 46 that only half of all lesions will be symptomatic and that only half of these will need surgical therapy after unsuccessful conservative treatment. In addition, there are no studies existing comparing prospectively different protocols in order to give reliable data for OCD lesion treatments at the elbow joint.
Conservative Treatment
In the past, most of the authors have recommended conservative treatment for stable initial lesions only, particularly in those patients with open physes.6,15,45,47 This treatment should include restriction from sports activities or other physical activities stressing the elbow joint and rest.15,16,23,47 -49 In initial stages with open physes, about 95% of the lesions may heal without surgery, 47 whereas conservative treatment is successful in only 50% of patients who have closed capitellar physes. Mitsunaga et al. 6 reported that, even with contained and stable lesions, problems remained in between 58% and 100% of the patients. After conservative therapy, two-thirds of the patients resumed partial participation in sports activities, whereas one-third left their initial level or changed to another sport. Fifty percent suffered from residual symptoms associated with the activities of daily life. 11 In contrast, Matsuura et al. 49 (91%) as well as Mihara et al. 47 (88%) found a rather high rate of healing after conservative therapy, but the outcome depended on the stage of the lesion and the stage of the physes, for example, the lower the grade of the lesions and with open physes success is better than in cases with higher grades and closed growth plates.47,49,50 Unstable lesions in patients with closed growth plates, fragmentation, or restriction of elbow motion of ≥20° do not benefit from conservative therapy.37,48,50 Success of a conservative regime is even less in noncompliant patients who continue with their sports activities.11,47 -49 Regarding adjuvant technical tools in a conservative setting a rather new treatment option of OCD lesions might be ultrasound. There are at least 2 recently published articles reporting on the use of low-intensity pulsed ultrasound51,52 for conservative nonoperative therapy of capitellar OCD lesions. However, owing to the small number of patients so far further studies on this kind of treatment are needed.
Surgical Treatment
A retrospective analysis exhibited that the elbow is the third often existing OCD lesion besides the knee and ankle joint needing surgery in 31.8% of the patients. 2 There seems to be consensus that advanced lesions, for example, unstable lesions, those with loose bodies or lesions with a fragmented cartilaginous layers or fragmented loose bodies need surgical intervention.20,23,37,53,54 As for other lesions, for example, in the knee joint, 1 several surgical procedures have been advocated even for the elbow joint. Surgical treatment includes different procedures such as:
Arthroscopic removal of loose bodies
Abrasion chondroplasty
Retrograde drilling
Microfracture/nano-drilling
In situ fixation
Autologous chondrocyte implantation (ACI)
Osteochondral autograft transplantation (mosaicplasty and osteochondral transplantation (OAT)
Costal osteochondral transplantation (COT)
The appropriate surgical intervention depends on many factors including lesion size, amount of lateral extension, and the presence of a stable cartilage cap as well as on the patients’ claim.15,16,21,60,62 The scientific problem is that reliable studies comparing different procedures prospectively do not exist. Almost all reports are retrospective level-4 studies.4,15,20,29,37,41,43,60 -68 Furthermore, there are no exact definitions of the different surgical procedures such as debridement and/or chondroplasty versus microfracturing or mosaicplasty versus OAT.4,15,20,29,37,41,43,60 -68 Even when authors had sampled a reasonable number of patients treated differently a comparison has not been done.29,69 Apart from this dilemma, simple surgical procedures can be divided in those with a
minimally invasive character procedures such as drilling either in a retrograde or anterograde manor to perforate the subchondral sclerosis surrounding the lesions, only indicated in stable lesions after a previous unsuccessful conservative therapy. 43
procedures with a rather “palliative” character, for example, simple removal of the loose bodies.15,29,48,69
When the cartilage layer is damaged and it is not possible to refixate the loose body, removal is the simplest procedure, but the lesions remain untreated and are accompanied with worst results.7,70 Thus, removal of loose bodies should at least be combined with bone marrow stimulation procedures such as drilling or microfracturing probably combined with the use of scaffolds in order to improve ingrowth of hyaline-like cartilage known as autologous matrix-induced chondrogenesis (AMIC). 71 Simple excision combined with superficial cartilage shaving does not produce good results, so far comparison is possible to the better results as seen with drilling or curettage.6,9 In addition, a long delay until surgery does not provide satisfactory results.6,9 All these procedures are not capable to restore the osteochondral unit completely because they produce hyaline like repair cartilage with a disorganized collagen fiber orientation being far away from the natural collagen structure known as Benninghoff arcades.15,67,72 -74 Thus, they should be defined as palliative procedure due to the low quality of the regenerated tissue. Nevertheless, there are somehow acceptable short- and medium-term results. The clinical advantage is that these procedures can be done arthroscopically. Bradley and Petrie 46 recommended that the choice of surgical technique should depend on the size of the lesion and integrity of the subchondral bone. They stated that microfracturing alone resurfaces the cartilaginous defects but do not reconstitute the subchondral bone. Even ACI produces only hyaline-like cartilage and there is uncertainty whether the subchondral bone can heal and the osteochondral unit can be reconstructed, even when ACI is combined with cancellous bone transplantation.75,76 In a systematic review on arthroscopic surgery of elbow OCD lesions, de Graaff et al. 43 criticized generally the poor quality of the articles on elbow OCDs comparing different surgical techniques such as fragment removal and debridement, fragment fixation, microfracturing, and OATS.
