
Abstract
Objective
To collate current literature pertaining to the published reports of indications for, and outcomes of, osteochondral allograft (OCA) transplantations in the shoulder so as to guide surgeons in the management of various etiologies of osteochondral lesions in this joint.
Design
A systematic review of the current literature was performed in February 2022 in the PubMed, Cochrane, and EMBASE databases using specific search terms and predetermined inclusion/exclusion criteria.
Results
One-hundred-twenty-three articles were initially identified, 30 full-text articles were assessed for eligibility, and 17 articles met inclusion criteria. Data were collected for study characteristics, etiology, lesion size/location, intervention/type of graft used, follow-up, and outcomes. In total, 83 shoulders were included (n = 83) in the review with an average follow-up of 45.7 months. Nine specific indications for OCA transplantation in the shoulder included: reverse Hill-Sachs lesions (33), Hill-Sachs lesions (22), pain pump chondrolysis (10), recurrent shoulder instability (7), osteoarthritis/degenerative changes (5), radiofrequency chondrolysis (2), prominent suture anchors (2), glenoid lesion (1), and osteochondritis dissecans (1). Seventeen patients had concomitant surgeries and two patients were lost to follow-up. Of the total 83 shoulders, 68 had favorable outcomes and 13 had unfavorable outcomes as determined by graft incorporation, pain scores, functionality/ROM, patient-reported satisfaction, and/or requirement for revision/arthroplasty. Of the 13 with unfavorable outcomes, a disproportionate number had concomitant surgeries and/or were performed for pain pump chondrolysis (6).
Conclusions
The use of OCAs appears to be a viable option for a variety of difficult-to-treat shoulder pathologies, particularly those characterized by isolated osteochondral injuries.
Introduction
Osteochondral allograft (OCA) transplantation replaces damaged chondral or osteochondral articular surface with mature hyaline cartilage and associated subchondral bone from screened donors. It represents an increasingly available biologic tissue approach to restore articular anatomy after traumatic and pathologic articular joint disease processes. The origins of this approach stem from resection reconstruction for oncologic etiologies. 1 The use of OCA has been well-documented for articular lesions secondary to trauma and articular disease processes in the femoral condyles, tibial plateau, patella, and ankle. However, their use in the shoulder has been more limited.
