
Abstract
Objective
To report radiographic and magnetic resonance imaging findings, patient-reported outcomes, and complications and/or reoperations following nonarthroplasty surgical intervention for focal glenohumeral cartilage defects.
Design
A literature search was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines. Patients were included if they possessed a chondral defect of the humeral head, glenoid, or both, which had been treated with a joint preserving nonarthroplasty procedure. Risk of bias assessment was performed using the Methodological Index for Non-Randomized Studies scoring system. Study demographics, surgical technique, imaging findings, patient-reported outcomes, complications, failures, and reoperations were collected.
Results
Fourteen studies with 98 patients (100 shoulders) met the inclusion criteria. Patient ages ranged from 7 to 74 years. The nonarthroplasty surgical techniques utilized included microfracture (67 shoulders), osteochondral transplantation (28 shoulders), chondrocyte transplantation (4 shoulders), and internal fixation (1 shoulder). The rates of radiographic union and progression of osteoarthritis ranged between 90% to 100% and 57% to 100%, respectively. Visual analog scores ranged from 0 to 1.9 at final follow-up. Mean postoperative ASES (American Shoulder and Elbow Surgeons) shoulder scores ranged from 75.8-100. Mean postoperative CSS (Constant Shoulder Score) scores ranged from 83.3-94. Mean postoperative SSV (Subjective Shoulder Value) ranged from 70% to 99%. Failure and reoperation rates ranged between 0% to 35% and 0% to 30%, respectively, with the most common reoperation being conversion to prosthetic arthroplasty.
Conclusions
In this systematic review, nonarthroplasty surgical techniques demonstrated acceptable rates of radiographic healing, improved patient reported outcomes, minimal complications, and low rates of failure or reoperation. Joint preserving techniques are likely viable options to prolong function of the native shoulder and provide short- to midterm pain relief in young and highly active patients.
Level of Evidence
Level IV.
Introduction
Focal cartilage defects involving the glenohumeral joint present both a diagnostic and management challenge. The etiology of cartilage injury within the glenohumeral joint can include previous surgery, trauma, osteochondritis dissecans, infection, avascular necrosis, inflammatory arthritis, glenohumeral joint instability, rotator cuff arthropathy, osteoarthritis, and chondrolysis. 1 Patients with glenohumeral cartilage or osteochondral defects may present with a variety of symptoms, including generalized achiness exacerbated with activity, progressive pain to the point of limiting sport activities, constant deep shoulder pain, sharp pain following an acute injury, or progressive crepitation associated with increasing pain.1-6
Joint-preserving interventions are preferred in younger patients with symptomatic lesions recalcitrant to conservative management, especially in patients considered too young for prosthetic joint replacement. The incidence of symptomatic glenohumeral cartilage defects has been reported to be as high as 13% to 17% in patients with rotator cuff tears 7 and overhead throwing athletes. 8 Other authors have reported a group of patients undergoing shoulder arthroscopy for subacromial impingement to have a 29% prevalence of humeral cartilage lesions and a 15% prevalence of glenoid cartilage lesions. 9
Current surgical treatment options for cartilage lesions involving the glenohumeral joint include microfracture, osteochondral autograft transfer (OAT), 10 osteochondral allograft transplantation (OCA), autologous chondrocyte implantation (ACI), 11 bulk allograft reconstruction, and shoulder arthroplasty. 12 Although symptomatic glenohumeral arthritis can be successfully treated with shoulder arthroplasty, younger and highly active patients should be considered for joint preservation surgery due to an increasing demand on shoulder replacement and potential hardware loosening. 13 A study by Sperling et al. 14 reported only 61% survivorship at 10 years in a cohort of patients with a mean age of 46 years at time of total shoulder arthroplasty.
Therefore, the purposes of this systematic review were to report radiographic healing, patient reported outcomes, and complications or reoperations following nonarthroplasty surgical intervention for glenohumeral cartilage defects. We hypothesized that there would be high rates of radiographic union and improved patient reported outcomes among the included studies.
Methods
Literature Search
A comprehensive search of the available literature was performed on November 6, 2018 according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRIMSA) guidelines ( Fig. 1 ). 15 Searched databases included PubMed (MEDLINE), the Cumulative Index for Nursing and Allied Health Literature (CINAHL), and the Cochrane Register of Controlled Trials & Cochrane Library. The search parameters were set from January 1, 1995 to November 6, 2018 and a Boolean algebra search was employed as follows: (cartilage lesion OR cartilage lesions OR cartilage defect OR cartilage defects OR osteochondral lesions OR osteochondral lesions OR osteochondral defect OR osteochondral defects) AND (glenoid OR humerus OR glenohumeral OR glenohumeral joint OR shoulder). An initial search resulted in 820 articles from PubMed, 67 articles from CINAHL, and 10 articles from Cochrane Library. All articles were organized using Microsoft Excel (2010; Microsoft Corp, Redmond, WA). Removal of duplicates and non-English articles (186 studies) resulted in 711 articles for title and abstract screening ( Fig. 1 ).
