
Abstract
Objective
The purpose of this study was to determine if differences in Wiberg classification play a role in the ability of donor patellar osteochondral allografts to match the native patellar surface when treating osteochondral defects of the patellar apex.
Design
Twenty (10 Wiberg I and 10 Wiberg II/III) human patellae were designated as the recipient. Each recipient was size-matched to both a Wiberg I and a Wiberg II/III patellar donor. A 16-mm circular osteochondral “defect” was created on the central ridge of the recipient patella. The randomly ordered donor Wiberg I or Wiberg II/III plug was harvested from a homologous location and transplanted into the recipient. The recipient was then nano-CT (computed tomography) scanned, digitally reconstructed, registered to the initial nano-CT scan of the recipient patella, and processed to determine root mean squared circumferential step-off heights as well as surface height deviation. The process was then repeated for the other allograft plug.
Results
There was no significant difference in mean step-off height between matched and unmatched Wiberg plugs; however, there was a statistically significant difference in surface height deviation over the whole surface (0.50 mm and 0.64 mm respectively, P = 0.03). This difference of 0.14 mm is not felt to be clinically significant. Tibial width was correlated to patellar width (r = 0.82) and patellar height (r = 0.68).
Conclusions
For osteochondral allograft sizes up to 16 mm there appears to be no advantage to match donor and recipient patellar morphology. Further study is warranted to evaluate defects requiring larger graft sizes.
Introduction
Osteochondral injuries to the patella most commonly occur secondary to trauma following patellar instability; however, they can also occur due to an osteochondritis dissecans lesion. 1 Chondral injury following patellofemoral instability events have been reported to be as high as 95%.2,3 Most of these injuries are low grade, but a portion include displaced and nondisplaced osteochondral lesions. A recent study demonstrated that 38% patients who experienced patellar instability were found to have an osteochondral fracture, with the patella being more commonly affected than the lateral femoral condyle. 4
The treatment of osteochondral lesions of the patella follows a similar algorithm to other areas of the knee. In the event of failure of nonoperative treatment, multiple surgical procedures have been described with varying degrees of success. If the lesions are salvageable, consideration can be given to drilling of the lesion,5-7 bone grafting,8-10 debridement, and internal fixation.11-14 Reconstructive techniques are used when the lesions are unsalvageable including autologous chondrocyte implantation,15-18 osteochondral autograft transfer,18-21 and osteochondral allograft transplantation.18,22-24
Currently, indications for osteochondral allograft transplant of the patella are similar to those for the tibiofemoral joint. These are typically reserved for lesions violating the subchondral bone that are greater than 1 cm2 that have failed nonoperative treatment. 25 Outcomes data with regard to osteochondral allograft transplantation to the patellofemoral joint is limited. The longest study demonstrated a graft survival of approximately 55% at 15 years (78% at 10 years) with over 89% of patients satisfied with their results at 10 years. 22 Other studies are smaller case series with shorter follow-up.19,23
Currently, the matching process to obtain an osteochondral allograft for the patella is similar to matching other locations within the knee—the grafts are matched based on tibial width (±2 mm) and the femoral condyle width. Previous arthroplasty literature indicates that patellar size is weakly related to tibial size; however, the literature is sparse. 26 Unlike the femoral condyles and tibial plateau, patellar surface morphology is highly variable and was originally described by Wiberg. 27 The variability is associated with the location of the patellar apex in the medial-lateral direction. As originally described, the central ridge of a Wiberg Type I patella is centered such that the medial and lateral facets are equal in size. In a Type II patella, the central ridge is situated slightly toward the medial border and the medial facet is smaller than the lateral. In a Type III patella, the central ridge is substantially medialized with a steeply sloped and small medial facet ( Fig. 1 ). The morphology of the medial trochlea usually mirrors the patella in that the size of the medial trochlea tends to decrease as the Wiberg type moves from I to III. 27 While matching the contour of the relatively flat surface of the lateral patellar facet may be straightforward, it is uncertain how the cartilage surface variability affects matching and subsequent outcomes for osteochondral allograft transplantation involving defects of the central ridge. Previous cadaveric and finite element analyses using femoral condyle models have indicated that cartilage step off heights between donor and recipient as little as 0.5 mm can affect force distribution.28-32 Clinically, similar results have been seen in grafts with more than 1 mm step off at the cartilage surface; however, this was in a small case series involving mosaicplasty of the femoral condyles. 33
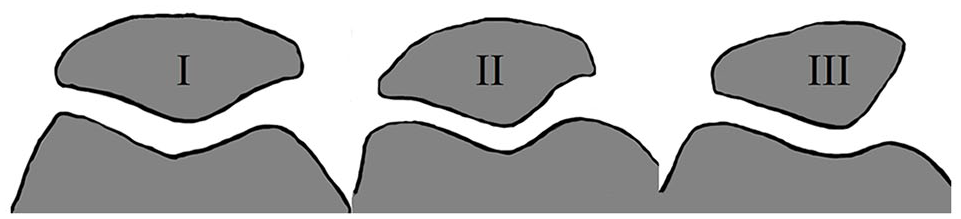
Depiction of patellar morphology based on Wiberg classification.
The purpose of this study was to use circumferential step-off height and cartilage surface mapping to determine if differences in patellar surface morphology (i.e., Wiberg classification) play a role in the ability of donor patellar osteochondral allografts to match the native patellar surface when treating osteochondral defects involving the central ridge of the patella. The secondary purpose was to evaluate the relationship between tibial width and patellar size.
