
Abstract
Objective
Takedown of the anterior meniscus to facilitate exposure of the cartilage defects located on the tibial plateau and/or posterior femoral condyle with subsequent reattachment is being performed clinically; however, clinical evidence is lacking to support the safety of this technique. The aim of this study was therefore to investigate whether meniscal extrusion develops after patients undergo meniscus takedown and transosseous refixation during autologous chondrocyte implantation (ACI).
Design
We analyzed data from 124 patients with a mean follow-up of 6.8 ± 2.5 years. Sixty-two patients who underwent (ACI) with anterior meniscus takedown and refixation by the senior surgeon (TM), were compared with a matched control group of patients who underwent ACI without meniscus takedown. Meniscal extrusion was investigated by measuring the absolute value and the relative percentage of extrusion (RPE) on 1.5-T magnetic resonance images (MRI) at final follow-up. The number of menisci with radial displacement greater or lesser than 3 mm was determined. In cases where a preoperative MRI was available, both pre- and postoperative meniscal extrusion was evaluated (n = 30) in those patients undergoing meniscal takedown.
Results
There was no significant difference in either absolute meniscus extrusion, RPE, or extrusion rate in patients with and without meniscus takedown. Among patients with meniscal takedown and both pre- and postoperative MRI scans, absolute meniscus extrusion, RPE, and extrusion rate showed no significant differences.
Conclusion
Meniscal takedown and subsequent transosseous refixation is a safe and effective technique for exposure of the tibial plateau and posterior femoral condyle.
Introduction
Autologous chondrocyte implantation (ACI) is a well-established treatment for large chondral defects of the knee.1-3 Several studies have reported durable and improved clinical outcomes after ACI over the long-term for tibiofemoral and patellofemoral defects.1-7 Most cases where the defect location is difficult to expose, it can be accessed through standard surgical arthrotomy, however, defects of the tibial plateau or posterior femoral condyle can be challenging to visualize and approach. To perform a thorough defect preparation and repair, hyperflexion of the knee and takedown of the anterior meniscal horn is often necessary. 8 After cartilage repair, transosseus sutures are used to reattach the anterior meniscal root to its insertion and the intermeniscal ligament is repaired.
The medial and lateral menisci are responsible for absorbing 50% to 70% of the load across their respective compartments and increasing the tibiofemoral contact surface area. 9 The menisci also serve to distribute lubrication in the knee joint, and contribute to proprioception. 10 Prior studies have demonstrated that meniscal extrusion in the native knee results in increased contact stresses across the tibiofemoral joint leading to degenerative changes and to the progression of osteoarthritis.11-14 Accordingly, preservation of the meniscus function is crucial to preventing or delaying degenerative changes in the knee joint.15,16 Meniscal extrusion, commonly defined as the distance between the periphery of the tibial plateau and the outer edge of the meniscus, is considered pathological if it exceeds 3 mm of radial displacement in the coronal plane. 17-19Technically, meniscus takedown and refixation is a useful technique for approaching defects on the tibial plateau or posterior femoral condyle; however, its safety for meniscal integrity and prevention of extrusion has not been established in the literature. The purpose of this study was to investigate whether meniscal extrusion occurs in higher rates in patients undergoing meniscus takedown and transosseous suture refixation during an ACI procedure as compared with a matched cohort of patients undergoing ACI without meniscal takedown. We hypothesized that anatomical repair using transosseous refixation of the anterior root of the meniscus in addition to repair of the intermeniscal ligament would provide secure fixation with similar rates of meniscal extrusion between groups.
