
Abstract
Background
Only a few studies exist that have assessed the efficacy of autologous osteochondral transplantation (AOT) treatment of osteonecrosis (ON) of the knee. The purpose of this study was to clarify the clinical and radiographic results of AOT performed on young patients with postcollapse ON of the knee.
Methods
This retrospective study included 14 young patients (6 men, 8 women, mean age 34.71 ± 5.41 years) with stage III knee ON undergoing AOT surgery. Mean follow-up time was 87 ± 10.23 months. The postoperative clinical and radiological evaluations were based on Hospital for Special Surgery (HSS) scores and plain x-rays. Paired t tests were used for the statistical analysis by SPSS software.
Results
Preoperative HSS (mean 66.86 ± 7.49 points) was significantly improved at mean 7 years to a postoperative HSS (mean 87.36 ± 8.63 points) (P < 0.001). The postoperative rangeof motion (ROM; 125.71° ± 4.74°) was not significantly different from the preoperative ROM (126.86° ± 7.13°) (P = 0.626). There was no progression of collapse observed in any knees at the last follow-up. No knees required any reoperations during the follow-up period.
Conclusion
Fourteen young patients with local ON of the knee were treated by AOT. No progression of bone collapse was seen and clinical improvement sustained at mean 7 years postsurgery. AOT seems to be a safe technique that can give long-term improvement and durability in young ON patients. However, large-sample and high-quality clinical trials are still needed in the future.
Introduction
Osteonecrosis (ON), a multi-etiological disease with the death of osteocytes as the end stage of several pathological processes, 1 is a debilitating disease that is poorly understood. ON of the knee can be classified as primary or secondary spontaneous ON of the knee (SONK). SONK typically affects a single condyle in elderly patients, generally the medial femoral condyle, and most patients do not have the risk factors usually associated with SONK.2,3 Secondary SONK is most commonly observed in young patients following exposure to corticosteroids and those with alcoholism and some chronic inflammatory diseases. As is well-known, it presents with several simultaneous foci with usually bilateral and multifocal involvement in the distal femur or proximal tibia, and the necrotic areas are larger than the lesions observed in primary SONK.2-5 Although the patients are younger, the suggested treatment alternatives are the same as that for SONK. 5
Various treatment methods for ON of the knee are available. These methods are based on staging and lesion size. ON of the knee can be treated nonsurgically or surgically. Nonoperative treatments include protected weightbearing, analgesics, and physical therapy. Several joint-preserving methods (arthroscopic debridement, core decompression, osteotomy, and osteochondral grafting), unicompartmental knee arthroplasty (UKA), and total knee arthroplasty (TKA) can also be implemented.5-7 Despite advances in knee arthroplasty techniques and improved durability of bearing surfaces, the risk of multiple revision arthroplasties persists due to osteolysis and loosening, particularly in young patients with high levels of activity. Therefore, preservation of the knee joint in patients with these diagnoses, especially in young patients with postcollapse ON, has attracted interest.
Autologous osteochondral transplantation (AOT), or mosaicplasty, is a well-established method for the treatment of focal cartilage lesions at the knee, talus, and humeral capitellum. AOT has been used for the treatment of osteochondral defects and collapsed lesions of the femoral condyles in spontaneous or secondary ON of the knee.8,9 The procedure can restore the structural integrity of condylar bone and the chondral continuity of the articular surface, with the goal of preventing or delaying condylar degeneration to the stage at which knee arthroplasty becomes the only viable option.
Some studies have assessed the efficacy of AOT4,8,9; however, most have reported only short-term follow-up of a small number of younger patients with postcollapse ON of the knee. Therefore, the purpose of this study was to determine the clinical and radiographic results of AOT performed on young patients with postcollapse ON of the knee after an average follow-up period of 7 years.
