
Abstract
Objective
The objective of this study was to identify and describe the existing literature on criteria used for return to play (RTP) following surgical management of osteochondral defects of the knee.
Design
A systematic review was performed to evaluate the surgical management of osteochondral defects of the knee in skeletally mature patients with a minimum of 2-year follow-up using Level I to IV studies in PubMed EMBASE from January 1998 to January 2016.
Results
Twelve studies with at least one explicitly stated criterion for RTP were identified from a review of 253 published articles. The majority of included studies were Levels II and IV (33%, respectively). Autologous chondrocyte implantation (ACI) was exclusively evaluated in 33.3% of papers and 16.7% evaluated osteochondral allograft transplantation (OCA). Eight different RTP criteria were used alone or in combination across the reviewed studies and time was the most often utilized criterion (83.3%). Minimum time to RTP ranged from 3 to 18 months.
Conclusions
This systematic review identifies current criteria used in the available literature to dictate RTP. Time from surgery was the most commonly employed criterion across the reviewed studies. Given the complex biological processes inherent to the healing of cartilaginous defects, further research is needed to design more comprehensive guidelines for RTP that are patient-centered and utilize multiple functional and psychological domains relevant to the process of returning to sport.
Keywords
Introduction
Articular cartilage is crucial for normal function of the knee joint. The spectrum of articular cartilage pathology ranges from single focal defects to diffuse degenerative disease. Knee arthroscopy is one of the most common orthopedic surgeries performed in the United States and chondral defects have been found in approximately 60% of these patients.1,2 An increase in sports participation among children, adolescents, and young adults is likely contributing to the prevalence of these injuries. 3 Unfortunately, articular cartilage has poor healing capacity due to its limited regenerative capacity, avascularity, and surrounding synovial environment.3,4 Surgical treatment is indicated for symptomatic chondral lesions with the hope of preventing further degenerative changes and potentially preventing the development of osteoarthritis.
Currently, surgical options for symptomatic focal cartilage lesions include a simple debridement, microfracture (MFX), osteochondral autograft transfer (OAT), osteochondral allograft transplantation (OCA), and autologous chondrocyte implantation (ACI). Microfracture, subchondral bone drilling that stimulates underlying bone marrow and produces a fibrocartilage layer of repair tissue, was made popular in the 1990s and was considered first-line treatment for these defects at this time.5,6 However, larger lesions have shown poorer outcomes and thus, its use is steadily decreasing. 7 OATs, on the other hand, is a technique in which the defect is restored with the patient’s own hyaline cartilage. However, postoperative success is based on the integration of a subchondral bony plug. 8 Although success has been shown in small to mid-size defects to minimize donor site morbidity, not all patients are candidates for this procedure. Good-to-excellent results were shown in 92% of femoral lesions, 87% of tibial lesions, and 79% of patellofemoral lesions. 9 More recently, OCA has gained popularity with the increase in availability of allograft materials. One study investigating the outcomes of this strategy in osteochondritis dissecans showed good or excellent results in greater than 70% of patients. 10 Finally, ACI, a 2-stage, cell-based technique, continues to evolve. The theoretical benefit of this procedure is growth of hyaline-like cartilage, which allows for favorable longer-term outcomes. 4 Current data shows promising results: the majority of these strategies may allow for higher incidence of return to play (RTP) and everyday activity in the young, active population.11-16 However, overall RTP determinations still remain dependent on the inherent physiological process related to chondral healing and level of activity.
Therefore, the aim of the present study is to identify and describe the existing literature regarding RTP following surgery for articular cartilage defects of the knee. It is hypothesized that most of the presently available literature uses time-based criteria to dictate RTP, return to sport, or return to unrestricted activity rather than imaging or performance-based criteria.
Methods
A systematic review of Level I to IV studies of patients undergoing surgical management of osteochondral defects of the knee was conducted. PubMed and EMBASE were queried for the terms autologous chondrocyte implantation, open osteochondral allograft, open osteochondral autograft, arthroscopic osteochondral autograft (e.g., mosaicplasty), arthroscopic osteochondral allograft (e.g., mosaicplasty), arthroscopic abrasion arthroplasty including chondroplasty where necessary, articular cartilage defects of the knee, rehabilitation, surgical management of articular cartilage defects of the knee, return to sport, return to unrestricted activity, return to full/ unlimited activity and return to play from January 1998 to January 2016. The aforementioned period was selected to ensure inclusion of more modern and established techniques in cartilage restoration procedures. Return to play was defined as any return to sporting activity. In addition, RTP was characterized as when patients were allowed to return to active participation in any sports or work-related activity without restrictions. As such, equivalent terms such as return to play, return to sport, return to restricted activity, and return to full/unlimited activity were included in our query to represent a full return to unrestricted postoperative activity.
