
Abstract
Objective
To identify preoperative imaging-based indicators of knee degeneration that correlate with graft failure risk and postoperative clinical outcome scores after osteochondral graft treatment for chondral defects of the knee.
Design
Prospectively collected data from 113 patients (mean age, 34 years; 65% male) treated with mosaicplasty or osteochondral allograft transplantation (OCA) was reviewed. Four different aspects of knee degeneration were examined based on preoperative radiographs or magnetic resonance imaging: (1) Osteoarthritis using the Kellgren-Lawrence (KL) grading system, (2) meniscus volume, (3) meniscus quality, and (4) synovitis. Primary outcomes included graft failure, defined by removal/revision of the graft or conversion to arthroplasty, and patient responses to clinical outcome scores.
Results
Forty-one knees (36%) underwent mosaicplasty, and 72 knees (64%) underwent OCA. Mean duration of follow-up was 4.5 years (range, 2-14 years). A preoperative KL grade of ≥3 was correlated with increased failure rates (P = 0.01), lower postoperative International Knee Documentation Committee form (IKDC), Activities of Daily Living of the Knee Outcome Survey (KOS-ADL), and Overall Condition scores (P < 0.01), and decreased improvement in Overall Condition scores (P = 0.01). Within an individual tibiofemoral compartment, a preoperative meniscus volume grade of ≥3 (indicating <50% meniscus volume remaining) was correlated with increased condylar graft failure rates (P < 0.01). Preoperative meniscus quality and synovitis grades were not associated with graft failure rates or clinically meaningful differences in postoperative outcome scores.
Conclusions
Greater preoperative osteoarthritis and meniscus volume loss were correlated with increased graft failure rates after osteochondral graft treatment for chondral defects of the knee.
Introduction
Focal chondral defects of the knee often coexist with early cartilage degeneration and osteoarthritis (OA). It is believed that an initial insult to the articular cartilage leads to an increased production of inflammatory mediators, matrix metalloproteinases, aggrecanases, and other proteases that continue to degrade the cartilage matrix in the joint, resulting in the loss of normal joint homeostasis.1-3 Clinically, these initial processes can manifest as persistent knee effusions with synovitis,4,5 and this sustained cascade of inflammation and catabolic enzyme activity precedes the development of overt radiographic abnormalities. 6
Cartilage restoration techniques can reestablish the articular surface congruity interrupted by focal defects. Cartilage restoration procedures may also be combined with concomitant osteotomies and/or ligament reconstruction to restore lower limb alignment and stability, respectively. However, there are few management strategies that effectively and sustainably address the inflammatory processes within the joint. These biochemical abnormalities can result in the progression of cartilage degradation and early failure of a newly implanted cartilage graft. This coincides with the observation that older patients, who generally have more advanced degenerative disease, have less favorable outcomes after a cartilage restoration procedure than younger patients.7-10
Mosaicplasty (osteochondral autograft transfer) and fresh osteochondral allograft transplantation (OCA) are popular cartilage restoration techniques that involve the single-stage transfer of viable, mature hyaline cartilage. These procedures have demonstrated 5- and 10-year survival rates of over 80%, as well as high rates of patient satisfaction and return to sport.11-15 Because of the ability of these structural osteochondral grafts to bear loads in the early postoperative period, treatment with mosaicplasty and OCA allow for a faster rehabilitation compared to cell-based cartilage repair strategies. However, despite their structurally stable nature, it is unknown whether preexisting intra-articular catabolic processes can compromise the integration and longevity of these grafts after implantation. For example, in the hip arthroscopy literature, a Tönnis grade of 2 or more on preoperative radiographs has been shown to predict a higher rate of conversion to total hip arthroplasty and less predictable improvement in outcome scores.16,17 For clinicians considering mosaicplasty or OCA for their patients, a similar preoperative imaging-based indicator of overall knee degeneration that correlates with the clinical outcomes of these procedures would help guide clinical decision making and aid in managing patient expectations. Although previous studies have examined the association of patient age with the outcomes of cartilage restoration surgery, no studies have specifically examined correlations between preexisting joint degeneration and the risk of graft failure or clinical outcome scores after mosaicplasty and OCA.
The purpose of this study was to identify preoperative imaging-based indicators of knee degeneration that correlate with risk of graft failure and postoperative clinical outcome scores after osteochondral graft treatment for chondral defects of the knee. The hypothesis was that increased osteoarthritis, decreased meniscus volume, and increased synovitis would be associated with a higher risk of graft failure and less improvement in clinical outcome scores.
Materials and Methods
Inclusion and Exclusion Criteria
Inclusion criteria included (1) symptomatic focal cartilage lesions (up to 2 affected areas) in the knee that were classified as International Cartilage Repair Society (ICRS) grade III/IV lesions at the time of OCA and did not involve substantial bone loss requiring shell allografts or additional bone grafting, (2) treatment with mosaicplasty or fresh OCA, and (3) a minimum of 2 years of follow-up. Exclusion criteria included (1) concomitant meniscus allograft transplantation (MAT) and (2) patellar or bipolar lesions treated with these cartilage procedures, since higher failure rates have been reported for these locations compared to the femoral condyles or trochlea.18-21 General contraindications that were followed for these cartilage procedures were advanced osteoarthritis (OA) involving all three compartments, simultaneous multiligamentous reconstruction, inflammatory arthritis or autoimmune conditions, and inability to comply with the postoperative rehabilitation protocol.