Materials and Methods
Patient Data
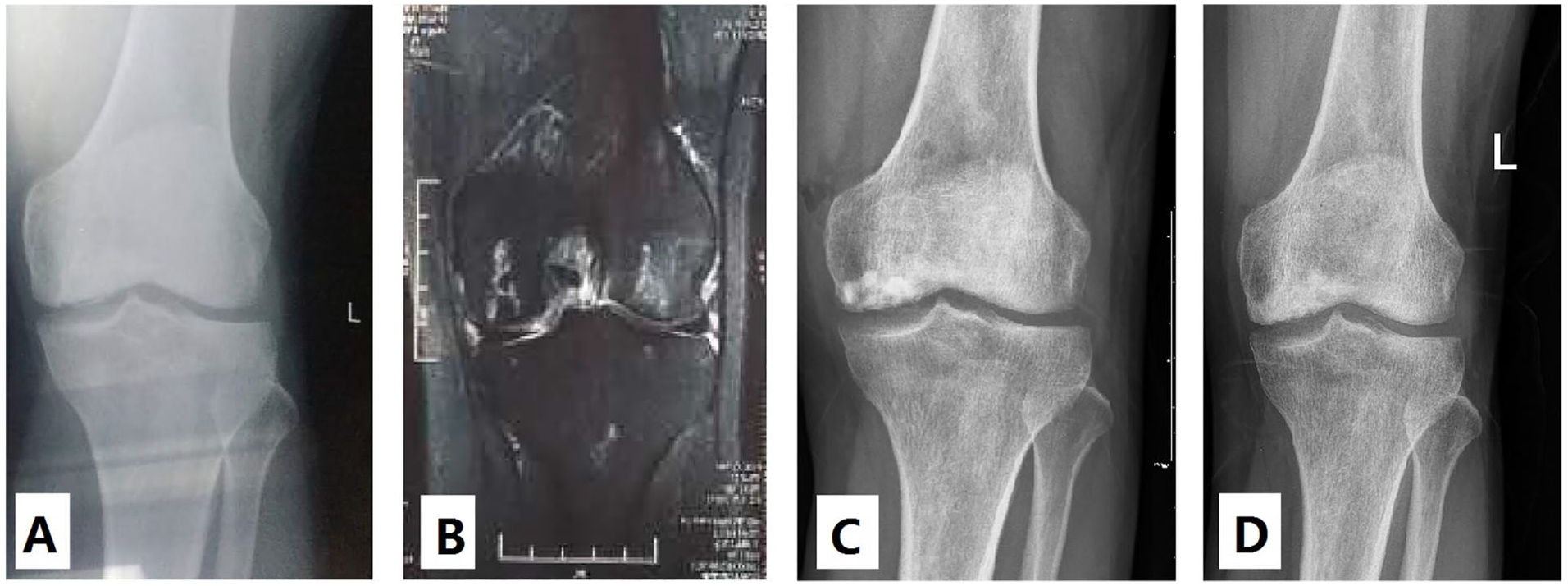
Between January 2004 and May 2011, 14 patients (6 men, 8 women; 14 knees) were diagnosed with ON of the knee at the authors’ institution. The mean age of the patients was 34.71 ± 5.41 years (range, 18-55 years), and the mean body mass index was 24.31 ± 3.22 kg/m.2 ON of the knee was diagnosed based on clinical and radiological findings. The modified Ficat and Arlet staging system was used for the radiological staging of ON 10 ( Fig. 1 ). In this system, stage I knees have normal appearance; stage II knees have cystic or osteosclerotic lesions, or both, with a normal contour of the distal part of the femur or the proximal part of the tibia, or both, with no subchondral fracture or flattening of the articular surface; stage III knees have a crescent sign or subchondral collapse; and stage IV knees have narrowing of