
Abstract
Background
Chondral lesions in the patellofemoral compartment represent a difficult entity to treat among active patients, with no clear consensus on the optimal treatment strategy. The purpose of this study was to review the functional outcomes of patients >40 years old with primary patellofemoral osteochondral lesions who underwent a cartilage restoration procedure with a structural graft.
Methods
Following institutional review board approval, 35 patients >40 years treated for patellofemoral chondral or osteochondral injuries were retrospectively identified. Seventeen (47%) had prior surgery (mean 1.4 procedures, range 1-4). Average follow-up was 3.6 ± 1.6 years. Average patient age was 51.5 years (range 40-72 years); 54% were male. Twenty-six (74%) had isolated trochlear lesions, 7 had isolated patellar lesions (20%), while 2 (6%) had bipolar lesions. Twenty patients (57%) were treated with synthetic biphasic scaffold plugs (SS), 9 (26%) with fresh osteochondral allograft (OCA) and 6 (17%) with osteochondral autograft transfer (OAT). Outcomes were measured with validated measures: Activity of Daily Living Score (ADL), International Knee Documentation Committee (IKDC) Subjective Evaluation form, and Marx Activity Scale (MAS).
Results
The average lesion size for the entire cohort was 3.1 ± 1.7 cm2. Average defect size was 2.6 ± 1.7 cm2 for the SS group, 4.3±1.5 cm2 for the OCA group, and 2.9 ± 0.8 cm2 for the OAT group (P > 0.051). Outcome scores for the entire population demonstrated significant improvement in ADL (P = 0.002) and IKDC scores (P = 0.004) between baseline and final follow-up, while MAS scores were maintained (P = 0.51).
Conclusion
Structural grafts are a viable treatment option for symptomatic focal osteochondral lesions of the patellofemoral joint in patients 40 years and older, with anticipated improvements in pain and function and maintenance of preoperative activity levels.
Introduction
Focal chondral and osteochondral lesions of the patellofemoral joint can cause significant pain and disability. During knee arthroscopy, the patella has been observed as the most common location for grade IV chondromalacia. 1 This likely relates to the fact that the patellofemoral joint absorbs forces up to 6.5 times body weight during activities of daily living. 2 Patients with focal cartilage defects of this joint can have an unacceptable reduction in quality of life, which may be prolonged since these lesions have limited healing potential without surgical intervention.3-5 This presents a challenging problem, especially in aging athletic populations who wish to remain active but are not candidates for arthroplasty. Treatment options for cartilage repair and restoration in the patellofemoral joint include marrow stimulation, autologous chondrocyte implantation (ACI), minced cartilage scaffold, osteochondral autograft transfer (OAT), osteochondral allograft transplantation (OCA), structural synthetic scaffold (SS), and patellofemoral arthroplasty.6-9
Noyes and Barber-Westin 10 reviewed available treatment options for cartilage lesions of the patellofemoral joint in patients younger than 50 years and were not able to determine an ideal surgical treatment option as there were unpredictable results across several studies. Microfracture has shown inferior results to osteochondral autograft transfer.11-13 Although ACI may result in improved outcome scores in patients 40 years and older, it is limited by unpredictable lesion fill, reliance on 2 surgeries, prolonged recovery, and a higher risk of reoperation.14-16 Structural grafts have the benefit of providing time-zero restoration of the articular surface, earlier weightbearing, quicker recovery, and earlier return to sport.11,17 OAT for the treatment of patellofemoral lesions has demonstrated good to excellent results with significant improvements in functional outcome scores.18,19 Similarly, OCA has had good success in improving clinical outcome scores with good longevity of the graft in several studies.20-23 Because these studies focus on a younger cohort of patients with an average age of 30 to 34 years, it remains unclear whether patients older than 40 years experience similar improved outcomes. Accordingly, further study of the results of cartilage restorative procedures for this patient demographic is warranted. The purpose of this work is to report on the functional outcomes and activity levels of patient’s aged 40 years and older with patellofemoral lesions treated with structural grafts. These grafts included synthetic biphasic plugs as primary grafts, fresh OCAs, or OATs. We hypothesized that structural grafting methods can be used to successfully treat symptomatic, focal patellofemoral chondral, and osteochondral lesions in patients older than 40 years as evidenced by improved postoperative functional outcome measures.
Methods
Institutional review board approval was obtained for this study. Following approval, a retrospective review of prospectively collected clinical data was performed to identify a cohort of patients older than 40 years who underwent treatment for osteochondral lesions of the patellofemoral compartment of the knee.
