
Abstract
Objective
Intra-articular corticosteroid injections (IACIs) are frequently used to suppress local inflammation, that is, in children with juvenile idiopathic arthritis (JIA). While systemic high-dosage corticosteroids are known to trigger osteonecrosis and result in osteochondral (OC) lesions, the effect of IACIs on joint cartilage and subchondral bone remains unclear. This study was conceived to analyze the coincidence of IACI and the subsequent manifestation of osteochondral lesions in a large cohort of pediatric JIA patients.
Design
Retrospective data assessment and comparative analysis of skeletally immature JIA patients treated with IACIs between 1993 and 2017.
Results
A total of 280 JIA patients were included in the analysis, the majority were girls (64%). Osteochondral lesions were present in 16 patients (5.7%) at a mean age of 10.7 years (range 4-14 years) and appeared on average after 63-month duration of disease. The majority was present at atypical locations such as the lateral femoral condyle. Multivariable analysis using cox regression showed that steroid injections were a risk factor to develop an OC lesion (hazard ratio [95%CI] for number of steroid injections per year, 8.20 [3.18, 21.16]).
Conclusions
Pediatric patients with JIA show a relatively high incidence of osteochondritic lesions, which present at an early age and in rather atypical locations and repetitive steroid injection need to be considered an associated risk factor.
Introduction
Juvenile idiopathic arthritis (JIA) is the most common rheumatic disorder in children younger than 16 years, and primarily affects the knee. The prevalence of the disease varies between different countries and regions and lies between 16 to 150 per 100,000 children. 1 Continuous inflammation leads to pain, joint effusion, joint stiffness, and reduced range of motion.2,3 The long-term consequences of the ongoing inflammation may include growth retardation and osteoarthritic destruction of the joint at a later stage. 3 The course of the disease and long-term prognosis is not predicable and varies from milder to more severe presentation with multiple complications. 4 While new pharmaceuticals such as immune-modifiers and biologicals have been highly successful in containing JIA and its most dire sequelae, 3 systemic and local application of corticosteroids both remain part of the therapeutic protocol.5,6
One adverse effect of steroid therapy is the development of osteochondral lesion in up to 40% of cases, reported for both, prolonged systemic application 7 and for repetitive high-dose intra-articular injection. 8 These lesions may progress, become instable and may require surgical treatment. 9
Pediatric JIA patients at our center are followed-up in close interdisciplinary collaboration between the orthopedic and rheumatology department. We observed multiple patients who presented with osteochondral lesions after repetitive intra-articular steroid injections. The aim of this study was therefore to evaluate whether there is a positive correlation between intra-articular corticosteroid injections (IACIs) and the appearance of osteochondral lesions in this patient group.
Methods
This retrospective study was approved by the local ethics committee (KEK-ZH 2015-0273). We reviewed all patients diagnosed with JIA, who were treated at the University Children’s Hospital Zurich between 1993 and 2017. Patients with incomplete medical records as well as other rheumatic disorders, or other known comorbidities and risk factors to develop osteonecrosis (ie, chemotherapy) were excluded. Following variables were collected: gender, type of JIA (oligarthritis, polyarthritis), age at initial JIA onset, duration of the disease (defined by either the time until an osteochondral (OC) lesion did appear, or until the last available follow-up). Furthermore, the number of injections were assessed for each knee individually. All available MRIs were included. Reported OC lesions were evaluated on the MRIs on their appearance, location and size at initial presentation, as well as progression during follow-up. Further information on any surgical intervention was collected.
Treatment and Diagnostic Algorithm
First-line JIA treatment consists of nonsteroidal antirheumatic (ie, ibuprofen) for 4 to 6 weeks. Patients with ongoing signs of local inflammation receive an intra-articular injection with a single body weight adapted dose Lederlon (triamcinolonhexacetonid, up to 20 kg, 20 mg; between 20 and 40 kg, 30 mg; and >40 kg, 40 mg). Clinical follow-up after the injection is at 2 weeks and 3 months. If symptoms persist, Methotrexat (MTX) or other biologics were added according to the treating physician’s decision. Children who presented with ongoing pain, locking symptoms, or reduced range of motion during the course of treatment receive medical imaging, that is, X-ray and/or magnetic resonance imaging (MRI).