Materials and Method
Patient Cohort
This study was approved by our institutional review board, and informed consent was obtained from all patients at the time they were entered into our institutional cartilage repair database. In this review of prospectively collected data, 322 patients underwent cartilage repair with ACI between July 2007 and May 2015 by the senior surgeon (TM). Among them, 78 patients underwent meniscal takedown to facilitate exposure of a cartilage defect on the tibia plateau and/or posterior femoral condyle. The senior surgeon takes down the meniscus in the majority of cases where these types of lesions are present. In rare cases with extremely posterior femoral condyle defects, takedown of the collateral ligament origin with a bone block off the femoral condyle is performed at our institution. 8
The indications for treatment of cartilage defects with ACI were one or more full-thickness symptomatic chondral defects of the knee with a consistent history, physical examination, magnetic resonance imaging (MRI), and arthroscopy to the defect(s). Contraindications to treatment included inflammatory joint disease, unresolved or recent septic arthritis, metabolic or crystal disorders. Tibiofemoral malalignment of >3° from the neutral mechanical axis into the involved compartment was corrected with concomitant osteotomy. Patellofemoral maltracking was addressed with anteromedialization tibia tubercle osteotomy (TTO) 20 to centralize patellar tracking, and proximal soft tissue balancing (lateral release, vastus medialis obliquus advancement) as necessary to align the extensor mechanism. Patients who underwent concomitant meniscal allograft transplantation or did not have postoperative MRI after ACI at a minimum of 1 year were excluded from this study. Thus, 62 patients met the inclusion criteria and were included in intervention arm (meniscal takedown) of this study. Of these, 30 patients had completed both pre- and postoperative MRI at our institution and were enrolled in the subgroup analysis to determine differences in extrusion between pre- and postoperative state.