Inclusion Criteria
For the current study, inclusion criteria were (1) age ≥40 years; (2) primary symptomatic patella, trochlea, or bipolar cartilage lesion(s) graded III or IV based on the Outerbridge classification24,25; (3) lesions of 1-9 cm2 in size; and (4) treatment with a structural graft (synthetic scaffold plug, osteochondral autograft or osteochondral allograft). Adjacent untreated regions in the operative knees had no more than Outerbridge grade II changes.
To be included, patients needed to have complete baseline, intraoperative, and minimum 2-year postoperative follow-up data. Exclusion criteria included patients with generalized osteoarthritis, ligamentous instability, lower extremity malalignment, inflammatory arthritis, and patients who had concomitant cartilage repair or restoration procedures of the distal femur or tibia.
After application of these criteria, we identified a total of 130 patients who were treated for isolated patellofemoral osteochondral lesions with structural grafts. Of these, 82 patients (63%) were younger than 40 years, while 48 patients (37%) were older than 40 years. Of those 48 patients, 35 (73%) had 2-year follow-up and were included in our review as they did not meet any other exclusion criteria.
Surgical Technique
All procedures were performed by a single, subspecialty-trained, sports medicine surgeon with more than 15 years of experience in cartilage restoration (RJW). In all patients, the procedure commenced with a diagnostic arthroscopy to identify any additional intra-articular pathology. After confirmation of a focal lesion in the patellofemoral compartment, an arthrotomy was made to access the lesion. If the lesion was isolated to the trochlea, the patella was not everted, but rather a medial or lateral parapatellar arthrotomy was created, which allowed the patella to be subluxed to access the lesion. If it was a patellar or bipolar lesion, a medial parapatellar arthrotomy was performed and the patella everted to allow sufficient access.
For the synthetic scaffold group (SS), commercially available plugs (OBI Trufit, Smith & Nephew, Andover, MA) were used in an off-label manner as a primary graft implanted at the defect site, rather than their intended use to backfill a donor site. At the site of the defect, recipient site bone plugs were removed using the appropriate instrumentation to create a cylindrical socket. Prefabricated SS plugs corresponding to recipient site diameter were fashioned to the appropriate depth and gently impacted flush with the surrounding articular cartilage in a manner to restore the normal surface contour of the patella and/or trochlea ( Fig. 1 ). Plug size varied from 7 to 11 mm in diameter. When multiple plugs were required, the initial synthetic plug was secured prior to removing the subsequent recipient site bone plug. It should be noted that these plugs were not Food and Drug Administration approved for use in this manner, and have since been discontinued and are no longer being utilized in this manner.
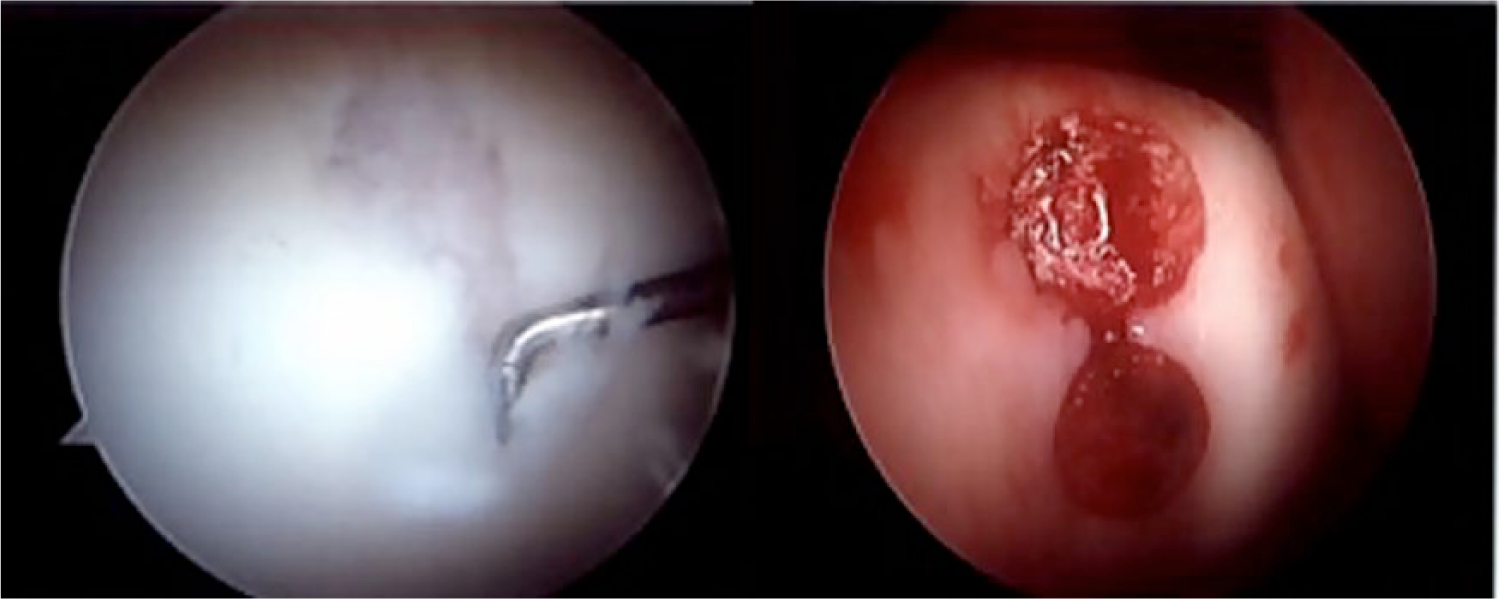
The use of synthetic scaffold plugs for treatment of a trochlear lesion.