Methods
Sixty fresh-frozen human patellae were provided by JRF Ortho (Centennial, CO; fresh osteochondral allograft distributer). Mean donor age was 20.1 ± 5.1years (range 12-29 years), and 38/60 (63%) of the grafts were male. The height (superior to inferior distance) and width of the patellar articular surface were measured with a calibrated caliper and the patellae were then classified into the appropriate Wiberg class (I, II, or III) 27 using visual inspection as well as measurement of the distance of the patellar apex from the lateral border of the patella (relative to patellar width). Wiberg I was defined as similar size medial and lateral patellar facets. Wiberg II had a slightly smaller medial facet. Wiberg III had a markedly smaller and more vertically oriented medial facet. Patellae were then grouped into Wiberg I and Wiberg II/III. 27 The reliability coefficients for measuring the width of the medial and lateral facets are 0.94 and 0.97, respectively. 34 Wiberg I patellas had lateral-to-medial facet width ratios of ≤55%.
Ten Wiberg I and 10 Wiberg II/III patellae were chosen as recipients. Each patella was then size matched (±2 mm of tibial width) to a Wiberg I and Wiberg II/III patella to produce 20 size-matched trios that included a Wiberg I or II/III recipient, Wiberg I donor, and Wiberg II/III donor. Each patella was refrigerated in proprietary medium when not in use.
Computed Tomography (CT) Scanning and Allograft Transplantation
All patellae underwent an initial nano-CT scan to determine the native chondral surface morphology. Individual patellae were scanned using a Phoenix Nantom S with Phoenix Datos|x 2 Acquisition, version 2.3.2 (phoenix X-ray, GE Inspection Technologies; Wunstorf, Germany). Scan settings of 90 kV, 250 µA, mode 0, 3 frames averaged, 1 skip, 1000 ms exposure time, 1000 images per scan, a diamond coated tungsten target, and a 0.5 mm aluminum filter were used. Scans were reconstructed at 40 µm resolution using Phoenix Datos|x 2 reconstruction v 2.2.1-RTM (phoenix X-ray, GE Inspection Technologies). 35
After the initial scan was performed, a 16-mm defect centered on the central ridge (apex) of the recipient patella was created to a depth of approximately 10 mm. A 20-mm diameter defect was originally planned; however, some of the recipient patellae were smaller than expected. Using a 20-mm defect risked cortical breach and/or uncontained defects in the superior-inferior borders in these smaller recipients. For consistency across the study, a 16-mm defect was therefore used for all recipients. Depth measurements of the defect were recorded at the 12, 3, 6, and 9 o’clock positions and double-checked.
Using a random number generator, either the matched Wiberg patella or unmatched Wiberg patella was chosen to be transplanted first. This process was performed to prevent any confounding error in the measurements due to cartilage deformation during the first transplant or while removing the first transplant. A 16-mm osteochondral plug was taken from the matching location on the patellar apex of the donor patella with appropriately sized coring trephine and oscillating saw. Care was taken to align the recipient and donor guides as perpendicular as possible to the cartilage surface. Given the hardness of the patellar bone, the recipient defect and osteochondral plug were prepared and harvested using the JRF Ortho osteochondral allograft instrumentation. This instrumentation produces donor plugs that are the same diameter as the recipient socket instead of under-sizing the socket by 0.5 mm. The plug orientation was marked at the 12 and 3 o’ clock positions. Using an oscillating saw, as well as Rongeur, the donor bone plug was trimmed to match the depth of the recipient defect at all 4 locations. The edges of the donor plug were then bulleted to allow ease of placement. The donor plug was then manually placed into the recipient defect and advanced until flush. The recipient patella with the first donor plug was then nano-CT scanned. The donor plug was then carefully removed, and the process was repeated for the other plug. To avoid damage to the recipient cartilage surrounding the defect, the plug was removed by drilling a 2.4-mm guide wire retrograde through the superficial (nonarticular) side of the patella and into the plug without breaching the surface. This wire was then tapped to push the plug out without damage to the surrounding recipient surface.
Step-Off Height Measurements
Reconstructed nano-CT scans of the recipient patellae were blinded, randomized, and uploaded into DragonFly 4.0 (Object Research Systems, Montreal, Quebec, Canada). The patella was then oriented such that an axis was directed completely perpendicular to the orientation of the plug, allowing appropriate cuts in order to assess step off height at 3° intervals around the entirety of the plug. The difference in the height of the plug cartilage and the native cartilage were recorded ( Fig. 2 ). In order to ensure measurement between patellae at the same location, measurements were taken and recorded as 0° for superior pole, and 180° directed at the inferior pole. These measurements were then classified into unacceptably proud (≥1 mm or ≥0.5 mm), acceptably proud (<1 mm or <0.5 mm), unacceptably sunken (more than 1 mm or 0.5 mm sunken), or acceptably sunken (less than 1 mm or 0.5 mm sunken). The root mean squared (RMS) step-off height for the circumference, percent of the circumference unacceptably proud, and percent of the circumference unacceptably sunken were calculated for the whole patella and each quadrant ( Fig. 3 ). 35
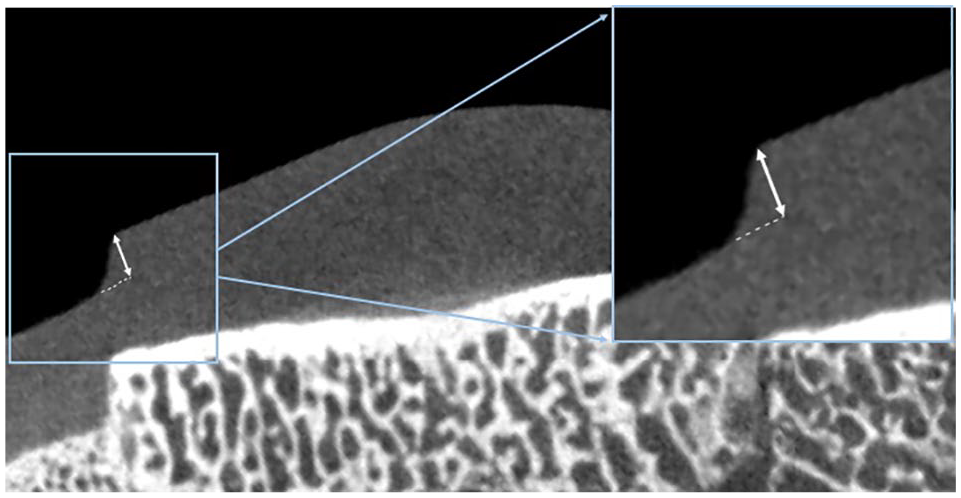
Three-dimensional reconstruction of a nano-CT scan with depiction of the step-off height measurement.