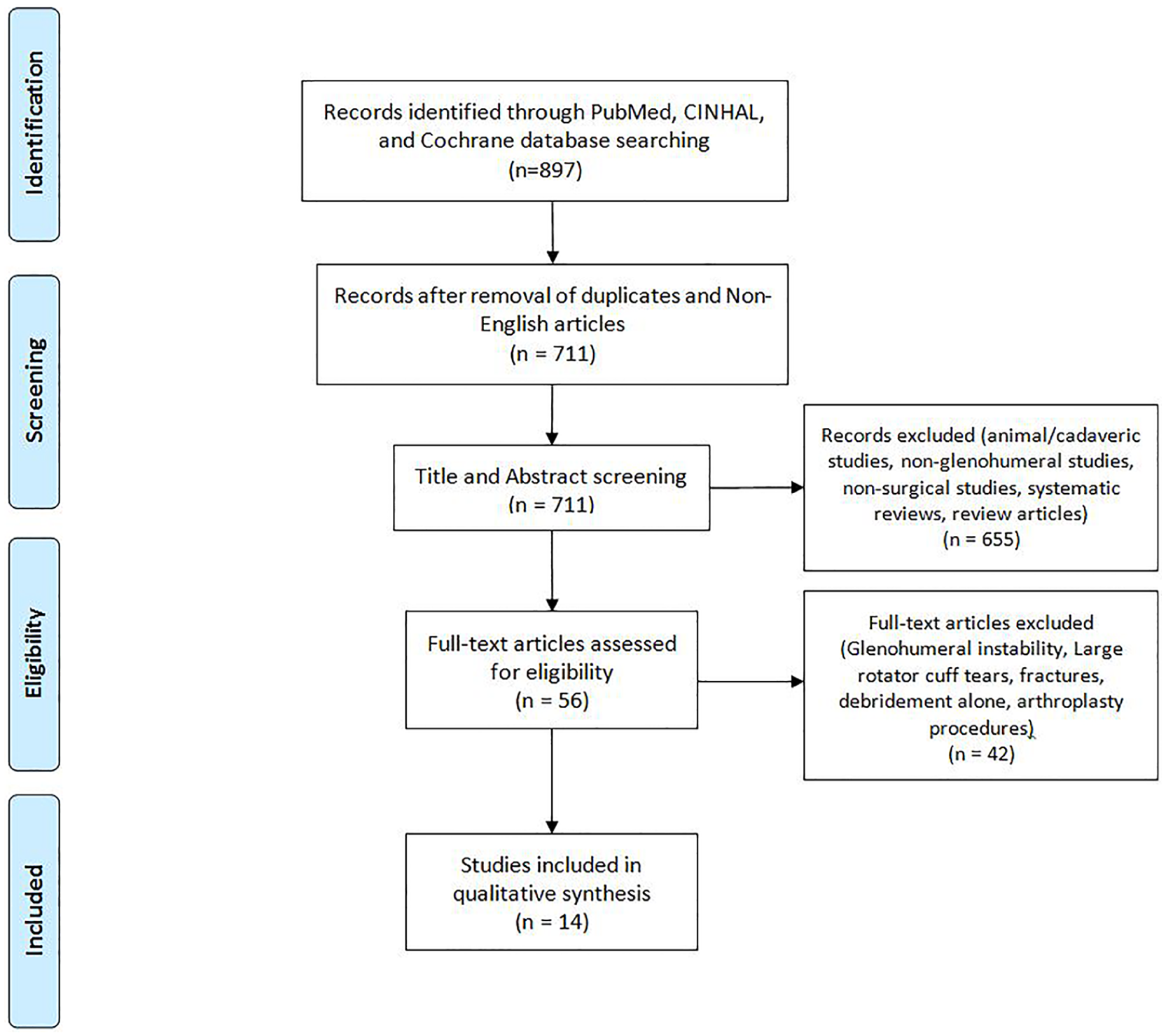
Flow diagram of the literature performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines. Fourteen studies were identified for inclusion. CINAHL = Cumulative Index for Nursing and Allied Health Literature.
Selection Criteria
Titles and abstracts of the 711 articles were reviewed by two independent authors (DPL and CBD), with only studies eliminated in consensus removed from the list. Any disagreements were resolved by discussion and consensus between reviewers and the senior author (CLC). Records that were excluded during title and abstract screening included animal or cadaveric studies, nonglenohumeral studies, nonsurgical studies, systematic reviews, and review articles ( Fig. 1 ). Following this process, 56 full texts remained and were manually reviewed for inclusion. Inclusion criteria were as follows: chondral defects of the humeral head, glenoid, or both, which had been treated with microfracture, fixation, OCA, OAT, or ACI. Exclusion criteria included debridement alone, shoulder arthroplasty, a clearly stated surgical indication for lesions due to glenohumeral instability, large rotator cuff tears, fractures, infection, or systemic inflammatory disease with involvement of the glenohumeral joint. If it could not be delineated which patients had procedures due to instability, the entire article was excluded. After the review, 14 studies were ultimately included in this systematic review ( Fig. 1 ).
Quality Assessment
There were not any randomized controlled trials or comparative studies found in the search. As a result, each study was assessed using the Methodological Index for Non-Randomized Studies (MINORS) scoring system. 16 MINORS is a validated tool designed for assessing the quality of non-randomized surgical studies. The maximum score is 16 points (8-item checklist scored from 0-2) for noncomparative studies and 24 points (12 item checklist scored from 0 to 2) for comparative studies, where higher scores represent a lower level of bias. Each study was scored independently by 2 reviewers (DPL and CBD) with any disagreements resolved in a consensus discussion with the senior author (CLC) when necessary. All MINORS score results are displayed in Table 1 and have been converted to percentages. Level of evidence was determined according to the Oxford Centre for Evidence-Based Medicine.