the joint space, with secondary changes in the proximal aspect of the tibia (when the disease is confined to the femur), such as cysts, marginal osteophytes, and destruction of cartilage.
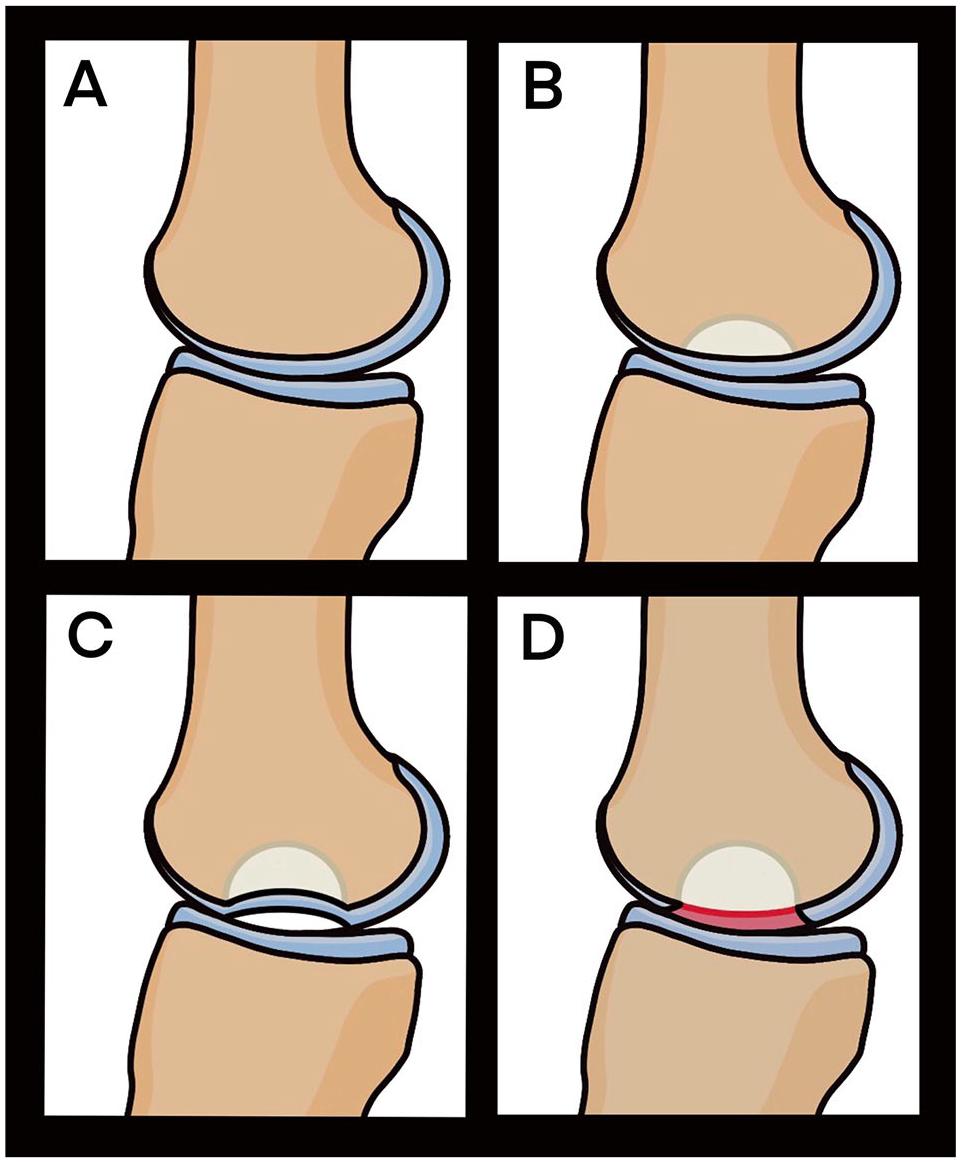
The modified Ficat and Arlet staging system. (
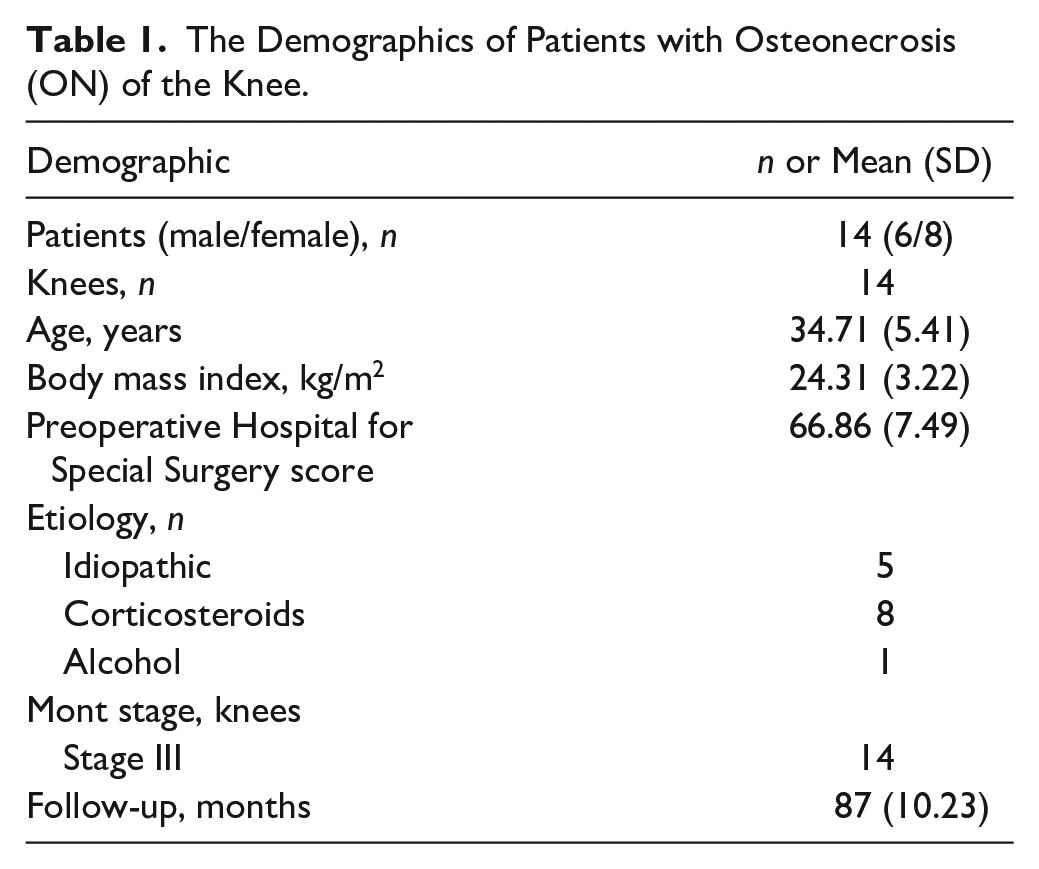
All patients were diagnosed with stage III (postcollapse stage) with small- and medium-sized (<4 cm2) focal chondral and osteochondral defects of the weightbearing surfaces of the medial femoral condyles, which we detected using arthroscopy. The mean follow-up period was 87 ± 10.23 months (range, 37-132 months). Table 1 presents the patients’ characteristics. The exclusion criteria were age more than 60 years, osteoarthritic changes in the knee joint (stage IV), large-sized chondral and osteochondral defects, and more than 2compartments with serious degeneration or collapse.