For the OCA group, the recipient site was prepared using the allograft OATS instrumentation set (MTF Inc, Edison, NJ). A guide pin was placed centrally in the lesion perpendicular to the articular surface, and the appropriate sized reamer was used to create a cylindrical socket to a depth of 6 to 8 mm. Using distal femoral hemicondyle allograft, plugs were harvested using cylindrical reamers and cut to match the depth of the donor site circumferentially. The allograft plugs were harvested from locations that would provide an approximate match in contour to the trochlea, although they were not site-specific. The plugs were then placed and impacted gently until flush with the adjacent articular surface. Plug diameter ranged from 15 to 25 mm. When multiple plugs were required, each successive plug was inserted before the core for the next location was removed ( Fig. 2 ).
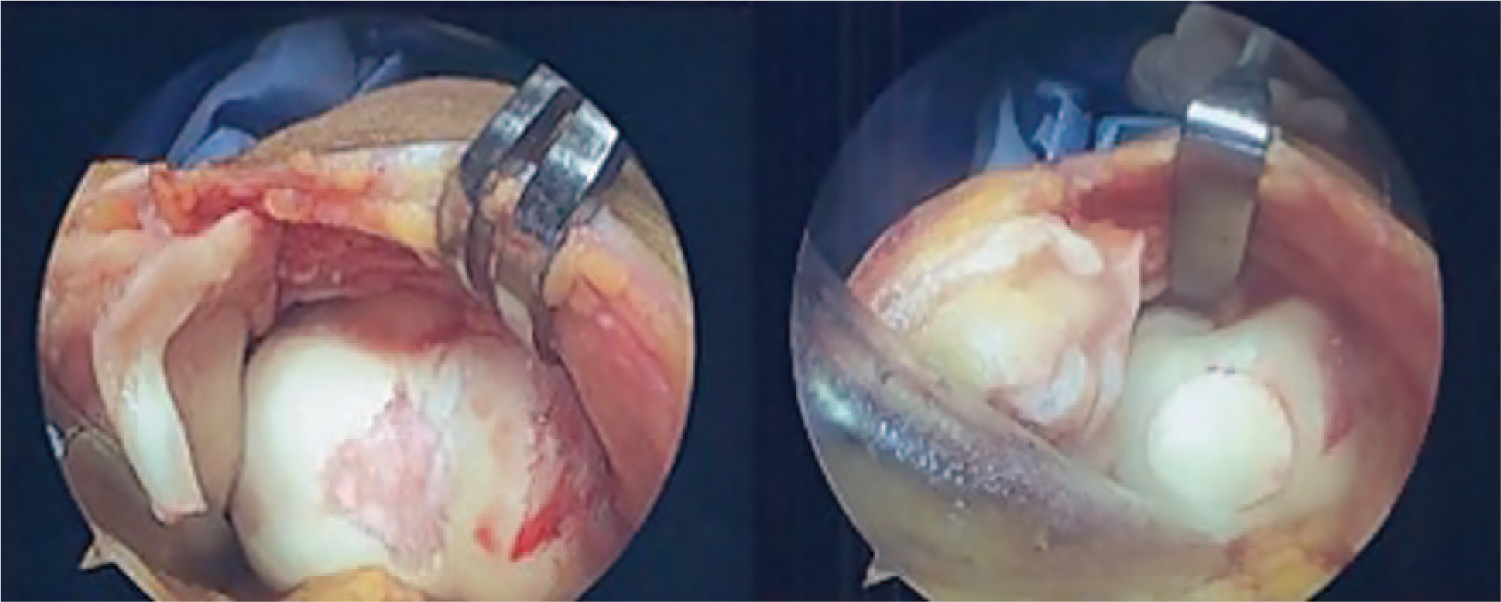
Osteochondal allograft plug for the treatment of a trochlear lesion.
