
Abstract
Objectives. The purpose of this study was to examine whether patients with diagnosed hypertension have an increased risk of graft failure following cartilage repair with either autologous chondrocyte implantation (ACI) or osteochondral allograft transplantation (OCA). We hypothesized that hypertension is related to higher ACI and OCA graft failure. Design. Patients who underwent ACI or OCA transplantation between February 2009 and December 2016 were included in this study. Inclusion criteria were (1) at least 2 years’ follow-up, (2) available information related to the living habits (smoking and medication status), and (3) available information related to the presence of hypertension, diabetes mellitus, or hyperlipidemia. To identify potential independent risk factors of graft failure, univariate screening was performed and factors with significance at a level of P < 0.1 were entered in multivariate logistic regression models. Results. A total of 368 patients (209 ACI and 159 OCA) were included into our study. In the ACI group, 61 patients’ (29.1%) graft failed. Univariate screening identified older age, female gender, defect size, higher prevalence of hypertension, and smoking as a predictor of graft failure. Following, multivariate logistic regression revealed female gender (odds ratio [OR] 1.02, P = 0.048), defect size (OR 1.07, P = 0.035), and hypertension (OR 3.73, P = 0.023) as significant independent risk factors predicting graft failure after ACI. In the OCA group, 29 patients’ (18.2%) graft failed and none of the included factors demonstrated to be a potential risk factor for graft failure. Conclusion. Hypertension, defect size, and female gender seem to predict ACI graft failure but not OCA failure.
Keywords
Introduction
Osteoarthritis (OA) is a severe joint disease and is currently the sixth leading cause of disability worldwide. Symptomatic OA can be a major cause of restricted activity, disability, and low quality of life resulting from gradual deterioration and inflammation of the articular cartilages. 1 Recently, a potential link between OA and metabolic syndrome has been revealed that led to the suggestion of a new classification for phenotyping OA that includes metabolic syndrome, aging, and posttrauma-related OA.2,3 Metabolic syndrome includes a number of conditions, including obesity, atherogenic dyslipidemia, impaired fasting glucose, and hypertension. 4 Metabolic OA is considered to be a subtype of OA, the second most frequent after aging. 5 This subtype targets the middle-aged population (between 45 and 65 years) 2 and these patients show faster development and progression of the disease, associated with increased pain. 6
Hypertension, a component of metabolic syndrome and an independent risk factor for cardiovascular and cerebrovascular disease, has been acknowledged as the third leading cause of disability worldwide.7,8 In 2005, the National Health and Nutrition Examination Survey reported that 65 million people in the United States suffered from hypertension.7,9 Moreover, Puenpatom et al. 6 reported, based on NHANES III data, that 59% of the population was suffering from metabolic syndrome along with OA. Hypertension (75%), abdominal obesity (63%), hyperglycemia (30%), elevated triglyceride (47%), and low HDL (44%) were the major metabolic syndromes associated with it. Furthermore, previous studies have suggested that hypertension, may be an independent risk factors for knee OA.10-12
Articular cartilage has a very limited healing potential, and once damage occurs, full recovery of its structure, function, and biomechanical properties is not expected, eventually progressing to OA.13-15 To delay or avoid this progression, the injured cartilage has to be restored. Various cartilage repair procedures can be utilized for such a purpose, depending on patient and lesion characteristics. Large full-thickness chondral and osteochondral defects are frequently treated with autologous chondrocyte implantation (ACI) and osteochondral allograft transplantation (OCA) resulting in high patient satisfaction and significantly improved functional outcomes.16-22 Despite low failure rates over a long-term follow-up, patients are at risk of graft failure and revision surgery.16-23 Consequently, tremendous effort is being placed on identifying factors that are prognostic in determining the success of the cartilage repair procedure.21,24-31 Age,26,27 gender, 27 body mass index (BMI), 28 number of previous surgeries, 27 duration of the symptoms,27,32 defect size, 28 defect location,29,30 and presence of OA 31 have been reported to have an effect on ACI success rate. Moreover, previous studies suggest that age, BMI, and previous surgeries are also associated with less favorable results in patients who underwent OCA transplantation.21,24,25 However, the effects of other comorbidities such as hypertension on cartilage repair procedures are yet to be determined.