A control group was formed by matching 62 ACI patients without meniscus takedown individually according to age, gender, body mass index (BMI), defect size, and affected compartment (medial or lateral tibiofemoral compartment). Demographics are summarized in Table 1 . As meniscus takedown was performed in almost all cases with involvement of the tibial plateau, matching for the specific defect location was not feasible, and we therefore matched only for the affected compartment. The closest available match was used for age, BMI, and defect size, but a deviation of 5 years for age, 4.0 kg/m2 for BMI and 10 mm for size was accepted. Failure was defined as a surgical removal of more than 25% of the ACI graft area; revision cartilage repair; additional surgical marrow stimulation treatment violating the subchondral bone of the treated defect, or a prosthetic replacement.
Patients’ Demographics.
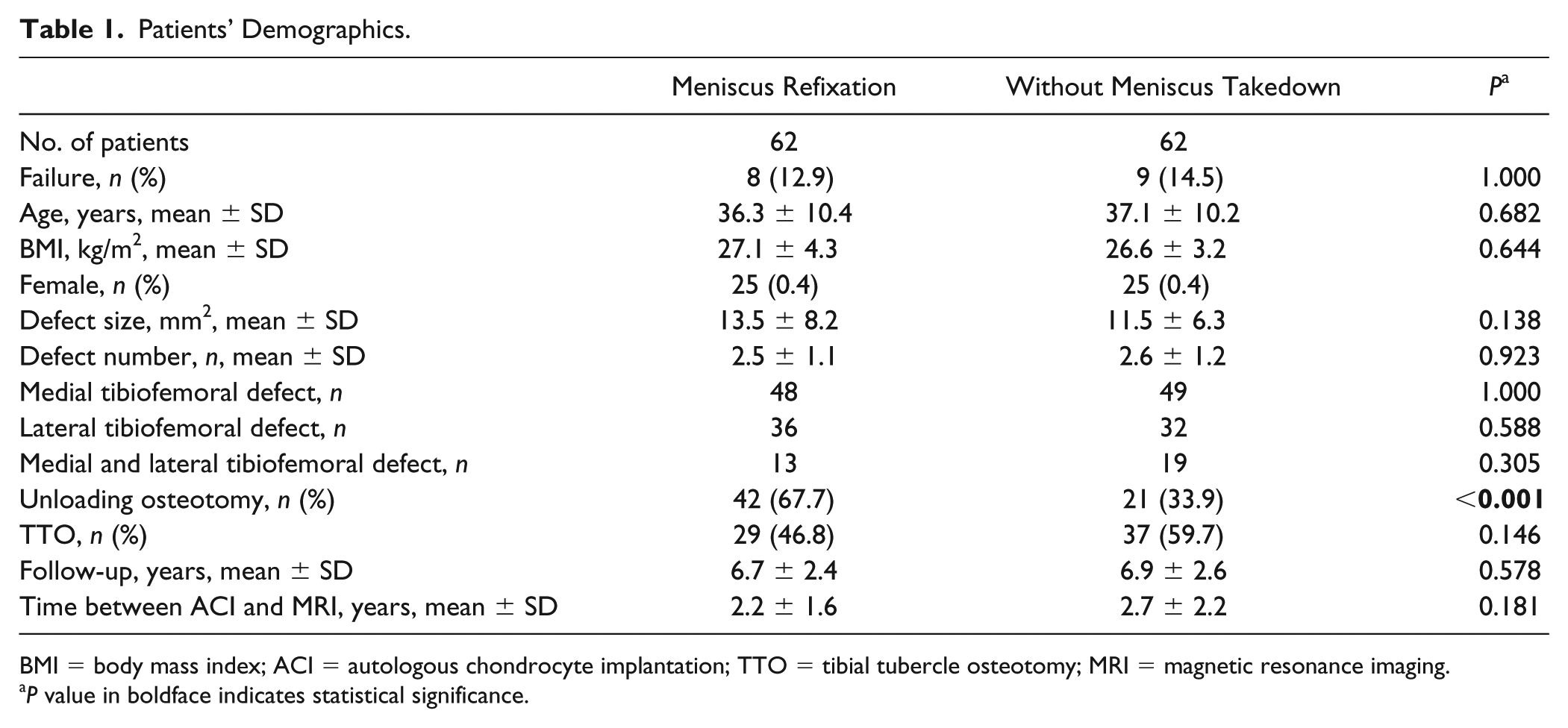
BMI = body mass index; ACI = autologous chondrocyte implantation; TTO = tibial tubercle osteotomy; MRI = magnetic resonance imaging.
P value in boldface indicates statistical significance.
Surgical Procedure
Cartilage repair with ACI has been described previously in great detail.21,22
In patients with a tibial plateau and/or posterior femoral condyle defect, the anterior horn of the meniscus is reflected by incising the intermeniscal ligament and anterior root, and then mobilizing the meniscus together with the joint capsule by sub-periosteal dissection off the tibia as a complete sleeve ( Fig. 1A and B ). 8 The knee is hyperflexed, and the tibia externally rotated for the medial compartment and internally rotated for the lateral compartment, providing excellent access to the defects.
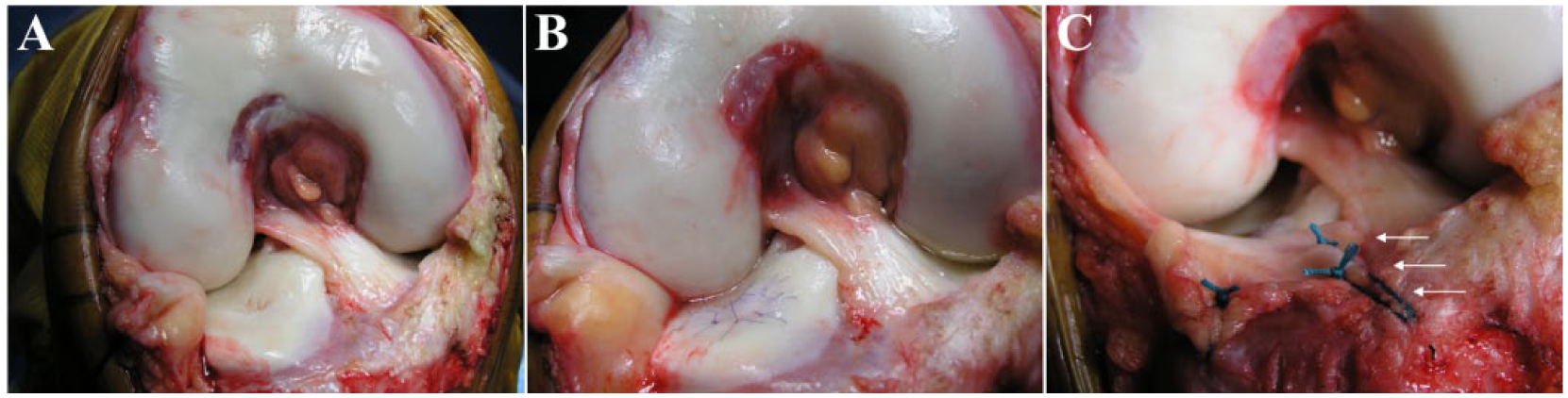
Perioperative images of a patient who underwent autologous chondrocyte implantation (ACI) for a lateral tibial plateau defect with meniscus takedown and reattachment. (
Patients with defects on the weight-bearing femoral condyles in the setting of >3° malalignment from the neutral mechanical axis were treated with a concurrent valgus- or varus-producing corrective osteotomy. Patients with patellofemoral defects with maltracking underwent concomitant TTO and soft tissue balancing to correct maltracking. The meniscus was repaired with transosseous 1-0 Vicryl sutures (Ethibond) using a tapered needle and the intermeniscal ligament was reduced and repaired ( Fig. 1C ). 8
Postoperative Rehabilitation