Indications and associated outcomes for OCA related to nononcologic processes are less well-characterized in the shoulder and proximal humerus. As such, the purpose of this study was to systematically review the indications and clinical outcomes of OCA transplantation in the shoulder to help guide surgeons and provide care practice options for the treatment of various etiologies of osteochondral lesions in the shoulder joint.
Methods
A comprehensive literature search was conducted in February 2022 to identify the pertinent data and clinical support in accordance with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) guidelines. A general search was conducted to identify clinical outcomes data for OCA transplantation of the shoulder joint using the following electronic databases: PubMed, EMBASE, and Cochrane (
PubMed:
((“osteochondral”[All Fields] or “osteoarticular”[All Fields]) AND (“allografts”[MeSH Terms] OR “allografts”[All Fields] OR “allograft”[All Fields]) AND (“humeral”[All Terms] OR “glenoid”[All Terms] OR “shoulder”[All Terms”] “glenohumeral”[All Terms] AND “Joint”[All Terms])).
EMBASE:
((osteochond* OR osteoartic* OR “osteo artic*”) AND allogra* AND (humer* OR glenoid* OR shoulder*) NEAR/7 joint*) OR ((osteochond* OR osteoartic* OR “osteo artic*”) AND allogra* AND “joint of shoulder region”/exp).
Cochrane:
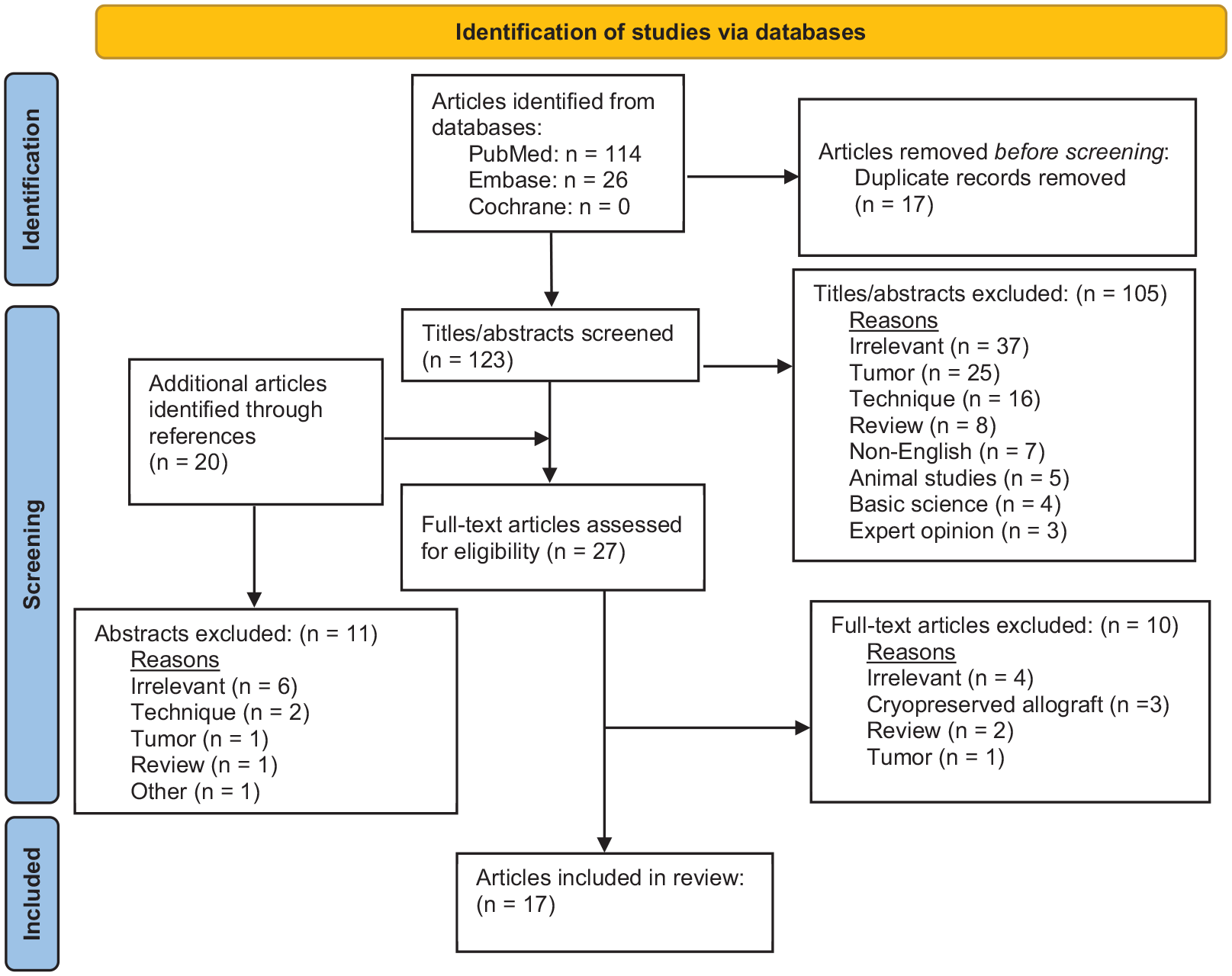
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) flowchart of the systematic literature review.
((“allografts”[MeSH Terms] AND (“osteoarticular”[All Text] OR “osteochondral”[All Text]) AND (“allograft”[All Text] OR “allografts”[All Text]) AND (“humeral”[All Text] OR “glenoid”[All Text] OR “shoulder”[All Text] OR “glenohumeral joint”[All Text])).
The results were filtered to English and full-text articles. References were reviewed to identify additional articles and confirm completeness. Inclusion criteria included original research studies that investigated the use of OCA transplantation in humans to treat chondral or osteochondral defects. Furthermore, the inclusion criteria for clinical studies required at least one patient, reported patient outcomes, and minimum follow-up of 12 months. Systematic reviews of clinical studies investigating outcomes of OCAs were included as relevant to this study. Exclusion criteria was as follows: articles not written in English, review or expert opinion articles, instructional courses, surgical technique articles, conference proceedings and presentations, OCAs for tumor, basic science or animal studies, articles that used OCAs that were cryopreserved