
Abstract
Objective
To standardize and to develop a fresh osteochondral allograft protocol of procurement, processing and surgical utilization in Brazil. This study describes the steps recommended to make fresh osteochondral allografts a viable treatment option in a country without previous fresh allograft availability.
Design
The process involves regulatory process modification, developing and establishing procurement, and processing and surgical protocols.
Results
Legislation: Fresh osteochondral allografts were not feasible in Brazil until 2009 because the law prohibited preservation of fresh grafts at tissue banks. We approved an amendment that made it legal to preserve fresh grafts for 30 days from 2°C to 6°C in tissue banks. Procurement: We changed the protocol of procurement to decrease tissue contamination. All tissues were procured in an operating room. Processing: Processing of the grafts took place within 12 hours of tissue recovery. A serum-free culture media with antibiotics was developed to store the grafts. Surgeries: We have performed 8 fresh osteochondral allografts on 8 knees obtaining grafts from 5 donors. Mean preoperative International Knee Documentation Committee (IKDC) score was 31.99 ± 13.4, improving to 81.26 ± 14.7 at an average of 24 months’ follow-up. Preoperative Knee Injury and Oseoarthritis Outcome Score (KOOS) score was 46.8 ± 20.9 and rose to 85.24 ± 13.9 after 24 months. Mean preoperative Merle D’Aubigne-Postel score was 8.75 ± 2.25 rising to 16.1 ± 2.59 at 24 months’ follow-up.
Conclusion
To our knowledge, this is the first report of fresh osteochondral allograft transplantation in South America. We believe that this experience may be of value for physicians in countries that are trying to establish an osteochondral allograft transplant program.
Keywords
Introduction
Fresh osteochondral allograft is an established procedure for the treatment of large osteochondral lesions of the knee joint with a history of more than a century since the first transplantation was done by Lexer in 1908. 1 Many surgeons in the United States and Canada have published their results of osteochondral allograft transplantation to treat a variety of pathologies such as posttraumatic defects, tumors, osteochondral defects, osteochondritis dissecans, osteonecrosis, and selective cases of degenerative disease of the knee.2-4 The favorable clinical results of this procedure has led to increasing popularity of fresh allograft transplantation. The inclusion of this procedure as part of the cartilage repair paradigm for the treatment of chondral or osteochondral lesions in the knee is routine in places where fresh allografts are readily available.
However, this procedure is not yet available for most countries in the world because numerous regulatory, logistical, and cultural issues have historically been difficult to overcome. Besides the United States and Canada, the Rizzoli Institute in Bologna, Italy has an established program of fresh osteochondral allografts and many surgeons outside North America would like to have this type of procedure available for repair of large osteochondral lesions of the knee. 5
Brazil is a country with 200 million inhabitants. Health care is mainly public and approximately 30% of the population has private insurance, which allows access to private hospitals, clinics, and physicians. The public health system is built in a pyramid model based on the complexity of the treatment. Hospitals responsible for complex cases are seldom affiliated with public universities where advanced treatment can be provided. The government regulates organ donation in Brazil and there are currently 5 musculoskeletal tissue banks nationwide. The objective of this study is to describe the development of a fresh osteochondral allograft protocol of procurement, processing, and surgical utilization in Brazil and to describe the steps recommended to make fresh osteochondral allografts a viable treatment option in a country without previous fresh allograft availability.
Methods
The process of starting a fresh allograft program involved approaching, analyzing, and proposing modifications in the regulatory process requiring legislation. Development and establishment of procurement, of tissue processing, and of transplantation protocols was also necessary.
Regulatory Analyses and Modification
We reviewed the regulatory process in conjunction with the Musculoskeletal Transplantation Bylaws Committee. We also analyzed the average time between the procurement and the release of musculoskeletal tissue in Brazil using Hospital das Clínicas Tissue Bank Database. Modification of the regulatory rules were prepared by the authors and proposed to the National Musculoskeletal Transplantation Bylaws Committee.
Procurement
We modified the procurement process routinely performed for bone and tendons procurement by our hospital. All tissues were harvested in a surgical operating room after heart, kidney, and liver donation in accordance with the Brazil Organ Donation Regulatory Act, which does not allow tissue to be harvested in clean rooms or morgues.
The procurement surgical technique was also modified. Before this protocol, the procedure was to harvest tendons and bone, opening the knee joint with an arthrotomy and dissecting the proximal tibia and distal femur from the surrounding soft tissue for later processing at the tissue bank. The change preserved the articular cartilage by removing the whole knee joint without violation of the articular cartilage for later processing at the tissue bank.