Data Extraction and Analysis
Studies were reviewed and the extracted data included study properties (year, level of evidence, number of patients), patient demographics (age, sex, lesion size, lesion location, and follow-up), surgical details, outcomes (patient reported, functional, clinical, and imaging), complications, failures, and reoperations. In one study, only data from patients who met inclusion criteria were reported and analyzed as a subset of patients who had a history of glenohumeral instability ( Table 1 ). Patient-reported outcomes were reported only when found in 3 or more studies. Due to a lack of comparative studies, inclusion of case reports, and the resulting heterogeneity of reported outcomes, data were not pooled and was instead reported as ranges. Additionally, when ranges or standard deviations for patient-reported outcomes were available in individual studies, they were reported as a measure of dispersion. Since the outcome measures were not pooled and reported as weighted averages in a meta-analysis, subjective analysis was performed instead. All data were analyzed using JMP Pro software (2018; version 14.1.0, SAS Institute Inc., Cary, NC). Figures were created using JMP Pro.
Results
Study Characteristics
Characteristics of the 14 studies meeting all inclusion criteria can be found in
Table 1
.1-6,17-24 There were 6 retrospective case series, 7 case reports, and 1 prospective case series. This resulted in a total of 100 shoulders in 98 patients. Microfracture alone was performed in 62 shoulders, OCA in 23, microfracture with periosteal flap in 5, OAT in 5, autologous chondrocyte transplantation (ACT) with collagen membrane seeding in 4, and internal fixation with poly-
Demographics of Included Studies (n = 14).
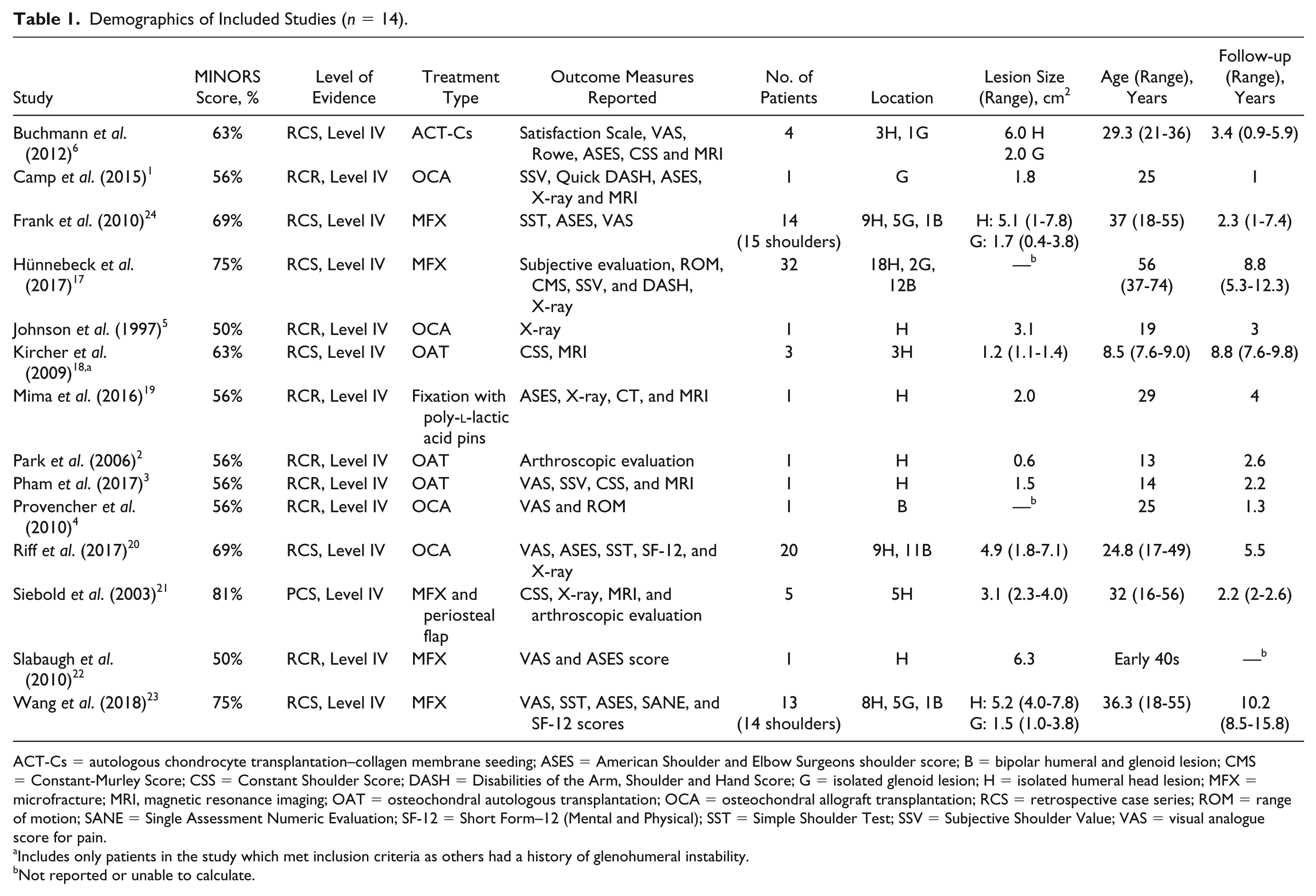
ACT-Cs = autologous chondrocyte transplantation–collagen membrane seeding; ASES = American Shoulder and Elbow Surgeons shoulder score; B = bipolar humeral and glenoid lesion; CMS = Constant-Murley Score; CSS = Constant Shoulder Score; DASH = Disabilities of the Arm, Shoulder and Hand Score; G = isolated glenoid lesion; H = isolated humeral head lesion; MFX = microfracture; MRI, magnetic resonance imaging; OAT = osteochondral autologous transplantation; OCA = osteochondral allograft transplantation; RCS = retrospective case series; ROM = range of motion; SANE = Single Assessment Numeric Evaluation; SF-12 = Short Form–12 (Mental and Physical); SST = Simple Shoulder Test; SSV = Subjective Shoulder Value; VAS = visual analogue score for pain.