or decellularized. One author performed the literature search (B.P.), and two authors independently reviewed the search results (B.P. and S.T.). Titles and abstracts were reviewed for all search results. Full-text articles were obtained to determine if the study met the established inclusion and exclusion criteria. Data were collected for study characteristics, etiology, lesion size/location, intervention/type of graft used, follow-up, and outcomes. A contingency table chi-squared test was also performed to evaluate possible confounding effects of concomitant surgery on OCA transplantation outcome.
Results
One-hundred twenty-three articles were initially identified after accounting for duplicates, 27 full-text articles were assessed for eligibility after accounting for additional articles found in references, and 17 articles met inclusion criteria. The publication dates of the included studies ranged from 1997 to 2021.
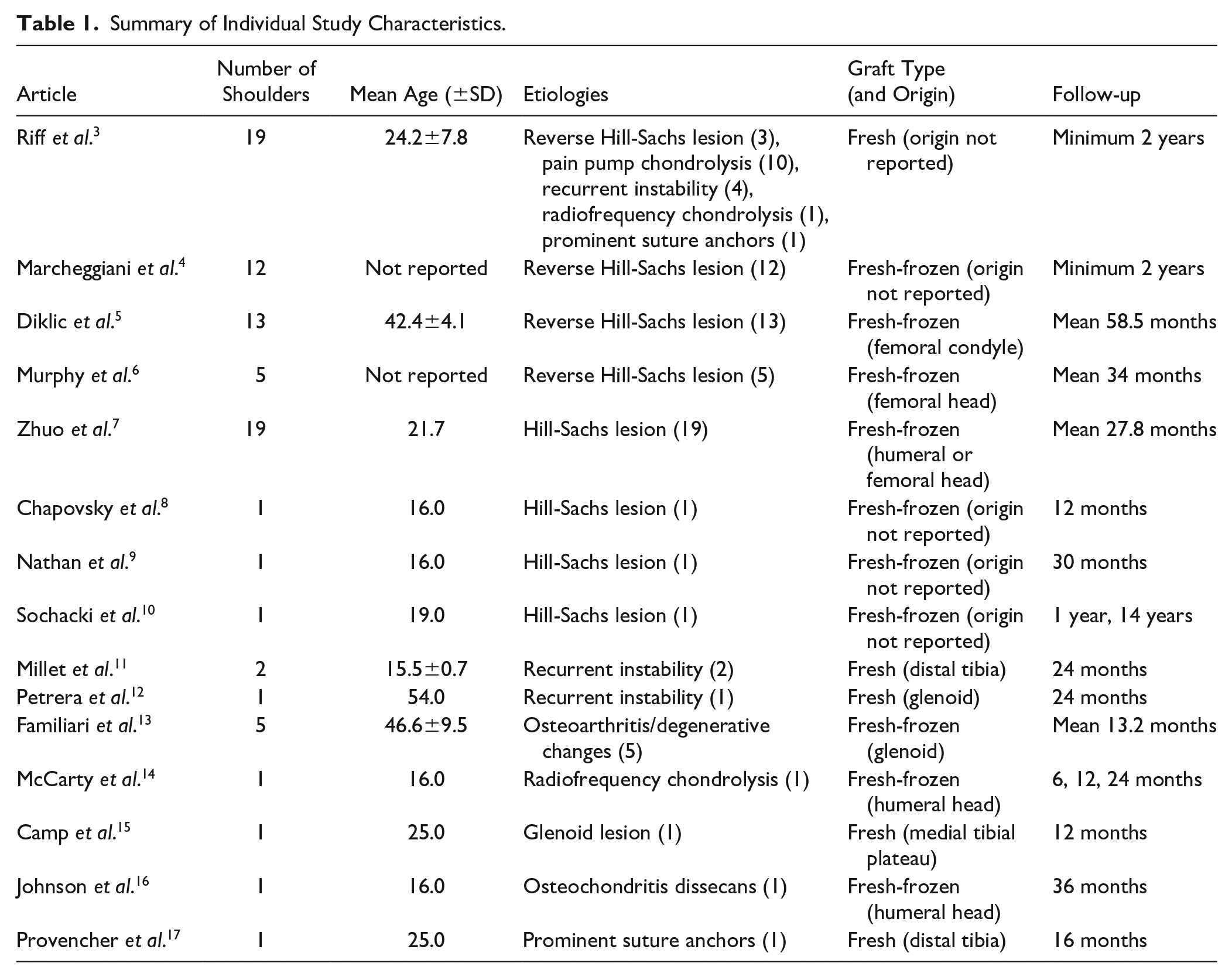
The levels of evidence included in the study were eight case reports, seven case series, and two systematic reviews. Among the included studies, a total of 83 shoulders were treated with an average follow-up time of 45.7 months (range 12-168 months). The various indications for OCA transplantation in the shoulder included reverse Hill-Sachs lesions (33), Hill-Sachs lesions (22), pain pump chondrolysis (10), osteoarthritis/degenerative changes (5), recurrent shoulder instability (7), radiofrequency chondrolysis (2), prominent suture anchors (2), glenoid lesion (1), and osteochondritis dissecans (1). Nineteen patients had concomitant surgeries (e.g., lateral meniscus allografts, partial joint replacement, Bankart lesion repair, or microfracture) and two patients were lost to follow-up. Table 1 summarizes the study characteristics of each article, and Table 2 demarcates the relative outcomes (i.e., success or failure) based on clinical and radiographic findings at final follow-up (cohort average of 45.7 months, range 12-168 months).
Summary of Individual Study Characteristics.
Summary of Successes, Failures, Lost to Follow-ups, and Success Rates.
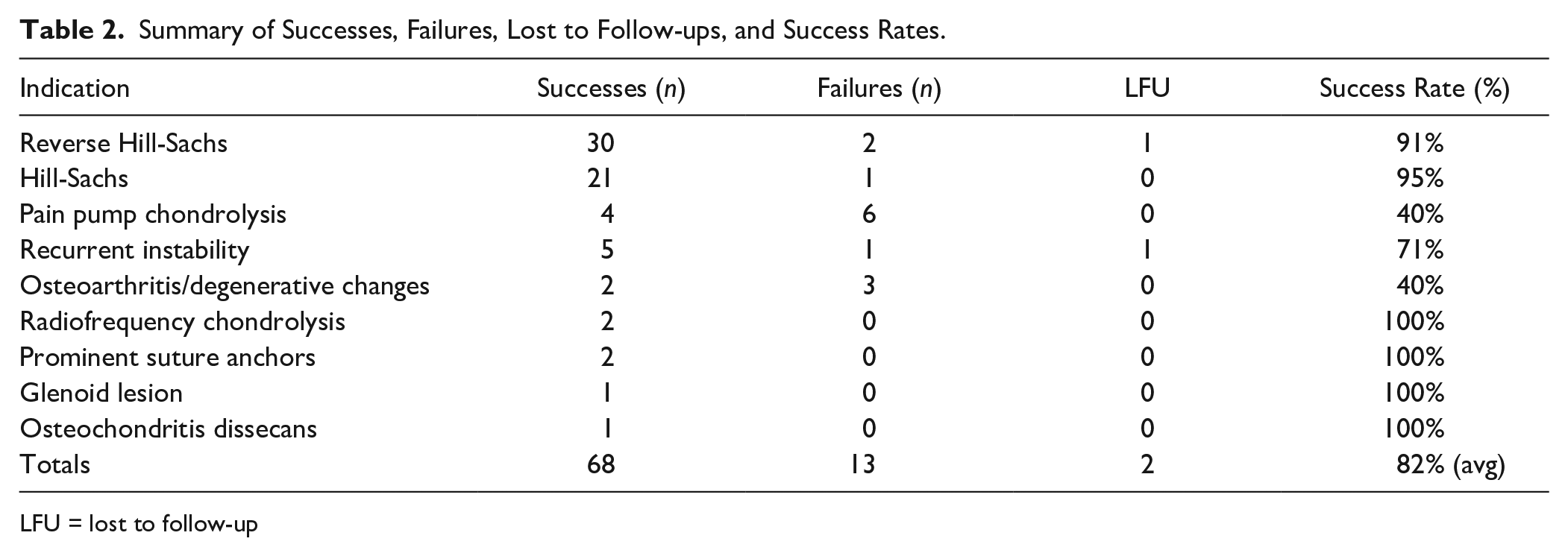
LFU = lost to follow-up
Concomitant surgeries were identified as possible confounders to the success or failure of the OCA transplantation. A contingency table chi-squared test was performed for all shoulders excluding those that were lost to follow-up or performed for pain pump chondrolysis (n = 71). Results showed that concomitant surgeries may have influenced the results, χ2(1, n = 71) = 7.06, P = 0.0079.