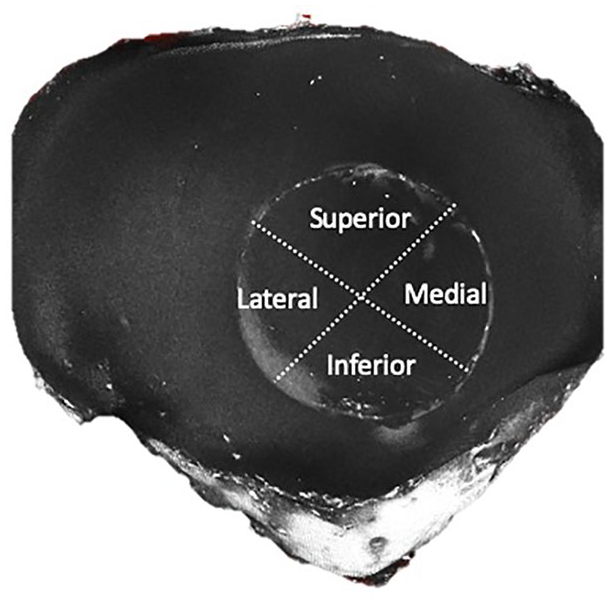
Depiction of the patellar quadrants created for subgroup analysis.
Surface Mapping
Reconstructed nano-CT scans of the native patella and donor-transplanted recipient patella were registered and orientated to each other via DragonFly. The registered objects were cropped to an area surrounding the osteochondral plug and then exported for further processing into MATLAB (Mathworks, Natick, MA).
In MATLAB, differences in density allowed for identification and differentiation of air, cartilage, and bone. Using vertical slices through the osteochondral plug, a 3-dimensional matrix of the cartilaginous surface was created. The initial data set registration and orientation performed in MATLAB allowed both the native patella and donor-transplanted recipient patella to be overlayed on the same set of axes. Using these plots (and the MATLAB poly23 function), perpendicular distances from over 3000 points across the surface of the osteochondral plug were used to measure the difference in surface height between the native patella and the transplanted osteochondral plug 35 ( Figs. 4 and 5 ).
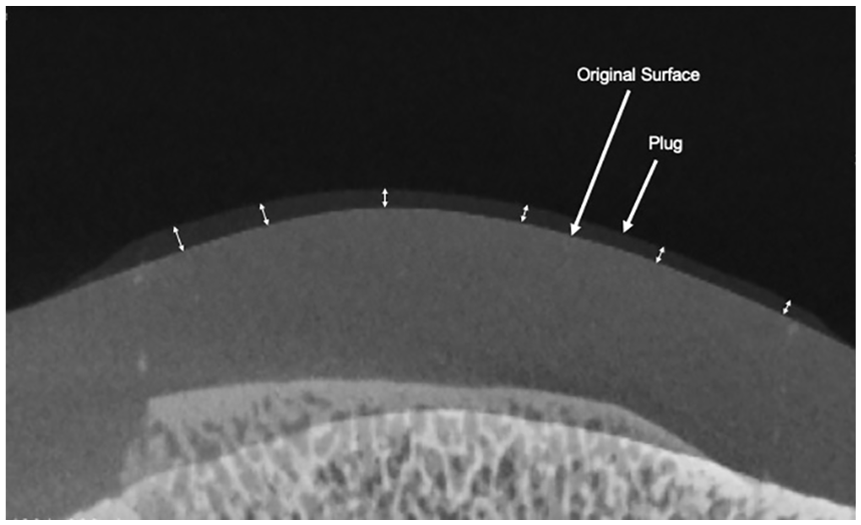
Three-dimensional reconstruction of a nano-CT scan demonstrating the overlay of the native and donor surfaces with depiction of the surface height deviation measurement.
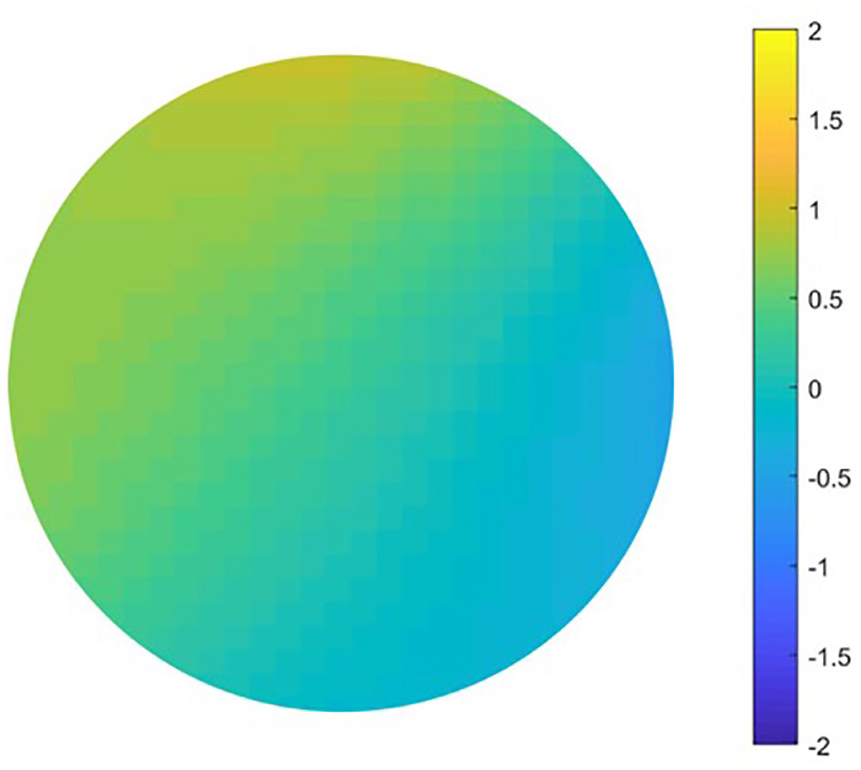
Example of a surface map depicting the surface deviation over the entire plug. The color legend is measured in mm proud (+) or sunken (−).