Patients
Data were queried from a single institutional registry dedicated to the prospective tracking of patient outcomes after articular cartilage restoration procedures. An institutional review board approved the registry, and all patients sign an informed consent form before participation. Of the 1,949 registry surgeries screened, 440 (23%) surgeries performed between 2002 and 2015 met the inclusion criteria. Of these, 154 patients did not have the minimum 2 years of follow-up. Seventy-seven patients did not have preoperative outcome scores and were thus excluded. Of the remaining knees, 6 were treated with concomitant MAT, 62 were treated with mosaicplasty or OCA of the patella, and 28 did not have a preoperative radiographs or magnetic resonance imaging (MRIs). These knees were therefore excluded. As a result, 113 knees in 113 patients had complete data and were analyzed. Demographic, preoperative, intraoperative, and postoperative data were collected for these patients. Demographic data included age, sex, and body mass index (BMI). Preoperative data included the number and type of previous ipsilateral knee surgical procedures and baseline patient-reported outcome scores. Standing lower limb alignment was assessed and recorded during the preoperative office visit. The use of preoperative long-leg radiographs to assess lower limb alignment was dependent on the individual surgeon’s practice; for the majority of patients, long-leg radiographs were only obtained if gross malalignment was detected and osteotomy was being considered. Intraoperative data included laterality, exam under anesthesia (range of motion, ligamentous stability), location, size and depth of the chondral defect(s), status of the articular surfaces in other compartments, meniscus status and concomitant procedures performed. Postoperative data included postoperative rehabilitation protocol, complications, reoperations, and patient-reported outcome scores at a minimum of two years after surgery.
Osteoarthritis, Meniscus Volume, Meniscus Quality, and Synovitis Scoring
Predetermined scoring systems ( Table 1 ) were used to assign grades representative of the degree of OA, meniscus volume, meniscus quality, and synovitis for each patient. OA grades were assigned from retrospective review of preoperative radiographs using the Kellgren-Lawrence (KL) grading system. 22 Meniscus volume, meniscus quality, and synovitis grades were assigned from the retrospective review of preoperative MRIs. Meniscus volume and quality grades were assessed for the compartment (medial or lateral) that was treated with mosaicplasty or OCA; therefore, knees that were treated for isolated trochlea defects were excluded from this particular analysis. Synovitis grades were assigned using the synovial thickening component of the WORMS (Whole-Organ Magnetic Resonance Imaging Score). 23 Additionally, the presence of loose bodies, fronds, and/or debris was noted. All scoring was performed by fellowship-trained musculoskeletal radiologists (V.K. and A.J.B.) blinded to the outcomes.
Osteoarthritis, Meniscus, and Synovitis Scoring Criteria.
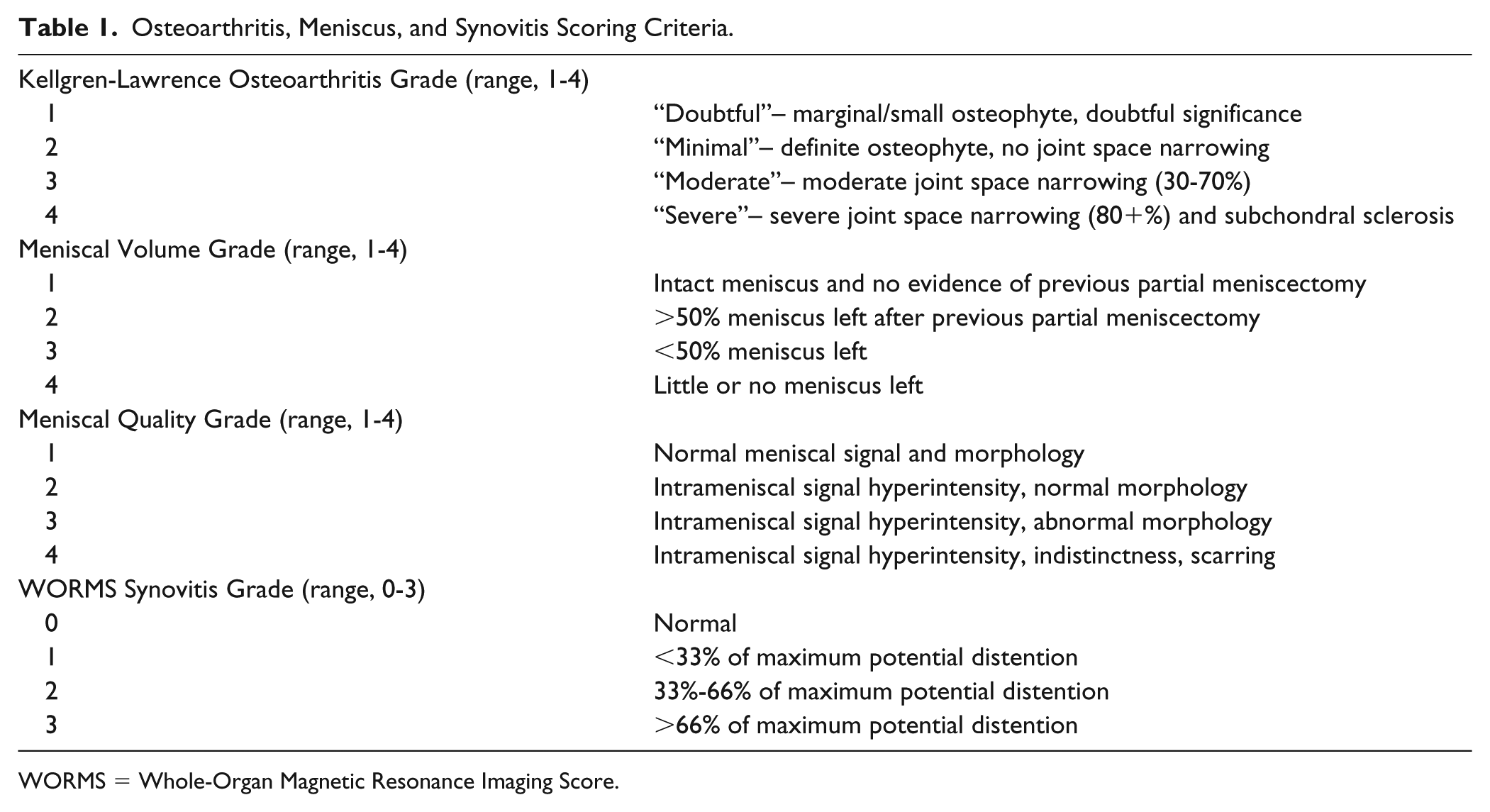
WORMS = Whole-Organ Magnetic Resonance Imaging Score.