Finally, for the OAT group, the recipient site was similarly prepared using the OATS instrumentation set (Arthrex, Naples, FL) to create a cylindrical socket at the chondral defect site to accept the donor graft. Size-matched donor plugs were harvested primarily from the femoral notch or superolateral trochlea and gently impacted until flush with adjacent cartilage surface. The OATS plug diameter ranged from 6 to 10 mm ( Fig. 3 ).
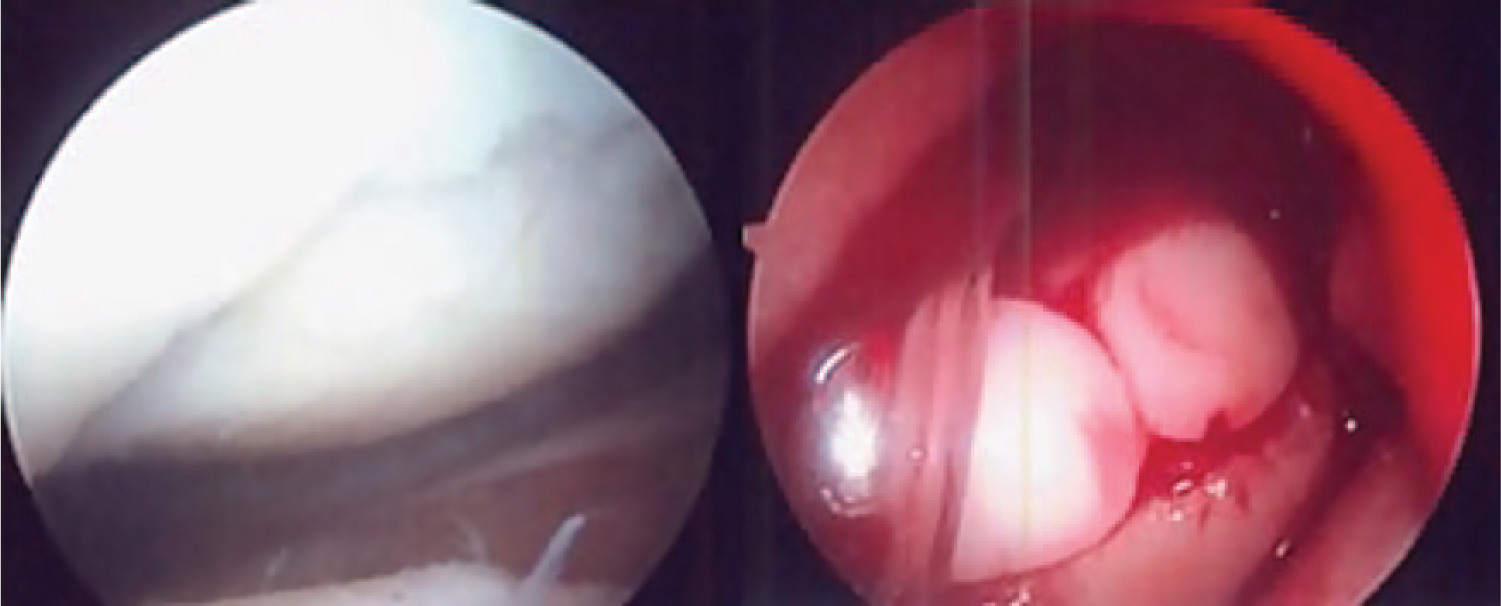
Autogenous osteochondral transfer for treatment of a trochlear lesion.
No plugs were unstable or required supplemental fixation. Decision making for the choice of structural graft was based on the senior surgeon’s preference for the lesion in question. OCA was typically favored for larger lesions, while synthetic scaffold was favored over OATs for smaller lesions due to the lack of donor site morbidity.
Patients in all groups underwent a structured protocol for post-operative rehabilitation. Continuous passive motion from 0° to 30° was initiated in the postanesthetic care unit and continued for 4 to 6 hours per day for 6 weeks postoperatively. Knee flexion was gradually increased as tolerated. Weightbearing was protected for 2 weeks in the scaffold and OCA groups and patients treated using OAT remained toe-touch weightbearing for 4 weeks. The goal for return to regular activities was generally between 6 to 8 months following surgery.
Assessment of Clinical Outcomes
Patients were evaluated pre- and postoperatively with a number of validated outcome measures. Knee function was addressed with the Activities of Daily Living (ADL) scale of the Knee Outcome Survey 26 and International Knee Documentation Committee (IKDC) Subjective Evaluation forms, 27 and patient activity level was assessed using the Marx Activity Scale (MAS). 28 Each of these forms was administered by an independent observer.