The RMS of the difference in height between native patella and the transplanted plug was then calculated for both the whole patella as well as for each quadrant. The proportion of the surface that was unacceptably proud and unacceptably sunken was calculated and compared between the 2 groups using both 1 mm and 0.5 mm as unacceptable cutoffs.
Statistics
An unpaired t test was used to compare step-off height and surface deviation between matched and unmatched Wiberg transplants (n = 20). Two-way ANOVA was used to determine the effect of transplant type (matched or unmatched Wiberg) and plug quadrant (medial, lateral, superior, inferior) on step-off height and surface deviation. Tukey’s multiple comparisons were used to compare step-off heights between each pair of quadrants. Prior studies have used both 0.5 mm31,32 and 1 mm 33 cutoffs for designated “unacceptably proud” or “unacceptably sunken” plugs. As a result, the proportion of the circumference and the proportion of the surface area found to be unacceptably proud or sunken was calculated using both 0.5 mm and 1 mm cutoffs.
Pearson correlation was used to determine if tibial width was an acceptable surrogate for patellar size. Descriptive statistics were used to describe the patellar width, height, and apex location.
Previous work with medial and lateral femoral condyle transplants demonstrated standard deviations of RMS surface height deviation to be between 0.21 and 0.38 mm.35,36 Given an increase in the expected variability of the surface shape for the 2 patellar morphologies, a more conservative standard deviation of 0.5 mm was used. A clinically relevant difference of 0.75 mm (slightly less than the acceptable 1 mm prominence) between groups was used with a power of 0.8 in a 2-tailed test (alpha < 0.05) to determine a sample size of 7 recipient patellae per group. To provide a safety factor, the study sample size was increased to 10 recipient patellae per group. The study was considered exempt by University of Michigan Institutional Review Board (HUM00148156).
Results
Sixty patellae were used for this study. Mean donor age was 20.1 ± 5.1years (range 12-30 years), and 38/60 (63%) of the grafts were male.
Step-Off Height
There was no significant difference in step-off height when comparing matched and unmatched Wiberg transplants ( Table 1 ). There was a significant difference between lateral and inferior (P = 0.001) and superior and inferior (P = 0.01) in the matched patellae group. There was no significant difference in the percent of unacceptably proud and sunken step-off heights between matched and unmatched Wiberg transplants when 1 mm and 0.5 mm was used as the unacceptable cutoff across all quadrants ( Figs. 6 and 7 ).
Root Mean Square Step-Off Height (mm) for Matched (n = 20) and Unmatched (n = 20) Wiberg Patellae in Each Quadrant of the Transplanted Plug a .

Significant difference between lateral and inferior quadrants *(P = 0.0013) and superior and inferior quadrants +(P = 0.01) in matched patellae.
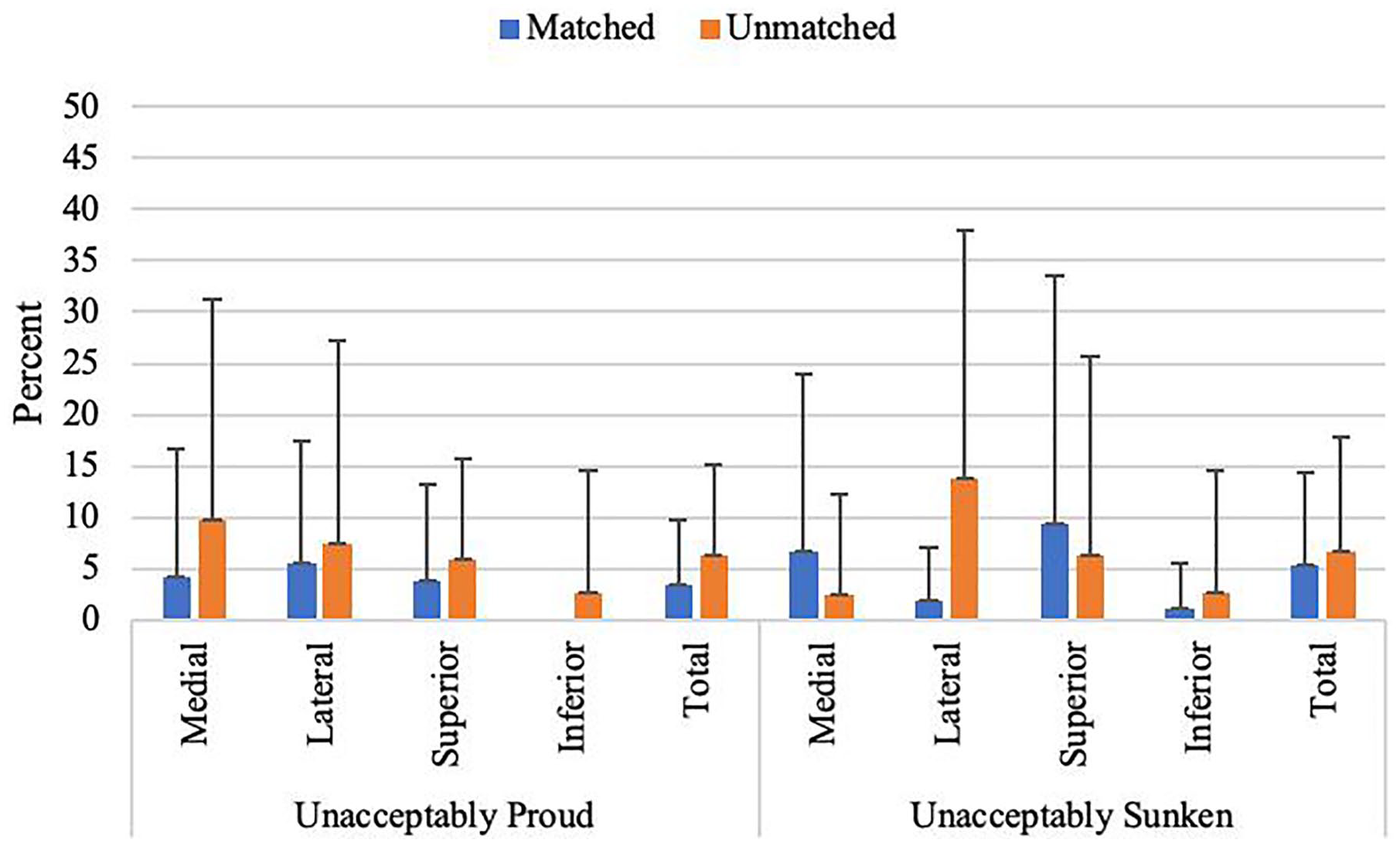
Mean percent (±SD) of step-off height unacceptably proud and unacceptably sunken (1-mm threshold).