Surgical Indications for Mosaicplasty and OCA
Mosaicplasty or OCA was selected as the treatment option for these patients based on clinical judgement of defect complexity, location, and size, and failure of previous surgical or nonsurgical treatments. The decision to perform either mosaicplasty or OCA was strictly based on chondral defect size; generally, mosaicplasty was performed for defects <2 cm2 in total area, and OCA was performed for defects ≥2 cm2 in total area. Prior failure of other cartilage restoration procedures such as microfracture was not a contraindication for these procedures. Autologous chondrocyte implantation (ACI) was rarely performed at our institution because of its 2-stage process and slower rehabilitation compared with that for osteochondral grafting.
Surgical Technique
All surgical procedures were performed by two fellowship-trained orthopedic surgeons (R.J.W. and S.A.R.) at a single institution with extensive experience in cartilage repair procedures. The decision to perform either mosaicplasty or OCA was generally based on a chondral defect area of <2 cm2 and ≥2 cm2, respectively. Any meniscus tears were addressed with arthroscopic partial meniscectomy or repair. Mosaicplasty was performed according to the method described by Hangody et al. 24 Donor osteochondral plugs were harvested from either the intercondylar notch or superolateral margin of the trochlea by hand with use of commercially available instruments (Arthrex, Naples, FL) and placed flush with the surrounding articular cartilage. The mean number of plugs transferred was 2.3 (range, 1-4). Fresh OCA was performed according to the dowel technique described by Williams et al. 25 Fresh cold-stored osteochondral allografts were obtained from commercially available sources. Preoperatively, donor and recipient were matched on the basis of size using standard anteroposterior radiographs. The mean number of dowels transplanted was 1.7 (range, 1-4).
Postoperatively, all patients remained touchdown or nonweightbearing for a minimum of 1 to 2 weeks. Immediate full range of motion was permitted. Brace wear was discontinued at 2 to 6 weeks, based on restoration of quadriceps strength and function. A supervised physical therapy program was undertaken postoperatively in all cases. The duration of the postoperative physical therapy program was dependent on the restoration of normal gait, return of quadriceps function, and performance of sport-specific skills. Return to athletics was initiated on an individual patient basis, typically starting with a running program at 6 months. Higher level activities were then progressed depending on return of lower extremity strength, coordination, balance, and proprioception.
Assessment of Clinical Outcomes
All reoperations after the index mosaicplasty or OCA were documented. Graft failure was defined as any procedure that involved removal or revision of the osteochondral graft, unicompartmental knee arthroplasty (UKA), or total knee arthroplasty (TKA). Patient-reported knee function was assessed with use of the International Knee Documentation Committee subjective form (IKDC) and the Knee Outcome Survey-Activities of Daily Living (KOS-ADL).26,27 Activity level was assessed with use of the Marx activity rating scale. 28 Finally, the overall condition of the knee was assessed using the patient perception component of the Cincinnati Knee Rating System. 29 This is a single item that asks “Rate the overall condition of your knee at the present time” on a numeric 1 to 10 rating scale, with 2 indicating “poor—I have significant limitations that affect activities of daily living,” 4 indicating “fair—I have moderate limitations that affect activities of daily living, no sports possible,” 6 indicating “good—I have some limitations with sports but I can participate; I compensate,” 8 indicating, “very good—I have only a few limitations with sports,” and 10 indicating “normal/excellent—I am able to do whatever I wish (any sport) with no problems.” 29 An independent observer performed postoperative data collection for all clinical outcome instruments.
Statistical Analysis
For each grading scheme, Kaplan-Meier survivorship analysis was performed for failures, with comparisons among groups conducted using the log-rank test. Comparison of subjective patient outcome scores among groups was performed with the Kruskal-Wallis test and between groups with the Dunn’s post hoc test. Comparisons between factors were performed using the Mann-Whitney tests for binary characteristics, chi-square or Fisher exact tests for discrete variables, and bivariate correlations for continuous variables. Two-tailed tests were used for all statistical analyses with a critical P value set to 0.05 to indicate significance. Statistical analysis was performed using JMP Pro 13 (SAS Institute, Cary, NC).
Results
Patient demographics, chondral lesion characteristics, and concomitant procedures are shown in Table 2 . Among these patients, the mean age was 34 years (range, 11-62 years), and the mean duration of follow-up was 4.5 years (range, 2-14 years). Forty-one (36%) and 72 (64%) knees were treated with mosaicplasty and OCA, respectively. Mean age, number of prior ipsilateral knee surgeries, duration of follow-up, chondral defect area, and number of plugs implanted were significantly different between treatment groups, with mosaicplasty patients on average being younger, having fewer prior ipsilateral knee surgeries, longer follow-up, smaller chondral defect area, and treated with more plugs compared with OCA patients ( Table 2 ).