Includes only patients in the study which met inclusion criteria as others had a history of glenohumeral instability.
Not reported or unable to calculate.
Imaging and Second-Look Arthroscopy
Eight studies reported radiographic outcomes, 6 reported MRI outcomes, and 2 performed second-look arthroscopy ( Table 2 ). Radiographic graft incorporation and restoration of articular surfaces ranged from 90% to 100% (5 studies). Specifically, Riff et al. 20 demonstrated graft incorporation in 90% (18/20) of patients treated with OCA to the humeral head at an average of 14.8 months. Six studies reported MRI outcomes with graft integration ranging from 75% to 100%. The rate of progression of Samilson grade 25 of osteoarthritis (OA) ranged from 57% to 100% (3 studies). Hünnebeck et al 17 reported progression of OA in 57% (12/23) patients, occurring significantly more in patients with preoperative OA (P = 0.01).
Reported Patient Outcomes.
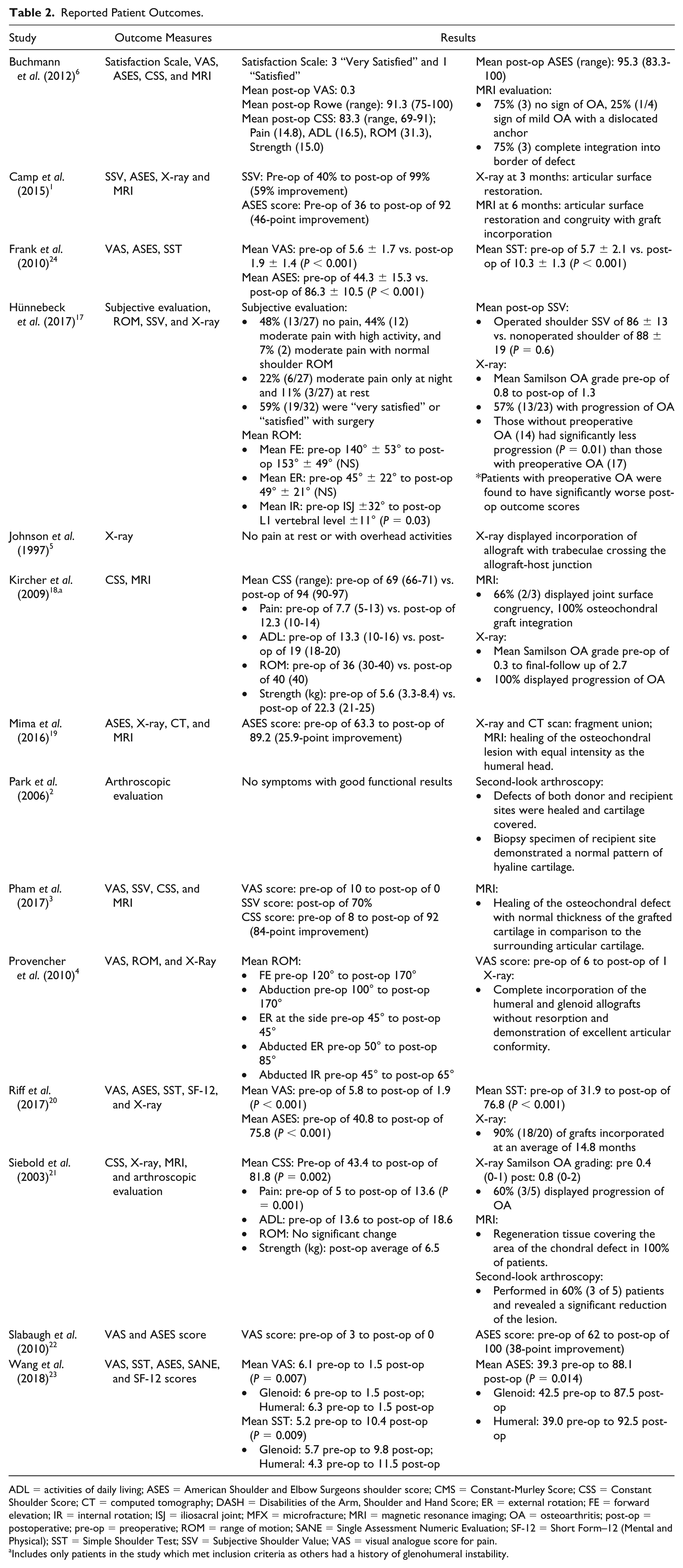
ADL = activities of daily living; ASES = American Shoulder and Elbow Surgeons shoulder score; CMS = Constant-Murley Score; CSS = Constant Shoulder Score; CT = computed tomography; DASH = Disabilities of the Arm, Shoulder and Hand Score; ER = external rotation; FE = forward elevation; IR = internal rotation; ISJ = iliosacral joint; MFX = microfracture; MRI = magnetic resonance imaging; OA = osteoarthritis; post-op = postoperative; pre-op = preoperative; ROM = range of motion; SANE = Single Assessment Numeric Evaluation; SF-12 = Short Form–12 (Mental and Physical); SST = Simple Shoulder Test; SSV = Subjective Shoulder Value; VAS = visual analogue score for pain.
Includes only patients in the study which met inclusion criteria as others had a history of glenohumeral instability.