In athletes with OCD of the elbow, there was a trend toward better results after OATS or COT and the authors concluded that simple removal should be avoided. 43 However, some authors did recommend simple fragment resection7,70 only for capitellar lesions with a diameter smaller than half of the diameter of radial head. Several authors have combined resection with drilling, curettage, and trimming10,11,16,17,21,22,77,78 and acceptable short-term results have been reported.21,44 Even though Bexkens et al. 78 had good clinical results with fragment removal and microfracture, only 62% of patients in their study returned to sports.
In contrast, Mihara et al. 79 recommend not to remove fragments combined with drilling and instead suggest that reconstruction of the lateral margin of the capitellum is important for achieving good clinical results. They did not recommend removal with drilling because of following degenerative changes. 79 In 2007, Takahara et al. 48 found that fragment fixation or reconstruction provided significantly better results than fragment removal alone (P < 0.05).
Bone-Peg Grafting and Refixation
While Maruyama et al. 80 and Oshiba et al. 66 had used bone pegs only in stable lesion grade II other groups performed refixation even in cases with loose bodies with a wide range. The rate of reported success was between 50% and 91%.20,47,62,66,79 -81 Patients with open phases and central lesions did better than those with closed phases and/or lateral lesions, including the lateral rim of the capitellum.20,62 Patients in whom the lesions had been refixed either with bone pegs,20,66,79,80 with resorbable pins62,79 or wires 81 seem to exhibit better results than those after bone marrow stimulation procedures.
Reconstruction
Only reconstructive techniques such as mosaicplasty14,65,82,83 or OATS67,74,84 are capable of repairing the lesions more or less completely. In principle, and theoretically, only OATS—the osteochondral grafts—are capable of reconstructing the osteochondral unit. With this technique, one may implant the plugs in an overlapping manner,67,74,84 in a mosaic pattern,73,88 or as a single plug 85 and a variant of the technique had been published already in 1964 by Wagner. 1 The cartilage layer of these plugs has the inborn normal architecture of collagen type-II fibrils.72,86,87 Mosaicplasty is a technical variant of the osteochondral transplantation procedure. In contrasts to OAT, in mosaicplasty, plugs are implanted not in an overlapping manner but as a mosaic with remaining clefts between the single plugs. 73 Thus, defects are filled with cartilage covering only 60% to 70% of the defect area. 73 The remaining gaps between the single plugs will be filled up spontaneously with fibrous tissue in growing from the subchondral bone only after transplantation.67,73,74,84 This might have an influence on the quality of the reconstruction and thus on the grafts stability and on the resulting clinical outcome.67,73,74,84 This particular technique had been introduced and studied by Hangody et al. 88 with several experimental and clinical studies. Unfortunately, in the literature, the terms mosaicplasty and OAT are sometimes used synonymously without any clear definition or differentiation.