Inclusion criteria consisted of (1) English language articles; (2) a population of adult, skeletally mature patients with a mean age of 18 years or greater; (3) patients with osteochondral defects; (4) patients undergoing a cartilage restoration or surgical intervention, and (5) patients with a minimum of 2-year follow-up. Articles focused on skeletally mature patients were selected to focus on RTP information following surgical procedures as nonoperative management remains the treatment of choice in patients with open physes. 17 Studies without RTP criteria, review articles, biomechanical, technique articles, those with follow-up less than 2 years, those related to arthroplasty procedures, revision or concomitant procedures, and studies on nonoperative management were excluded. The authors included both open and arthroscopic, as well as autograft and allograft procedures to encompass and capture as much RTP criteria as possible. Specific procedures included in the study are listed in Table 2 . Any study in which the mean patient age at the time of surgery was less than 18 years was excluded to only encompass management of osteochondral defects in a skeletally mature population. In total, 32 studies were excluded for lacking explicit RTP criteria ( Fig. 1 ).
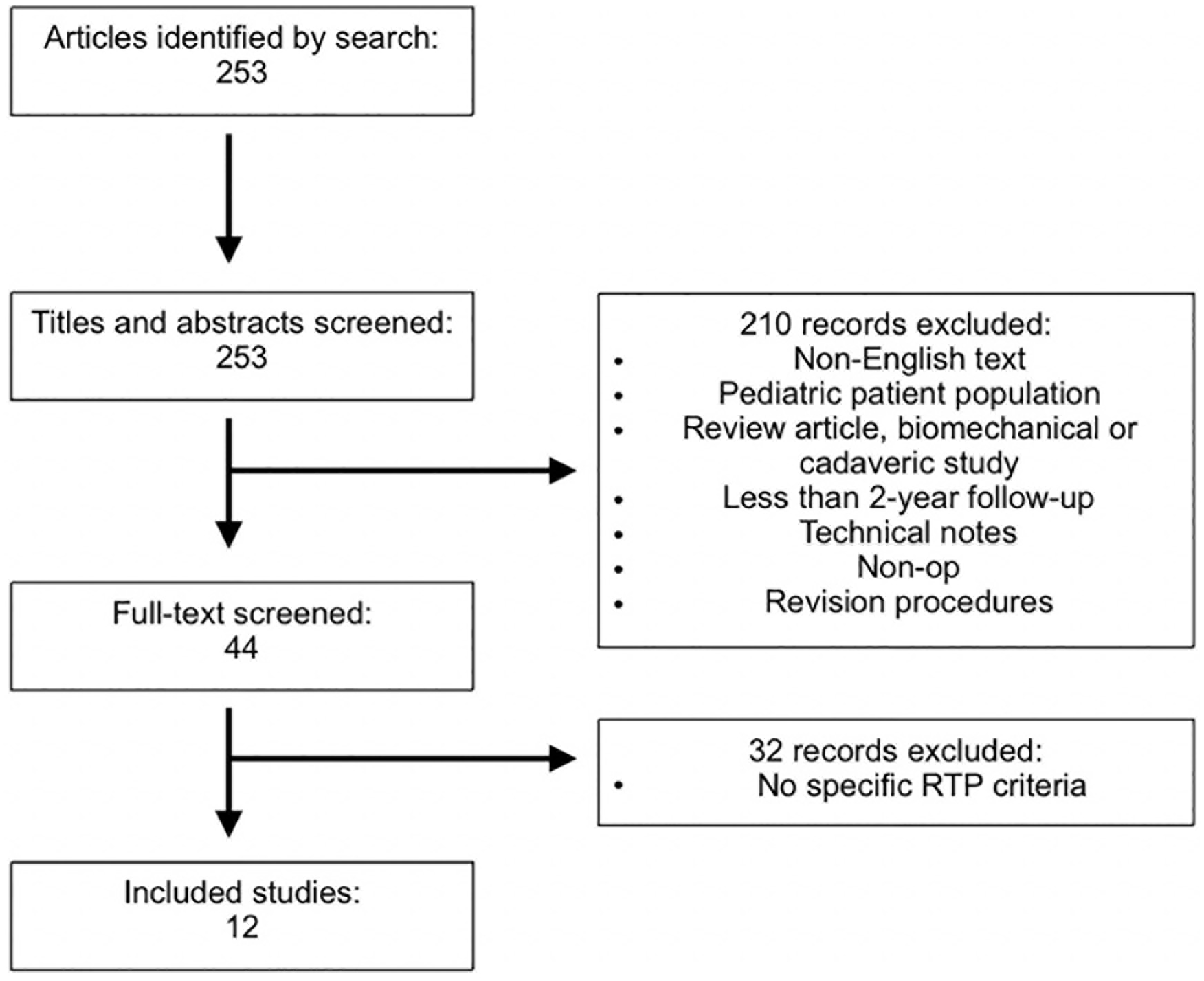
PRISMA diagram depicting inclusion and exclusion criteria for analyzed studies. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; RTP = return to play.