Patient-Reported Outcomes
Patient-reported postoperative outcomes were described heterogeneously across all studies with no consistent outcome measures reported ( Table 2 ). The most commonly utilized outcomes were: visual analogue scale for pain 26 in 7 studies, American Shoulder and Elbow Surgeons (ASES) 27 questionnaire in 6 studies, Constant Shoulder Score (CSS) 28 in 4 studies, Subjective Shoulder Value (SSV) 29 in 3 studies, and Simple Shoulder Test (SST) 30 in 3 studies.
Mean postoperative VAS scores ranged from 0 to 1.9 across 7 studies, with all 3 retrospective case series reporting statistically significant pre- to postoperative improvement (P < 0.05).20,23,24 ( Fig. 2 ). Of 7 studies reporting ASES scores, the mean postoperative range was 75.8 to 100 ( Fig. 3 ). In the 6 studies reporting preoperative scores, the mean improvement ranged from 25.9 to 48.8 with 3 series reporting statistically significant improvement at final follow-up (P < 0.05).20,23,24 Mean CSS scores were reported in 4 studies and ranged from 81.8 to 94. Mean postoperative SSV scores were available in 3 studies and ranged from 70% to 99%.
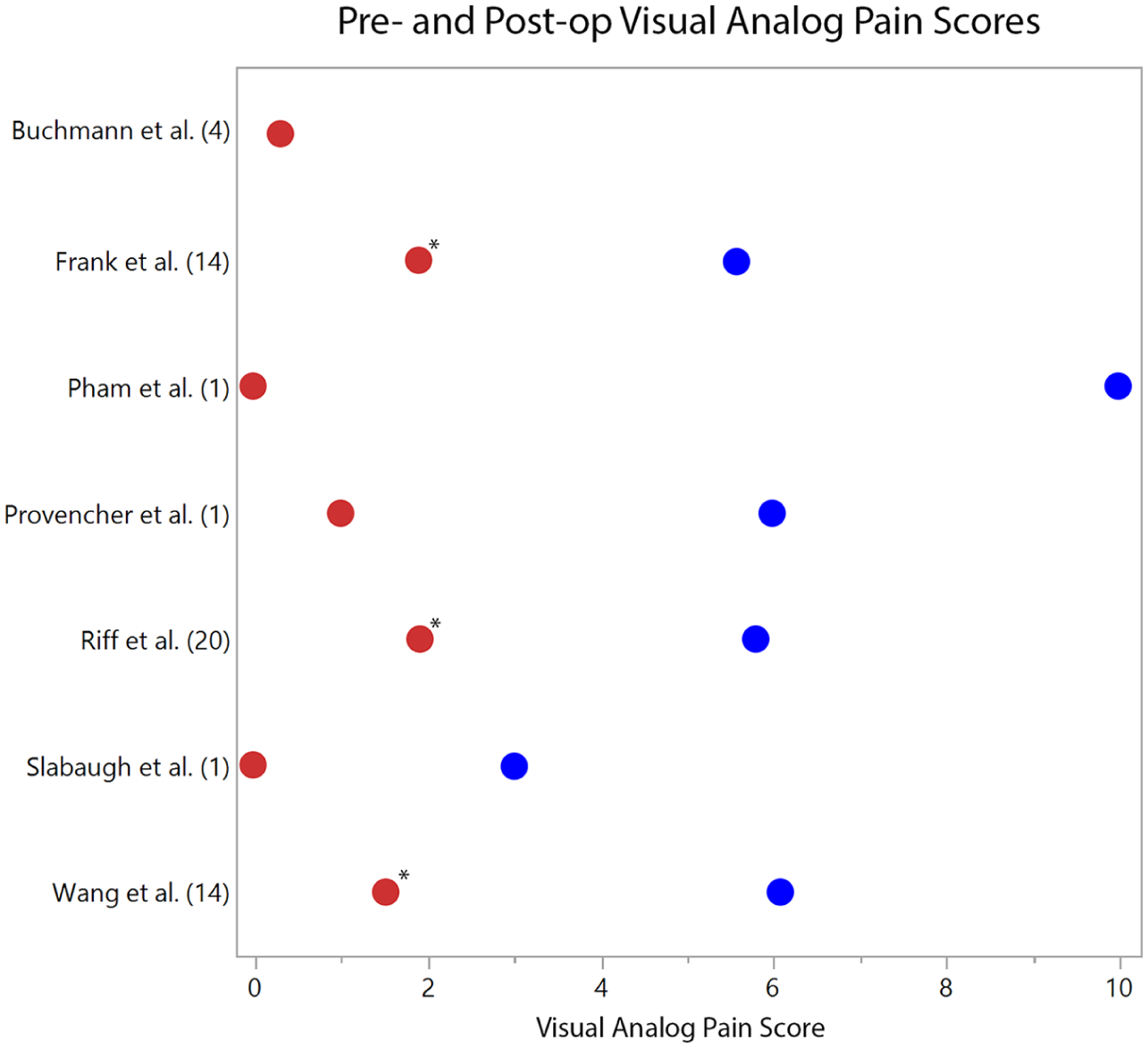
Pre- (blue dots) and postoperative (red dots) visual analogue scale (VAS) pain scores on a scale of 0 to 10, with 0 being no pain and 10 being the most. The respective studies are listed with their cohort size (n). *Statistically significant improvement in VAS scores (P < 0.05) is denoted when provided by the study.