The systematic review by Sayegh et al. 18 evaluated clinical and radiological outcomes for OCA after glenoid bone loss in glenohumeral instability. 18 The systematic review by Saltzman et al. 19 evaluated outcomes of OCA for large osteochondral defects of the humeral head. 19 All shoulders included in these reviews were referenced in our current systematic review via citation of the original sources. After accounting for duplicates and after applying our inclusion/exclusion criteria, no new shoulders were identified in the findings by Sayegh et al. and Saltzman et al.
Reverse Hill-Sachs Lesion
A total of 33 patients across four different articles were identified who underwent fresh (n = 3) or fresh-frozen (n = 30) OCA transplantation for reverse Hill-Sachs lesions in the shoulder. 3 6
Diklic et al. 5 describe a retrospective cohort study in which 13 patients (10 men and three women, average age 42.4 years) underwent fresh-frozen OCA transplantation for chronic posterior shoulder dislocation with associated impression (impaction) fracture of the anteromedial aspect of the humeral head (i.e., reverse Hill-Sachs lesion). Follow-up data were collected at an average of 54 months and included ROM measurements, Constant-Murley scores, and radiographic results. Amongst the cohort, the mean postoperative Constant-Murley score was 86.8 (range, 43 to 98). Of the 13 patients, 12 had successful outcomes after allograft transplantation as determined by adequate ROM, satisfactory Constant-Murley scores, and evidence of successful graft incorporation on radiographs. The remaining patient developed spontaneous osteonecrosis of the humeral head and had an unsatisfactory result. However, it should be noted that this remaining patient had a history of a chronic locked posterior dislocation (greater than 9 months) and an osteochondral defect involving 50% of the articular surface. 5
Marcheggiani et al.
4
describe another case series in which 12 patients were treated with fresh-frozen humeral head OCAs for reverse Hill-Sachs impaction fractures in the setting of locked posterior glenohumeral dislocations. The size of the lesions in this cohort ranged from 30% to 50% of the humeral head. The sexes and ages of the patients were not reported. Clinical and radiographic data were collected at a mean follow-up of 66
Murphy et al. 6 document a prospective study in which five patients (three male and two female, average age 53.4 years) underwent OCA transplantation for reverse Hill-Sachs lesions sustained from posterior shoulder dislocations. The size of the lesions ranged from 30% to 50% of the humeral head and fresh-frozen femoral allografts were used to restore the defects. The mean follow-up was 34 months, and radiological and functional outcomes were assessed in the outpatient setting. The mean postoperative Constant-Murley score was 83 (range, 45-96) and all shoulders had successful graft incorporation on commuted tomography (CT). Of the five total patients, four had no restriction of activities of daily living (ADLs) and three had zero pain. Based on individual radiological and functional metrics, four out of the five patients were determined to have successful outcomes. The remaining patient who had a negative overall outcome was reported to have continued pain, restricted ADLs, and a postoperative Constant-Murley score of 45. 6
Riff et al. 3 describe three additional patients (two male and one female, average age 33.7 years) who underwent fresh OCA transplantation for reverse Hill-Sachs lesions. One of these patients was lost to follow-up, but the remaining two patients were both treated with 25 mm plugs and had follow-up data obtained at a minimum 24 months. As determined by ASES scores >50, patient satisfaction with the surgical result, and lack of conversion to arthroplasty, both patients were determined to have successful outcomes. 3 A summary of all shoulders that underwent OCA transplantation for reverse Hill-Sachs lesions are included in Suppl. Table S3.