Since patients with symptomatic cartilage defect have a high chance to develop OA, and hypertension appears to be an independent predictor of OA, we aimed to examine whether patients with hypertension have an increased risk of graft failure following cartilage repair with either ACI or OCA. It was hypothesized that hypertension is related to higher ACI and OCA graft failure.
Materials and Methods
Patient Population and Inclusion Criteria
Our institutional review board approved this study, and informed consent was obtained from all patients at the time they were entered into our institutional database. In this review of prospectively collected data, we analyzed data from patients who underwent ACI or OCA transplantation between February 2009 and December 2016 by a single surgeon. Participants were selected based on the following inclusion criteria: (1) at least 2 years of follow-up, (2) availability of information regarding smoking and medication status, and (3) availability of information related to the presence of comorbidities such as hypertension, diabetes mellitus, or dyslipidemia. Patients with less than 2 years of follow-up or with incomplete medical information were excluded from this study. The indication for treatment of cartilage defects with ACI or OCA were one or more full-thickness chondral or osteochondral defects of the knee with symptoms matching the defect location. Surgery was indicated in patients who were resistant to nonoperative therapy. Patients were evaluated through a physical examination, radiography, magnetic resonance imaging (MRI), and arthroscopic surgery before cartilage repair was considered. Contraindications to treatment included inflammatory joint disease, unresolved or recent septic arthritis, metabolic or crystal disorders, and established osteoarthritis (Kellgren-Lawrence III-IV). Tibiofemoral malalignment >3° from the neutral mechanical axis into the involved compartment was corrected with concomitant osteotomy. Patellofemoral maltracking was addressed with anteromedialization tibia tubercle osteotomy (TTO) 33 to centralize patellar tracking, and proximal soft tissue balancing (lateral release/lengthening, vastus medialis obliquus advancement, medial patellofemoral ligament reconstruction) as necessary to centralize the extensor mechanism. All procedures were performed by the senior author. Clinical notes were reviewed to determine patient specific factors such as (1) age in years, (2) BMI (kg/m2), (3) gender (female or male), (4) defect size (cm2), (5) concomitant high tibial osteotomy (HTO), (6) concomitant TTO or (7) distal femoral osteotomy (DFO), (8) concomitant meniscus allograft transplantation (MAT), (9) concomitant ligamentous repair/reconstruction, (10) hypertension, (11) dyslipidemia, (12) diabetes mellitus, and (13) smoking. Patients were considered having one or more comorbidities (hypertension, dyslipidemia, and diabetes mellitus) if they were diagnosed and regularly took medication for the specific condition. In this study, the effect of the aforementioned factors on ACI or OCA graft failure was investigated.
Definition of Graft Failure
Graft failure was defined as a surgical removal of more than 25% of the graft area; revision cartilage repair procedure of the treated defect, or prosthetic replacement. 34
Surgical Procedure
ACI Procedure
The details of the ACI procedure have been described previously in greater detail.35,36 Briefly, following concomitant procedures (if necessary), chondral defects were debrided back to healthy cartilage and intact subchondral bone; defect sizes were measured and templated. The senior author used a type I/III bilayer collagen membrane derived from porcine peritoneum and skin (Bio-Gide, Geistlich Pharma, Princeton, NJ). The membrane was then cut precisely to the template. Each membrane was positioned at the site of the defect and secured with multiple 6-0 Vicryl sutures (Ethicon, Somerville, NJ). The suture line was sealed to be watertight with fibrin glue and the defect was injected full with autologous chondrocytes. After February 2010, the technique was simplified, and the collagen membrane was seeded with autologous cultured chondrocytes in the operation room right before implantation. 37 The seeded membrane was placed on the cartilage defect and secured with resorbable suture and fibrin glue.
OCA Transplantation
OCA was performed as described in detail previously.38,39 Briefly, after induction of anesthesia, concomitant procedures were performed before OCA if necessary. Mini-parapatellar arthrotomy was performed to visualize the cartilage defect. Any degenerated cartilage as well as fibrous tissue were debrided. The defect was then sized with a sizing guide and an identical sized reamer was used to ream to a depth of approximately 6 to 8 mm using constant cold irrigation. The donor condyle was prepared using the same sizing guide. After harvesting the allograft plug, it was trimmed to the previously measured depth using a sagittal saw. The allograft was then pulse lavaged removing any remaining marrow elements to decrease immunogenicity. Finally, the graft was placed into the recipient site with manual pressure only, until it was flush circumferentially.