All selected studies were reviewed separately by 2 authors, and any further relevant studies were compiled from the individual reference sections. The methods section of each article was further analyzed by the senior author. Studies that met all criteria were ultimately selected and data were subsequently collected and compiled from each. Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) criteria was utilized. 18 The primary outcome of interest was the criteria used to determine when patients were able to RTP. Further information on specifics or details related to RTP was also documented. In addition, journal of publication, demographic data, level of evidence, procedures performed, and rates of RTP were also identified and recorded. Lastly, statistical analysis was performed with descriptive statistics. Weighted means were calculated and the number and proportion of studies including specific RTP criteria were determined. The rate of return to previous level of sport by primary procedure was determined across the studies and reported as a range. The heterogeneity of the included studies prevented a formal meta-analysis.
Results
Study Identification
A total of 253 articles were initially identified. In the initial screening process, 210 articles were excluded for the following reasons: non-English articles, pediatric patient population, review article, technical note, biomechanical or cadaveric study, less than 2 years of follow-up, focused on nonoperative modalities, or revision procedures. The full text of the remaining 44 articles was reviewed for eligibility. Thirty-two articles were excluded due to the lack of specific RTP criteria, which left a total of 12 studies for inclusion. This process is highlighted in a PRISMA diagram ( Fig. 1 ). Three studies were Level I evidence, 4 were Level II, 1 was Level III, and the remaining 4 studies were Level IV evidence.
Demographics and Procedures
There were a total of 743 patients across the 12 included studies. Eleven of the 12 studies included an average age of 34.0 years (range, 14–64). The minimum follow-up period in these studies was 18 months, with an average follow-up of 39.4 months when weighted by number of patients per study (Table 1). In regard to procedures, 33.3% (4/12) of papers exclusively evaluated ACI and 16.7% (2/12) exclusively evaluated osteochondral allograft transplantation (OCA). One paper each (8.3%) evaluated microfracture and osteochondral autograft transfer systems (OATS). Four comparative studies were included in which 25% (3/12) involved comparisons with microfracture and the remaining study compared ACI with OATS procedures. Specific to ACI, there was an equal distribution of articles evaluating first- and second-generation ACI procedures with 4 articles each (Table 1).
Individual Study Data with Procedure Studied, Demographic Data, and Return to Play Criteria.
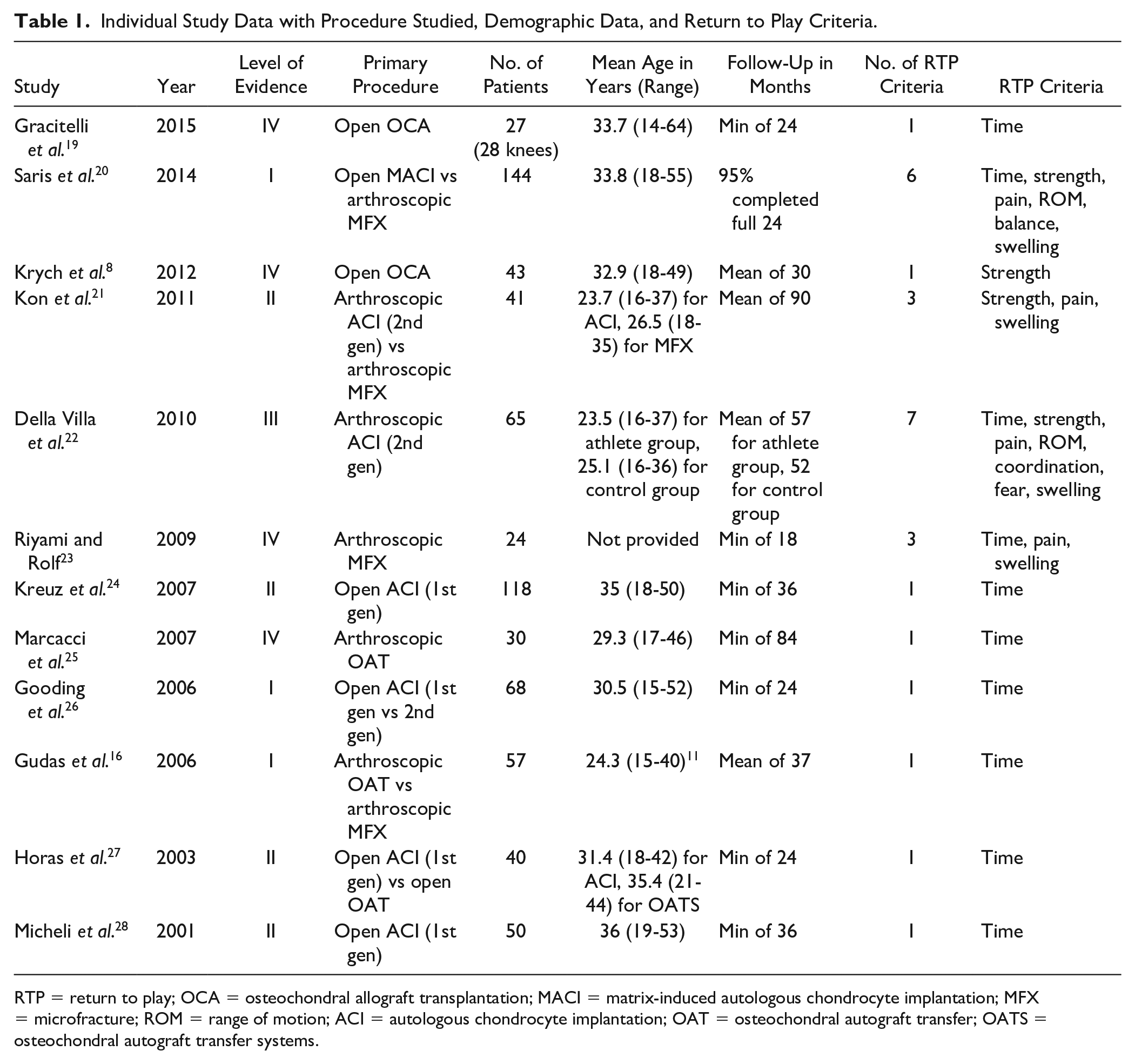
RTP = return to play; OCA = osteochondral allograft transplantation; MACI = matrix-induced autologous chondrocyte implantation; MFX = microfracture; ROM = range of motion; ACI = autologous chondrocyte implantation; OAT = osteochondral autograft transfer; OATS = osteochondral autograft transfer systems.