Hill-Sachs Lesions
A total of 22 patients were found across three different studies to have undergone OCA transplantation for Hill-Sachs lesions in the shoulder. 7 10
Zhuo et al. 7 describe a retrospective study involving 19 patients (12 males and seven females, mean age 21.7 years) with large Hill-Sachs lesions involving >30% (mean 35.7 ± 3.02%) of the humeral head with associated recurrent anterior instability who were treated with OCAs. The mean duration of symptoms prior to surgery was 8.05 years (range, 2-20). All patients who could not cooperate with correct rehabilitation, had previous surgery to the ipsilateral shoulder, had obvious glenoid bone loss of >20%, or had significant glenohumeral joint arthritis were excluded in their study. There were 19 concomitant procedures performed in 17 of the 19 patients, which included 17 Bankart repairs, one superior labrum repair, and one superior labrum debridement. Follow-up data were obtained at a mean of 27.8 months (minimum 24 months) and included clinical assessment of patient satisfaction, active ROM measurements, ASES scores, Constant-Murley scores, and Rowe scores. Radiological data were also collected at three months to evaluate for graft incorporation. 7
Based on the postoperative data and patient reported outcomes, 18 out of the 19 patients in the study by Zhuo et al. 7 had positive outcomes. The 18 patients with positive outcomes were either satisfied or very satisfied with the procedure and had significant improvements in clinical outcome scores (i.e., ROM, ASES, Constant Murley, and Rowe). The remaining patient with a failed outcome was not satisfied with the procedure. There were no recurrent episodes of dislocations or subluxations detected in any of the 19 patients (success or failure) during the follow-up period. Postoperative CT scans showed graft union in all 19 patients at an average of 3.47 months (range, 3-6 months) after surgery. The incidence of graft resorption at two years was 43.1%. Three demographic factors, including age (P = 0.16), duration of instability (P = 0.021), and size of Hill-Sachs lesion (P = 0.001), were determined to be statistically significant when comparing the resorption and nonresorption groups. However, no significant difference was found between these groups in terms of clinical outcome scores. 7
Chapovsky et al. 8 describe a case report in which a 16-year-old male athlete suffered from multiple anterior shoulder dislocations despite arthroscopic repair of a Bankart lesion. Subsequent magnetic resonance imaging (MRI) revealed a large, engaging Hill-Sachs lesion of the humeral head, which was then repaired arthroscopically using three fresh-frozen OCAs. The patient also underwent anterior inferior ligament repair and anterosuperior capsular shifting at the same time as the allograft. After the procedure, there were no recurrent instances of instability or dislocation, and the patient had no restrictions on activity at 12-month follow-up. He had full return-to-sport without complication and the procedure was ultimately deemed successful. 8
In the case report described by Nathan et al., 9 a fresh OCA was used to treat a 16-year-old male with autism who sustained a Hill-Sachs lesion after a seizure and resulting anterior shoulder dislocation. The lesion involved 30% of the humeral head and the patient suffered from persistent anterior shoulder instability after the injury. After undergoing open OCA transplantation, radiographs showed complete graft incorporation at 20 months and his shoulder was stable and functional at 30 months. No recurrent instances of instability or dislocations were reported and the procedure was deemed successful. 9
Sochacki et al. 10 offer a case report in which an active 19-year-old male had recurrent instances of right anterior shoulder instability in the setting of a large Hill-Sachs lesion. Preoperative imaging studies showed a lesion measuring 17.2 mm coronal width by 8 mm axial depth with 38º of articular loss. A fresh-frozen OCA using two headless compression screws was used to repair the lesion. One-year postoperative radiographs showed filling and osseous integration of the allograft. The patient also had concomitant repair of a Bankart lesion. At 14-year follow-up, the patient had no pain and no recurrent episodes of instability. He had full ROM in forward elevation, abduction, internal rotation, and external rotation as well as full, symmetrical strength compared with the contralateral shoulder. He also had a negative apprehension sign with the arm in 90º abduction and external rotation. His WOSI score was 294 at the final follow-up, and the surgery was overall determined to be successful. 10 A summary of all included shoulders who underwent OCA transplantation for Hill-Sachs lesions are included in Suppl. Table S4.
Pain Pump Chondrolysis
Riff et al. 3 documented a case series in which 10 patients underwent OCA transplantation in the shoulder for pain pump chondrolysis. The average age of the patients in this cohort was 20.9 years, and the size of the OCA plugs ranged from 15-mm in diameter to a mushroom cap plug comprising nearly the entire articular surface. Of the 10 patients, seven underwent concomitant surgeries including lateral meniscal allograft (LMA), microfracture (MFX), or both. Follow-up data were obtained at an average of 67 months and included patient satisfaction, ASES scores, VAS scores, Simple Shoulder Test (SST) scores, and SF-12. 3
Of the 10 total patients, six were determined to have failed outcomes and four were determined to have successful outcomes. Regarding the six cases of failure, four patients required conversion to total shoulder arthroplasty (TSA) and the remaining two patients were dissatisfied with the surgical result. It should be noted that in all six cases of failure, concomitant surgeries were performed. Regarding the four successful cases, all patients were satisfied, had adequate patient-reported outcome scores, and did not require conversion to TSA. 3 A summary of all included shoulders who underwent OCA transplantation for pain pump chondrolysis are included in Suppl. Table S5.
Recurrent Shoulder Instability
Seven patients in the review underwent OCA transplantation for recurrent shoulder instability.3,11,12
Riff et al. 3 document four male patients (average age 27 years) with recurrent instability that were treated with fresh OCAs. The sizes of the allografts were as follows: 18-mm plug (one patient), 30-mm plug (one patient), and mushroom plugs (two patients, both with concomitant LMA). Follow-up data were obtained at an average of 67 months and included patient satisfaction, ASES scores, VAS scores, Simple Shoulder Test (SST) scores, and SF-12. Using these metrics, two patients were determined to have successful outcomes and one patient was determined to have a failed outcome. The remaining patient was lost to follow-up. Regarding the patient with a failed outcome, it should be noted that a mushroom graft was used and a concomitant LMA procedure was performed. No concomitant procedures were performed in the patients with successful outcomes. 3
Millet et al. 11 offer two additional patients who were successfully treated with fresh OCAs for recurrent instability. The ages of the patients were 15 and 16 years, respectively, and both were male. Follow-up data were collected at 24 months and included CT evaluation of the graft; Disabilities of the Arm, Shoulder, and Hand (DASH) scores; ASES scores; VAS pain scores; and recurrent instances of instability. Both patients had improved pain, resolution of mechanical symptoms, successful return to sport, adequate patient-reported outcome scores, and no recurrences of instability. Postoperative CT evaluation showed full bony integration of the grafts in both cases. 11
The case report by Petrera et al. 12 illustrates the successful use of a fresh glenoid OCA in the treatment of chronic posttraumatic posterior instability associated with glenoid bone loss in a 54-year-old male football player. At his 24-month follow-up, radiographs confirmed concentric glenohumeral joint alignment without evidence of pseudoarthrosis or osteolysis. Moderate glenohumeral osteoarthritis was noted. The patient had full ROM in all directions except internal rotation, which was limited to the thoracolumbar level. He had 5/5 strength in all directions and was fully satisfied with the procedure. 12 A summary of all shoulders who underwent OCA transplantation for recurrent shoulder instability are included in Suppl. Table S6.