Postoperative Rehabilitation
Following ACI Procedure
Motion was emphasized in the first 6 weeks using continuous passive motion (CPM), active and isometric straight leg raises, stationary bike by 3 weeks, and with touchdown weightbearing. From 7 to 12 weeks, patients progressed from partial to full weightbearing. Functional activities were allowed from 4 months onward, including bicycle, treadmill, elliptical trainer, outdoor distance walking, hiking, and swimming. Jogging was allowed at 12 to 14 months if a normal knee exam and near normal MRI was present (minimal subchondral bone marrow edema and isotonic appearance of the ACI graft to the adjacent articular cartilage). Patients were restricted from inline impact activities (running) for 12 to 18 months and cutting sports were allowed after 18 months. The ACI rehabilitation protocol considered each patient’s individual surgical reconstruction, graft maturation, and previous activity level, which were reflected in individualized variations in the rehabilitation protocol. 40
Following OCA Procedure
Protected weightbearing was allowed with the knee in a brace for the first 4 to 6 weeks, followed by progression to full weightbearing as tolerated. During this period, patients were permitted to begin unrestricted range of motion exercises, quadriceps sets, straight-leg raises, and patellar mobilization. A stationary bicycle was permitted at 4 weeks. Open chain exercises were not permitted in this first phase. Strengthening was added at the 6-week point and was increased over the next 2 to 3 months. Patients progressed to sport-specific activities by 4 to 6 months after surgery for isolated OCA, and by 8 to 12 months for those undergoing concomitant procedures. 21
Statistical Analysis
SPSS (version 21.0; IBM Corp, Armonk, NY) was used to perform statistical analyses. Continuous variables were reported as mean ± standard deviation with minimum and maximum value, whereas categorical variables were reported as numbers and percentages. To identify potential risk factors of ACI or OCA failure, univariate analysis was utilized and those factors which showed significance at a level of P < 0.1 were entered in multivariate logistic regression models. Normal distribution was assessed by the Shapiro-Wilk test. Continuous data were compared with the independent-sample t test. Categorical data were compared with the chi-square test or the Fisher’s exact test, as appropriate. The results of the multivariate logistic regression analyses are presented as odds ratios (ORs) with accompanying 95% confidence intervals (CIs). Results were considered to be statistically significant when the null value (1.00) was absent from the CI or P < 0.05.
Results
A total of 446 patients underwent cartilage repair procedure with ACI or OCA between February 2009 and December 2016. Of these, 45 patients (10%) were excluded from this study due to incomplete data, and 33 patients (7.5%) were lost during the follow-up period. Hence, 368 patients (82.5%) met the inclusion criteria. Of these patients, 209 underwent ACI and 159 had OCA procedure with a slight female predominance (52.7%). The mean age at the time of surgery was 33.4 ± 9.7 years (range, 14-58 years) with a mean follow-up of 4.3 ± 2.4 years (range, 2-11.5 years). Baseline demographic and clinical characteristics of the ACI and OCA patients are demonstrated in Tables 1 and 2 , respectively.
Demographic Data of Patients Who Underwent Autologous Chondrocyte Implantation (ACI).