Processing
We standardized the processing protocol for the grafts in order to perform the transplantation within 12 hours of harvesting. Tissue processing was performed in a clean room (ISO 5 class) following Good Manufacturing Practice (GMP) conditions. We performed cytotoxic tests of cartilage samples preserved for 30 days in storage in a serum free media GIBCO Ham-F12 with GlutaMAX and antibiotics (Invitrogen, Life Technologies) to determine if the proposed media was safe. Samples were tested after incubation analyzing macroscopically and microscopically the zone index reaction in clone 929 cells (ATCC CCL-1).
Surgical Protocol and Transplantation
Patients from 15 to 45 years old with osteochondral lesions larger than 4 cm2 were included in this study. Patients who suffered from inflammatory disease of the joint, smokers, and patients with tricompartmental knee arthritis were excluded from the protocol. Radiology examinations were performed to determine the size and location of the osteochondral defect. The proximal tibia medial-lateral width was measured on the anteroposterior knee radiography film. Potential recipients signed an informed consent and were listed with the tissue bank. Information provided included weight, height, size of the proximal tibia, and location and size of the defect.
All surgical procedures were scheduled for the day after laboratory tests would be released. Patients were admitted on the day of the surgical procedure and the knee was approached with a lateral or medial parapatellar arthrotomy, depending on the location of the defect. Alignment and stability of the limb were accessed prior to the surgery. Osteotomies and ligament reconstructions were performed in advance or simultaneously with the allograft procedure.
Two surgical techniques were used in this protocol: osteochondral dowel and shell techniques. The osteochondral dowel technique was used for contained medial and lateral femoral lesions with sizing dowels from 15 to 30 mm ( Fig. 1 ). Shell technique was used for uncontained femoral condyle, trochlea, tibial plateau, and patellar lesions as described by Bugbee et al. 6 ( Fig. 2 ). Fixation was used when necessary with metallic 3.0-mm cannulated screws.
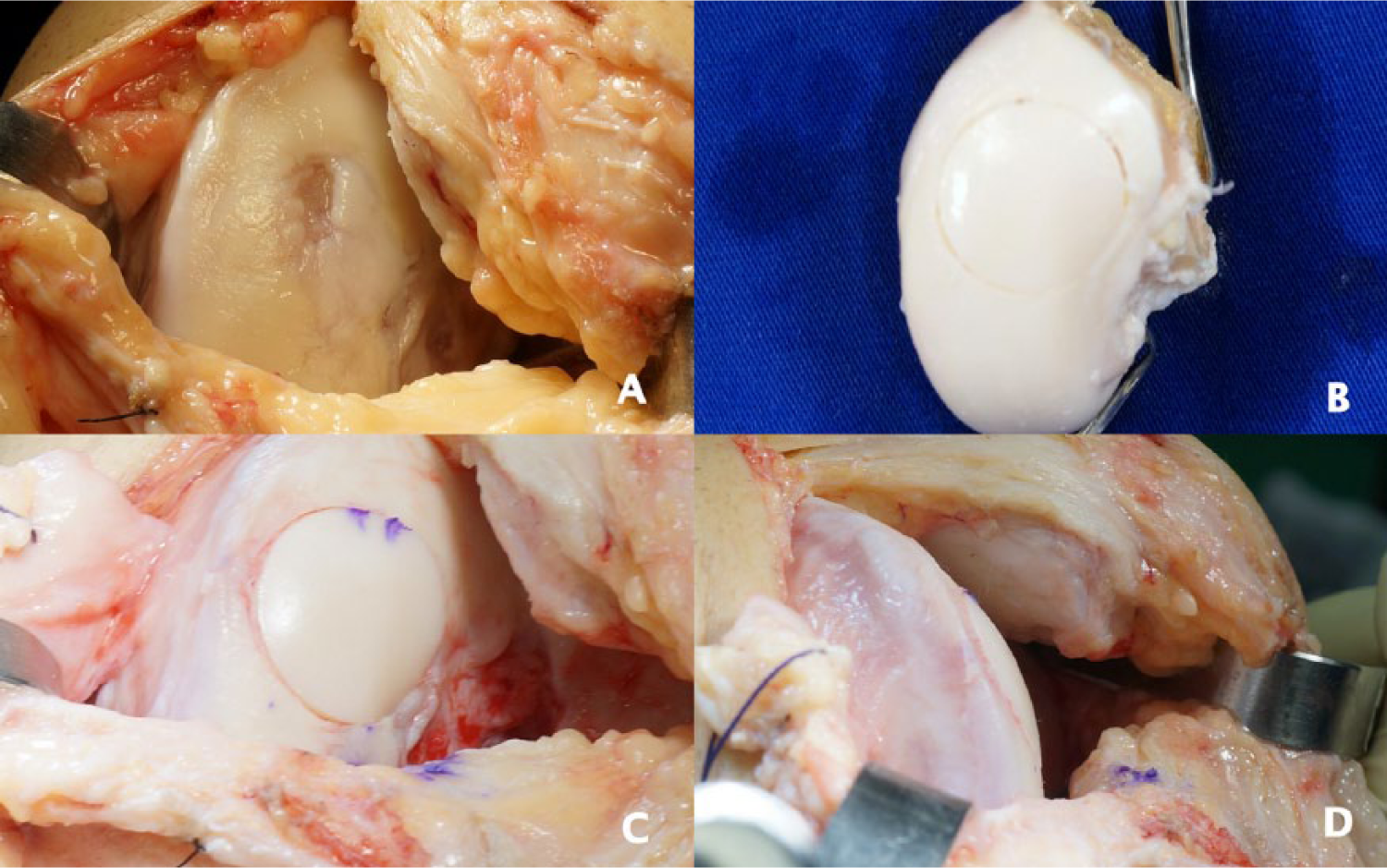
(
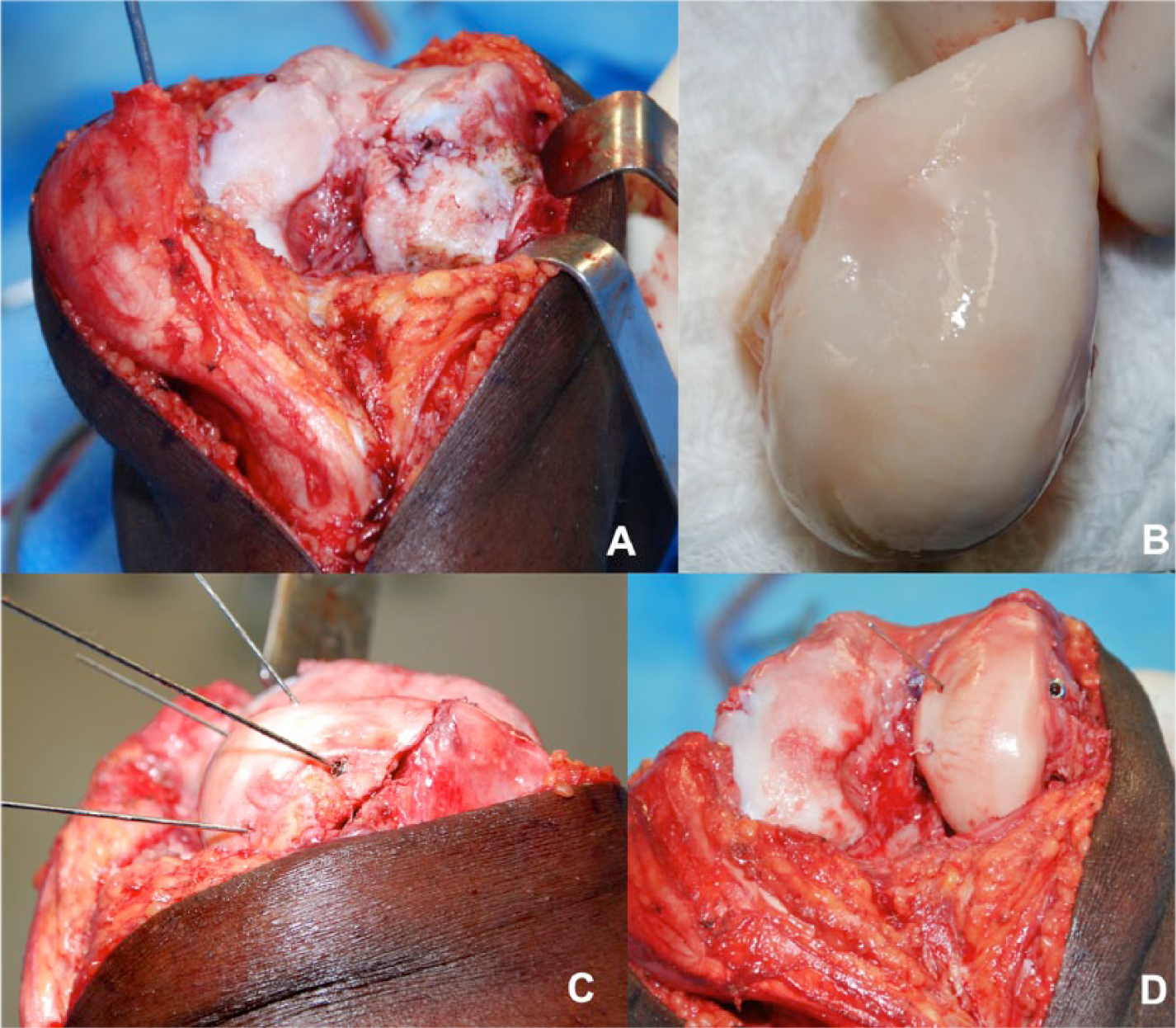