Regarding the fit of osteochondral transplants harvested from the knee joint and transplanted into the capitellum there are at least 2 interesting articles.89,90 Mapping of the cartilage depths at the recipient site at the capitellum and the donor site (knee joint) by means of MRI in both sites exhibited that best match for capitellar reconstruction is with the posterior aspect of the medial condyle and the distal-most aspect of the anterior-lateral femoral condyle. 89 A topographic analysis on the congruence of the capitellum and distal femur using computed tomography scans showed that there is a less than 0.1-mm difference in the topographic articular surface match among the 4 commonly used donor sites of the distal femur and the capitellum. The findings suggest that all 4 donor sites provide close articular matching for the capitellum articular surface, with the lateral trochlea articular surface providing the best match. 90
The COT procedure is using osteochondral plugs harvested from ribs.55,61,79 In comparison with osteochondral articular grafts, these transplants have a completely different structure of the cartilage and lacks the typical osteochondral transition. 91 Nevertheless, based on their convincing mid-term results of between 25 and 45 months postoperatively, several authors recommend that reconstructive techniques, such as mosaicplasty,14,65,82,83 OAT,13,20,56,58,67,74,84,92 or COT grafting harvested from ribs55,61,79 could be used since they are more successful than nonreconstructive procedures, at least for larger lesions (>50% of the capitellar size) or those involving the lateral capitellar margin.11,27,55,56,79 For all reconstructive techniques it seems to be of importance that the lateral capitellar rim is reconstructed to achieve optimal results.92 -94
Osteochondral Autograft Transplantation
Transplanting osteochondral grafts in an overlapping manner is suggested to result in a more stable reconstruction. 73 To our knowledge, Shimada et al. 56 were the first to report on the use of OAT for OCD lesions of the capitellum resulting in an improvement of the average radio-capitellar congruity from 35.7% preoperatively to 64.2% at follow-up (mean 25.5 months) and that the score also improved during the same time. Kolmodin et al. 93 found that autograft reconstruction was found to yield reliable outcomes regardless of lesion location, as 87% of lateral lesions had excellent or good outcomes while 91% (21/23) of central lesions had excellent or good outcomes.
A survey of the literature on the significance of lesion location of capitellar OCD lesions showed, regardless of the location, that after OAT in 87% of lateral lesions and 91% of central lesions excellent or good results were found. 93 In addition, there was a trend toward better results after a more aggressive reconstructive surgery of lateral lesions particularly for those including the lateral capitellar rim. Furthermore, the authors found that the failure rate of nonreconstructive procedures was significant for lateral lesions and that one study reported a failure rate of 44% for bone peg grafting. 93 Matsuura et al. 91 reported the largest cohort (87 out of 103) of patients with capitellar OCD lesions treated with OAT. The authors compared central capitellar lesions with lateral ones, but epidemiological data did not show any important difference between either group. After OAT treatments, they found a rather high rate of return to previous sports activities among patients (100% for central and 86% for lateral lesions). Overall, they found a rather good clinical and radiological outcome but patients with lateral lesions exhibited significant radial head subluxation and arthritic signs. The MOCART (magnetic resonance observation of cartilage repair tissue) score did not show obvious differences between the groups. 91
Kirsch et al. 68 gave a recent overview on 6 reports on OAT with transplants taken from the femoral condyles to repair the capitellar OCD lesions. The ability for young athletes to return to the same or higher level of sport after OAT of the capitellum appears to be remarkably good. This systematic review found that 94% (119/126) of patients were able to return to a high competitive level of sports. Four of the 7 studies reported a 100% return to sport rate, whereas the other 3 reported rates ranging from 83% to 94%. Unrestricted return to athletic competition was possible by approximately 6 months (range, 3-14 months) in most patients. Overall, this study demonstrates that surgeons and patients can anticipate a high likelihood of returning to competitive athletics after OAT for OCD of the capitellum. 68
There are at least 6 more reports on the OAT procedure used for treatment of OCD lesions in the elbow joint.20,67,74,84,85 All these studies confirmed the good to excellent results in almost all patients with an excellent and almost complete integration of the grafts with a minimum of osteoarthritic changes. Another report included at least a rather large number of patients treated with OATS but did not compare the results of 19 patients to other techniques that have been included in the report. In addition, it is unclear whether they performed a mosaicplasty or OAT procedure. 20 Most recently, Bae et al. 85 reported on the successful use of single osteochondral plugs for capitellar reconstruction. Unfortunately, they had a rather short follow-up. Nevertheless, their results are similarly promising like others reporting on the OATS procedure.