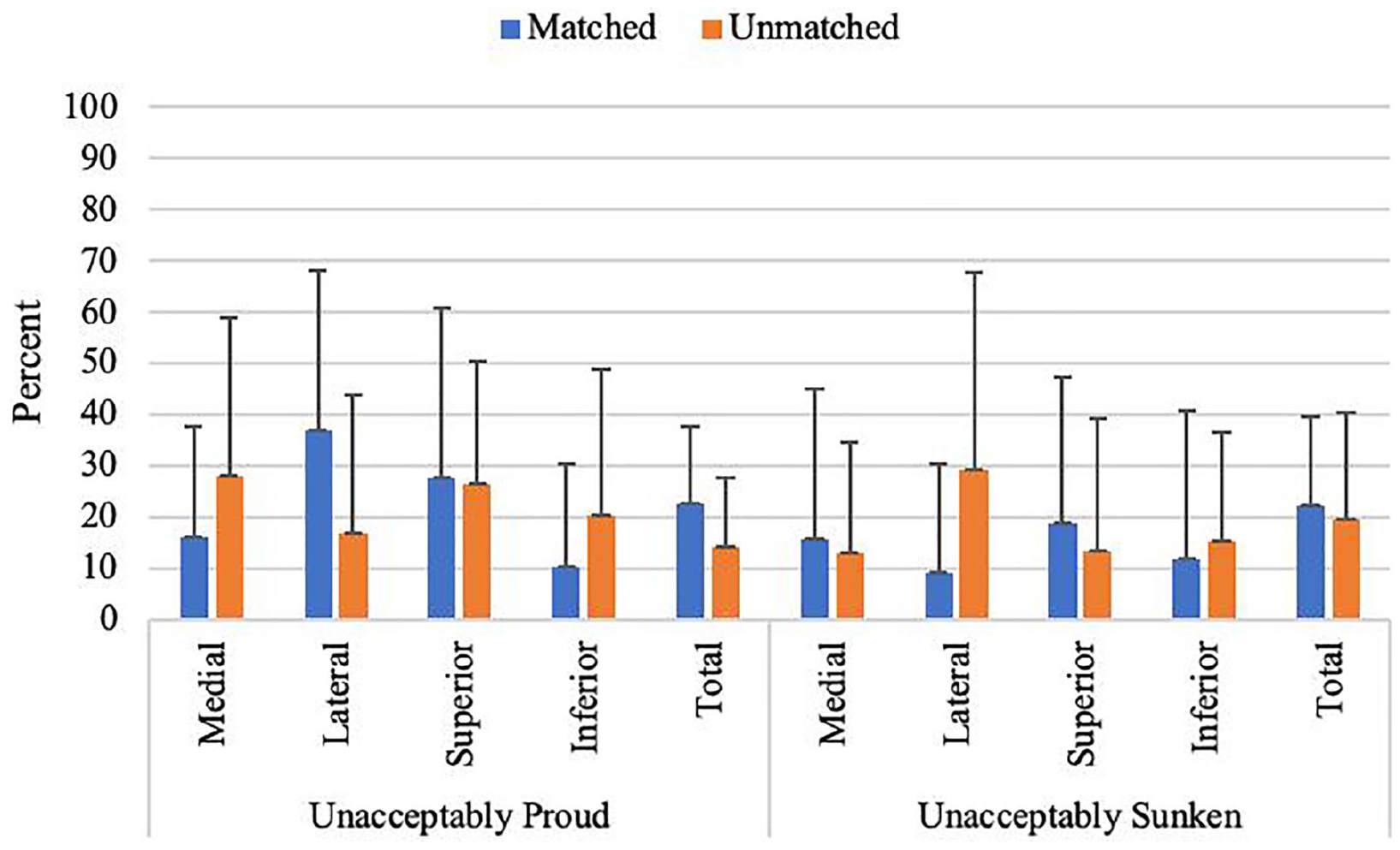
Mean percent (±SD) of step-off height unacceptably proud and unacceptably sunken (0.5-mm threshold).
Surface Deviation
There was a statistically significant difference in surface height deviation when comparing matched and unmatched Wiberg transplants (P = 0.03). There was no significant difference in surface deviation between quadrants ( Table 2 ).