Statistical Methods
Descriptive statistics were reported in terms of means and standard deviations for continuous demographic and clinical characteristics and in terms of total number and percentage of patients for discrete variables. Comparisons of pre- and postoperative outcomes scores were performed with a paired t test.
Results
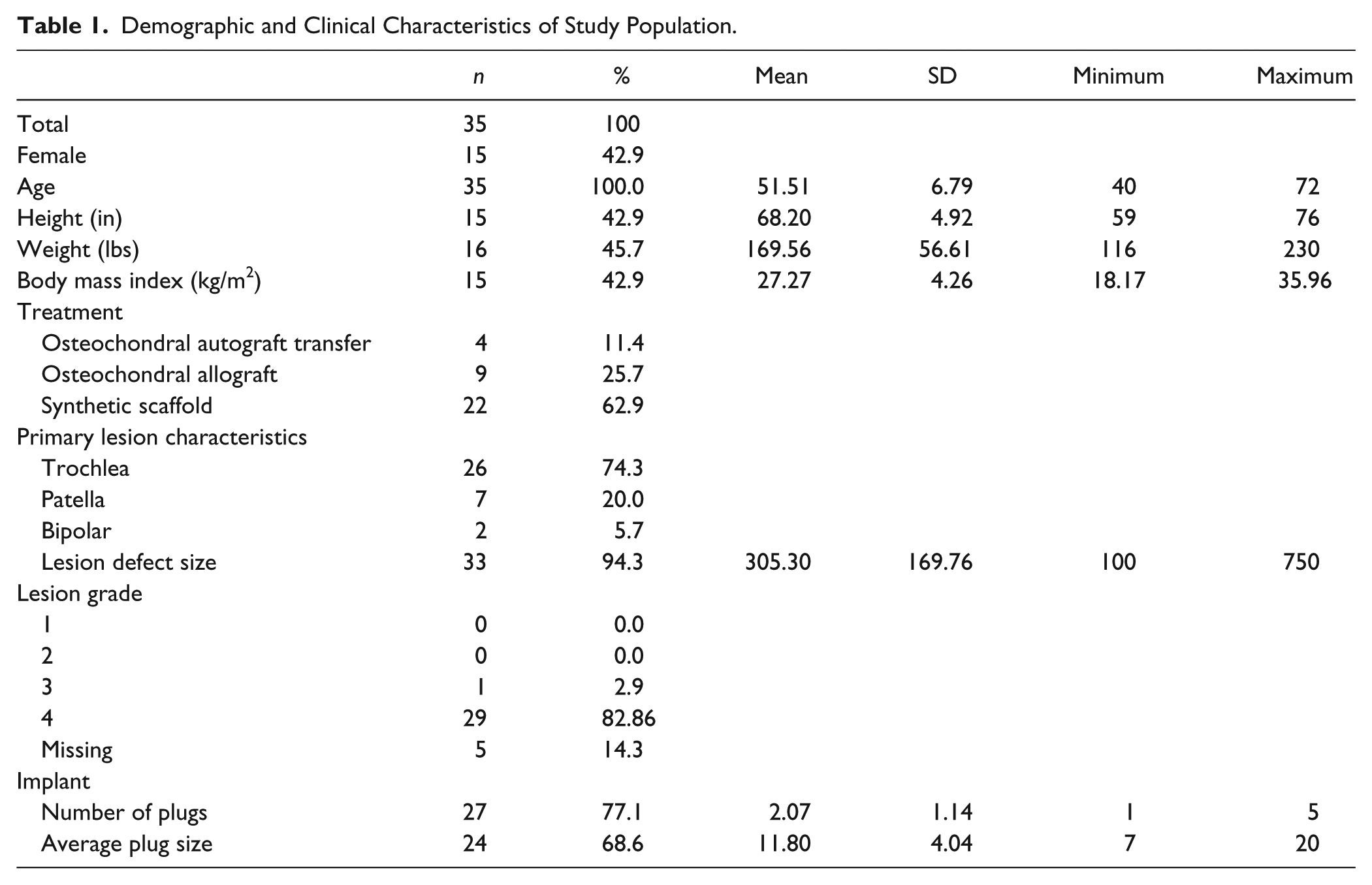
A total of 35 patients met all inclusion criteria. Seventeen patients had undergone surgery previously; 5 underwent arthroscopic debridement/chondroplasty, 3 received ligament reconstruction, 2 had partial meniscectomies, while surgical details were unknown for the remaining 7, although no distal realignment procedures were performed in these patients. Males comprised 57% (n = 20) of the cohort while 43% (n = 15) of patients were female. Mean age was 51.5 ± 6.8 years, and additional demographic information is summarized in Table 1 . Twenty-two (63%) patients were treated with SS plugs (OBI Trufit, Smith & Nephew, Andover, MA), 9 (26%) with fresh OCA plugs (MTF, Edison, NJ), and 4 (11%) with OAT. Twenty-six (74.3%) patients had primary trochlear lesions, 9 (25.7%) patients had primary patellar lesions, and 2 (5.7%) had bipolar lesions ( Table 2 ). All patients had minimum 2-year follow-up (average 3.6 ± 1.4 years). No patients experienced any intra- or postoperative complications.