Patient Demographics and Surgery Characteristics. a
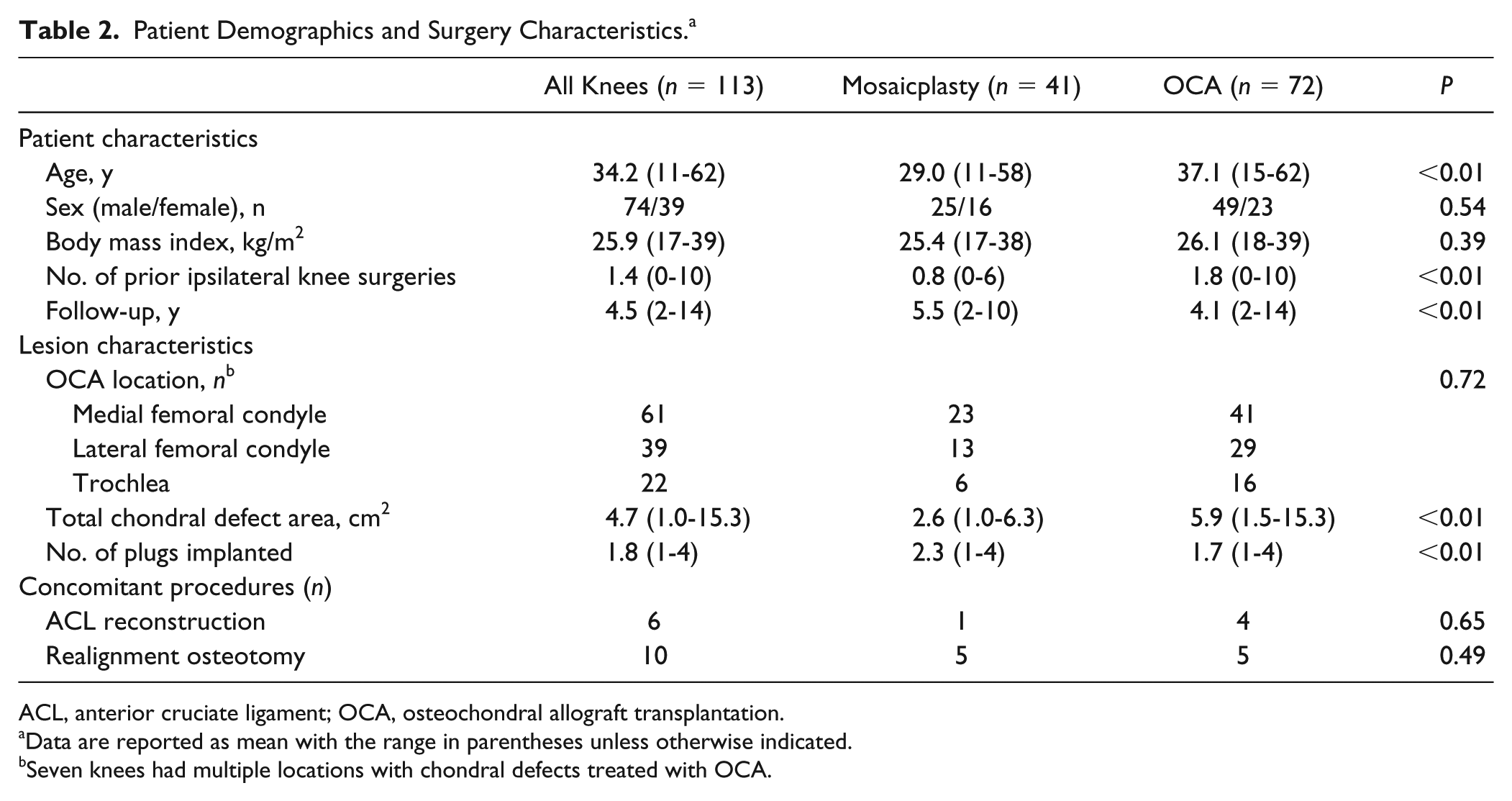
ACL, anterior cruciate ligament; OCA, osteochondral allograft transplantation.
Data are reported as mean with the range in parentheses unless otherwise indicated.
Seven knees had multiple locations with chondral defects treated with OCA.
At final follow-up, failures were documented in 22 knees (19%) as defined by evidence of graft failure (n = 6) or subsequent revision OCA (n = 5), UKA (n = 3), and TKA (n = 8). The mean time to failure was 51 months (range, 7-94 months). Failures occurred in 4 mosaicplasty patients (12%) and 18 OCA patients (24%). Kaplan-Meier survival analysis demonstrated a survivorship of 95% at 2 years and 90% at 5 years for mosaicplasty patients and 90% at 2 years and 74% at 5 years for OCA patients (P = 0.05).
Association between Preoperative Osteoarthritis Grades (Kellgren-Lawrence) and Clinical Outcomes
Preoperative radiographs were available for 97 (86%) knees for KL grading. Of these, 64%, 16%, and 20% of knees had a KL grade of 1, 2, and 3-4, respectively. The mean KL grade was 1.6. Higher KL grade was correlated with older age (P < 0.01), more previous ipsilateral knee surgeries (P < 0.01), larger chondral defect size (P < 0.01), treatment with OCA (P = 0.02), and lower preoperative Marx activity scores (P < 0.01). Kaplan-Meier survival analysis demonstrated worse graft survivorship with higher KL grades ( Fig. 1 ).
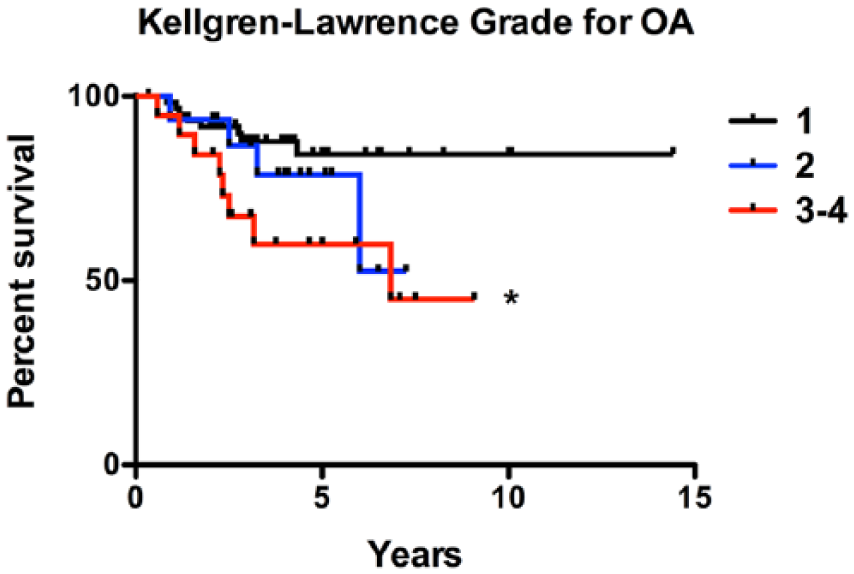
Kaplan-Meier survival analysis of patients treated with mosaicplasty or osteochondral allograft transplantation organized by preoperative Kellgren-Lawrence (KL) grade. *Indicates significant difference compared with KL grade of 1.