Return to Play Criteria
In order to be included in this analysis, each study needed to contain at least 1 explicitly stated RTP criteria. Time was the most often commonly used RTP criterion, utilized in 83.3% (10 of 12) of the studies. Seven studies (58.3%) used time as the only criterion. Additional criteria mentioned included pain (4 studies; 33.3%), strength (4 studies; 33.3%), range of motion (ROM) (2 studies; 16.7%), balance (1 study; 8.3%), coordination (1 study; 8.3%), absence of swelling (4 studies; 33.3%%), and fear of reinjury (1 study; 8.3%). These criteria are listed in Table 2 .
Combinations of Return to Play Criteria in the Literature.
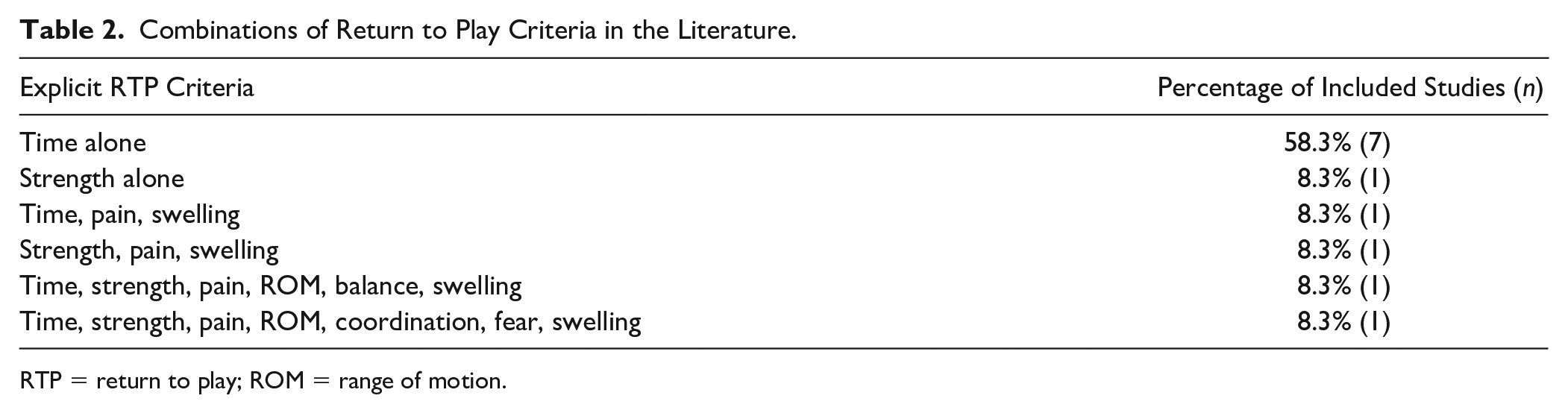
RTP = return to play; ROM = range of motion.
Time
Ten studies reported a required period of time before an RTP decision was considered. There was no consensus on minimum time before RTP, but 4 months (3 studies) and 6 months (4 studies) were the most widely indicated minimum time until RTP. Four studies made specific distinctions on time to return to sport in terms of the level of activity, with Gracitelli et al. 19 requiring a return to “high-loading” activities between 6 and 12 months after open OCA, Saris et al. 20 recommending 12 to 18 months until a return to “high-impact sports” after in a comparative study of open matrix-induced autologous chondrocyte implantation compared with arthroscopic microfracture, 12 months until contact sports in Kreuz et al.’s 24 investigation of first-generation open ACI, and Micheli et al. 28 recommending 12 months until returning to “high-level” sports after first-generation open ACI ( Table 3 ).
Reported Return to Play Times for Each Included Study.