Root Mean Square Surface Deviation (mm) for Matched (n = 20) and Unmatched (n = 20) Wiberg Patellae in Each Quadrant of the Transplanted Plug.

P = 0.03.
There was a significant difference in the percent of unacceptably proud surface deviation between matched and unmatched Wiberg transplants when 1 mm was used as the threshold; however, this difference was not found when 0.5 mm was used as the threshold (P = 0.02; Figs. 8 and 9 ).
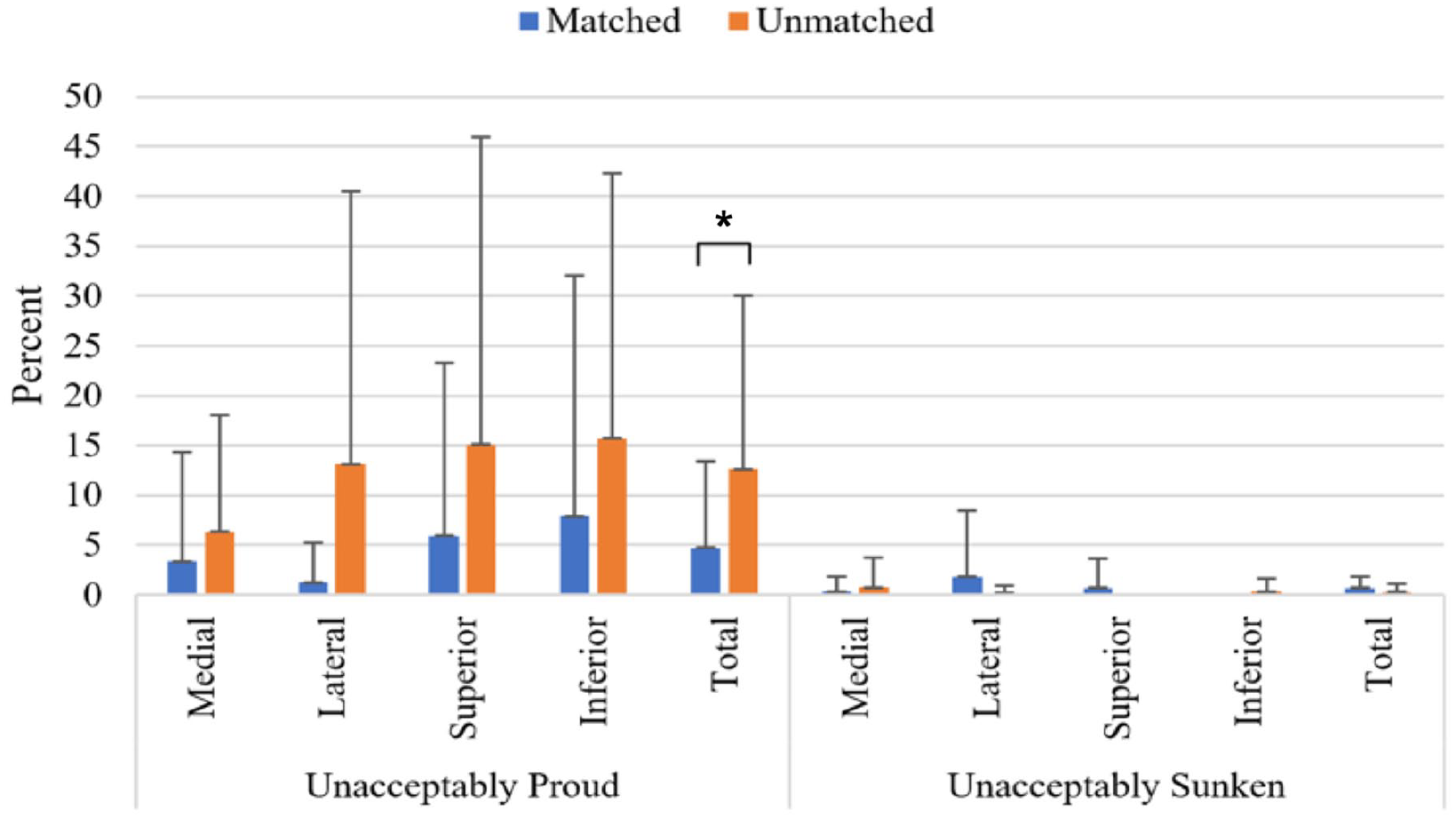
Mean percent (±SD) of surface deviation unacceptably proud and unacceptably sunken (1-mm threshold), *P = 0.02.