Statistical Analysis
Descriptive data were presented as medians and interquartiles for continuous variables and as frequency (%) for categorical variables. Demographics and characteristics of both patient groups were compared by using the Pearson’s χ2 test or Fisher’s exact test for categorical variables and the Wilcoxon rank sum test for continuous variables. A subanalysis was performed in patients only with available MRIs to control for potential investigation bias. OC development (time to event) probability was assessed using Kaplan-Meier (KM) survival curves. The association between OC development clinical factors (age at diagnosis of JIA, gender) and treatment factors (number of steroid injections) was estimated using a Cox proportional hazards model. All analyses were performed using SAS software, version 9.3 (SAS Institute, Cary, NC); statistical tests were 2-sided. P values <0.05 were considered statistically significant for all analyses.
Results
Between 1993 and 2017, 280 patients (179 [63.9%] female and 101 [36.1%] male) with JIA were identified. The majority of the patients suffered from oligoarthritis (67.7%). The median age at JIA diagnosis was 5.9 years (0.58-16 years), with no difference with regard to gender, nor patients with or without a later identified OC lesions (P = 0.5). Due to practice of selective steroid injections, each knee was looked at separately, resulting in 560 possibly affected knees.
Osteochondral lesions were found in 24 knees (4.3%) in 16 patients (5.7%), with bilateral lesions in 8 patients (2.8%). The majority of the lesions (n = 12) presented at the lateral femoral condyle, followed by the medial condyle (n = 7), and other locations such as the tibia plateau and the patella (n = 5). The average size at initial presentation was 13.7 × 14.3 × 5.4mm, in anterior-posterior and lateral diameter, and depth (Example: Fig. 1 ).
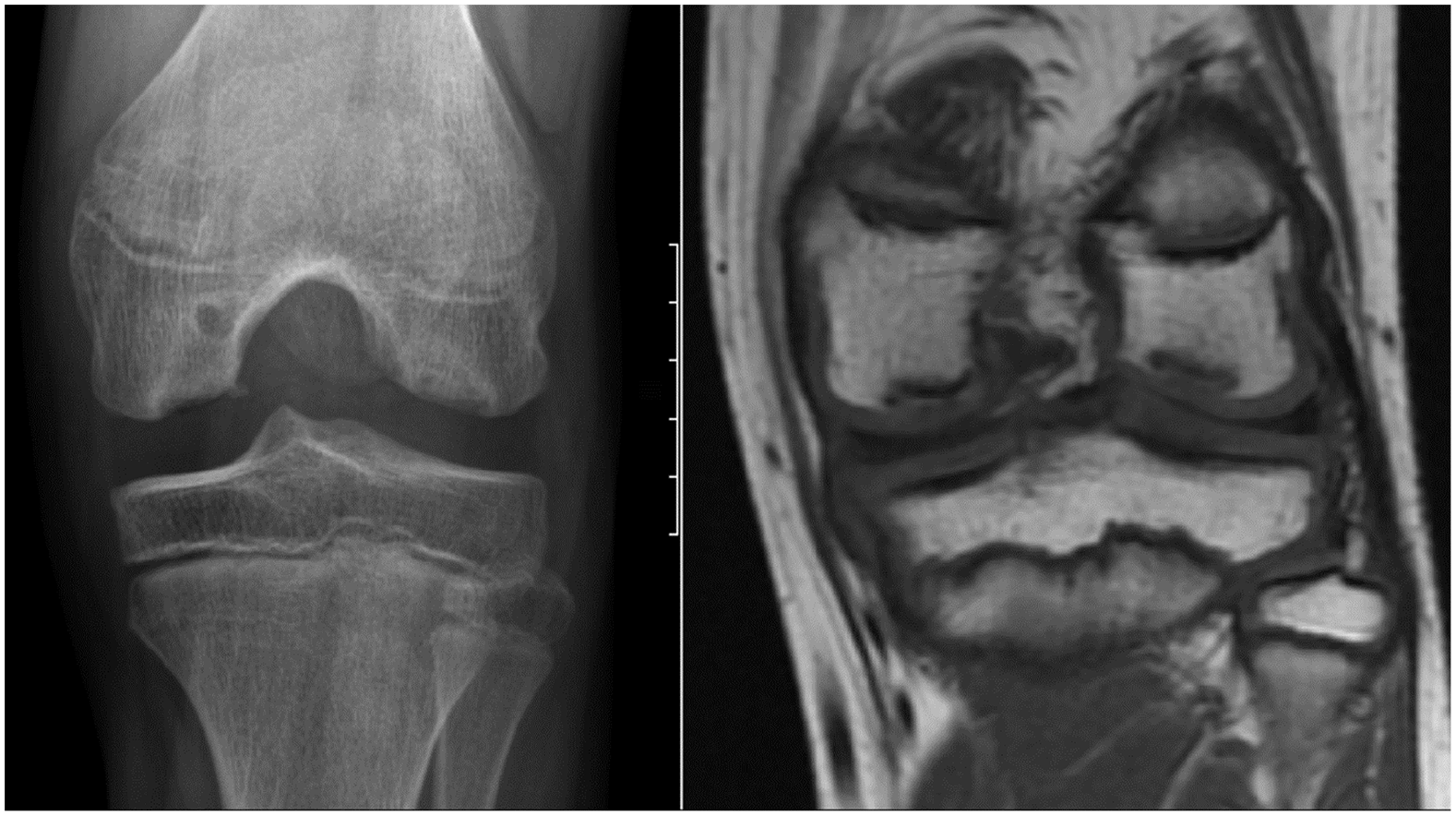
Radiographic aspects (left: X-ray “tunnel view,” right MRI T1) of osteochondritis dissecans (OCD) lesions in an 11-year-old female at time of diagnosis, with co-appearance of the typical OCD lesion at the medial aspect of the medial femoral condyle and a second lesion at the lateral condyle.