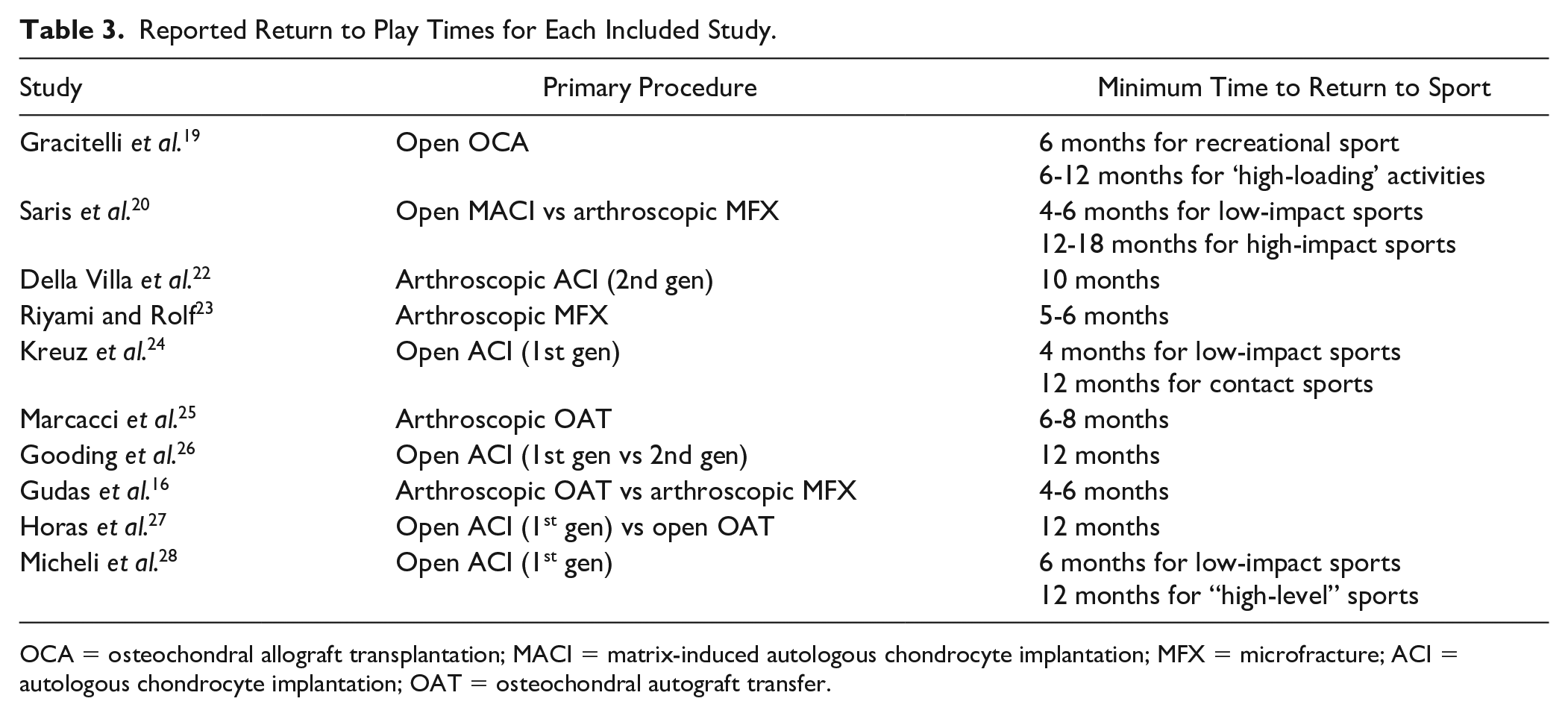
OCA = osteochondral allograft transplantation; MACI = matrix-induced autologous chondrocyte implantation; MFX = microfracture; ACI = autologous chondrocyte implantation; OAT = osteochondral autograft transfer.
Pain and Swelling
No study noted the presence of pain as a primary criterion for consideration of RTP. Furthermore, no study specifically noted a measurement tool used to assess level of pain. The absence of swelling was factored into the RTP decision in 4 articles ranging from a lack of swelling or an effusion at rest in 2 studies20,23 and when performing sport-specific drills or exercises in the remaining 2 studies.21,22
Strength
Strength was the sole criterion for RTP in one study, yet this factor was included as part of the algorithm for RTP in 3 other articles. One article required postoperative quadricep and hamstring strength to reach a level that was “80-90% of the contralateral leg” 20 before RTP was considered. Other studies permitted RTP after a “return of lower extremity strength,” 8 “complete endurance recovery” when compared with the uninjured extremity, 21 and isokinetic testing with quadriceps and hamstring strength of at least 80% of the maximal peak torque when compared with the contralateral leg. 22
Range of Motion
Two articles mention ROM as an RTP criterion. One article noted full passive and active ROM as a requirement 20 while the other required full ROM specifically when patients performed pre-assigned rehabilitation exercises. 22
Other Criteria
There were a few criteria that were only listed by single studies. Saris et al. 20 listed balance as a criterion, requiring 75% to 80% of balance on the injured leg when compared with the contralateral extremity. Della Villa et al. 22 listed “the ability to perform exercises with good coordination” and the absence of any “fear of reinjury” as criteria for their patients before RTP. No specific instruments were used to evaluate coordination or balance in either study.