Osteoarthritis/Degenerative Changes
Five patients were identified as having underwent OCA transplantation for osteoarthritis/degenerative changes in the glenohumeral joint. 13
Familiari et al. 13 treated five patients (three men and two women, average age 46.4 years) with glenohumeral osteoarthritis using fresh-frozen allografts. All five patients also underwent concomitant hemiarthroplasty (HA). Due to persistent pain, three of the five patients required conversion to TSA at 9, 12, and 30 months, respectively, and therefore, were considered cases of failure. For the remaining two patients, one had a full recovery and a subjective shoulder value (SSV) of 83% and Constant-Murley score of 91 at final follow-up. The remaining patient had persistent anterior shoulder pain with internal rotation at one year follow-up, but at subsequent follow-ups (between 3 and 8 years) had an uncomplicated and satisfactory course with an SSV of 80% and Constant-Murley of 59. 13 A summary of all shoulders that underwent OCA transplantation for osteoarthritis/degenerative changes are included in Suppl. Table S7.
Radiofrequency Chondrolysis
McCarty et al. 14 explain a case study in which a 16-year-old female was treated with an OCA for radiofrequency chondrolysis. The patient, a competitive gymnast, experienced chronic right shoulder pain during activity and was initially determined to have anterior shoulder instability. A course of physical therapy was unsuccessful, and the patient underwent an arthroscopic stabilization procedure during which a radiofrequency energy device was used to treat the anterior capsule. After continued shoulder discomfort and progressive loss of motion for 1 year after the procedure, she then underwent arthroscopic debridement and capsular release. These additional procedures provided minimal symptomatic relief. 14
Two years after thermal capsulorrhaphy, radiographs demonstrated loss of glenohumeral joint space, cyst formation on both the glenoid and humeral sides of the joint, and osteophyte formation. The patient underwent repeat right shoulder arthroscopy to assess the condition of the glenohumeral cartilage, which showed a markedly attenuated anterior capsule and significant cartilage loss. They proceeded with an open revision capsular release followed by glenoid microfracture and resurfacing using small intestine submucosa. Her condition improved initially with decreased pain and increased ROM, but at 4-months postoperatively, she was involved in a high-energy motor vehicle collision which was followed by a return of her shoulder pain and loss of motion. An MRI showed progressive degenerative changes in the joint attributed to the prior thermal capsulorrhaphy. After a failed course of physical therapy and given the patient’s young age, high functional demands, and desire to avoid artificial joint replacement, the decision was made to reconstruct the proximal humerus using a fresh-frozen OCA and resurface the glenoid using a lateral meniscal allograft. 14
At 12-month follow-up, the patient’s visual analog score had improved from 4 to 0, SST had improved from 1 to 8, ASES had improved from 50 to 83, and SF-12 Physical Component score had improved from 29 to 46. Her SF-12 Mental Component score had remained constant at 59. At 24-months, the patient still had no pain and her active ROM measurements for forward elevation, external rotation, and internal rotation were 160°, 50°, and T12, respectively. Radiographic evaluation at 24-months showed joint space preservation without evidence of graft collapse or hardware migration. 14
The case series by Riff et al. 3 documents a 20-year-old female with radiofrequency chondrolysis who was successfully treated with a fresh, mushroom-shaped OCA. The patient also underwent a lateral meniscal allograft procedure at the same time and follow-up data were obtained at a cohort average of 67 months. Based on an ASES score >50, lack of required conversion to TSA, and patient-reported satisfaction with the result, the procedure was considered a success. 3
A summary of all shoulders who underwent OCA transplantation for radiofrequency chondrolysis are included in Suppl. Table S8.
Prominent Suture Anchors
Riff et al.’s 3 case series included an instance of prominent suture anchors in a 21-year-old male that were successfully treated with a fresh OCA. The patient received a mushroom plug graft and also underwent a concomitant LMA procedure. Follow-up data were collected at an average of 67 months for all patients in Riff et al.’s cohort. In this patient’s case, the operation was considered successful based on patient satisfaction, lack of requirement for re-operation, and adequate postoperative subjective scores (i.e., VAS for pain, ASES, SST, SF-12). 3
Provencher et al. 17 document a case report in which a 25-year-old male was successfully treated with fresh OCA for extensive glenohumeral degenerative changes caused by a loose but prominent metal suture anchor from a prior Bankart repair. The patient had two plugs (one 20 mm and one 25 mm) placed in a snowman fashion. At 16-month follow-up, the patient had near-complete resolution of pain (rated 0-1/10 compared with 6/10 preoperatively), adequate ROM measurements, and full muscle strength in all muscle groups. CT at final follow-up showed complete incorporation of both grafts with excellent articular conformity. There was no evidence of resorption and the patient was extremely satisfied with his outcome. 17
A summary of all shoulders who underwent OCA transplantation for prominent suture anchors is included in Suppl. Table S9.