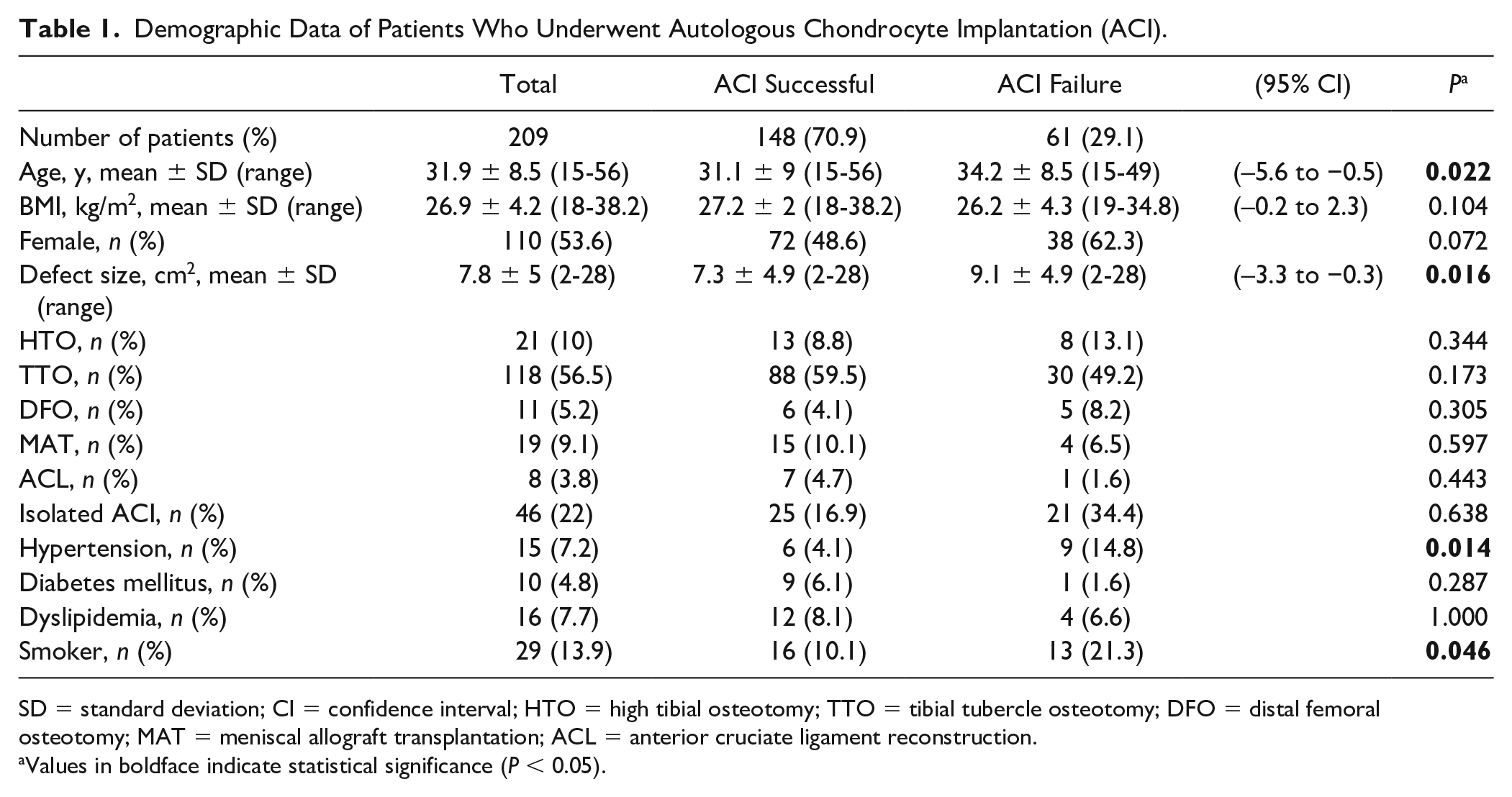
SD = standard deviation; CI = confidence interval; HTO = high tibial osteotomy; TTO = tibial tubercle osteotomy; DFO = distal femoral osteotomy; MAT = meniscal allograft transplantation; ACL = anterior cruciate ligament reconstruction.
Values in boldface indicate statistical significance (P < 0.05).
Demographics Data of Patients Who Underwent Osteochondral Allograft Transplantation (OCA).