The mean age at OC diagnosis was 10.7 years (range 4-14 years). Patient who presented with an OC lesion had a slight earlier onset of the disease (5.3 vs. 5.9 years). However, neither age of onset (P = 0.5) nor duration of the disease (P = 0.36) was found to be statistically different between the 2 groups. Further no difference was found for the JIA subtype (P = 0.88) or gender (P = 0.12).
Six patient patients underwent arthroscopic treatment with partial removal (n = 4) or refixation (n = 2) plus/minus microfracturing. One patient, with extended lesions at the medial and lateral femoral condyle required bilateral total knee arthroplasty 5 years after OC diagnosis and progressive destruction of the joint. Seven patients were lost to follow-up, that is, due to referral.
Univariate analysis showed that OC lesions appeared statistically significant more often in knees which received steroid injections (P = 0.0007, odds ratio [OR] = 4.87; [1.79, 13.23]), knees with multiple steroid injections had a higher risk to develop OCD (P = <0.0001). Further multivariable analysis using Cox regression revealed that both steroid injections and the number of steroid injections per year had a statistically significant higher hazard ratio to develop an OC lesion ( Tables 1 and 2 ). The probability of development OCD is showed in the KM survival curve ( Fig. 2 ). A subsensitivity safety analysis was performed including only patients from both groups in whom an MRI was available. In total 109 MRIs were done in 73 in female and 36 in male patients. No significant difference was shown in patient characteristics compared with the entire population. This analysis did not confirm the association of steroid injections and the development of an OC lesion (P = 0.38, OR 1.41 [0.472, 4.22]). Last, no other adverse reaction related to the injections, such as infection, calcification, cutaneous atrophy, or cutaneous depigmentation was documented.
Cox Regression Multivariable Analysis: Prediction of Development of Osteochondritis Dissecans (OCD) in Knees (n = 560) of Patients with Juvenile Idiopathic Arthritis (JIA)—Presence of Steroid Injections (Categorical Variable) as Main Exposure Factor. a
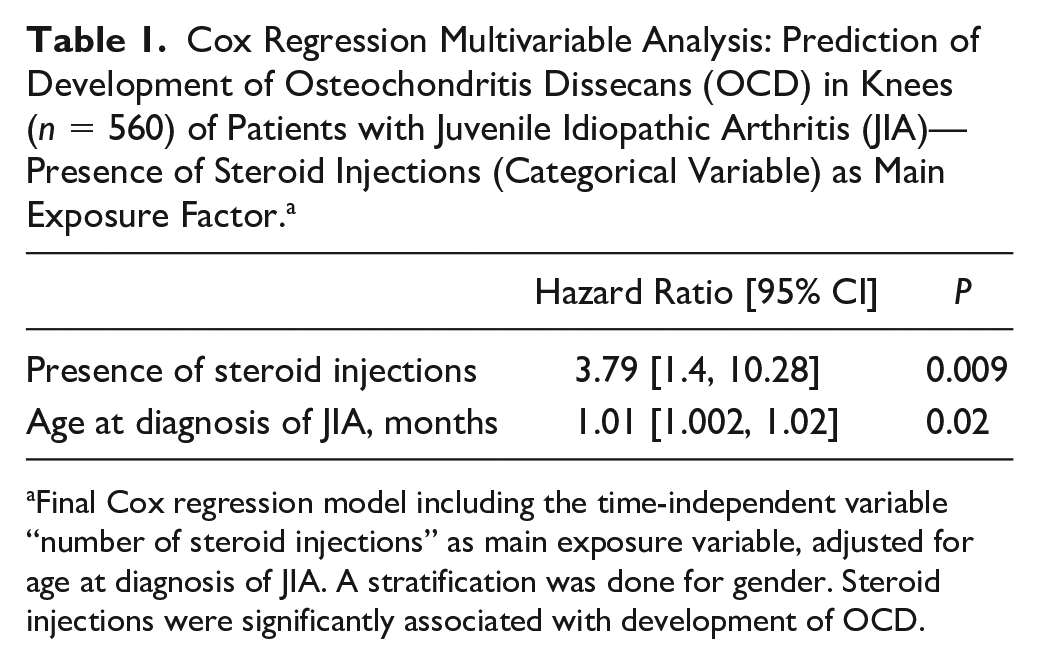
Final Cox regression model including the time-independent variable “number of steroid injections” as main exposure variable, adjusted for age at diagnosis of JIA. A stratification was done for gender. Steroid injections were significantly associated with development of OCD.