Glenoid Lesion
Camp et al. 15 detailed a case report of a 25-year-old male, multi-sport athlete who underwent OCA transplantation for an isolated glenoid lesion. The patient had no acute traumatic event and had no history of instability or dislocation. After failing a comprehensive course of physical therapy, an MRI was obtained and showed a central osseous defect in the glenoid measuring 16 × 7 mm, a large cavitary cystic lesion in the glenoid with surrounding bone marrow edema, and high-grade chondromalacia of the overlying cartilage. There were some degenerative changes to the anterior and posterior labrum, but no evidence of obvious labral tearing, rotator cuff abnormality, or humeral-sided cartilage lesions. The decision was made to proceed with OCA transplantation to the glenoid lesion using a fresh medial plateau tibial OCA. Postoperative MRIs at 3 and 6 months showed successful graft incorporation with appropriate congruity of the articular surfaces of the graft and glenoid. Compared with preoperative scores, the patient’s SSV score improved 59% (from 40% to 99%), ASES score improved 46 points (from 46 to 92), and QuickDASH (shortened Disabilities of Arm, Shoulder, and Hand) improved 34 points (from 36 to 2). It should be noted that the patient developed a transient plexopathy, which Camp et al. attribute to possible traction-related injury. However, at 6 months, the plexopathy resolved and the patient had fully restored sensation and strength (5/5 throughout). 15 A summary of this case is included in Suppl. Table S10.
Osteochondritis dissecans
Johnson et al. 16 describe a case report in which a 19-year-old male underwent OCA transplantation for osteochondritis dissecans (OCD) of the humeral head in his dominant arm occurring after a fall onto an outstretched arm during a soccer game. Radiographs showed a radiolucent area in the humeral head that was approximately 2 cm in diameter, and an MRI confirmed the presence of OCD. After undergoing two separate debridement procedures with only transient relief in symptoms, the patient and surgeon agreed to proceed with OCA transplantation to the humeral head using a matched, fresh-frozen graft. At 3-year follow-up, the patient had no pain at rest or with overhead activities, a smooth pain-free arc of abduction, and no crepitation. Radiographs confirmed incorporation of the allograft and the patient returned to participating in soccer, tennis, and golf. 16 A summary of this case is included in Suppl. Table S11.
Discussion
This is the first systematic review, to our knowledge, to collate and characterize the use of OCA in the shoulder. Nonetheless, the identified indications included a wide spectrum of etiology, including impaction fractures of the shoulder as a result of dislocation events (e.g., Hill-Sachs and reverse Hill-Sachs lesions), failed prior surgery for recurrent instability, and postarthroscopy chondrolysis. Using the outcomes at final follow-up (cohort average 45.7 months, range 12-168 months), the overall success rate for OCA transplantation across the wide range of these shoulder etiologies was 82%, with 68 successes, 13 failures, and two lost to follow-up (LFU). In order to identify whether concomitant surgery may have confounded the success or failure of each OCA procedure, a contingency table chi-squared test was performed for all shoulders except those who were lost to follow-up or performed for pain pump chondrolysis. Results showed that concomitant surgeries may have influenced the results of OCA procedures.
It should be noted, however, that the observed success rate is based on cohorts that skew young in age ( Table 1 ). The mean (±standard deviation) age of patients from the cohorts included in this review is 31.2 ± 12.8 years. Thus, any interpretation of OCA outcomes, and any recommendations that may be derived from this, should be taken in the context of this younger patient demographic.
The results of this review also illustrate the relative effectiveness of OCAs in treating “pain pump chondrolysis,” as 4 of 10 patients with this historically complicated condition had relative “successful” outcomes. This iatrogenic pathology typically represents a complication in young patients who present with advanced degenerative joint disease and who are not optimal candidates for shoulder arthroplasty. OCA in this population, as with the other complex indications, represents an alternative treatment option for biologic joint reconstruction of the shoulder.
Of note, this data set includes majority utilization of fresh-frozen allograft with only 25 cases reporting the use of fresh OCA. OCAs can be categorized into three main types: fresh, fresh-frozen, and cryopreserved. Fresh OCAs are harvested within 24 hours of the donor’s death and are stored at 4°C (39.2°F) in a variety of sterile media to allow time for infectious disease screenings to be completed. 20 The benefit of fresh allografts stems from preservation of chondrocyte health, as suggested by Görtz and Bugbee et al. (2006, Journal of Bone and Joint Surgery) and confirmed in animal studies by Pallante-Kichura et al. (2013, Journal of Orthopaedic Research) and in human studies using delayed gadolinium-enhanced MRI to compare native and transplanted cartilage by Brown et al. (2014, Journal of Bone and Joint Surgery).21,22,23 In contrast, fresh-frozen allografts undergo deep-freezing procedures to as low as −80ºC, which has been shown to prolong shelf-life, improve graft availability, and reduce immunogenicity, but seem to result in reduced chondrocyte viability.21,22 Cryopreserved allografts similarly undergo deep-freezing to as low as −70°C, but are uniquely stored in cryoprotectant chemicals such as glycerol or dimethyl sulfoxide. 24 Cryopreserved methods have shown variable degrees of cell viability, the reasons for which are still subject of debate. 21 The focus of our review was to provide a descriptive, rather than exhaustive, list of indications and outcomes of OCA transplantation in the shoulder. Three studies (two case reports with one patient each and one case series with four patients) were identified in our review process that utilized cryopreserved allografts. 25 Had these three studies been included, they would add very few patients (six total) and no new indications. Now that we have outlined the uses of OCA technology in the shoulder, as a separate study, it would be interesting to compare efficacy of fresh versus cryopreserved allografts in humans.
Also of note, we observed that avascular necrosis (AVN) was not included among the indications of reported cases. AVN is a well-described indication in other joints and has been the index diagnosis for cases of OCA transplantation in the proximal shoulder conducted by the senior author. As a result, we have separately reported a case describing the use of OCA to successfully treat avascular necrosis in the proximal humerus. That case is not included in the data presented here.