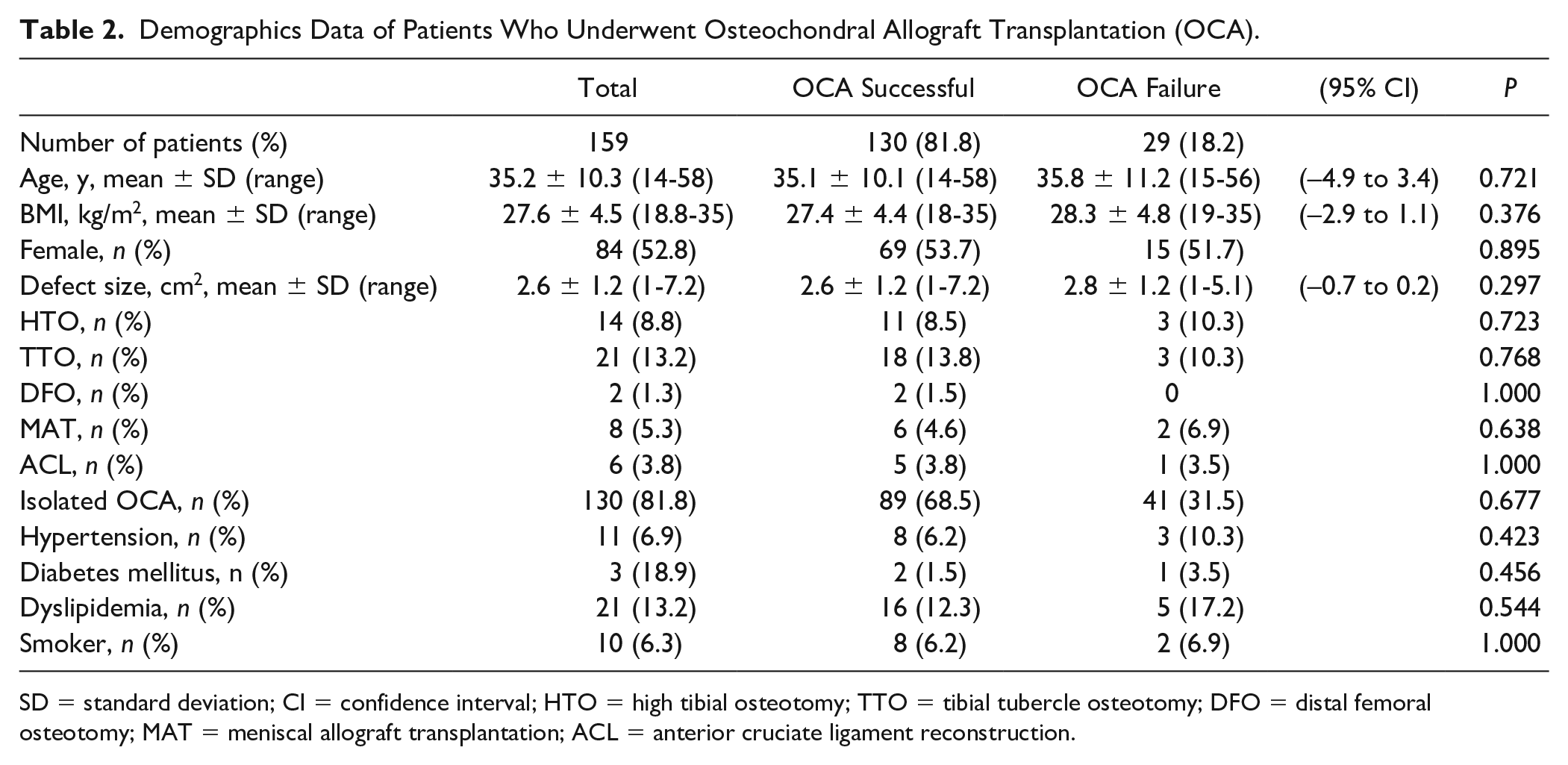
SD = standard deviation; CI = confidence interval; HTO = high tibial osteotomy; TTO = tibial tubercle osteotomy; DFO = distal femoral osteotomy; MAT = meniscal allograft transplantation; ACL = anterior cruciate ligament reconstruction.
From those patients who underwent ACI (n = 209), 61 patients’ (29.1%) graft failed. These patients were significantly older (P = 0.022) and had a larger defect size (P = 0.016) compared with those whose graft remained intact. Moreover, among those patients whose ACI graft failed, significantly more patients had hypertension (ACI failure 9 patients [16.4%] vs. ACI successful 6 patients [4.1%]; P = 0.007) and were smokers (ACI failure 13 patients [21.3%] vs. ACI successful 16 patients [10.1%]; P = 0.046) compared to patients with remaining graft integrity ( Table 1 ). On the other hand, there was no significant difference between the failure and successful groups in the number of concomitant surgeries: HTO (ACI failure 8 patients [13.1%] vs. ACI successful 13 patients [8.8%]; P = 0.344), TTO (ACI failure 30 patients [49.2%] vs. ACI successful 88 patients [59.5%]; P = 0.173), DFO (ACI failure 5 patients [8.2%] vs. ACI successful 6 patients [4.1%]; P = 0.305), MAT (ACI failure 4 patients [6.5%] vs. ACI successful 15 patients [10.1%]; P = 0.597), and ACL reconstruction (ACI failure 1 patient [1.6%] vs ACI successful 7 patients [4.7%]; P = 0.443). In addition, no significant difference was seen between the failure and successful groups in those patients who underwent ACI alone without any concomitant surgeries (isolated ACI; ACI failure 21 patients [34.4%] vs. ACI successful 25 patients [16.9%]; P = 0.638).