Demographic and Clinical Characteristics of Study Population.
Demographics of Each Treatment Group, Including Lesion Location. a
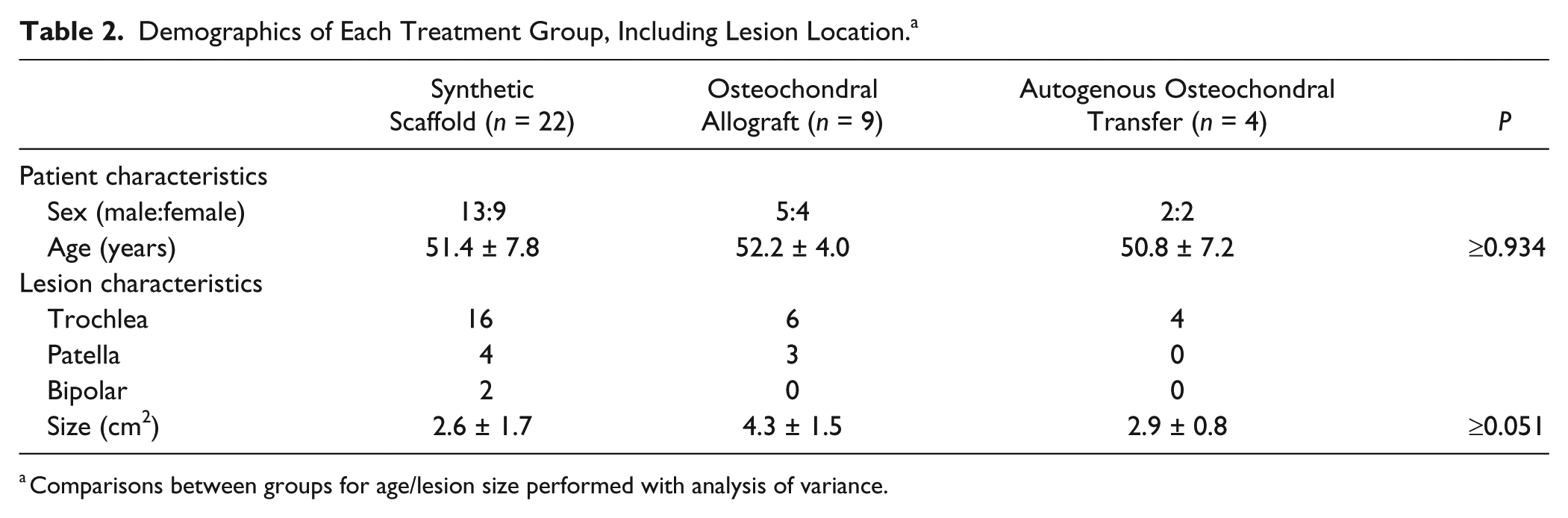
Comparisons between groups for age/lesion size performed with analysis of variance.
The average lesion size for the entire cohort was 3.1 ± 1.7 cm2. Average defect size was 2.6 ± 1.7 cm2 for the SS group, 4.3 ± 1.5 cm2 for the OCA group, and 2.9 ± 0.8 cm2 for the OAT group (P ≥ 0.051). Outcome scores for the entire population demonstrated significant improvement in ADL (P = 0.002) and IKDC scores (P = 0.004) between baseline and final follow-up, while MAS scores were maintained (P = 0.51) ( Fig. 4 ). It should be noted that there was a transient decrease in activity level in the year following treatment; however, the activity scores rebounded with no statistically significant differences between preoperative and final postoperative assessment. Further intergroup comparisons were not feasible as a post hoc power analysis revealed that we were underpowered for such comparisons (power ≤0.38). At the time of final follow-up, 5 patients (14.3%) required reoperation, with 4 undergoing conversion to a total knee arthroplasty and 1 requiring a manipulation under anesthesia for postoperative stiffness.