The rehabilitation protocol was the same in both groups. Motion was emphasized in the first 6 weeks using continuous passive motion (CPM) and stationary bicycling, active and isometric straight leg raises and touchdown weightbearing. Between 7 and 12 weeks, patients progressed from partial to full weightbearing. Patients were restricted from inline impact activities (running) for 12 to 18 months and cutting sports until 18 months postoperative. The ACI rehabilitation protocol considered each patient’s individual surgical reconstruction, graft maturation, and previous activity level, which were reflected in individualized variations in the rehabilitation protocol. 23
Magnetic Resonance Imaging
MRI examinations were used in this study for the pre- and postoperative evaluation of meniscal status after ACI with (Case) and without (Control) meniscus takedown. Meniscal integrity and meniscal extrusion were evaluated using sagittal and coronal proton density-weighted fast spin echo MRI scans (1.5-T; Siemens). Sagittal and coronal plane images were obtained in 3-mm sections with an interslice gap of 3 mm. In cases of meniscal extrusion, the length of extrusion beyond the margin of the tibial articular cartilage may differ between images. Consequently, the image with the greatest extrusion was selected for the measurement. 24 Images were evaluated and measured by 2 independent orthopedic surgeons who were blinded to case status. Each surgeon measured meniscal extrusion twice with a 1-month interval. The mean of all 4 measurements per patient (2 observers, 2 time points) was used for analysis. Meniscal extrusion was considered when lateral displacement of more than 3 mm beyond the tibial rim was present. 25 Meniscal displacement was measured using the technique described by Verdonk et al. 26 The absolute value of meniscal displacement in the coronal plane was defined as the distance between the outer margin of the proximal tibial plateau at the proximal articular surface and the outer edge of the extruded meniscus. Since knee size differs between individual patients, the amount of meniscal extrusion was also calculated as the relative percentage of extrusion (RPE). RPE was calculated as the absolute value of the displaced portion of the meniscus divided by the absolute value of the entire meniscal width ( Fig. 2 ).
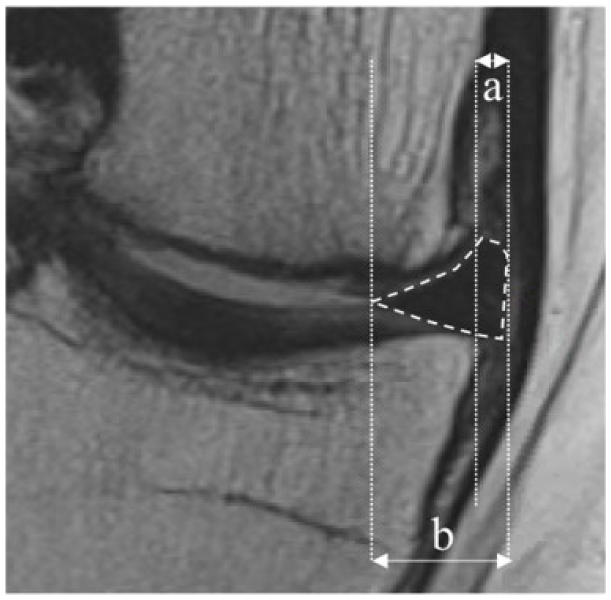
Meniscal extrusion (meniscus is contoured by the dashed line) is defined as the greatest distance (a) from the most peripheral aspect of the meniscus to the border of the tibia, excluding any osteophytes on coronal images. PRE is defined as the percentage of the width of extruded menisci (a) compared with the entire meniscal width (b) (RPE = a/b × 100).