Return to Play Rates
A total of 7 (58.3%) of the studies provided patient RTP rates while 10 studies (83.3%) provided minimum recovery periods before RTP was permitted. First-generation ACI procedures were found to have the highest RTP rates (100%) 24 among the reviewed articles while arthroscopic MFX yielded the lowest rate with a reported 52% RTP. 16 The remainder of RTP rates are listed in Table 4 .
Rate of Return to Previous Level of Sport by Primary Procedure.
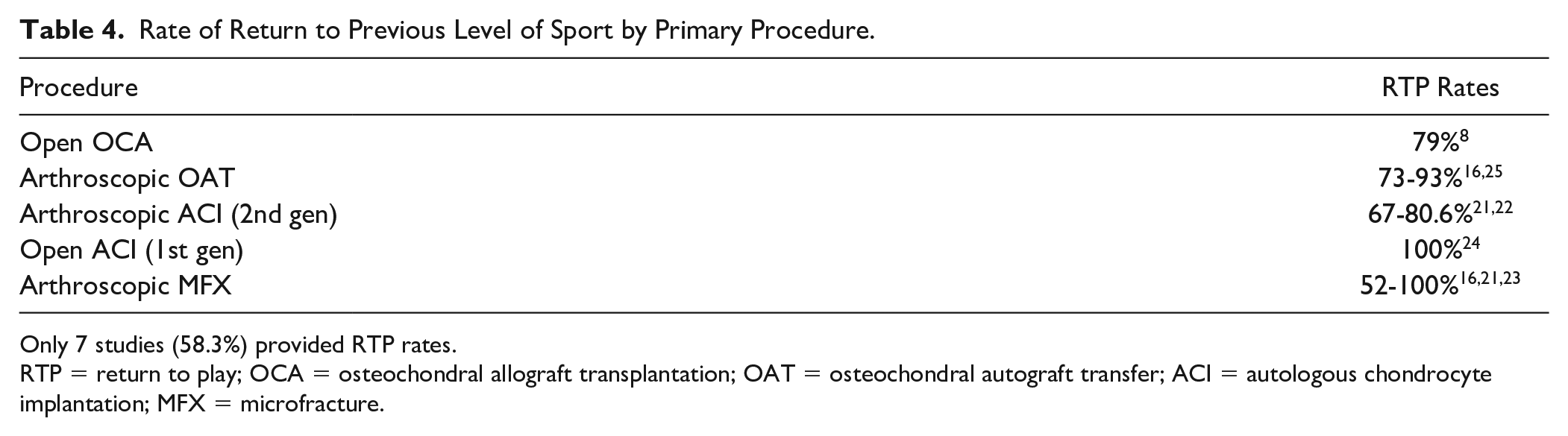
Only 7 studies (58.3%) provided RTP rates.
RTP = return to play; OCA = osteochondral allograft transplantation; OAT = osteochondral autograft transfer; ACI = autologous chondrocyte implantation; MFX = microfracture.
Discussion
The present study provides a comprehensive analysis of RTP criteria following surgical management of osteochondral lesions of the knee. Across the 12 studies included in this review, 8 different RTP criteria were used either alone or in combination. Time was the most often utilized criterion (83.3%) and was the only criterion explicitly reported in over half of the studies (58.3%). However, there was significant variation between studies in terms of minimum time to RTP, with a range of 3 to 18 months. Other RTP criteria included strength (33.3%), pain (33.3%), swelling (33.3%), ROM (16.7%), balance (8.3%), coordination (8.3%), and fear of reinjury (8.3%). Six different RTP combinations were employed, but none reached consensus.