Costal Osteochondral Graft Transplantation
There are only 3 reports on the use of COT.55,61,79 Mihara et al. 79 were the first to report the use of osteochondral autografts obtained from the ribs for the treatment of advanced OCD lesions at the capitellum. Seven out of their 27 male basketball players had been treated with this variant and 6 of those COT-treated patients returned to baseball playing at 4 months postsurgery. Even when they followed up 27 patients with a rather different kind of treatment, they did not compare the results between groups with different used techniques. The 2 other reports on 26 patients 55 and 22 patients 61 exclusively used COT. Both studies found in almost all patients high percentage of good to excellent results after a mean follow-up of 27 to 39 months.55, 61 Furthermore, both groups mentioned minor additional necessary surgeries (5/26 patients, 55 4/22 patients, 61 ) including screw removal, loose body removal, and shaving off of spur formations. But, theoretically, it seems to be disadvantageous with this technique as the COT does not reconstruct the osteochondral transition. 92
Mosaicplasty
Iwasaki et al. 14 were the first to report on this particular technique for treatment of OCD lesions at the capitellum.14,82,83,88 In a small series of 8 teenage patients, 7 of the patients had excellent results at a follow-up at 24 months. 82 Radiographically, graft incorporation and a normal contour of the subchondral cortex were found in all patients 82 at 4 years postoperatively. Similar results have been reported by Ovesen et al. 65 on a rather small group of patients (n = 10) with an advanced OCD at the capitellum humeri with excellent results in 80% at a mean follow-up of 30 months (range, 10-60 months). Most recently, Funakoshi et al. 95 found rather good and satisfactory results even in cases with involvement of the lateral rim with a good graft integration seen on MRI and clinically a rather high rate of return to the preoperative sport level.
Allograft Transplantation
Mirzayan and Jim 63 are the first and still the only group found to report on the use of allografts to repair advanced capitellar OCD lesions. All 9 basketball players who had been treated with fresh femoral allografts returned to throwing and were still active in their sport or played at least 2 years of baseball before leaving the sport unrelated to the elbow problems. 63
Autologous Chondrocyte Implantation
As for allografts also for ACI very little is known on its use in the treatment of OCD lesions in the elbow joint. Only 2 articles have been found related to cell transplants for elbow OCD. Sato et al. 96 reported already in 2004 on tissue-engineered cartilage for the treatment of elbow OCD lesions. Patzer et al. 97 recently reported on an all-arthroscopic surgical technique for 3-dimensional ACI implantation to treat osteochondral lesions of the humeral capitellum.
Additional and Preventive Procedures
It is important to treat additional comorbidities that might be responsible for the initiation of the OCD lesions and to avoid recurrences. But little is known about these potentially causative conditions. Kiyoshige et al. 98 reported on results from seven lesions where the patients were suffering from an elbow valgus malalignment. The malalignment could be treated with a closed wedge-osteotomy of the lateral epicondyle to reduce load on the radio-capitellar joint, for example, the capitellum. Six out of the 7 baseball players returned to their full preoperative sports activity. Furthermore, an unstable elbow joint due to ruptured ulnar collateral ligaments should be stabilized19,33 because such a ligament insufficiency is also believed to be a possible etiological factor of capitellar OCD lesions. 12
Long-Term Results
Little is known about long-term results on the different elbow OCD treatment conditions. No studies exist comparing different therapeutic regimens in a long-term follow-up. Takahara et al. 4 determined the long-term outcome of capitellar OCD lesions for 53 patients. The average age of the patients at treatment was 16.6 years (range, 10-34 years), the average follow-up was 12.6 years (range, 3-25 years). Seven of 14 (50%) patients who were treated conservatively and 18 of 39 (46%) who were treated by surgical removal of the fragment were found to have residual elbow symptoms associated with daily living activities (poor outcome). The initial radiographs of the elbow were available for 45 patients; a poor outcome was seen in 6 of 19 (32%) early lesions and 13 of 26 (50%) advanced lesions. Fourteen elbows had evidence of osteoarthritis on the initial radiographs, and a poor outcome was seen in 9 (64%) of these elbows. After removal or detachment of the fragment, 7 osteochondral defects were assessed as large, and all 7 had a poor outcome. They also found that conservative therapy resulted in a success rate of 70% in JOCD cases but continued stress to the affected elbow worsened the result. 4 Regarding the difference between JOCD and AOCD, they found that those with JOCD had better results after conservative treatment than AOCD patients. AOCD patients benefited more from surgical therapy surgical therapies. Those with a lesion size less than 50% of the capitellum did better than those with lesions larger than 50% of the capitellum. 