A KL grade of 3-4 was associated with lower postoperative IKDC, KOS-ADL, and Overall Condition scores (indicating worse scores) compared to a KL grade of 1 (P ≤ 0.01). Additionally, a KL grade of 3-4 was associated with decreased improvement in Overall Condition scores compared to a KL grade of 1 (P = 0.01) ( Fig. 2 ). Average outcome change scores for each group and statistical comparisons among groups are provided in Table 3 .
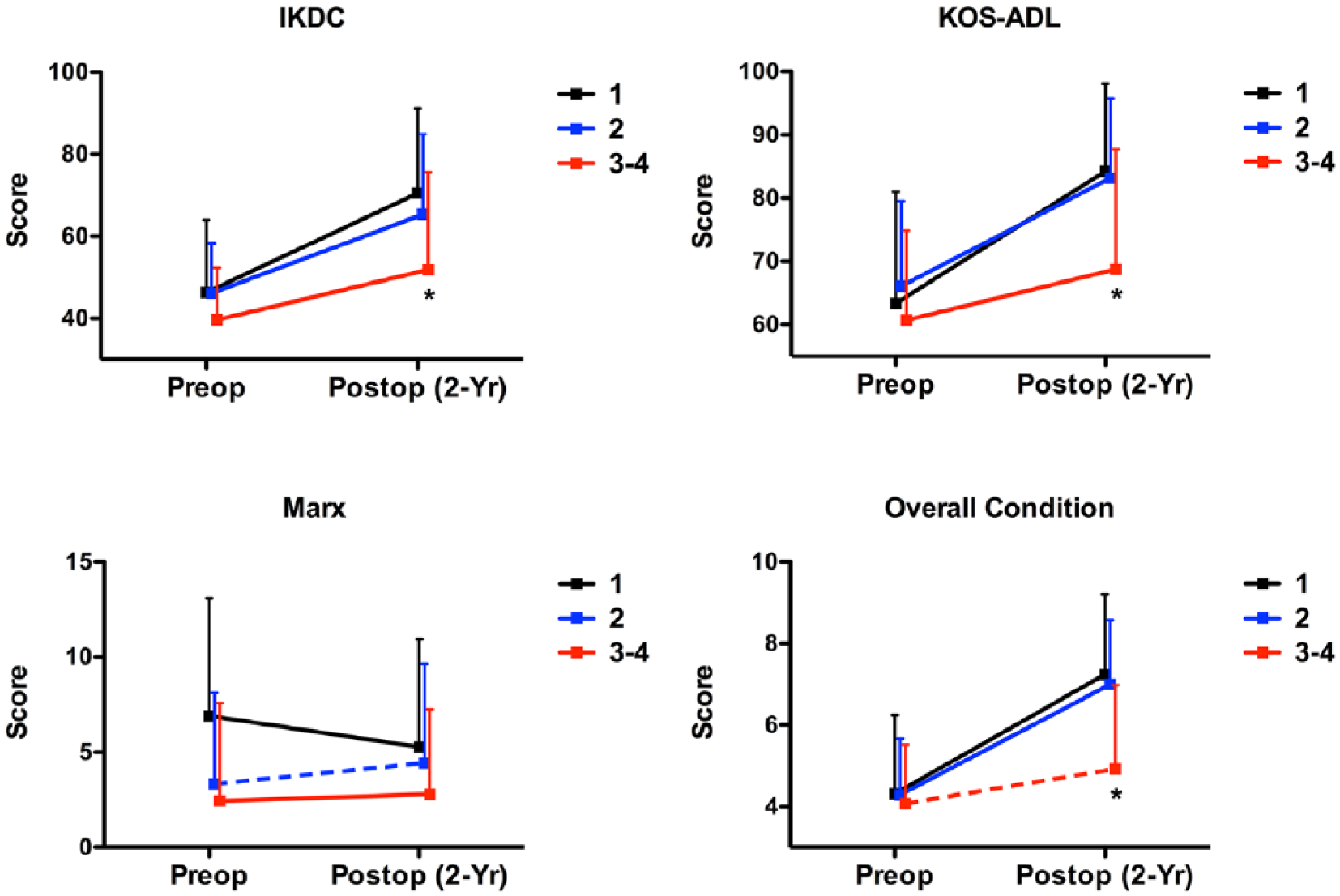
Preoperative and minimum 2-year postoperative patient-reported outcome scores organized by preoperative Kellgren-Lawrence (KL) grade. *Indicates significantly different KL 3-4 postoperative score compared with KL 1 postoperative score. Dotted line indicates significantly different change score compared with KL 1 change score.