We recognize that a major limitation of this review is the level of evidence, with the majority of publications meeting criteria being case reports or case series. No properly conducted clinical trials were available in the literature. Moreover, the case reports and case series that were included reported inconsistent patient-reported outcome metrics, which were used to determine success or failure of the procedure.
Conclusion
This systematic review collates the various indications for OCA transplantation in the shoulder joint specifically. It also illustrates the effectiveness of OCA as a biologic treatment option for a wide range of difficult-to-treat shoulder conditions, illustrating the increasingly available nature of this procedure. While the current literature is limited as it pertains to OCA in the shoulder with most articles being case reports and case series, it represents a ripe area of research moving forward and could benefit from multi-center trial evaluation of more common and primary indications.
Supplemental Material
sj-docx-1-car-10.1177_19476035231205678 – Supplemental material for Osteochondral Allograft Transplantation in the Shoulder: A Systematic Review of Indications and Outcomes
Supplemental material, sj-docx-1-car-10.1177_19476035231205678 for Osteochondral Allograft Transplantation in the Shoulder: A Systematic Review of Indications and Outcomes by Brian Prigmore, Suzanne Tabbaa and Dennis C. Crawford in CARTILAGE
Supplemental Material
sj-docx-10-car-10.1177_19476035231205678 – Supplemental material for Osteochondral Allograft Transplantation in the Shoulder: A Systematic Review of Indications and Outcomes
Supplemental material, sj-docx-10-car-10.1177_19476035231205678 for Osteochondral Allograft Transplantation in the Shoulder: A Systematic Review of Indications and Outcomes by Brian Prigmore, Suzanne Tabbaa and Dennis C. Crawford in CARTILAGE
Supplemental Material
sj-docx-2-car-10.1177_19476035231205678 – Supplemental material for Osteochondral Allograft Transplantation in the Shoulder: A Systematic Review of Indications and Outcomes
Supplemental material, sj-docx-2-car-10.1177_19476035231205678 for Osteochondral Allograft Transplantation in the Shoulder: A Systematic Review of Indications and Outcomes by Brian Prigmore, Suzanne Tabbaa and Dennis C. Crawford in CARTILAGE
Supplemental Material
sj-docx-3-car-10.1177_19476035231205678 – Supplemental material for Osteochondral Allograft Transplantation in the Shoulder: A Systematic Review of Indications and Outcomes
Supplemental material, sj-docx-3-car-10.1177_19476035231205678 for Osteochondral Allograft Transplantation in the Shoulder: A Systematic Review of Indications and Outcomes by Brian Prigmore, Suzanne Tabbaa and Dennis C. Crawford in CARTILAGE
Supplemental Material
sj-docx-4-car-10.1177_19476035231205678 – Supplemental material for Osteochondral Allograft Transplantation in the Shoulder: A Systematic Review of Indications and Outcomes
Supplemental material, sj-docx-4-car-10.1177_19476035231205678 for Osteochondral Allograft Transplantation in the Shoulder: A Systematic Review of Indications and Outcomes by Brian Prigmore, Suzanne Tabbaa and Dennis C. Crawford in CARTILAGE
Supplemental Material
sj-docx-5-car-10.1177_19476035231205678 – Supplemental material for Osteochondral Allograft Transplantation in the Shoulder: A Systematic Review of Indications and Outcomes
Supplemental material, sj-docx-5-car-10.1177_19476035231205678 for Osteochondral Allograft Transplantation in the Shoulder: A Systematic Review of Indications and Outcomes by Brian Prigmore, Suzanne Tabbaa and Dennis C. Crawford in CARTILAGE
Supplemental Material
sj-docx-6-car-10.1177_19476035231205678 – Supplemental material for Osteochondral Allograft Transplantation in the Shoulder: A Systematic Review of Indications and Outcomes
Supplemental material, sj-docx-6-car-10.1177_19476035231205678 for Osteochondral Allograft Transplantation in the Shoulder: A Systematic Review of Indications and Outcomes by Brian Prigmore, Suzanne Tabbaa and Dennis C. Crawford in CARTILAGE
Supplemental Material
sj-docx-7-car-10.1177_19476035231205678 – Supplemental material for Osteochondral Allograft Transplantation in the Shoulder: A Systematic Review of Indications and Outcomes
Supplemental material, sj-docx-7-car-10.1177_19476035231205678 for Osteochondral Allograft Transplantation in the Shoulder: A Systematic Review of Indications and Outcomes by Brian Prigmore, Suzanne Tabbaa and Dennis C. Crawford in CARTILAGE
Supplemental Material
sj-docx-8-car-10.1177_19476035231205678 – Supplemental material for Osteochondral Allograft Transplantation in the Shoulder: A Systematic Review of Indications and Outcomes
Supplemental material, sj-docx-8-car-10.1177_19476035231205678 for Osteochondral Allograft Transplantation in the Shoulder: A Systematic Review of Indications and Outcomes by Brian Prigmore, Suzanne Tabbaa and Dennis C. Crawford in CARTILAGE
Supplemental Material
sj-docx-9-car-10.1177_19476035231205678 – Supplemental material for Osteochondral Allograft Transplantation in the Shoulder: A Systematic Review of Indications and Outcomes
Supplemental material, sj-docx-9-car-10.1177_19476035231205678 for Osteochondral Allograft Transplantation in the Shoulder: A Systematic Review of Indications and Outcomes by Brian Prigmore, Suzanne Tabbaa and Dennis C. Crawford in CARTILAGE
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Institutional ethics approval was not required as this systematic review retrieved and analyzed data from previously published studies.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.