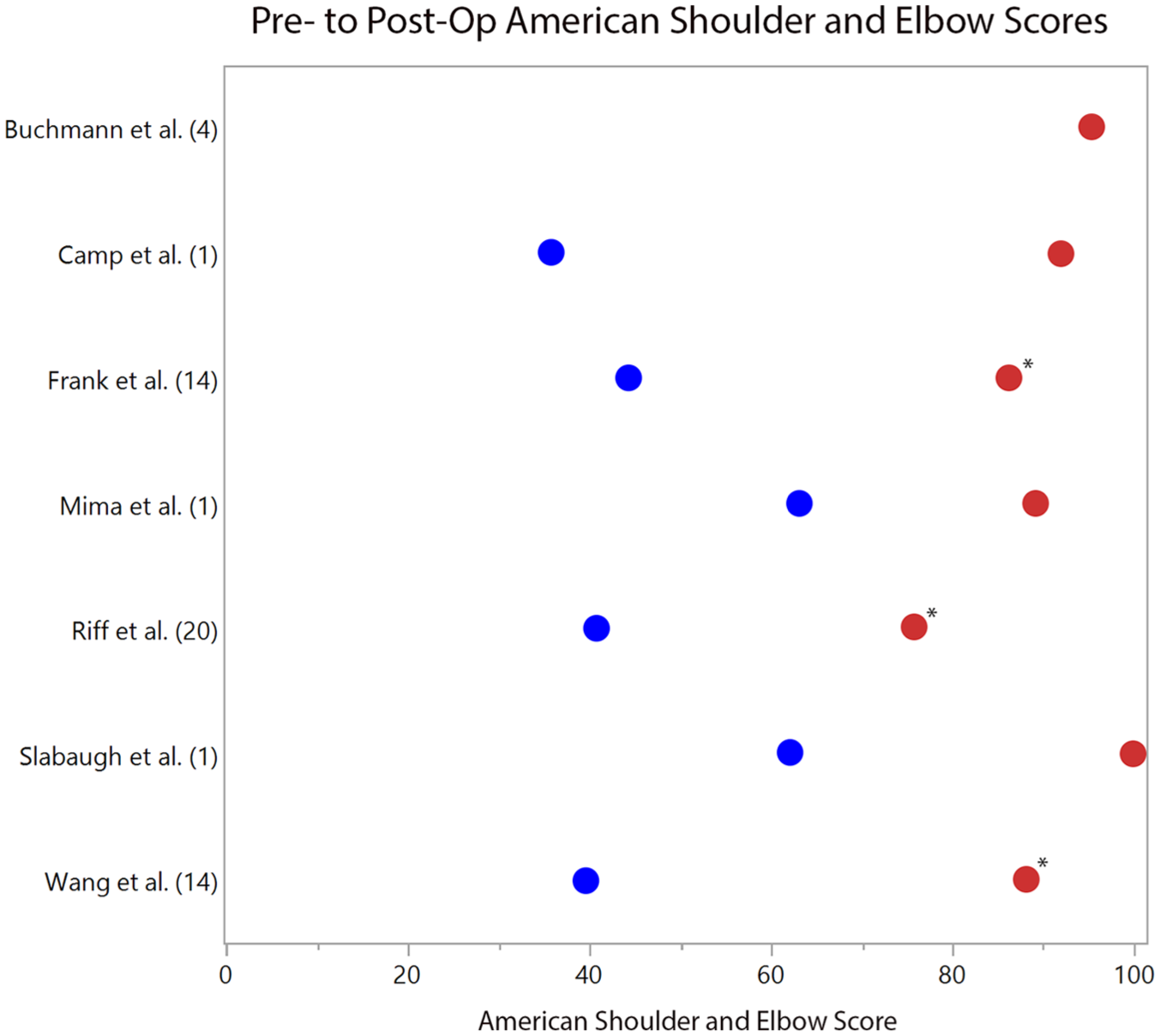
Pre- (blue dots) and postoperative (red dots) American Shoulder and Elbow Surgeons (ASES) questionnaire scores. The respective studies are listed with their cohort size (n). *Statistically significant improvement in ASES scores (P < 0.05) is denoted when provided by the study.
The largest study meeting inclusion reported additional subjective patient outcomes on 32 patients. Hünnebeck et al. 17 reported no difference for overall Constant Murley Scores 28 (CMS) between the operative and nonoperative shoulder, with mean scores of 74 ± 26 versus 75 ± 28 (P = 0.5), respectively. Fifty-nine percent (19/32) were “satisfied” or “very satisfied” with their surgical outcomes, with 48% (13/27) reporting no pain, and 44% (12/27) reporting moderate pain only while performing high-level activity.
Complications, Reoperations, and Failures
Similar to the outcomes reported among included studies, complications, reoperations, and failures were reported heterogeneously ( Table 3 ). Complications were rare, as only 1 patient experienced a transient postoperative brachial plexopathy with return of normal strength and function at 6-month follow-up. 1 The other 13 studies reported no complications in the perioperative period.2-6,17-24 The overall rate of failure and/or reoperation ranged from 0% to 35% and 0% to 30%, respectively6,17,20,23,24 ( Table 3 ). Of note, patients who required reoperation and patients who would choose not to undergo the initial procedure again were considered failures. The most common reoperation was conversion to prosthetic arthroplasty, occurring at a mean follow-up of 47 months, 17 25 months, 20 and 2.5 months. 23
Surgical Details, Complications, and Failures.