The Demographics of Patients with Osteonecrosis (ON) of the Knee.
This study was approved by the institutional review board of our hospital, and the procedureswere conducted in accordance with the principles of the Declaration of Helsinki. Written informed consent was obtained from all participants, which were stored in our hospital database to be used only for clinical research. All work is reported in line with the STROCSS (Strengthening the Reporting of Cohort Studies in Surgery) criteria. 11
Surgical Techniques
First, we performed diagnostic arthroscopy prior to the procedure to confirm adequacy of the available graft or to treat the coexisting pathology, and we carefully assessed the size and location of the necrosis, osteochondral defects, and combined disorder, such as anterior cruciate ligament injuries, osteochondritis, osteoarthritis, and meniscal injuries. Next, we made a standard midline incision and elevated it subcutaneously; eversion of the patella was not necessary. At the site of the lesion, any unstable cartilage flaps were debrided using a curette out to the edge of the viable and stable cartilage. This was followed by curettage of the necrotic bone, removal of the pathologic bone, and perforation of the sclerotic bone using an electric drill until a bleeding bone was encountered. For deeper and larger necrotic cavities, the bone defect was tightly packed with artificial bone (calcium hydroxyapatite) after debridement.
AOT tools (Arthrex, AR-1992) were used to harvest and transfer the osteochondral grafts. Osteochondral cylindrical donor grafts 5 to 10 mm in diameter according to lesion size and 15 to 20 mm in length were harvested from the less-weightbearing periphery of the articular surface of the femoral condyle. Approximately 1 to 5 recipient holes were made perpendicular to the chondral surface, and press-fit transplantation of each plug to the recipient hole was performed. All grafts were inserted at the same level around the healthy cartilage ( Figs. 2 and 3 ).
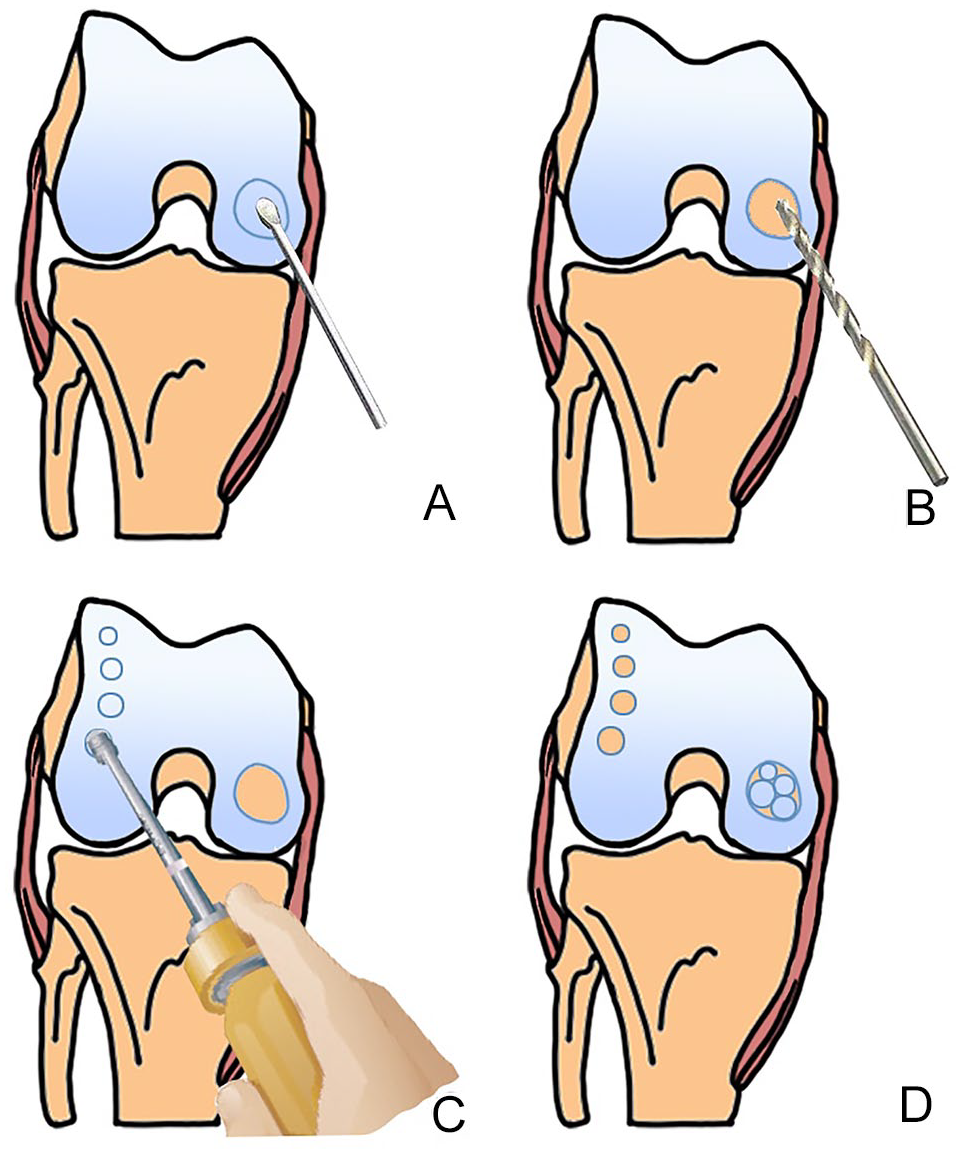
A schematic diagram of the autologous osteochondral transplantation (AOT) procedure. (
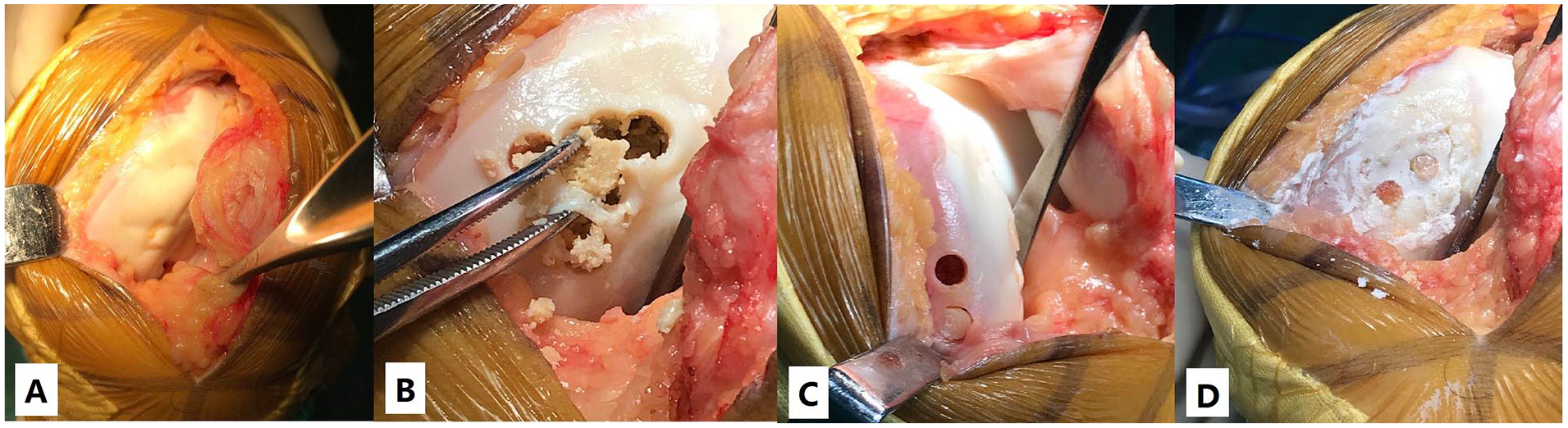
(
Postoperative Management
The same postoperative management program was adopted for all patients. The knee was dressed using elastic bandages, and the drainage was removed after 24 hours. Immobilization was applied for 2 weeks after surgery, and during this period, the patients were encouraged to perform isometric muscle-strengthening exercises. Patients were allowed to perform full range of motion (ROM) exercise after 2 weeks. The patients were instructed to perform touchdown weightbearing with crutches for 2 to 6 weeks and then gradually increase weight bearing until full weightbearing could be tolerated, between 12 and 16 weeks.