Statistical Analysis
SPSS (version 21.0; IBM Corp) was used to perform statistical analyses. Demographic results are reported as mean and standard deviation. Using the Shapiro-Wilk test confirmed normal distribution of the data. Consequently, the absolute value of the meniscal extrusion and the RPE of patients with and without meniscus takedown were compared using the independent unpaired t test. Preoperative absolute value of meniscal extrusion and RPE were compared with postoperative MRI using paired t test, in patients with meniscus refixation. For categorical data, the Fisher exact test or Pearson chi-square test was used as appropriate. The reliability of meniscal extrusion measurements was assessed using the intraclass correlation coefficient (ICC), which quantifies the proportion of the difference caused by measurement variability. All reported P values are 2-tailed and the significance level was set at 0.05.
Results
Baseline demographics showed no significant differences between groups except concomitant unloading osteotomy ( Table 1 ). Patients with meniscus refixation underwent significantly more unloading osteotomies (n = 42, 67.7%) than patients without meniscus takedown (n = 21, 33.9%) (P < 0.001). In the meniscus reattachment group, meniscus extrusion (>3 mm) occurred in 14.3% (6 of 42 patients) with, and 5% (1 of 20 patients) without concomitant unloading osteotomy (P = 0.280). During the follow-up period, 53.2% of patients underwent subsequent surgery of the affected joint. A detailed list of performed subsequent surgeries is presented in Table 2 . No significance was seen between the groups regarding the number of subsequent surgeries (meniscus refixation group: 32 patients (51.6%); without meniscus take-down: 34 patients (54.8%) (P = 0.857)).In patients with meniscal refixation during ACI, 8 patients (12.9%) were considered a failure, while failure occurred in 9 patients (14.5%) without meniscal takedown (P = 1.000).
Subsequent Surgeries Performed During the Follow-Up Period.
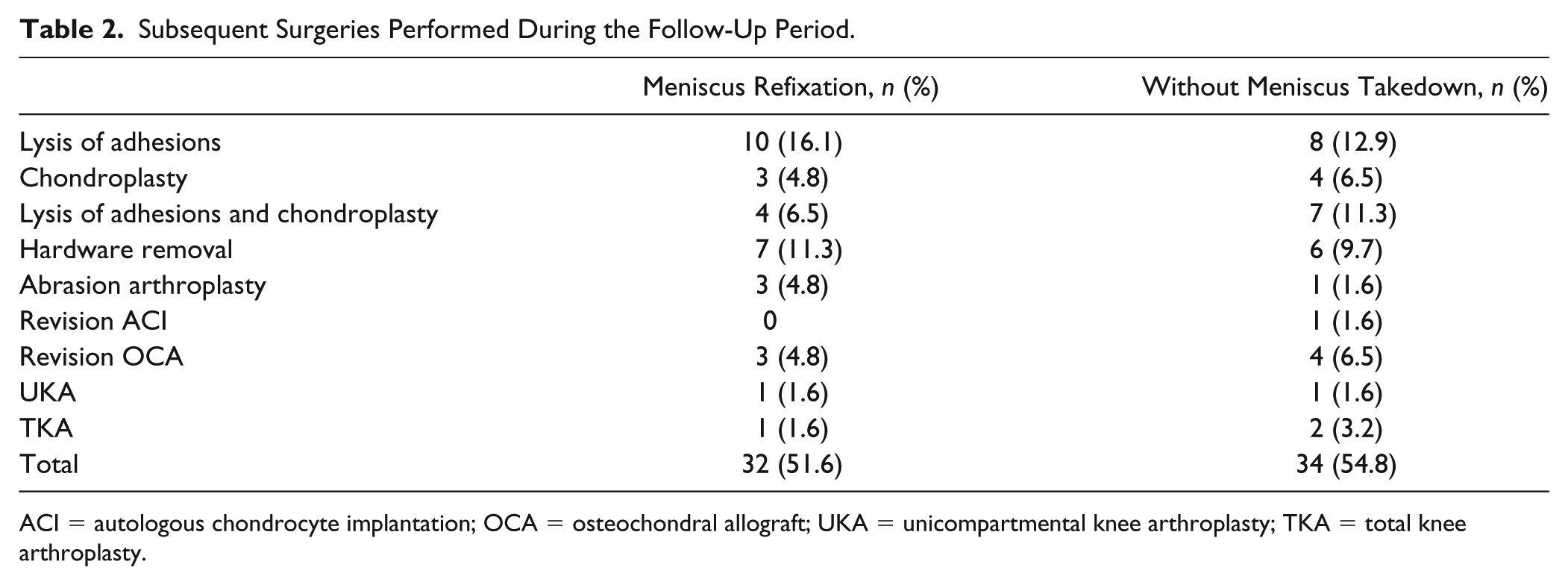
ACI = autologous chondrocyte implantation; OCA = osteochondral allograft; UKA = unicompartmental knee arthroplasty; TKA = total knee arthroplasty.
Each group consisted of 45 medial (72.6%) and 17 lateral menisci (27.4%). Neither absolute meniscal extrusion nor RPE differed significantly between groups (P = 0.108 and P = 0.306, respectively). Meniscal extrusion of more than 3 mm was observed 11% of patients with meniscal takedown and refixation compared with 18% without meniscus takedown (P = 0.256) ( Table 3 ).
Comparison of Radial Displacement between Patients with Meniscal Refixation after Meniscus Takedown and Control Patients without Meniscus Takedown.
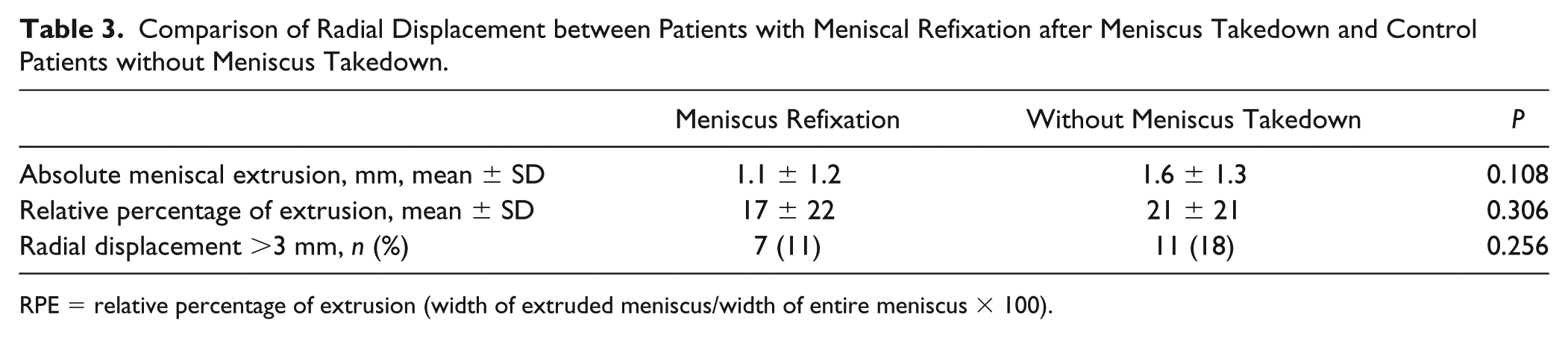
RPE = relative percentage of extrusion (width of extruded meniscus/width of entire meniscus × 100).