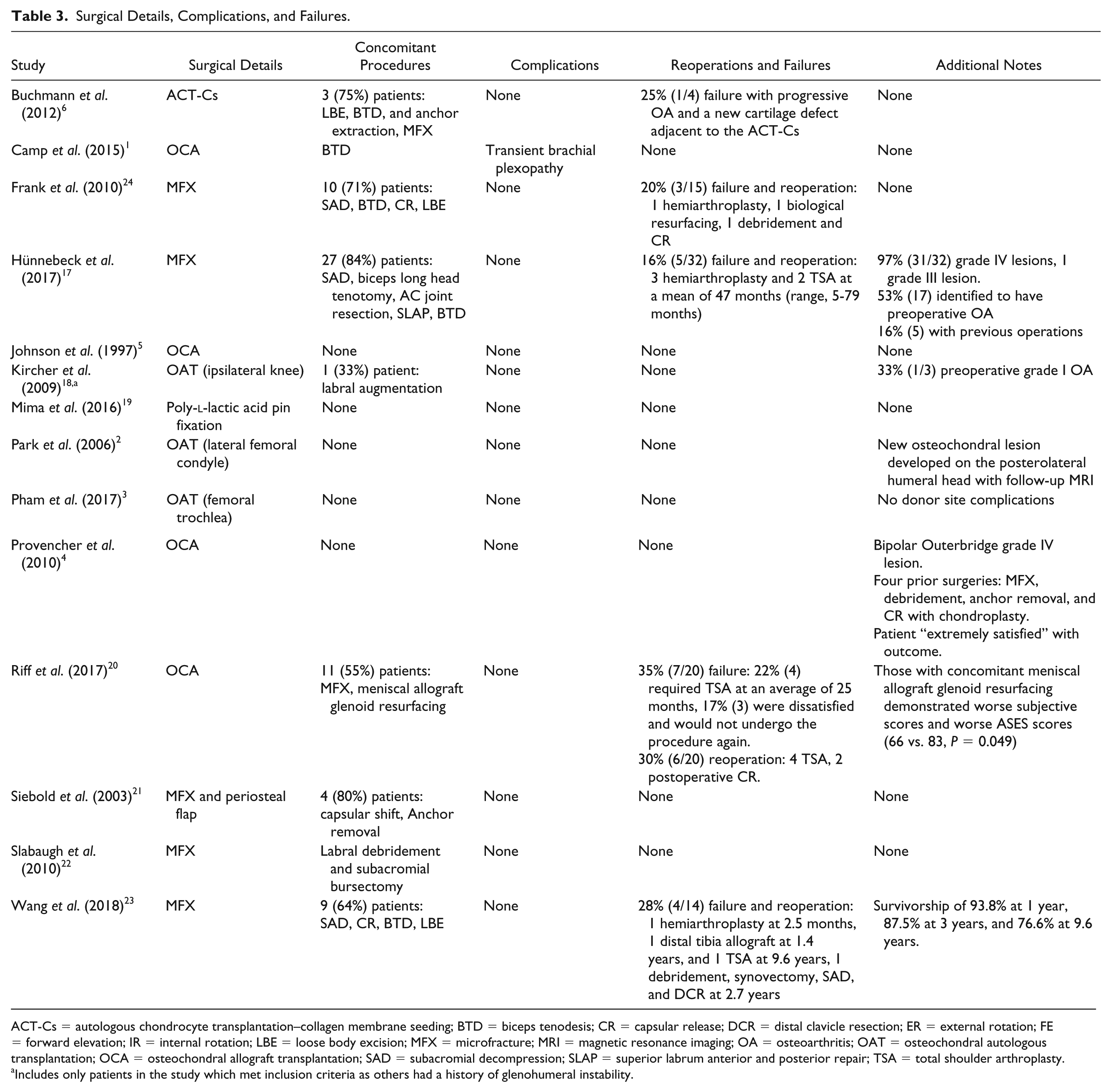
ACT-Cs = autologous chondrocyte transplantation–collagen membrane seeding; BTD = biceps tenodesis; CR = capsular release; DCR = distal clavicle resection; ER = external rotation; FE = forward elevation; IR = internal rotation; LBE = loose body excision; MFX = microfracture; MRI = magnetic resonance imaging; OA = osteoarthritis; OAT = osteochondral autologous transplantation; OCA = osteochondral allograft transplantation; SAD = subacromial decompression; SLAP = superior labrum anterior and posterior repair; TSA = total shoulder arthroplasty.
Includes only patients in the study which met inclusion criteria as others had a history of glenohumeral instability.
Discussion
Osteochondral defects of the glenohumeral joint occur secondary to a number of etiologies and present a management challenge in young and highly active patients. Prosthetic arthroplasty has been well described as a treatment option for advanced cartilage defects involving the glenohumeral joint for older patients; however, for younger and more active patients, literature is limited regarding outcomes following non-arthroplasty surgical management. The current systematic review demonstrates rates of radiographic union and progression of OA to range between 90% to 100% and 57%-100%, respectively, across 8 studies. Postoperative VAS improved to a range of 0 to 1.9 (7 studies), mean ASES scores improved to 75.8 to 100 (7 studies), mean CSS scores improved to 83.3 to 94 (3 studies), and mean SSV improved to 70% to 99% (3 studies).
Overall, this systematic review found high rates of radiographic graft incorporation and restoration of articular surfaces; ranging from 90% to 100% (5 studies). Six studies reporting MRI outcomes revealed graft integration ranging from 75% to 100%.
In spite of high healing rates, progression of Samilson osteoarthritis grade ranging from 57% to 100% (3 studies). One study revealed no sign of osteoarthritis in 75% of patients with progression of osteoarthritis in the remaining 25%. Radiographic and MRI evaluation in this series demonstrates high rates of healing without significantly preventing progression and development of glenohumeral osteoarthritis. To our knowledge, no studies have evaluated outcomes of non-arthroplasty management with respect to radiographic healing, graft incorporation, and progression to OA.