(
Statistical Analysis
Clinical outcomes of all patients were analyzed using the International Knee Documentation Committee (IKDC) subjective scores, the Knee Injury and Osteoarthritis Outcome Score (KOOS) score and the modified Merle-D’Aubigne Postel questionnaire comparing preoperative and 24 months postoperative results. All results were tested for distribution with Komogorov-Smirnov test. Subjective IKDC and KOOS score showed normal distribution and the 1-way analysis of variance and the Bonferroni post hoc test were used to compare preoperative and postoperative results. Modified Merle-D’Aubigne Postel test show nonnormal distribution and the related measures Friedman test and the post hoc Wilcoxon test were used for comparison of preoperative and postoperative results. For all tests P < 0.05 was considered significant. Intention-to-treat analysis was used and lost to follow-up data was analyzed using worst-case scenario strategy. Data analysis was performed using SPSS 20.0 software for MAC (IBM Corp, Armonk, NY, USA).
Results
Regulatory Analyses and Modification
A protocol of fresh osteochondral allografts was approved by the Scientific Committee of the Orthopedic Department, Hospital das Clínicas, based on the experience of the United States and Canada with fresh osteochondral allografts. This protocol was presented by the authors to the national regulatory committee of tissue banks as an amendment to change the regulatory process. This amendment proposed that preservation of fresh musculoskeletal grafts at 2°C to 6°C in a storage media for up to 30 days be made legal. The regulation regarding musculoskeletal tissue was modified on October 21, 2009 allowing fresh osteochondral allografts to be stored in tissue banks for orthopedic procedures in Brazil.
Procurement
All osteochondral tissues were harvested in a surgical operating room after heart, kidney, and liver donation. Harvesting technique was modified in order to preserve the articular cartilage by removing the whole knee joint without violation of the articular cartilage and to avoid tissue contamination ( Fig. 3 ). The knee joint was harvested with a femoral osteotomy 10 cm above the joint line and a tibial and fibular osteotomy 2 cm below the most distal aspect of the anterior tibial tuberosity without violation of the articular knee capsule. The whole knee joint was stored at 2°C to 10°C in a triple-sealed package with ringer lactate and was transported to the university tissue bank for processing. All tissues were procured in an operating room within 12 hours of donor death.