Outcomes Assessment
Clinical Outcomes
The Hospital for Special Surgery (HSS) knee rating scale scores at the latest follow-up were used to evaluate the clinical results. The HSS, which is used to evaluate postoperative recovery of knee function in adults, includes 5 main aspects: pain, function, muscle strength, absence of deformity, and ROM. The score standard has a maximum of 100 points (best possible outcome), and excellent, good, fair, and poor results are defined as HSS scores of >85, 70 to 84, 60 to 69, and <60, respectively.
Radiographic Outcomes
We used anterior-posterior and lateral X-rays in the radiographic follow-up after AOT surgery. Radiographic progression was defined as knee collapse aggravation or progression to joint space narrowing (stage IV) in the X-ray. The measured distance was between the lowest point of the knee collapse and the tangent of the femoral condyle. The radiographic progression was used to evaluate postoperative recovery. The radiographic progression was determined by 2observers independently. In the case of any disagreement, all the authors discussed the issue until a consensus was reached.
Statistical Analysis
The data were analyzed using SPSS version 21.0 statistical software (IBM Corp, Armonk, NY). Mean ± standard deviation and frequencies were calculated for all general demographic and routine clinical data. All data were expressed as mean ± standard deviation. To compare study variables during the study period, paired t tests were used. A statistically significant difference was defined as P < 0.05.
Results
Clinical Outcomes
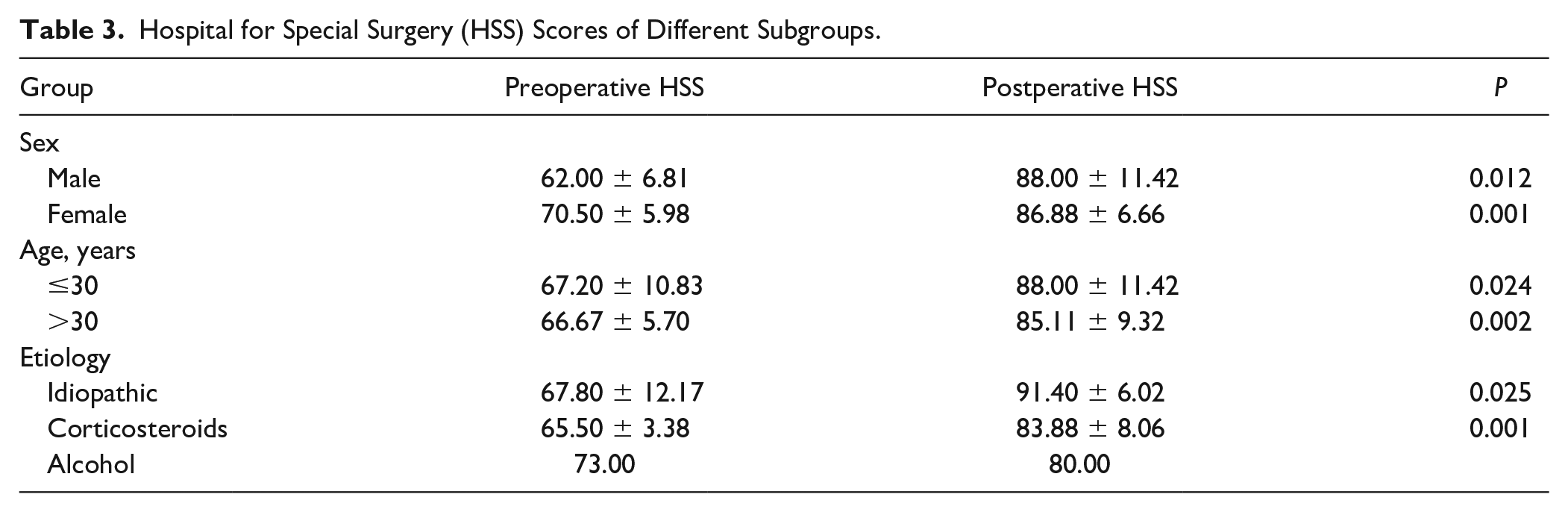
The postoperative HSS at the 1-year follow-up (mean, 73.29 ± 4.27 points; P = 0.001), 3-year follow-up (mean, 79.86 ± 5.17 points; P < 0.001), 5-year follow-up (mean, 84.43 ± 6.69 points; P < 0.001), and last follow-up (mean, 87.36 ± 8.63 points; P < 0.001) were improved compared with the preoperative HSS for all knees (mean, 66.86 ± 7.49 points). The postoperative HSS score was 9/5 (excellent/good). The postoperative ROM of the ON knees with stage III (125.71° ± 4.74°) was less than the preoperative ROM (126.86° ± 7.13°), but there was no significant difference between the pre- and postoperative ROM (P = 0.626). The pre- and postoperative outcomes of the clinical parameters are shown in Table 2 . The HSS scores of the different subgroups are presented in Table 3 .