In patients who underwent meniscus takedown and refixation, pre- and postoperative absolute meniscus extrusion showed no significant difference (preoperative 1.6 ± 2.5 mm vs. postoperative 1.3 ± 1.5 mm; P = 0.589). There was also no significant difference in RPE between pre- and postoperative MRI in patients with meniscal takedown and refixation (preoperative 14 ± 21 mm vs. postoperative 21 ± 24 mm; P = 0.265). Preoperative meniscal extrusion of more than 3 mm was observed in 3 out of 30 patients (10%) with all 3 patients demonstrating similar meniscal extrusion on postoperative MRI. Among the 30 patients with pre- and postoperative imaging, a total of 5 (16%) had postoperative meniscal extrusion. There were no significant differences between pre- and postoperative meniscal extrusion (P = 0.447) ( Table 4 ).
Pre- versus Postoperative Comparison of Displacement in Patients with Meniscus Takedown.

RPE = relative percentage of extrusion (width of extruded meniscus/width of entire meniscus × 100).
Interobserver reliability ranged from 0.899 to 0.951, and intraobserver reliability ranged from 0.821 to 0.912.
Discussion
This is the first study to demonstrate the outcomes and safety of anterior meniscal takedown for exposure of posterior femoral or tibial chondral defects during cartilage repair. Meniscal extrusion did not differ between patients with meniscal takedown and a cohort of matched patients without. Additionally, in meniscal takedown patients with pre- and postoperative MRIs performed at our institution, there was no increase in meniscus extrusion.
As there is no other literature specifically addressing the outcomes of meniscal takedown, we elected to compare our data to meniscal root repairs. Meniscal root tears are avulsion injuries of the posterior meniscal tibial attachment,27,28 similar to the anterior takedown in the present study. Meniscal root tears result in incompetence of the hoop strain mechanism of the meniscus and loss of the ability to resist extrusion under axial loading, leading to meniscus extrusion and subsequent increased articular cartilage contact pressures with increased risk of osteoarthritis.29-31 Surgical repair of meniscal root tears aims for anatomic reduction and fixation with transosseous sutures or suture anchors.16,28,32,33 Multiple techniques for transosseous meniscal root repair have been described using accessory portals, passing devices, various suture configurations, and drilling techniques.28,34-36 Reconstruction and healing of the meniscal root using the transosseous repair technique has been confirmed by biomechanical studies, MRI, as well as second-look arthroscopy.16,28,35,37-40 Additionally, clinical outcome studies of transosseous repair of meniscal root tears have reported significant functional improvements, and a reduction in meniscal extrusion as demonstrated by MRI, second-look arthroscopy, and delayed cartilage degradation.16,33,41-43
The importance of anatomic meniscal stabilization to normalize joint contact forces is being supported by several biomechanical studies.15,16 It has been reported that transtibial pullout suture repair (TPR) restores the loading profile of the knee to the intact state.39,40 Kim et al. 16 compared the outcomes of 28 patients after partial meniscectomy with those of 30 patients after TPR. TPR resulted in significantly better clinical and radiologic outcome than did partial meniscectomy. In addition, it was noted that meniscal healing with restoration of meniscal hoop tension was observed on MRI and second-look arthroscopy. Chung et al. 41 reported improved outcomes in patients with TPR compared to partial meniscectomy in patients with a minimum of 5-year follow-up without progression of arthrosis. Lee et al. 42 observed at second-look arthroscopy complete healing of repaired menisci without additional signs of chondral deterioration at a minimum of 2 years follow-up. They also noted improved clinical outcomes and no radiographic progression to OA. Kim et al. 43 reported the appearance of firm scar tissue adhesions between the inferior surface of the meniscus and the articular cartilage of the tibial plateau after meniscal tear repairs. These results suggest that repair of a disrupted meniscal root is feasible.
However, unfavorable results after pullout meniscal root repair have also been reported. Seo et al. 38 did not observe complete healing in all patients that underwent second-look arthroscopy, despite clinical improvement. In another study, Cho et al. 37 observed good clinical results but did not observe complete healing by arthroscopy. Moon et al. 44 found that meniscal extrusion progressed on follow-up MRI at a mean of 33 months after pullout meniscal root repair in 51 cases.