4 Bauer et al. 7 found after a mean of 23 years following surgical fragment removal that nearly 50% of the patients older than 16 years at the date of treatment and 25% of the young patients (younger than 16 years) still suffered from symptoms. Similar results were seen regarding degenerative changes on X-rays. Ueda et al. 70 reported on patients with a follow-up of 5 years in minimum (minimum 5 years, range, 5-12 years) treated with arthroscopic fragment resection and divided their patients in group 1 with lesions smaller than the half of the radial head diameter and in group 2 with lesions large than the half of the diameter. The mean follow-up was 8 years (minimum 5 years, range, 5-12 years). Unfortunately, they did not use one of the usual scores. Their most important finding was that the range of motion improved significantly in both groups without any significant postoperative differences between the groups. 70 Radiologically, there was no severe osteoarthritis postoperative differences at follow-up but the rate of osteoarthritis had increased in 29% of the patients in group 1 and in 43% in group 2 with a significant difference between groups. 70
Similar results after arthroscopic debridement or removal had been published by Brownlow et al. 64 After a mean follow-up of 6.5 years, the authors found problems in 38% of the patients in terms of recurrence of catching or locking and nearly 15% of them had to give up their preferred sport. In contrast to these reports on resection and/or debridement, more recent articles report on reconstructions of advanced capitellar OCD lesions. Using the OATS procedure, Vogt et al. 84 reported in their long-term follow-up study (8-14 years postoperatively) in 7 out of 8 patients, a good or excellent clinical result with a graft integration in all and a congruent surface in 6 of 7 patients and only in 2 out of 7 patients, radiographically a mild osteoarthritis. These long-term outcomes were confirmed by Weigelt et al. 67 who found excellent and good results after a mean postoperative period of 7 years (range, 3-14 years) in 14 out of 18 with a free range of motion, excellent graft integration, and only mild (radiographically) osteoarthritic signs in only 3 of the 14 reexamined patients. 67
Conclusion
The natural history of OCD of the elbow is not well-known. But it is obvious that mechanical stress at the elbow, for example, the capitellum, is supposed to be the most important etiological factor because of the fact that almost all of the patients are involved in sports activities that are stressing the elbow joint.
Conservative treatment seems to be successful only in initial early lesions without damage or loosening of the cartilage layer in young patients with still open physes. Thus, in many patients, conservative therapies seem reasonable if the growth plates are still open.
The best therapy for elbow OCD patients may be early diagnosis and prevention by avoidance of the heavy joint disturbing activities. Nevertheless, there is a large group still suffering from different symptoms after such a nonsurgical therapy. Although there are a numerous articles reporting on different surgical procedures mentioned above, there is no reliable prospective study comparing these surgical treatment options in a prospective and randomized manner. However, it seems clear based on existing reports that it is not an advisable procedure to simply remove loose bodies and debride the ground base of the lesion. Furthermore, bone-marrow stimulating procedures are not capable of restoring the damaged osteochondral area, but they still are those techniques that are performed most often but with suboptimal results.18,37
Instead a clear trend toward better results is seen after refixation of fragments as well as after any reconstructive procedure, for example, OAT, mosaicplasty, or COT.20,43 Especially for a return to sport, the use of osteochondral autografts seems recommended. 99 The reports on OAT experiences with a long-term follow-up are in our opinion convincing.67,84 The arthroscopic techniques may be tempting to use but still there is a need of more evidence to determine the superiority of the open versus arthroscopic techniques in treating elbow OCD. Thus, the question should not be whether it can be done arthroscopically or is to be done open with arthrotomy; instead the question should be which technique is the best one to reconstruct the capitulum with long-term durability. 7 Westermann et al., 100 when examining the return to sport after surgical treatment of capitellar OCD lesions, noted that “return to the highest preoperative level of sport was best after osteochondral autograft procedures (94%) compared with debridement and marrow stimulation procedures (71%) or OCD fixation surgery (64%).”
Based on the findings of this review, refixation of fragment could give symptom relief in capitellar OCDs but only the osteochondral autografting techniques restore the very important osteochondral unit with the transition between cartilage and subchondral area. We believe that guidelines can contribute to the choice of treatment in OCD of the elbow but should be based on methodologic well-designed research. In the treatment of capitellar OCD most techniques cannot restore the hyaline cartilage; the exception is the osteochondral autografting technique.
Footnotes
Author’s note
Mathias Werner is now affiliated with Vivantes Klinikum Friedrichshain, Dept of Osteopathology, Berlin, Germany.
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.