Comparison of Outcome Change Scores by Kellgren-Lawrence, Meniscus Volume, Meniscus Quality, and WORMS Grades. a
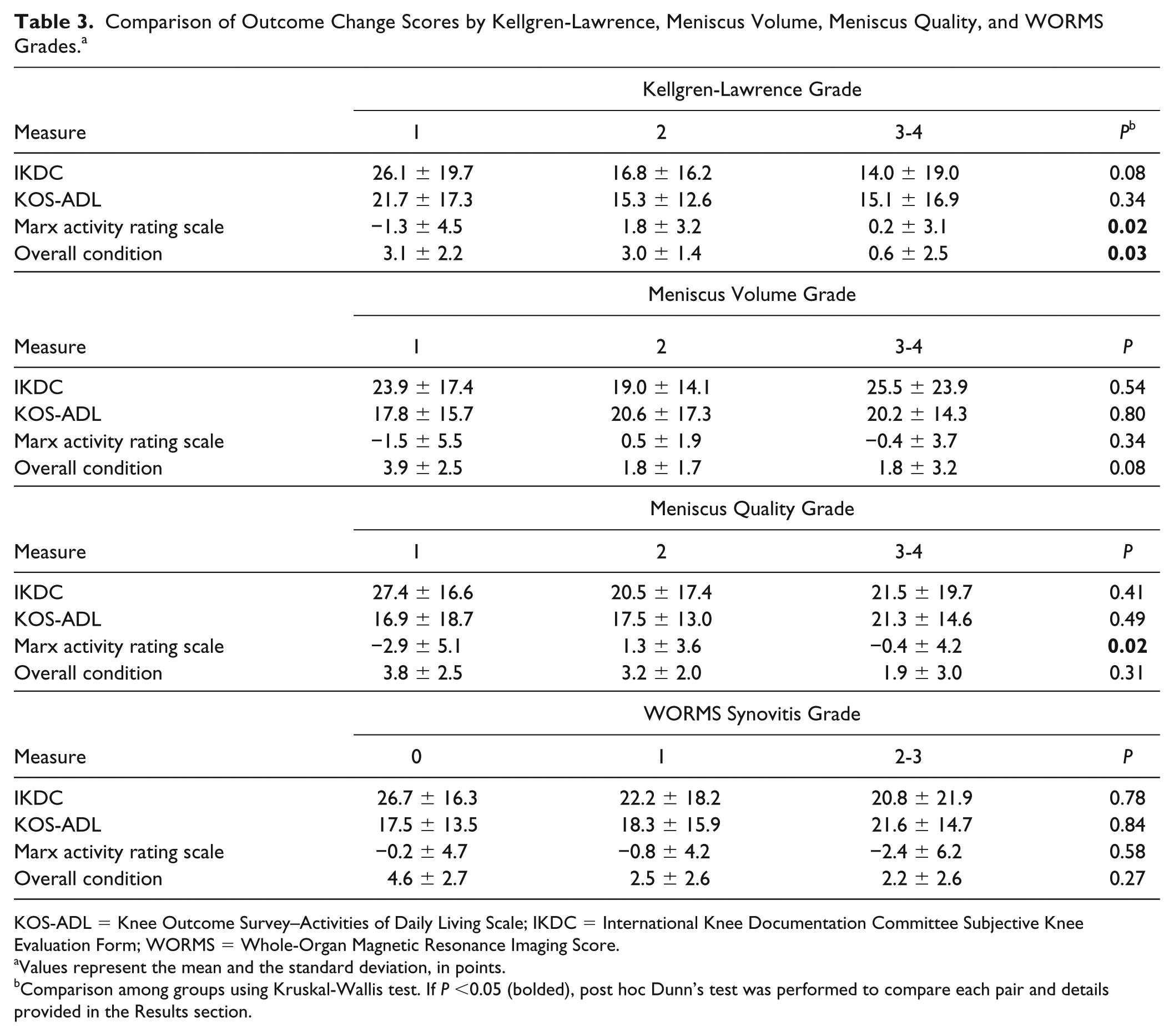
KOS-ADL = Knee Outcome Survey–Activities of Daily Living Scale; IKDC = International Knee Documentation Committee Subjective Knee Evaluation Form; WORMS = Whole-Organ Magnetic Resonance Imaging Score.
Values represent the mean and the standard deviation, in points.
Comparison among groups using Kruskal-Wallis test. If P <0.05 (bolded), post hoc Dunn’s test was performed to compare each pair and details provided in the Results section.
Association between Preoperative Meniscus Volume and Quality Grades and Clinical Outcomes
Of the knees treated for femoral condyle defects, preoperative MRIs were available for 75 (74%) knees for meniscus scoring. For meniscus volume, 53%, 24%, and 23% of knees had a grade of 1, 2, and 3-4, respectively. The mean meniscus volume grade was 1.8. Decreased meniscus volume was correlated with older age (P < 0.01), more previous ipsilateral knee surgeries (P = 0.02), larger chondral defect size (P < 0.01), treatment with OCA (P < 0.01), and higher KL grade (P < 0.01). Kaplan-Meier survival analysis demonstrated worse graft survivorship with decreased meniscus volume ( Fig. 3 ).