The observed variability in minimum time to RTP was at least in part the result of including several different surgical procedures in this study. Previous research has demonstrated several differences in average missed time following the various operative techniques for osteochondral lesions of the knee. For instance, within current literature, average time to RTP ranges from 8 to 10 months after microfracture,21,29,30 and 12 to 18 months following ACI.21,22,31 Meanwhile, RTP time following OCA and OAT are similar, with an average time of 10 months 8 and 7 to 9 months,32,33 respectively. While the overall aim of operative management of an osteochondral lesion of the knee is similar regardless of surgical technique, namely, to fill the defect and restore the articular surface, the underlying biological repair process varies by procedure. Microfracture relies on the development of a fibrocartilage layer from bone marrow stimulation, 5 ACI uses cultured chondrocytes to produce a hyaline-like cartilage over the defect,5,6 and both OCA and OAT provide an immediately functioning articular surface dependent on subchondral bony integration. 8 These differences have important implications for rehabilitation as the recovery timeline following any surgical procedure must be consistent with the involved physiology. 34 As such, the observed variability in minimum RTP between procedure types is somewhat expected. Interestingly, however, 4 of the studies that used time as a RTP criterion compared different surgical procedures but none described different RTP timelines by procedure.16,20,26,27 In addition, there was notable variability in RTP timelines between different studies of the same surgical procedure. For instance, minimum RTP time after first-generation open ACI, using an autologous periosteum flap to maintain the position of the autologous cell suspension, varied from 12 weeks to 12 months.24,26-28
Numerous studies have used a variety of modalities (e.g., histology, biochemical analysis, radiographic and magnetic resonance imaging (MRI), second-look arthroscopy, and clinical examination) to describe the healing process after surgical management of osteochondral lesions in both humans and animal models.35-38 Based on the findings of such investigations, clinicians have developed recovery timelines for the various surgical procedures. For instance, return to high-impact sports following ACI is often delayed for 12 to 18 months, based on the observation that graft remodeling occurs past 18 months.22,24,38,39 However, translating the results of such studies into clinical practice is not always straightforward and rehabilitation protocols remain largely based on expert opinion. Disagreement persists on even the most basic components, such as when to initiate weight-bearing and ROM restrictions. 40 Minimal and optimal recovery periods prior to RTP consideration are even less well-defined. Only recently have studies sought to critically evaluate established rehabilitation protocols based on clinical outcomes and patient-reported outcome measures. For instance, Della Villa et al. 22 found that an accelerated, aggressive rehabilitation protocol in patients undergoing second-generation ACI for osteochondral lesions of the knee actually allowed for earlier RTP (mean 10.6 months) without sacrificing clinical outcomes at 5-year follow-up.
While time from surgery offers some benefit in establishing a starting point for RTP consideration, it should not be the only consideration. Rather, time should be incorporated into a more comprehensive RTP checklist that includes both functional and psychological domains, as has occurred with RTP following anterior cruciate ligament (ACL) reconstruction. 41 The recovery process after surgical management of an osteochondral defect of the knee is dependent on numerous factors (e.g., lesion size and location, procedure, patient motivation, sport, level of play), with significant variation from patient to patient. As such, the rehabilitation process should be personalized for each patient, and the overall timeline for RTP should be adjusted, as necessary, based on objective and subjective feedback. Progression through the rehabilitation process and eventual RTP should be criterion-based rather than purely time-based. 22 Several studies in this review utilized different rehabilitation timelines for low-impact and high-impact sports,19,20,24,28 but this consideration alone is not sufficient.
Only a third of the studies in this review used a functional criterion to guide RTP. Strength, pain, and swelling were utilized most frequently (33%), followed by ROM (16.6%), balance (8.3%), and coordination (8.3%). In terms of strength, 2 studies utilized a specific threshold that needed to be achieved relative to the contralateral leg (80%-90% for quadriceps and hamstring)20,22 while 2 studies employed more generic endpoints such as “return of lower extremity strength” 8 and “complete endurance recovery.” 21 However, no explanations were provided as to the derivations or clinical justifications of these strength thresholds. Four studies stated that patients had to be pain free before RTP,20,21-23 2 of which specified no pain during exercise or sport-specific drills.21,22 Similarly, 4 studies noted that knee swelling or effusion precluded RTP consideration.20,21-23 Two studies described full knee ROM as an explicit RTP criterion, though definitions of “full” were not provided. It should be noted that several studies required full ROM early in the rehabilitation period before advancing to subsequent stages. Achieving full knee ROM, particularly terminal extension, is important for quadriceps function 34 and has been correlated with patient satisfaction, limiting functional limitations in sport activities, and preventing the development of osteoarthritis in patients undergoing ACL reconstruction. 42 Saris et al. 20 required balance to be 75% to 80% of the contralateral leg, though details regarding the specific method of measuring balance and the justification for this cutoff value were not provided. Lastly, Della Villa noted that athletes had to be “able to perform exercises with good coordination” prior to RTP, although a specific value or objective measure of coordination was not provided. 22
Within our review, only one study considered an athletes’ psychological state when determining readiness for RTP. Specifically, this study required patients to perform exercises without fear of reinjury before they were cleared for a return to sport. 22 The importance of psychological readiness prior to RTP has received considerable attention in ACL literature after Kvist et al. 43 first identified fear of reinjury as a significant factor in patients who did not return to pre-injury level of activity after ACL reconstruction. A subsequent meta-analysis found that fear of reinjury was the most commonly cited reason for a postoperative reduction in, or cessation of, sports participation after ACL reconstruction. 44 Burland et al. 45 recently found the decision to return to sport after ACL reconstruction was largely dependent on psychosocial factors, such as hesitancy, lack of self-confidence, fear of reinjury, and changes in priorities or personal expectations. Although not routinely used, several scoring systems have been developed to assess a patient’s psychological state after ACL reconstruction including the Tampa Scale for Kinesiophobia (TSK),43,46,47 the ACL Return to Sport After Injury (ACL-RSI) scale, 48 and the Knee Osteoarthritis Outcomes Scale (KOOS). 49 Webster et al. 48 cited fear of reinjury as a reason to restrict RTP after ACL reconstruction. Similar to ACL ruptures, osteochondral injuries of the knee are often the result of a traumatic event in up to 62.5% of cases with the potential for long-lasting psychological effects that hinder successful RTP.8,20,22,23,26,27 Despite these associations with ACL injuries in terms of the lasting psychological effects, little data or measurement instruments exist to quantify or evaluate the psychological impact of cartilaginous injuries.