Cox Regression Multivariable Analysis: Prediction of Development of Osteochondritis Dissecans (OCD) in Knees (n = 560) of Patients with Juvenile Idiopathic Arthritis (JIA)—Number of Steroid Injections per Year as Main Exposure Factor. a
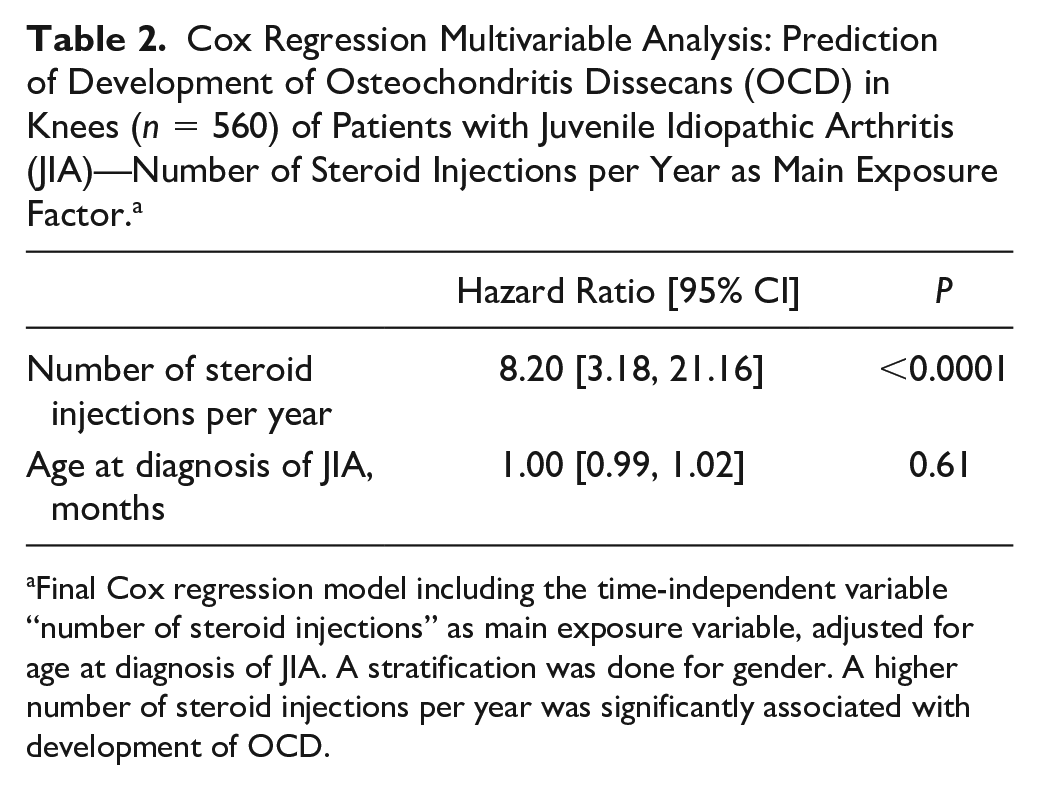
Final Cox regression model including the time-independent variable “number of steroid injections” as main exposure variable, adjusted for age at diagnosis of JIA. A stratification was done for gender. A higher number of steroid injections per year was significantly associated with development of OCD.