Consequently, multivariate logistic regression analysis was conducted including the 4 potential predictors (age, defect size, hypertension, and smoking), as well as female gender (P = 0.072) as it fulfilled the criteria for multivariate regression inclusion. Multivariate logistic regression revealed that female gender (OR 1.02, CI 1.01-3.64, P = 0.048), defect size (OR 1.07, CI 1.01-1.14, P = 0.035), and hypertension (OR 3.73, CI 1.20-11.6, P = 0.023) were significant independent risk factors predicting graft failure after ACI ( Table 3 ). Mean time to graft failure was 4.6 ± 3.0 years (range, 1-10.8 years). Among those patients whose ACI graft failed, 14 patients (23%) underwent chondroplasty, 38 patients (62.2%) had a revision cartilage repair procedure, and 9 patients (14.8%) underwent partial or total knee arthroplasty.
Multivariate Logistic Regression for Predicting Graft Failure Following Autologous Chondrocyte Implantation.
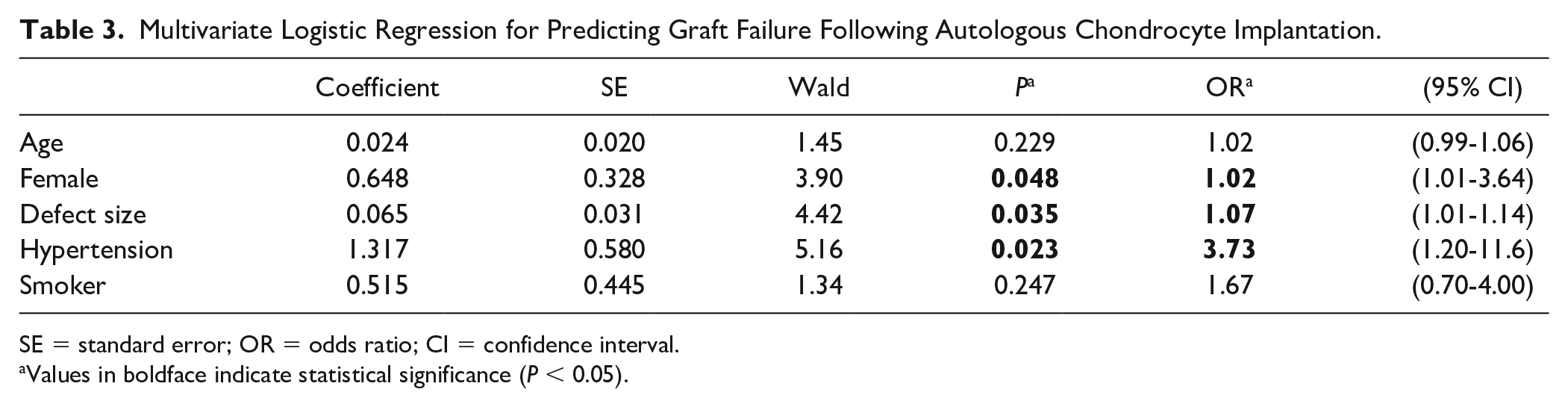
SE = standard error; OR = odds ratio; CI = confidence interval.
Values in boldface indicate statistical significance (P < 0.05).
Among those patients who underwent OCA transplantation (n = 159), 29 patients’ (18.2%) graft failed. Baseline demographics and clinical characteristics were similar between the failure and successful group ( Table 2 ). Consequently, multivariate logistic regression was not performed, as none of the factors demonstrated to be a potential significant risk factor for OCA graft failure. Mean time to graft failure was 2 ± 1.4 years (range 0.5-4.7 years). Among those patients whose OCA graft failed, 12 patients (41.4%) underwent chondroplasty, 15 patients (51.7) had a revision cartilage repair procedure, and 2 patients (6.9%) underwent partial or total knee arthroplasty.