While many studies employed routine radiography and MRI to monitor healing,11,16,19,20,23-25 no study used imaging as an explicit component of the RTP decision-making process. Among professional soccer and rugby players undergoing MFX, Riyami and Rolf 23 prohibited impact activities involving pivoting until signs of healing were apparent on MRI. However, 37.5% of players were allowed to RTP by 6 months despite MRI revealing incomplete healing in the majority of these patients. All players were back to full competition by 18 months, but only 62.5% of patients had complete healing on MRI as defined by a modified version of the Henderson MRI classification for cartilage healing. 50 Maximum improvement of MRI score was observed between 6 and 12 months, and a high degree of correlation was observed between function and healing on MRI throughout the entire study period (r2 = 0.993 at 18 months). 23 Similarly, Kreuz et al. 24 noted improvement in Henderson classification scores up to 36 months after first-generation ACI, though RTP was permitted as early as 4 months after surgery. A recent meta-analysis, however, questions the utility of using MRI to predict clinical outcomes after articular cartilage repair of the knee, noting that only 28% of the included studies found a correlation between clinical outcome measures and the composite magnetic resonance observation of cartilage repair tissue (MOCART) or Henderson score. 51 In summary, while imaging may be utilized as a noninvasive method of monitoring healing following surgical repair of an osteochondral lesion, its utility in determining optimal timing of RTP remains largely unknown given the observed variability in radiographic changes and the controversial relationship between radiographic findings and clinical outcomes.
Second-look arthroscopy is considered by some to be the gold standard for assessing healing after surgical repair of an osteochondral defect of the knee.23,51 While several studies in this review utilized repeat arthroscopy at various time points postoperatively, none required second-look arthroscopy prior to RTP.16,20,23,26,27 At the request of team medical personnel, Riyami and Rolf 23 performed second-look arthroscopy in 10 professional soccer and rugby players at a mean of 5.8 months after MFX to ensure lesion healing prior to RTP, but this was not a component of the authors’ standard RTP protocol. If the repaired tissue felt soft, players were advised to proceed with an additional period of rehabilitation. Interestingly, knee function, as measured by modified Cincinnati subjective and objective functional scores, correlated better with International Cartilage Repair Society (ICRS) scores on second-look arthroscopy findings, than modified Henderson MRI scores. 23 Conversely, Gudas et al. 11 noted no significant difference in Tegner activity level scores at 10-year follow-up between patients with low (grades 1-2) versus high (grade 3) ICRS scores measured at a mean of 12.4 months after OAT and MFX. While second-look arthroscopy may provide valuable information, it cannot be relied upon to guide RTP given the potential for complications, added morbidity, and increased costs associated with an additional procedure. 23
This study has several limitations that warrant further discussion. First, multiple surgical techniques were included given the limited number of studies that address RTP considerations. Similarly, there was significant heterogeneity between studies in terms of osteochondral lesion size and location (e.g., patella, medial and lateral femoral condyles, trochlea), incidence of previous surgery, concomitant procedures performed, and patient characteristics such as sport-participation and overall activity level. Furthermore, discrepancies likely exist between the explicit RTP criteria reported in the included studies and the actual RTP decision-making process occurring on a patient-by-patient basis. Allowing an athlete to RTP after a surgical procedure is often a multifaceted process that relies on a combination of objective and subjective outcomes, the clinical judgment of the surgeon, therapist, and athletic trainer, as well as the patient’s motivation and objectives. As such, the descriptions of the RTP protocols in the included studies likely oversimplify this complex process. In addition, several studies employed multistage recovery protocols with specific milestones that had to be reached before advancing to a subsequent stage. Since such milestones occurred earlier in the recovery process prior to considerations of RTP, they were not considered RTP criteria in this study. For instance, Kon et al. 21 and Della Villa et al. 22 employed a 4-stage rehabilitation program that required patients to run for 15 minutes without pain or swelling in order to advance to stage 3. Marcacci et al. 25 required full ROM, good strength, and no effusion or pain for progression through the rehabilitation protocol, but only time was listed as an explicit RTP criterion. However, while some components of this process are difficult to standardize, the overall lack of attention devoted to clearly describing RTP criteria constitutes a significant limitation of the cartilage restoration literature as it precludes comparisons between studies and hinders the development of a comprehensive, evidence-based RTP protocol.
Conclusions
This systematic review identifies current criteria used in the available literature to dictate RTP. Time from surgery was the most commonly employed criterion across the reviewed studies. Given the complex biological processes inherent to the healing of cartilaginous defects, further research is needed to design more comprehensive guidelines for RTP that are patient-centered and utilize multiple functional and psychological domains relevant to the process of returning to sport.
Footnotes
Authors’ Note
Investigation performed at Columbia University Irving Medical Center, New York, NY 10032.
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
No ethical approval needed for the present study.