(
Processing
The knee joint was removed from the triple package and a medial parapatellar arthrotomy was done preserving the extensor mechanism. Soft tissues were removed in order to preserve the distal femur, proximal tibia, and lateral and medial meniscus bodies and the insertions on the tibia. A caliper was used to measure the lateral-medial width of donor’s proximal tibia in millimeters and this was combined with sex, weight, and height of the donor. A list of patients who needed fresh allograft transplantation was available and matching was obtained in the following cases:
Femoral condyle lesions: Matching was obtained when the measurement of the proximal tibia of the donor was equal or larger than the recipient.
Tibial plateau, trochlea, and patella lesions: Matching was obtained when the measurement of the proximal tibia of the donor was equal or maximum 2 mm greater or smaller than the recipient.
After debridement of soft tissue and processing, tissue samples were taken for microbiological tests and the grafts were stored in a commercial serum-free culture media with antibiotics in 4°C until all the tests were released.
Preservation media was composed by Ham F-12 GIBCO with Glutamax containing amino acids and vitamins, adding 12.5 mg of amphotericin b, 25 mg of gentamicin, 5,000,000 IU of penicillin and 50 mg of streptomycin sulfate. Cytotoxicity analyses demonstrated negative results for toxic effect on clone cell 929 (ATCC CCL-1) after 30 days of storage.
Surgical Protocol and Transplantation
We have performed 8 fresh osteochondral allografts transplantation surgeries on 8 knees for the treatment of osteochondral lesions from March to October 2012. Patients received the osteochondral allograft transplantation at an average of 15.3 days from donor tissue harvesting (range from 14 to 16 days). The cohort included four males and four females, with a mean age of 30.1 years (range 17-44 years) and average lesion size of 10.6 cm2 (range 4.6-22.4 cm2).