Clinical Outcomes of Knees With Postcollapse ON After AOT Surgery.
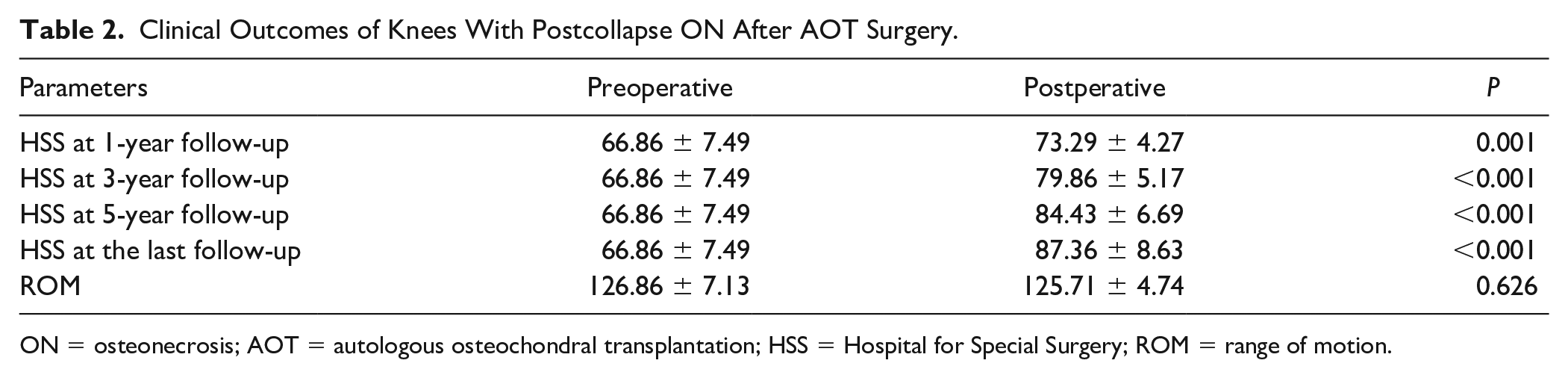
ON = osteonecrosis; AOT = autologous osteochondral transplantation; HSS = Hospital for Special Surgery; ROM = range of motion.
Hospital for Special Surgery (HSS) Scores of Different Subgroups.
Radiographic Outcomes
All knees showed radiographic evidence of graft healing. We did not find radiographic progression in any knees at the last follow-up ( Fig. 4 ) nor any significant differences in the complications after AOT.
(
Complications
No joint infection or deep vein thrombosis were observed in any patients. No knees required any reoperations during the follow-up period.
Discussion
ON of the knee is a relatively rare disease, with few reports focusing on treatment options.4,8,9 Although early diagnosis has been facilitated by the use of magnetic resonance imaging (MRI), no consensus exists for the treatment protocol. Therefore, surgeons usually have difficulties in selecting an appropriate method for treating these patients, especially young patients with postcollapse ON of the knee. The treatment for ON of the knee aims to preserve the knee joint, restore articular function, and prevent or delay joint degeneration and knee arthroplasty.
Nonsurgical treatments include observation, weightbearing with protection, drug treatment (nonsteroidal anti-inflammatory drugs, bisphosphonates, and prostaglandin I-2), and physical therapy. 12 However, the effects of these conservative treatments can be unsatisfactory. A previous study reported a clinical failure rate of >80% (26 of 32 knees) in patients with ON of the femoral condyle receiving conservative treatment. 13 Another study by Mont et al. 14 showed that only 8 of 41 symptomatic knees that were treated nonoperatively had a successful clinical outcome, and 8 of the 10 asymptomatic knees in the study had no additional symptoms or signs of radiographic progression; thus, they recommended observation of asymptomatic knees with ON. They also recommended the application of joint-preserving methods such as core decompression instead of conservative treatments for symptomatic ON of the knee.
UKA or TKA is usually advised in the treatment of elderly patients with symptomatic, high-grade (modified Ficat and Arlet stages III and IV) osteonecrotic lesions of the distal femur. 6 However, TKA and UKA are not suitable for young, active patients because most of them will likely outlive their prosthesis and require one or more revision surgeries. 15 Thus, some researchers have advocated joint-preserving surgical modalities such as arthroscopic debridement, 12 core decompression, 14 abrasion chondroplasty, 5 and microfracture. 16 Wiedel et al. 17 applied arthroscopic examination and debridement in the treatment of 10 knees with steroid-induced ON. They found that arthroscopic debridement provided consistent relief of internal derangement symptoms and, in some cases, improved functional status.