The clean transection and near immediate repair of the anterior meniscal root during our takedown procedure is an ideal scenario for healing, and results similar to, or better than those seen with traumatic root tears should be expected.
Meniscus extrusion, in our study, did not progress after transosseous anterior horn fixation, which may be a consequence of the ideal healing environment of an acute injury, and/or the different load distribution patterns of the anterior and posterior meniscus. The anterior horn bears a lesser proportion of load than does the posterior horn.11,25 Surgical technique may also explain differences as in our study an open technique was used, which allows precise anatomic reduction and fixation of the anterior horn of the meniscus with restoration of load distribution without overtensioning of the meniscal fibers. 45 Additional anatomic repair of the intermeniscal ligament helps to restore meniscal tension. The rich vascular supply of the anterior and posterior meniscal roots provides enhanced healing after transosseous meniscal refixation. 46
Cartilage defects on the posterior femoral condyle or tibial plateau present a unique challenge to the orthopedic surgeon, however, only few studies reported the surgical approach of these lesions.47-50
Lamblin et al. 47 introduced the “drawer-exposure” for osteonecrotic lesions of the tibial plateau, in which an osteotomy of the tibial plateau is performed in conjunction with the transplantation of a fresh-frozen osteochondral allograft. Wajsfisz et al. 48 described the arthroscopic retrograde osteochondral autograft transplantation (OATS) technique addressing cartilage defects on the tibial plateau. In this technique, the surgeon reams a tunnel through the tibia using an angular calibrator to exactly reach the defect on the tibial plateau and to ensure the appropriate orientation of the tunnel. Subsequently, an osteochondral plug is inserted through the tibial tunnel under arthroscopic control. Ueblacker et al. 49 also investigated the utilization of retrograde OATS technique to the central tibial plateau (5 patients) and demonstrated high short- to mid-term satisfaction rates among patients. These procedures for the treatment of tibial plateau defects require complicated and complex surgical steps, the utilization of bone grafts, and are not pertinent for approaching posterior femoral condyle defects. Ronga et al. 50 presented a case report using arthroscopic ACI for the treatment of a cartilage defect in the lateral tibial plateau. However, while it is challenging to use this technique for posterior femoral condyle defects, meniscal takedown and subsequent transosseous refixation has proven to be a safe and straightforward procedure for cartilage defects on the tibial plateau and posterior femoral condyle.
Another surgical option is to take down the origin of the collateral ligament with a bone block off the femoral condyle, which completely opens up the side of the knee. 8 However, isolated meniscal takedown yields ideal exposure of the tibial plateau and/or posterior femoral condyle defects in the vast majority of cases and the takedown of the collateral ligament is not required.
Our study has limitations. Serial MRI scans over a longer time period postoperation might have demonstrated progressive extrusion not seen at the early time point of, on average, 2.5 years. However, several studies on radiological outcomes after meniscus transplantation reported that meniscal extrusion does not progress during the mid-term follow-up.24,51 Nonetheless, as for any subject, future studies with longer follow-up periods are desirable. Second, the focus of our study was to assess meniscal extrusion after meniscus takedown, rather than clinical functional outcomes, which have been reported in prior studies,16,52,53 including one that specifically evaluated patients treated with this technique for bipolar tibiofemoral cartilage lesions. 54 Last, meniscus extrusion was assessed in a non-weightbearing fashion in the current study, which might not have yielded sufficient sensitivity to detect changes in resistance to hoop stress. Thus, future research is warranted to validate the results of the present study using a weightbearing assessment such as ultrasound.
Conclusion
In conclusion, our matched cohort study identified overall low meniscus extrusion rates that were not different between patients with and without meniscal takedown during cartilage repair with ACI. Meniscal takedown and subsequent transosseous refixation is a safe and effective technique for exposure of the tibial plateau and posterior femoral condyle.
Footnotes
Authors’ Note
This investigation was performed at the Cartilage Repair Center, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA.
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by our institutional review board.
Informed Consent
Informed consent was obtained from all patients at the time they were entered into our institutional cartilage repair database.
Trial Registration
Not applicable.