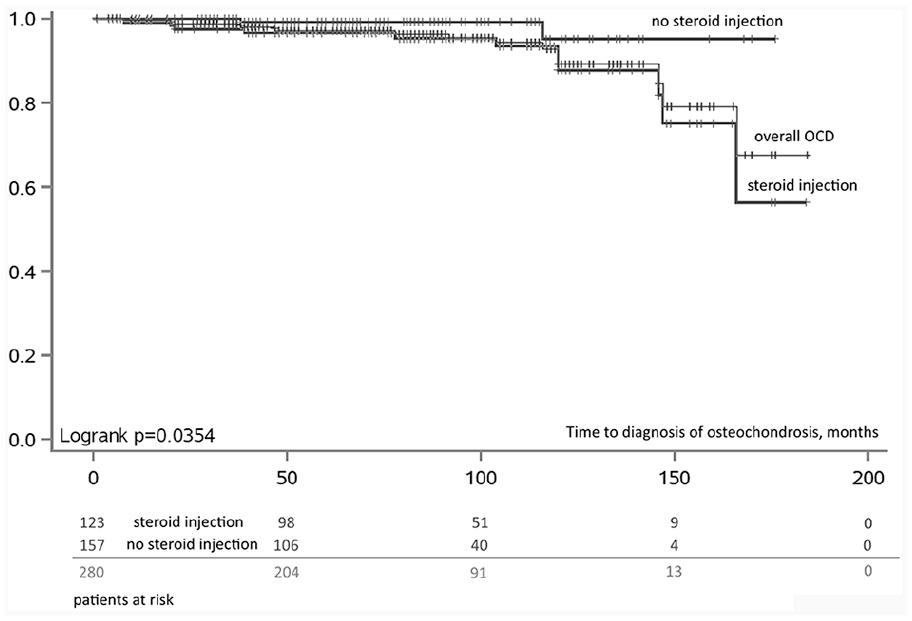
Kaplan-Meier chart, survival probability over time to diagnosis of osteochondrosis in moths (patient level). From diagnosis of juvenile idiopathic arthritis (JIA) to osteochondral (OC) diagnosis (or last follow-up). Groups: patients at risk with no steroid injection, patients at risk who received steroid injections, and all patients.
Discussion
Our analysis showed that intra-articular steroid injections significantly increased the risk of OC lesions. However, the overall pathomechanism of juvenile OC lesions remains elusive. Some early studies postulated that OC lesions are the result of local inflammation 9 but subsequent histologic studies did not support this hypothesis.10,11 It is presumed that a combination of both mechanical and biologic factors are at play.9,12 Juvenile OC lesions appear most commonly in the knee, but might also be present in other joints and are generally localized in specific locations. 13 Often they are found in children participating in community or club-level sports 13 and typically manifest after exceeding and repetitive strain. In the general population, boys are 3.8 times more often affected than girls, with a cumulative incidence of up to 0.03%. 14 Those lesions are most commonly found between the age of 11 and 15 years, and classic OC lesion are rare in younger kids.14,15
The early presence of OC lesions in pediatric patients with JIA has been described; but, in this specific patient group their incidence remains unclear.4,11 The influence of biologic factors such as local or systemic inflammation pathways is controversial.9,12 However, when looking at the natural history, untreated JIA will inevitably lead to cartilage joint destruction. Damage to the subchondral bone due to ongoing intra-articular inflammation was also shown in animal models. 16 Furthermore, MRI analyses suggest that already in early stage JIA, a reduction of the joint cartilage thickness can be observed. 17 The level of disease activity might therefore be a relevant intrinsic risk factor for OC development. As the 27-joint Juvenile Arthritis Disease Activity Score (JADAS-27) was not sufficiently documented in our cohort, we were not able to evaluate disease activity directly in our analysis. We postulated that duration and onset of the disease could serve as an indirect marker, both did not show a significant correlation with the appearance of OC lesions. All JIA-treatment modalities aim to reduce the inflammation, therefore it is questionable whether the inflammation itself, when adequately suppressed, is responsible to trigger OC lesions.