Core decompression has been reported to provide symptomatic relief. In a study by Mont et al., 14 72 of 91 (79%) knees had a good or excellent Knee Society Score (KSS; 61 had an excellent score and 11 had a good score) at a mean period of 7 years. Marulanda et al. 18 reported a 92% success rate with percutaneous techniques combined with limited weightbearing for 4 to 6 weeks and that KSS was >80 points in 56 of 61 knees. However, these procedures had successful clinical outcomes only in the patients with early-stage ON (i.e., before condylar collapse).
These techniques are based on the perforation of the underlying subchondral bone and enable the migration of pluripotent mesenchymal stem cells from the bone marrow into the defect zone. However, these methods have resulted in the formation of fibrocartilaginous scar tissue, in which the structural and biomechanical properties are inferior to those of the hyaline cartilage. 9 Osteochondral allo- or autografting are other joint-preserving surgical techniques that restore mature hyaline cartilage to the affected area in large, postcollapse, or complex lesions, providing an additional treatment option for ON of the knee.9,19 Görtz et al. 6 reported an 89% (25 of 28 knees) success rate in knees that underwent osteochondral allografting for postcollapse disease. The mean International Knee Documentation Committee (IKDC) pain score improved from 7.1 to 2.0, the mean IKDC function score improved from 3.5 to 8.3, and the mean KSS function score improved from 60.0 to 85.7 at a mean follow-up period of 2 years.
However, Bayne et al. 20 reported poorer outcomes in patients with corticosteroid-associated ON of the knee who underwent osteochondral allografting. The authors believed that revascularization of the allografts was poor because of the continuous use of high doses of steroids, resulting in graft subsidence. 20 In addition, the procedure involves the potential risks of disease transmission and immune graft rejection and also has a high cost. Therefore, in our study, we selected AOT for younger patients with postcollapse ON of the femoral condyle.
AOT has 3main advantages: (1) its technical feasibility and cost-effectiveness; (2) its reconstruction of the mechanically durable articular bone plate and the articular hyaline cartilage, with removal of collapsed tissue; and (3) its lack of inducing an immune rejection response. Thus, AOT is currently more widely used for ON of the knee. A key to its success is the size of the osteochondral articular cartilage defect. In our study, all patients had small and medium-sized (<4 cm2) focal chondral and osteochondral defects and achieved satisfactory results. Similarly, Fujita et al. 9 reported 3cases of steroid-induced ON of the femoral condyle treated successfully with graft AOT. In their study, the average defect size was 2.83 cm2 (range, 1.5-5.0 cm2), and all patients achieved satisfactory results.
In contrast, Wang 21 reported a poor result in a patient with a 6-cm2 defect who underwent osteochondral autograft. The author believed that cartilage lesions larger than 6 cm2 were associated with increased fibrous tissue formation and fissuring between the grafts and the host tissues. 21 Hangody et al. 22 suggested that a defect size between 1 and 4 cm2 is a promising factor for the success of the procedure. Tanaka et al. 23 advised that careful preoperative planning is required for the treatment of larger lesions of more than 4 cm2 because the defect lesion could not be completely covered with the osteochondral plugs.
Osteochondral autograft stability is critical in preserving the histologic properties of the cartilage and also to the success of the operation. Appropriate press-fit transplantation of each plug to the recipient hole is important to achieve a smooth and integrated articular cartilage.
Our present study has some limitations. First, the sample size was relatively small. However, to the best of our knowledge, this study enrolled the largest number of young patients with postcollapse ON of the knee who underwent AOT surgery to date. Second, the study did not include a control group. Because of the specific indications of this surgery for this uncommon disease, acquiring a large sample of patients or a matched control group is difficult. Third, we did not perform further MRI or computed tomography examinations because the patients recovered well and had no clinical symptoms at the time of follow-up. Further research is needed to more comprehensively elucidate the long-term clinical and radiologic outcomes of AOT surgery for postcollapse ON of the knee. Further studies with a larger sample size or a multicenter trial are also needed.
Conclusions
Treating postcollapse ON of the knee is considered a clinically challenging procedure. The AOT technique is a safe, effective treatment option for young patients with postcollapse of the knee. Excellent clinical and radiologic results were acquired after an average follow-up period of 7 years. In addition, AOT can prevent or delay the development of degenerative changes of the knee and does not compromise patients’ future options. We believe that AOT has the potential to become a salvage procedure for ON of the knee. However, large-sample and high-quality clinical trials are needed to test this belief.
Footnotes
Acknowledgments and Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by grants from Beijing Natural Science Foundation (No. 7204301).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the institutional review board of our hospital the approval number is 2006-055, and the procedures were conducted in accordance with the principles of the Declaration of Helsinki.
Informed Consent
Written informed consent was obtained from all participants.
Trial Registration
Not applicable.