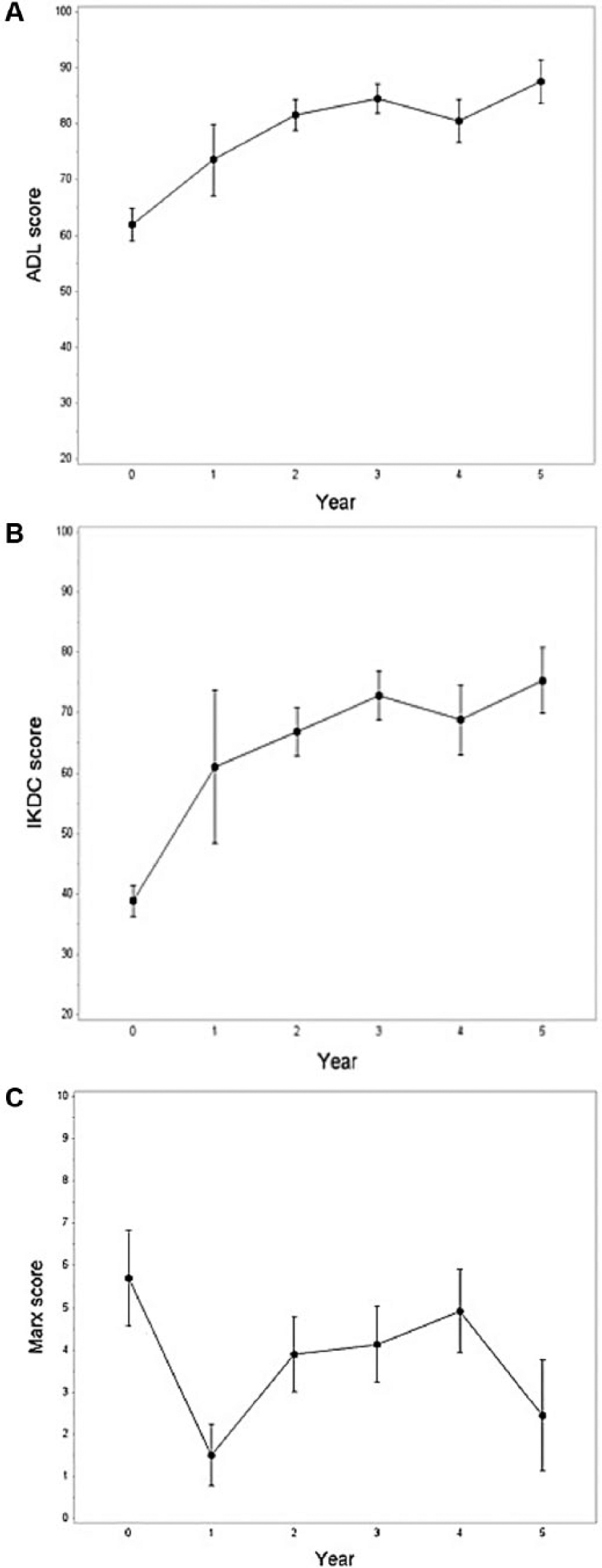
Clinical outcome scores for (
Discussion
Chondral and osteochondral lesions of the patella and trochlea are an especially difficult problem for patients and surgeons alike. In this study, we present clinical outcomes of patellofemoral cartilage restoration procedures in a population of patients older than 40 years. This study demonstrated improved functional outcomes at a minimum of 2 years following the use of structural grafting for the treatment of these osteochondral patellofemoral lesions. Ultimately, patients demonstrated significant early improvement in pain and function without loss of activity by multiple validated clinical outcome measures in this analysis. Accordingly, structural grafts appear to be a viable treatment option for this clinically challenging problem in patients older than 40 years. However, further recommendations on graft choice cannot be delineated from our results.
Noyes and Barber-Westin 10 recently reviewed the treatment of osteochondral lesions of the patellofemoral joint in patients younger than 50 years. In reviewing the outcomes of ACI, patellofemoral arthroplasty, and OCA implantation in several available clinical studies, they identified relatively unpredictable results, with moderately high failure rates. They concluded that they were unable to determine the ideal surgical treatment for these patients. As a result, the data from this study may aid in the treatment algorithm, particularly for patients older than 40 years, as relatively good results were observed, although follow-up duration was significantly shorter in our study (average 3.6 years vs. 6.2 years). Cartilage restoration techniques have not been widely studied in this patient demographic, particularly for use in the patellofemoral joint. The results of this study support cartilage restoration procedures in this cohort, particularly when compared with microfracture which has been shown to deteriorate at an unacceptably high rate 18 to 36 months following surgery in patients older than 40 years.11-13,29
Autogenous chondrocyte implantation has been used with some success in the patellofemoral joint. Pascual-Garrido et al. 16 reported significant improvements in their series of 52 patients at an average of 4 years postoperatively. In that study, the reoperation rate was 44% with a clinical failure rate (defined as requiring arthroplasty or OCA) of 7.7%. Biant et al. 30 reported a 27% failure rate with those patients requiring a revision surgery or arthroplasty at an average of 5.7 years after ACI for lesions at all locations. Despite this high failure rate, 98 out of 100 patients said they would have the procedure again. Rosenberger et al. 14 reported on a cohort of 56 patients with a minimum age of 45 years who were treated with ACI for cartilage lesions throughout the knee. The reoperation rate due to complications with the periosteal patch or arthrofibrosis was 43%. 14 Because of the unpredictable quality and quantity of lesion fill, the need for 2 procedures, high reoperation rate, and prolonged recovery (mean of 18 months to return to sport) compared with OAT (mean of 7 months), 31 we prefer structural grafting of cartilage lesions over ACI whenever possible.