Furthermore, in our cohort, as well as in other studies, the OC lesion present differently from “classic” lesions, which may also point to a different pathomechanism. Additionally, JIA is more common in girls who are otherwise less affected by classic OC lesions.1,11 In the JIA population, the location of the lesion within the knee is rather atypical, that is, at the lateral femoral condyle, further they appear to be more progressive.4,11 Other studies also reported on an earlier appearance, in our analysis, the lesions were identified on average just over 5 years after initial JIA diagnosis at a mean age of 10.7 years. Others reported even a shorter disease interval of about 3.5 years until OC appearance. 4 In our cohort, we were not able to identify an additional history of trauma as a possible risk factor, as one other study reported minor trauma in about 50% in their JIA patients with OC lesions. 11
Corticosteroid treatment may have both, a beneficial effect by suppressing local or systemic inflammatory pathways, and detrimental effect in the longer term by reducing the regenerative capacity within mechanically loaded tissues. Intra-articular corticosteroid injections (IACI) remain a frequently used adjunct therapy in adult patients with knee osteoarthritis, 18 despite efficacy decreasing over time and with number of repetitions. 5 Dose-effect models support the idea of a “tipping point” during corticosteroid treatment in JIA. In pediatric JIA patients, a recent randomized controlled trial was able to show that local inflammatory symptoms can be decreased for 6 months on average with steroid injections alone. 19 However, a systematic review found only weak evidence that IACIs improve long-term patient outcome in this patient group. 2
Safety and adverse events of intra-articular steroid injections remain controversial. The most common reported side effects are skin hypopigmentation, subcutaneous atrophy at the injection site and postinjection pain. 2 In our cohort, none of those complications was reported. But the retrospective analysis did not allow to specifically screen for predefined adverse events and existing documentation was insufficient, which is a main limitation of our retrospective study.
The increased risk of osteonecrosis under systemic corticosteroid therapy is well documented and even proposed cutoff values for dosages with an increased complication rate exist. 8 In pediatric patients with JIA, generally lower dosages of systemic glucocorticoid are used, and on average limited to 5 mg per day. For intra-articular application, on the other hand, drug safety and dosage recommendations remain unclear, despite being widely practiced and generally considered safe. It was shown that locally applied steroids do also show systemic effects. 20 While a systematic review by the Cochrane Collaboration found only limited evidence to support the use of intra-articular steroid application, 6 another systematic review concluded that higher glucocorticoid doses are, in fact, associated with cartilage damage and chondrotoxicity.21,22 Other studies corroborate the possible association of locally applied steroids and OC incidence, as some of their patients received a high amount of repetitive injections (i.e., up to 12 in the same joint).4,11 An early study, on the other hand, prospectively evaluated the effects of steroid injections on human cartilage using MRI and ultrasound, and found no visible cartilage damage. 23 Adverse effects of IACIs on cartilage were also evaluated in a number of animal studies with repetitive increasing dosages of hydrocortisone causing damage to cartilage chondrocytes and cell loss.24-29 Additionally, iatrogenic damage to the cartilage, which might trigger osteonecrosis in a specific area is very unlikely when using a standard suprapatellar approach.
We evaluated the development of the lesions in the available follow-up MRIs, but data were very limited and the treatment heterogeneous, which did not allow a sufficient conclusion. Healing with residual deformity was achieved in most cases; however, 2 patients required repeated arthroscopic interventions due to ongoing symptoms. Generally, after OC identification the practice of IACIs was stopped and no further lesion, at least in the available follow-up period, occurred. This challenges a hypothesis of a preexisting vulnerability, as well as an ongoing inflammation as a cause of OC.
Our analysis did demonstrate that intraarticular steroid injections can be considered a risk factors to develop osteochondral lesions. However, identification of early OC lesion is often only possible on MRI, and imaging is performed mainly once a patient becomes symptomatic. Our subanalysis including only patients with MRIs and did not confirm the initial finding; however, the subpopulation is at risk for selection bias. Furthermore, it remains questionable whether all early lesions were identified. Especially since early MRI findings only include slight bone bruise and edema, 12 and other staging scores even only report initial thickening of articular cartilage and low signal changes as primary changes. 30 A prospective screening of all JIA patients with the focus on any chondral or subchondral change would allow a more valid approach. Furthermore, it has to be considered that JIA as a systemic inflammatory disease may affect multiple joints. 31 To focus only on the main affected joint, due to the limited available data, is another clear limitation of our study.
Conclusion
Patients with JIA who received repetitive intra-articular steroids injections showed a relatively high incidence of OC lesions and the repetitive administration of intra-articular corticosteroids need to be considered an associated risk factor. However, the exact pathomechanism of those lesions remains unclear. The lesions present early (around the age of 10 years), in rather atypical localization and tend to be progressive. Therefore, early MRI screening as well as prompt surgical treatment can be recommended.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This retrospective study was approved by the local ethics committee (KEK-ZH 2015-0273).