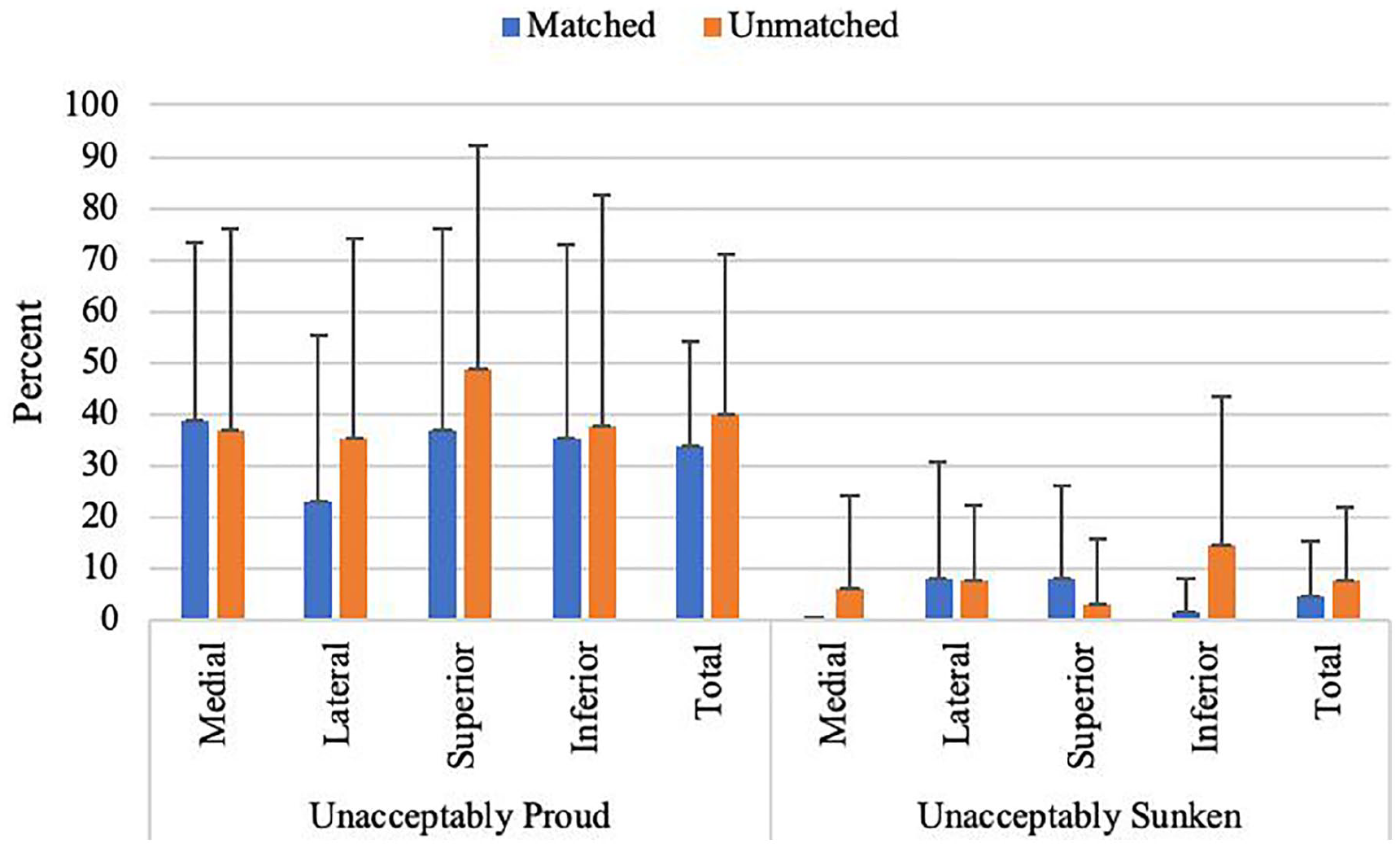
Mean percent (±SD) of surface deviation unacceptably proud and unacceptably sunken (0.5-mm threshold).
Patellar Size
Mean patellar width and height was 41.4 ± 3.8 and 30.6 ± 2.4 mm, respectively. On average, the patellar apex was located 23.5 ± 3.2 mm from the lateral border of the patella. In those patella classified as Wiberg I morphology, the apex was 53.0 ± 2.6% of the width from the lateral articular border (range: 45.9% to 56.8%). Wiberg II (n = 23) patellar apex was located a mean of 59.9 ± 3.4% (range: 55.3% to 72.1%), and the Wiberg III (n = 7) patellar apex was a mean of 61.6 ± 6.4% (range: 55.3% to 72.7%) of the width from the lateral border. There was a linear correlation of tibial width to patellar width (r = 0.82) and patellar height (r = 0.68). Using simple linear regression, neither patellar width, height, nor tibial width correlated or predicted step-off height or surface deviation.
Discussion
Osteochondral allografts for the patella are currently matched based on tibial and femoral condyle width as measured on an AP radiograph or MRI (magnetic resonance imaging). There is currently no consideration given to differences in patellar cartilage surface morphology. This is the first study to investigate the effects of surface morphology on the ability to adequately match osteochondral allograft transplants involving the patella.
Only one small case series of osteochondral autograft transplants to the femoral condyles has previously published the effects of cartilage step-off height on clinical outcomes. This series of 5 patients demonstrated that clinical results were not adversely affected as long as the cartilage step-off height between the graft and native cartilage was less than 1 mm. 33 Previously, cadaveric biomechanical and finite element analysis studies demonstrated increased forces secondary to step-off heights as little as 0.5 mm in the medial femoral condyle.28-32 To date, there have been no published biomechanical studies involving the patellofemoral joint. Our study demonstrated no significant differences in step-off heights between matched (Wiberg I → Wiberg I, Wiberg II/III → Wiberg II/III) and unmatched Wiberg transplants. There were small differences between the superior/lateral and inferior quadrants within the matched plugs (0.21-0.25 mm). These differences were felt to be more related to the lower variation/standard deviation in this group compared to the unmatched group. Overall, differences in patellar morphology, as evidenced by Wiberg classification, had minimal effect (<0.2 mm differences) on step-off heights following osteochondral allograft transplantation involving the central ridge of the patella. Future studies are needed to determine the magnitude of the step-off that may produce adverse effects on local force distribution and graft and/or opposing surface damage in the patellofemoral joint.
There is no current literature on the effects of surface height deviation between the transplanted cartilage surface and the native cartilage surface. Our study demonstrated a statistically significant difference in surface height deviation between matched and unmatched Wiberg transplants. However, this is likely not clinically significant as the magnitude of the difference between the mean height deviations of the matched (0.5 mm) and unmatched (0.63 mm) plugs was only 0.14 mm. This difference is due to the variations in cartilage contour when comparing patellae with different Wiberg classification. The ultimate effects of this difference are currently unknown. No difference was observed when investigating by quadrant between matched and unmatched Wiberg transplants.