Discussion
The purpose of the present study was to investigate whether patients with hypertension have an increased risk of graft failure following cartilage repair with either ACI or OCA. In this review of a prospectively collected data set, we analyzed 209 patients who underwent ACI and 159 patients who had OCA transplantation. Univariate analysis revealed that older age, female gender, larger defect size, hypertension and smoking are potential risk factors of ACI graft failure. Yet, only female gender (OR 1.02, CI 1.01-3.64, P = 0.048), defect size (OR 1.07, CI 1.01-1.14, P = 0.035), and hypertension (OR 3.73, CI 1.20-11.6, P = 0.023) demonstrated to be independent predictors of failure. In patients who underwent OCA transplantation, however, baseline demographics and clinical characteristics were similar between the failure and successful group. Consequently, hypertension seems not to be a significant risk factor for failure in patients that underwent OCA transplantation. Thus, the current study demonstrated that hypertension, female gender, and defect size are independent predictors of ACI graft failure but do not determine survivorship after OCA transplantation. This is the first study investigating the effects of hypertension on cartilage repair procedures.
Hypertension is the most common cardiovascular risk factor and contributes to widespread morbidity and mortality worldwide. 41 Despite a paucity of literature on the effects of hypertension on cartilage repair, multiple theories can be pronounced about how hypertension might influence ACI graft regeneration.
First of all, an established association between hypertension and inflammation exits.42-45 Hypertensive patients are reported to have higher plasma interleukin-6 (IL-6),46-48 interleukin-1 beta (IL-1β),49,50 and tumor necrosis factor–α (TNF-α)46,48 levels compared with normotensive patients even when blood pressure targets are achieved.42-45 This observation is further supported by the fact that even when blood pressure targets are achieved, many hypertensive patients remain at risk for a cardiovascular event, which is thought to be related to the underlying inflammation.42-45 The same cytokines, but mostly IL-1β and TNF-α, are elevated when homeostatic joint environment becomes disrupted due to trauma, chronic overload, or surgery.51-53 IL-1β and TNF-α in an autocrine/paracrine manner, stimulate their own production and induce chondrocytes to produce proteases, chemokines, nitric oxide, and eicosanoids such as prostaglandins and leukotrienes. The action of these inflammatory mediators within cartilage is predominantly to drive catabolic pathways, inhibit matrix synthesis, and promote cellular apoptosis.52,54 Moreover, IL-1β has been reported to be detrimental to the articular cartilage.55-57 Intraarticular bleeding, following surgery or injury, results in a transient high level of these aforementioned proinflammatory chemokines. 58 It can be theorized that in hypertensive patients, with already elevated plasma IL-1β49,50 IL-6,46-48 and TNF-α46,48 levels, these catabolic cytokines might reach a pathological elevation. Furthermore, these factors might filter through the synovial membrane into the joint following surgery, or may be overproduced in the joint as a result of the already elevated proinflammatory cytokines in the blood, which created an inflammatory environment, resulting in a continuous proinflammatory cytokines presence. 59 Consequently, these changes might provide an unfavorable milieu for the implanted immature tissue, resulting in an altered tissue regeneration, and/or integration, and finally leading to graft failure.
Immature tissues, such as freshly implanted ACI grafts, are more fragile and susceptible than normal mature cartilage,60,61 as its cells are not yet fully embedded in the potentially chondroprotective enclosure of a cartilaginous extracellular matrix. 62 Accordingly, Scotti et al. 56 reported that IL-1β causes a transient reduction of GAG and type II collagen accumulation and increased production of matrix metalloproteinase (MMP)-1 and MMP-13 in human engineered cartilage. Likewise, other studies demonstrated that bovine engineered cartilage does not grow when exposed to IL-1β after 14 days of culture, even after a recovery period or physiological loading.57,63 Therefore, we theorize that ACI is more sensitive to a pro-inflammatory environment than OCA, in which a mature hyaline cartilage is transplanted. Generally, the success of OCA relies on the quality of the transplanted tissue, and the sufficient subchondral integration and remodeling of both the graft and surrounding host bone.64-67 Bone healing is a unique biological process regulated by a complex array of signaling molecules and proinflammatory cytokines. TNF-α, IL-1β, and IL-6, are expressed at the site of fractured bone and have been shown to enhance repair. 68 TNF-α and IL-1β are expressed at both very early and late phases in the repair process, which suggests that these cytokines are important in the initiation of the repair process and play important functional roles in intramembraneous bone formation and trabecular bone remodeling.69,70 Consequently, the elevated TNF-α, IL-1β, and IL-6 in hypertensive patients might not affect bone healing negatively following OCA transplantation. This might explain the finding of the current study that hypertension is an independent risk factor for ACI failure with over 3.73-fold increased risk but has no effect on OCA graft survival.