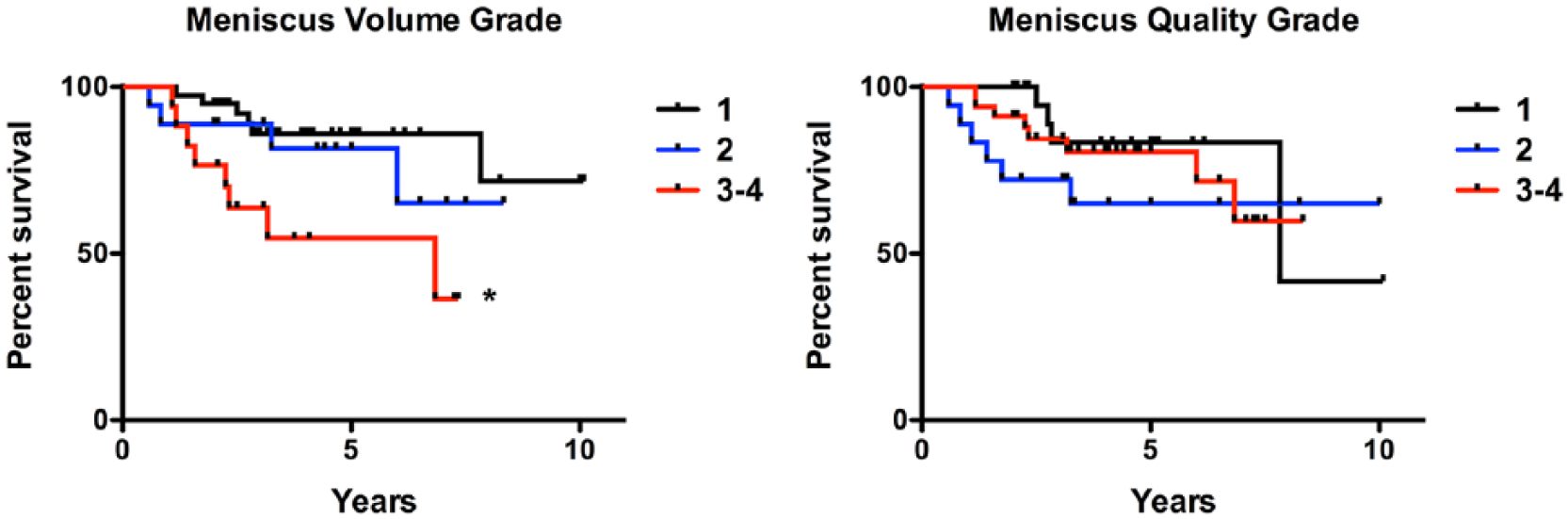
Kaplan-Meier survival analysis of patients treated with mosaicplasty or osteochondral allograft transplantation organized by preoperative meniscus volume grade and meniscus quality grade. *Indicates significant difference compared to meniscus volume grade of 1.
For meniscus quality, 31%, 24%, and 45% of knees had a grade of 1, 2, and 3-4. The mean meniscus quality grade was 1.8. Decreased meniscus quality was correlated with older age (P < 0.01), larger chondral defect size (P < 0.01), treatment with OCA (P < 0.01), higher KL grade (P < 0.01), decreased meniscus volume (P < 0.01), and lower preoperative Marx activity scores (P = 0.01). Kaplan-Meier survival analysis demonstrated no differences in graft survivorship among meniscus quality grades ( Fig. 3 ).
Meniscus volume grades of 2 and 3-4 were significantly associated with lower postoperative Marx activity scores compared with a meniscus volume grade of 1 (P = 0.04). There were no significant associations between meniscus quality grades and postoperative clinical outcome scores. Meniscus quality grades of 2 and 3-4 were significantly associated with higher Marx activity change scores compared with a meniscus quality grade of 1 (P ≤ 0.03), although the clinical relevance of this finding is uncertain ( Table 3 ).
Association between Preoperative Synovitis Grades (WORMS) and Clinical Outcomes
Preoperative MRIs were available for 75 (66%) knees for WORMS synovitis grading. Of these knees, 20% of knees had a grade of 0, 67% had a grade of 1, and 13% had a grade of 2-3. The mean preoperative WORMS grade was 0.9. Thirty-nine (52%) knees had loose bodies, fronds, and/or debris in the synovial cavity. Higher preoperative synovitis grade was correlated with male sex (P = 0.04), larger chondral defect size (P = 0.02), treatment with OCA (P < 0.01), and higher KL grade (P < 0.01). Kaplan-Meier survival analysis demonstrated no significant difference in graft survivorship among synovitis grades ( Fig. 4 ). Additionally, there was no significant association between synovitis grade and postoperative clinical outcome scores or outcome change scores ( Table 2 ).
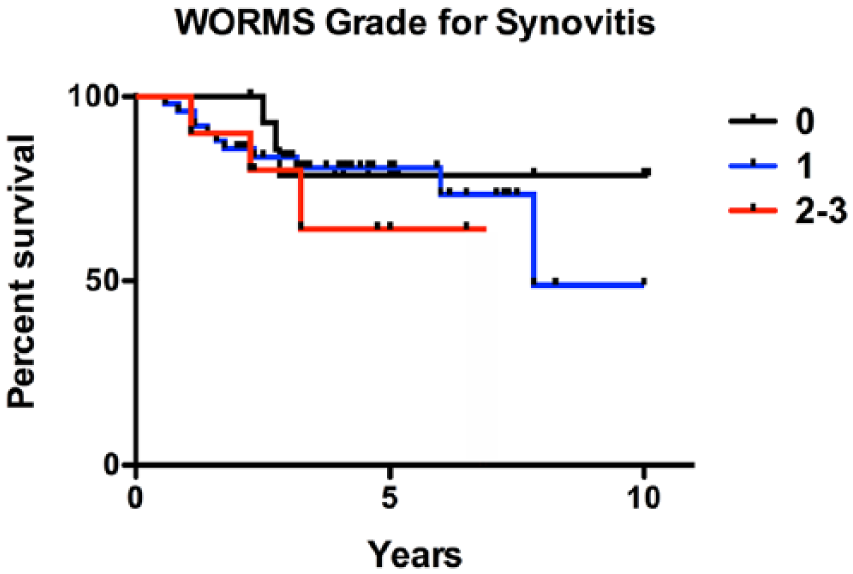
Kaplan-Meier survival analysis of patients treated with mosaicplasty or osteochondral allograft transplantation organized by preoperative whole-organ magnetic resonance imaging score (WORMS) synovitis grade. There was no significant difference in survivorship among groups.
Discussion
The principal findings of this study of knees treated with structural osteochondral grafts for cartilage defects were (1) higher preoperative KL grades were correlated with increased graft failure rates, lower postoperative IKDC, KOS-ADL, and Overall Condition scores, and decreased improvement in Overall Condition scores; (2) within an individual tibiofemoral compartment, a greater degree of meniscus volume loss was correlated with increased condylar graft failure rates; and (3) preoperative meniscus quality and synovitis grades were not associated with graft failure rates or clinically meaningful differences in postoperative clinical outcome scores.