In addition to measuring specific step-off height and mean surface deviations, analysis was also performed on the percentage of the graft that was unacceptably proud and sunken using thresholds of 0.5 mm and 1 mm.31-33 There were no significant differences in unacceptably proud or sunken step-off height measurements at either threshold. When analyzing surface deviation, unmatched Wiberg donors had a significantly higher proportion of the surface that was unacceptably proud (1 mm cutoff) compared to the matched donors (12.6% vs. 4.7%, P = 0.02). While the proportion of the surface that was proud was relatively low in both groups, the clinical significance is unknown. Due to the lack of other significant differences in the percent of the surface proud or sunken; however, the significance of this finding on the overall construct is likely minimal.
Tibial width has been shown to be a weak indicator of patellar size in the knee arthroplasty literature. 26 In the current study, tibial width had a moderate to strong correlation with both patellar width and height (r = 0.68, r = 0.82, respectively). The use of tibial width to match patellar donors allows continued standardization in the matching process for osteochondral allograft transplants for the entire knee. It also allows for the relatively easy matching of donors and recipients without requiring allograft procurement companies to specifically measure patellar height, width, and Wiberg classification for each donor. Such measurements would increase the processing time and would increase the subjectivity of classification (Wiberg classification). These additional requirements would likely decrease the match rate resulting both in delays in matches and patient care, as well as increasing the likelihood of donor tissue going unused. Both of these situations would go against the current goals in tissue donation of providing expeditious patient care and maximizing the effectiveness of using the gift of tissue provided by human tissue donors.
There was no correlation between tibial width, patellar height, or patellar width, and step-off height and surface deviation measurements. There was therefore no effect of patellar size on the accuracy of the transplant. While there is currently no related patellar literature, a previous study investigating the effects of varying defect size has been performed on femoral condyles. That study reported that as defect size increases, the mismatch of surface congruity increases in a topographic model. 37 This study also demonstrated that for femoral condyles, an acceptable articular cartilage surface match can be obtained, regardless of whether the donor condyle is matched in size.
The current study has some limitations. First, the study was performed ex vivo; therefore, no biomechanical conclusions can be made. Second, one surgeon performed all osteochondral allograft transplants; therefore, variations in surgeon experience and technique cannot be accounted for. Third, only 16-mm allograft plugs were used from the patellar apex. The ability to generalize these results to larger defects is therefore limited. While the apex is the most difficult location to match, only assumptions can be drawn from harvesting at other areas of the patella. Last, no clinical outcomes can be gleaned from this study.
Future work in a similar laboratory setting will include evaluation of step-off heights at the subchondral bone interface. Even when the cartilage surface was flush, there were cases where incongruity still occurred at the bony interface ( Fig. 10 ). It is possible that bone incongruency may produce disruptions in compression force distribution that could result in poor graft integration or earlier graft failure; however, this has not been previously investigated in the literature. Additionally, studying the effectiveness of oversized donors or visually, as opposed to anatomically, matched grafts may be beneficial. Further work outside of the laboratory setting should include finite element analysis, biomechanical lab analysis, and/or clinical data to determine the threshold for graft step-off height and surface contour differences (proud or sunken) that may contribute to an increased rate of clinical failure for these grafts.
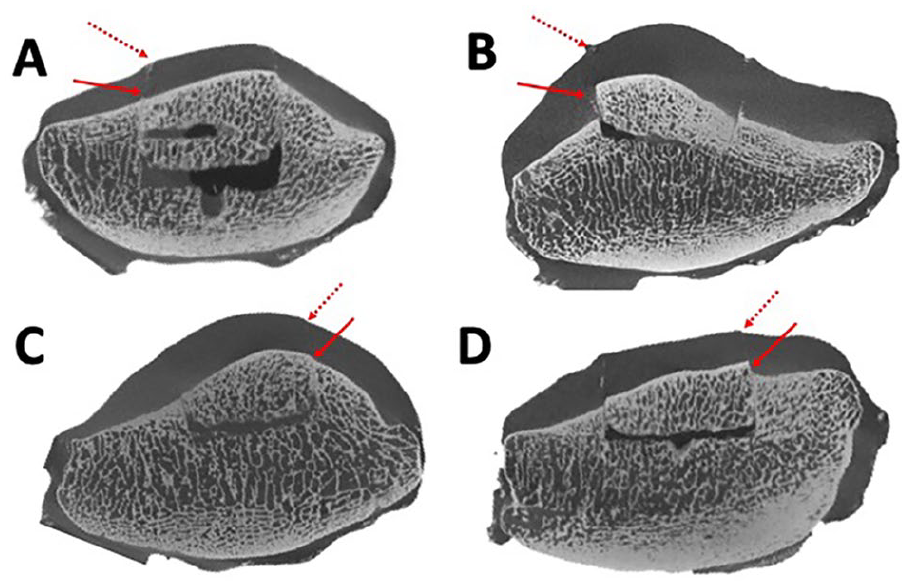
Although the cartilage surface of the donor plug may be flush with the native cartilage on gross examination (dotted arrow), concurrent alignment of the subchondral bone may (solid arrow in
In conclusion, the current study supports the current practice of matching patellar osteochondral allografts based on tibial width alone, regardless of patellar surface morphology, as Wiberg classification had no clinically significant effect on graft step-off height or surface deviation.
Footnotes
Authors’ Note
Work performed at the University of Michigan.
Acknowledgments and Funding
The authors would like to thank Jordyn Sessell for her extensive logistical support for this study. The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Study was funded by JRF Ortho. Research reported in this publication was supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases of the National Institutes of Health under award number P30 AR069620.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: John A. Grant: speaking honoraria from JRF Ortho, Conmed Linvatec, Vericel; research support from JRF Ortho, Arthrex, Aesculap Biologics. The other authors have no conflicts of interest to disclose.
Ethical Approval
This research study was reviewed and approved by University of Michigan Institutional Review Board (HUM00148156).
Informed Consent
Informed consent was not sought for the present study because this was a basic science study utilizing donated tissue.