Another possible explanation for our observation is that hypertensive patients have a higher chance of postoperative bleeding, causing increased blood exposure to the joint, hence the freshly implanted graft. Elevated blood exposure has been reported to have a negative effect on engineered cartilage, and thus might be an additional potential risk factor for ACI graft failure.71,72
Finally, hypertension is responsible for a narrowing of blood vessels, principally due to a reduced capacity of cells to produce nitric oxide, and therefore leading to a reduced peripheral blood flow. 73 As cartilage is an avascular tissue, required nutrients and oxygen must diffuse through synovial fluid and subchondral bone to reach the chondrocytes. The reduced blood flow in subchondral bone might compromise the exchange of nutrients and oxygen, which in turn leads to degenerative changes within the cartilage.74,75 Given the fact that freshly implanted chondrocytes, as implanted in ACI, are under a sensitive process of proliferation and differentiation, this impaired oxygen and nutrients exchange might disturb this delicate milieu resulting in an inadequate maturation of the cells and finally in failure of the graft.
Our study also revealed that female gender and defect size are independent predictors of ACI graft failure which is in accordance with the literature.27,28 Jungmann et al. 27 reported a significantly higher incidence of reinterventions in the subgroup of female patients (26.7%) compared with male patients (17.3%; odds ratio 1.7; P = 0.021). Moreover, Ebert and colleagues 28 showed that defect size was significantly correlated (P < 0.05) with the MRI composite score and all pertinent MRI descriptive parameters, besides graft infill and subchondral bone.
The present study’s univariant analysis also indicated that older age and smoking are potential risk factors for ACI graft failure. Yet, these factors did not reach the level of significance with multivariate regression. Numerous studies reported age as prognostic factor of ACI failure.26,27 The chondrogenic potential of aged donors’ chondrocytes is reduced, 76 and the production of growth hormones, cytokines, and connective tissue proteins changes over time, which ultimately predisposes for degenerative diseases. 77 Thus, it is thought that older patients have an increased risk of ACI failure. However, our results suggest that if the patient has no other risk factor besides older age, articular cartilage repair with ACI might still result in favorable outcome, as reported in previous studies.78,79 Smoking also has reported adverse effects on cartilage repair.80,81 In a laboratory study by Schmal et al., 82 knee lavage fluids of patients with circumscribed cartilage lesions treated with either microfracture or ACI were analyzed. Synovial expression of total protein content, insulin-like growth factor–I (IGF-I), and basic fibroblast growth factor (bFGF) was significantly diminished in smokers compared with nonsmokers. Furthermore, Jaiswal et al. 81 found that in patients undergoing ACI, smokers had significantly worse clinical outcomes than nonsmokers with graft failures only seen among smokers. Nonetheless, while the current study also found the reported negative effect of smoking on ACI graft survival, it was determined not to be an independent predictor of failure.
Our study has several limitations: First, hypertension was only used as a dichotomous variable (yes/no), and the effect of the exact blood pressure was not investigated. Second, the chronicity of comorbidities and the effect of patients’ medication was not evaluated either. Thus, we emphasize the need for further studies that investigate the effects of these factors on cartilage restoration. Finally, our department is a tertiary center that predominantly treats larger defects and thus, these findings cannot be automatically extrapolated to smaller lesions.
Conclusion
In summary, the current study demonstrated that older age, female gender, larger defect size, hypertension and smoking are potential risk factors of ACI graft failure. Yet, only female gender, defect size and hypertension were independent predictors of failure. In fact, hypertensive patients had an over 3.7-fold increased risk of ACI graft failure. In patients who underwent OCA transplantation, hypertension was determined not to be a significant risk factor for graft failure. Consequently, the authors suggest that treating surgeons should carefully assess patients’ characteristics and comorbidities, and that OCA transplantation might be preferred for the treatment of symptomatic cartilage defects in the knee if patients present with hypertension.
Footnotes
Authors’ Note
Investigation performed at the Cartilage Repair Center, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts, USA
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Our institutional review board approved this study.
Informed Consent
Informed consent was obtained from all patients at the time they were entered into our institutional database.
Trial Registration
Not applicable.