This review also demonstrated improved patient reported outcomes (VAS, ASES, CSS, and SSV scores) following nonarthroplasty surgical management of glenohumeral cartilage lesions. With several studies reporting statistically significant improvements, these results suggest patients experience improved pain and function. It has been established that patients of younger age undergoing shoulder arthroplasty have higher rates of prosthetic loosening and failure, thus suggesting the need for joint preserving options. 14 Several studies in current literature have also provided similar short-term results of pain relief and improved function; however, results are generally temporary and patients with features of advanced disease experience lesser postoperative improvement and high probability for conversion to shoulder arthroplasty.31-35 Van Thiel et al. 34 published a retrospective series of 71 patients undergoing arthroscopic debridement in patients with glenohumeral OA. Patients reported subjective pain relief in 77% (55/71) at a mean of 2.25 years postoperatively. Patients in this cohort with ongoing pain and progressing to shoulder arthroplasty exhibited higher grade of preoperative arthritis scores, joint space narrowing, and large osteophyte formation.
In this systematic review, the rate of complications was extremely low, occurring in only one patient who was treated with OAT. The complication was a brachial plexopathy and it ultimately resolved without further treatment. Reoperations ranged from 0% to 30% and failures ranged from 0% to 35%. A prospective study of 9,410 patients undergoing shoulder arthroscopy also reported a very low complication rate of 0.99%. 36 Similar to studies evaluating nonarthroplasty management of glenohumeral cartilage lesions, the most common reoperation remains conversion to prosthetic shoulder arthroplasty, occurring at a mean of 2.5 to 47 months (4 studies) in this review. Mitchell et al. 37 reported a series of 49 shoulders with a mean age of 52 years undergoing arthroscopic management of glenohumeral cartilage loss. In that study, 26% of patients progressed to total shoulder arthroplasty at a mean of 2.6 years. Skelly et al. 38 reviewed 33 patients, with an average age of 55.2 years, who underwent arthroscopic debridement and capsular release. Fourteen patients (42.4%) progressed to shoulder arthroplasty at a mean of 8.8 months. While also considering the patient reported outcomes following nonarthroplasty surgical management of glenohumeral cartilage lesions, the literature suggests joint preserving techniques to be viable options to prolong the function of the native shoulder and provide short- to midterm pain relief without significantly decreasing the progression of osteoarthritis. Despite evidence of healing and attempted joint preservation, many patients experience progression of OA to the point of needing reoperation, most often in the form of conversion to prosthetic arthroplasty. Additional studies are needed to further investigate nonarthroplasty surgical treatment options to delineate which techniques provide the most beneficial long-term outcomes in young and active patients.
Limitations
The results of this systematic review should be interpreted in the context of several limitations. First, there is no consensus as to the best management of glenohumeral cartilage lesions in young and highly active patients. Therefore, the majority of studies included were level IV case reports or retrospective case series with relatively small patient cohorts. Second, the included studies also generally lack randomization, blinding, and comparative control groups. Third, the outcome measures were inconsistent across the 14 included studies, allowing for a source of bias while making it difficult to draw meaningful conclusions. 39 When attempting to explore the causes of heterogeneity of included studies, no significant correlations were found between the type of surgical intervention pursued, glenohumeral cartilage defect size or location, level of evidence, patient age, or follow up timelines. Fourth, the exclusion criteria may have eliminated pertinent data that could have altered conclusions, specifically studies evaluating glenohumeral cartilage defects as a result of joint instability. Fifth, various surgical treatment options were employed to address lesions and resulting follow-up timelines varied. Several of the nonarthroplasty treatment options utilized in this review resulted in small cohorts of patients. There is certainly surgeon selection bias in terms of management strategies, which further contributes to the heterogeneity of the data. Finally, this review only includes published data with reported outcomes and may therefore have publication bias.
Conclusions
There are numerous joint-preserving surgical options for the treatment of osteochondral lesions involving the glenohumeral joint in young and highly active patients without a clear consensus as to which approach provides the best outcomes. In this systematic review, nonarthroplasty surgical techniques demonstrated acceptable rates of radiographic healing, improved patient-reported outcomes, minimal complications, and low rates of failure or reoperation. The rate of arthritis progression, however, was high. Joint preserving techniques are likely viable options to prolong function of the native shoulder and provide short- to midterm pain relief.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Aaron J. Krych discloses the following: Aesculap/B. Braun: research support; American Journal of Sports Medicine: editorial or governing board; Arthrex, Inc.: IP royalties; paid consultant; Arthritis Foundation: research support; Ceterix: research support; Histogenics: research support; International Cartilage Repair Society: board or committee member; International Society of Arthroscopy, Knee Surgery, and Orthopaedic Sports Medicine: board or committee member; Minnesota Orthopedic Society: board or committee member; Musculoskeletal Transplantation Foundation: board or committee member; Vericel: paid consultant; Open Payments Database: general payments from Arthrex Inc., Musculoskeletal Transplant Foundation, Ceterix; Orthopedics, Inc., Gemini Medical LLC, and Gemini Mountain Medical. Jonathan D. Barlow discloses the following: Stryker: paid consultant; CDC Medical: education fees; Arthrex Inc.: travel and lodging, food and beverage. Diane L. Dahm discloses the following: American Orthopaedic Society for Sports Medicine: board or committee member; Arthrex Inc.: research support; GE Healthcare: travel and Lodging; NBA/GE Strategic Advisory Board: board or committee member; spouse owns stock in Tenex Health, Inc. and Sonex Health, LLC: stock or stock options; spouse receives royalties from Tenex Health, Inc. and Sonex Health, LLC: IP royalties. Christopher L. Camp discloses the following: Arthrex Inc.: travel and lodging. The other authors have nothing to disclose.