Synthetic scaffolds have been sparingly used to treat patellofemoral osteochondral lesions. The only reported study was that by Joshi et al. 32 in 2012. They treated a cohort of 10 patients with full-thickness chondral defects of the patella, with an average age of 33 years, with the same synthetic scaffold plugs utilized in this study. Although their results demonstrated transient improvement in symptoms, they unfortunately noted significant clinical and radiographic deterioration by 24 months with a 70% reoperation rate. These results were not noted in our study. This difference in outcomes may relate to the overall differences in activity levels between patients given the difference in mean age, although the use of different outcome measurement tools precludes direct comparisons between these studies. Our results demonstrated improved clinical outcome scores, with maintained activity levels, although there was a decline in activity postoperatively, whereas patients in the study by Joshi et al. 32 returned to running and high-impact activities by 12 months. This transient decrease in MAS noted in our patients at 1 year may be functionally significant; however, patients can be encouraged that their activity levels should gradually return to their preoperative baseline with longitudinal follow-up.
OCA use in the patellofemoral joint has been extensively studied with several cohort studies identifying significant improvement in clinical outcome scores and survivorship of greater than 65% at 5-year follow-up in mixed cohorts of patients, although the mean age was <40 years.20-22 The results of our study demonstrate similar improvement in clinical outcome scores in an older population of patients, although follow-up duration was shorter than the aforementioned studies. Further follow-up of this cohort is important to determine longevity of these grafts in this population.
OAT results in hyaline cartilage repair at the center of the lesion with a predominance of type I collagen fibrocartilage at the periphery. It has been demonstrated to have good to excellent outcomes with a survival rate of 92% at 10 years. 33 When specifically used to treat patella lesions, Nho et al. 34 demonstrated significant improvements in their 22 prospectively followed patients at 4 years postoperation as assessed by Short Form–36, ADL, and IKDC scores. Astur et al. 19 also showed significant improvements in Lysholm, Kujala, and Fulkerson scores and excellent graft incorporation at 2 years’ follow-up in 33 patients with isolated patella lesions treated with OAT (average size ≤2.5 cm in diameter). We found similar functional improvements in our OAT group (average age = 50.8 years) with an average lesion size of 2.9 cm2.
Limitations of this study include a relatively small sample size, although it provides useful data on alternative cartilage restoration procedures in this population of older patients and aids in clinical decision-making. In addition, lack of randomization to the respective treatment groups limits introduces heterogeneity and limits comparison between outcomes of each group. The specific graft choice was determined by a single surgeon with significant expertise using the criteria of lesion size, location and patient specific factors. Allograft was favored for larger lesions, while OATs was initially performed for smaller defects and eventually replaced with off-label synthetic scaffold usage to minimize donor site morbidity. However, the patient demographics, including age and gender, were similar across all 3 treatment groups, and all treatment groups demonstrated significant improvement in outcomes from preoperative baseline, thereby supporting the primary study hypothesis. There were some differences in prior surgical procedures, which may influence outcome scores, although incomplete data made further analysis of these difficult. Additionally, we did not have information on the acuity of these osteochondral lesions and we cannot determine whether they resulted from an acute injury or represented early presentation of focal arthritic change. Finally, we did not have the ability to review preoperative radiographs for Fairbank’s changes or magnetic resonance imaging scans for chondral wear, as they were not available on all patients; however, intraoperative variables collected included grading of adjacent articular surfaces ensuring there were no significant chondral changes in these compartments (Outerbridge grade II or less).
Conclusion
Structural grafts are a viable treatment option for symptomatic focal osteochondral lesions of the patellofemoral joint in patients 40 years and older, with anticipated improvements in pain and function and maintenance of preoperative activity levels.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was obtained from The Hospital for Special Surgery INSTITUTIONAL REVIEW BOARD (Study # 2013-024-CR3).
Informed Consent
Written informed consent was obtained from all subjects before the study.
Trial Registration
Not applicable.