Existing studies on cartilage restoration procedures suggest that older age is associated with higher failure rates and less improvement in clinical outcomes.7-9,12,30,31 This may primarily be a result of the degenerative processes and declining healing potential that progress with increasing age. Osteoarthritis is considered a whole-joint disease in which all of the joint tissues, including the articular cartilage, bone, and synovium, simultaneously contribute to and are affected by the intra-articular catabolic environment that results in joint destruction. 3 However, current treatment protocols generally do not directly address the preexisting milieu of pro-inflammatory cytokines, catabolic mediators, and matrix degradation enzymes at the time of a cartilage restoration surgery. Although the etiology of graft failure is often multifactorial, few studies have examined the extent to which a catabolic environment can contribute to reduced survivorship of a newly implanted cartilage graft.
Restorative cartilage procedures have gained interest and popularity as a pre-arthroplasty treatment option, particularly in younger patients. Nonetheless, when performed in the setting of OA, the clinical results of these procedures have varied widely. Hangody et al. 32 showed that despite a higher rate of preoperative osteoarthritic changes in a population of young athletic patients, clinical outcomes of mosaicplasty in this group demonstrated a success rate similar to that of patients having no OA. Similarly, Minas et al. 33 examined the outcomes of ACI in a young cohort (mean age, 38 years) with early OA and showed a 5-year survival rate of 93% and significant improvement in WOMAC (Western Ontario and McMaster Universities Osteoarthritis Index) scores. Conversely, in patients aged 40 years and older treated with OCA, Wang et al. 10 demonstrated a trend toward higher failure rates in knees with more advanced OA. Filardo et al. 34 analyzed the results of matrix-assisted autologous chondrocyte transplantation for the treatment of cartilage lesions in arthritic knees with a KL grade of 2-3. At final follow-up, 27% of patients had failed, and half of the patients considered their condition not better than before treatment.
Based on the results of this study, a KL grade of ≥3 may represent a threshold at which graft survival declines and postoperative patient-reported outcomes are inferior. This supports the theory that more advanced OA changes may compromise the healing process and regenerative potential required for optimal results after restorative chondral procedures. For condylar defects treated with osteochondral grafts, lower preoperative meniscus volumes in the treated compartment were associated with higher failure rates. The menisci primarily serve to decrease contact pressures, whereas meniscectomies have been shown to lead to overloading of the adjacent articular surfaces.35,36 These results underscore the need to address meniscus deficiency when treating condylar lesions within the same compartment and suggest using <50% meniscus volume as a threshold to consider MAT in order to improve graft survival, although, it remains to be seen whether MAT can provide sufficient chondroprotection to a cartilage graft.
We have noticed that a subset of patients experience recurrent, aseptic knee effusions after mosaicplasty and OCA within the first several months after surgery. This occurrence has not been explicitly investigated or well described. These effusions are concerning, as they can indicate the presence of catabolic processes, which may compromise the integrity of a cartilage repair. 37 Although preoperative synovitis grades were not correlated with graft failure rates and clinical outcome scores in this study, a potential causal relationship between synovitis and resultant effusion and graft survival still warrants further investigation. The findings of this study may have been limited by the use of preoperative, rather than postoperative, grades of synovitis. Measurement of synovitis, which may be increased by the cartilage surgery itself, in the early postoperative period would be more ideal since it better matches the intensity of intra-articular inflammation to which the osteochondral graft is exposed. However, immediate postoperative MRIs were not routinely obtained in this patient cohort, as this practice is not the standard of care, and thus this analysis could not be performed. Ultimately, direct measurement of inflammatory and chondrodegenerative biomarker levels in knee aspirations should be performed in order to gauge the effect of the intra-articular biologic milieu on graft integrity and clinical outcomes.
Several other limitations of this study deserve mention. Mosaicplasty and OCA patients were combined in order to perform the analyses with an appropriate level of power. However, these procedures are not identical, as mosaicplasty is done using autologous tissue and has donor-site morbidity, while an immune response may be invoked by allograft tissue transplantation. Mean follow-up was only 4.5 years, allowing us to only examine the intermediate term following osteochondral grafting. Longer follow-up would allow for more precise measurement of graft failure as an outcome, as many patients may decide to cope with pain and continue with conservative treatments for many years before eventually undergoing arthroplasty. Since this was a retrospective study, many patients who met the inclusion criteria had to be excluded since their preoperative imaging studies were not available. Additionally, intraoperative assessment of chondral damage outside of the treated defect and meniscus deficiency would be more valuable predictors compared with preoperative imaging scores, as preoperative imaging often underestimates the disease burden and OA progression. However, these factors were not recorded in detail by the registry and therefore could not be used for this study. Finally, evaluation of meniscus grades was only applicable for patients who received condylar grafts. Both these limitations restricted the number of patients that could be analyzed, potentially leading to a type II error.
In conclusion, a preoperative KL grade of 3 or more was significantly correlated with an increased graft failure rate, lower postoperative knee outcome scores, and decreased improvement in Overall Condition scores after treatment of cartilage defects with osteochondral grafts in the knee. Additionally, a preoperative meniscus volume grade of 3 or more (indicating <50% meniscus volume remaining) was significantly correlated with an increased failure rate of condylar osteochondral grafts within the same compartment. For surgeons considering mosaicplasty or OCA for their patients, these results can help guide clinical decision making and aid in managing preoperative patient expectations.
Footnotes
Authors’ Note
Investigation performed at the Hospital for Special Surgery, New York, NY.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Institutional review board approval (#2013-024-CR4) was obtained for the Hospital for Special Surgery Cartilage Repair Registry used in this study. Notification of this approval is available on request.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
All patients sign an informed consent form before participation.
Trial Registration
Not applicable.