Six lesions were on the femoral condyle (2 lateral and 4 medial), 1 medial tibial plateau (with meniscus), and 1 patella. Preoperative diagnoses was osteochondritis dissecans in 5 patients, posttraumatic defects in 2 patients and osteonecrosis following chemotherapy for leukemia during childhood in 1 patient ( Table 1 ). All patients had a minimum follow-up of 2 years. Four (50%) of 8 patients had further surgical procedures after the osteochondral allograft implantation. Three patients were operated for implant removal and 1 patient was considered to be a clinical failure.
Patient Information.
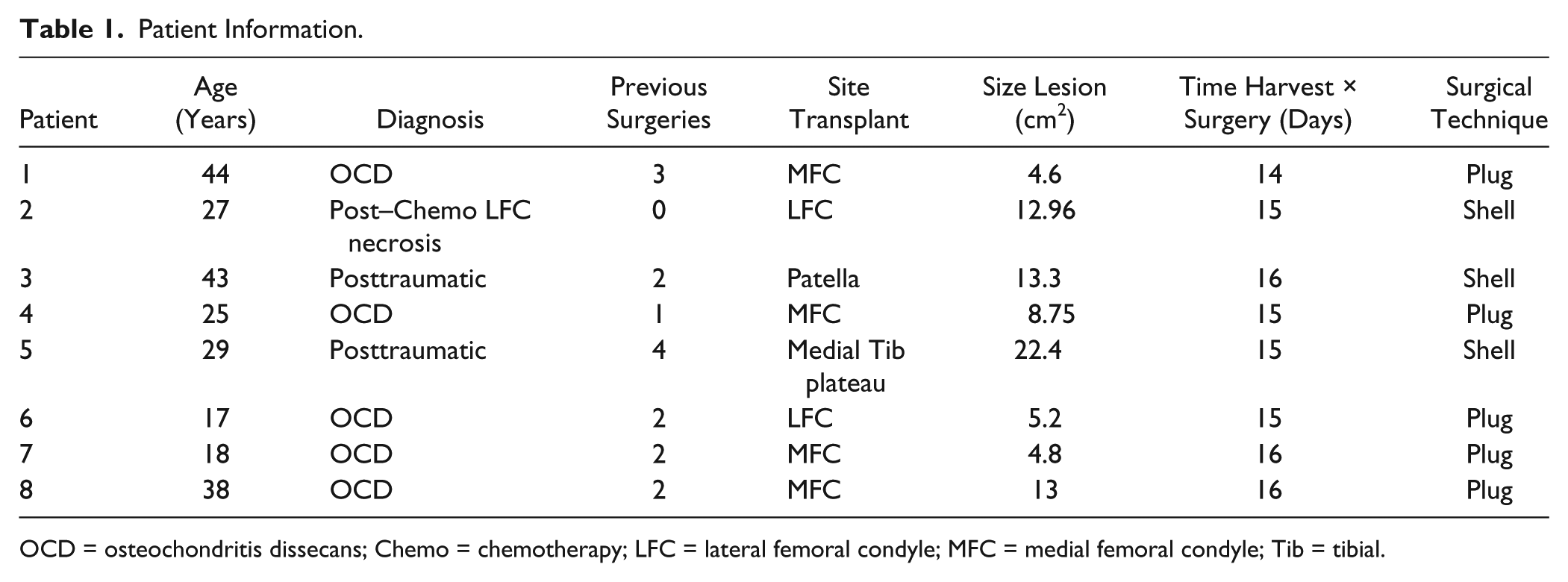
OCD = osteochondritis dissecans; Chemo = chemotherapy; LFC = lateral femoral condyle; MFC = medial femoral condyle; Tib = tibial.
One patient had a previous knee infection after tibial plateau surgery 3 years prior to the allograft surgery. He was asymptomatic at the time of the transplantation and blood analyses (C-reactive protein, erythrocyte sedimentation rate, and leukogram) were normal. Three months after a tibial plateau allograft with meniscus repair, he fell off of a motorcycle with a blunt trauma to his knee and developed an acute infection progressing to failure of the graft.
Mean subjective IKDC score was 31.99 ± 13.4 preoperative and 81.26 ± 14.7 after 24 months’ follow-up. Mean KOOS score preoperative was 46.8 ± 20.9 and 24 months postoperative was 85.24 ± 13.9. Mean preoperative Merle D’Aubigne-Postel score was 8.75 ± 2.25 and at 24 months’ follow-up the score was 16.1 ± 2.59 (Table 2).
Clinical Results.
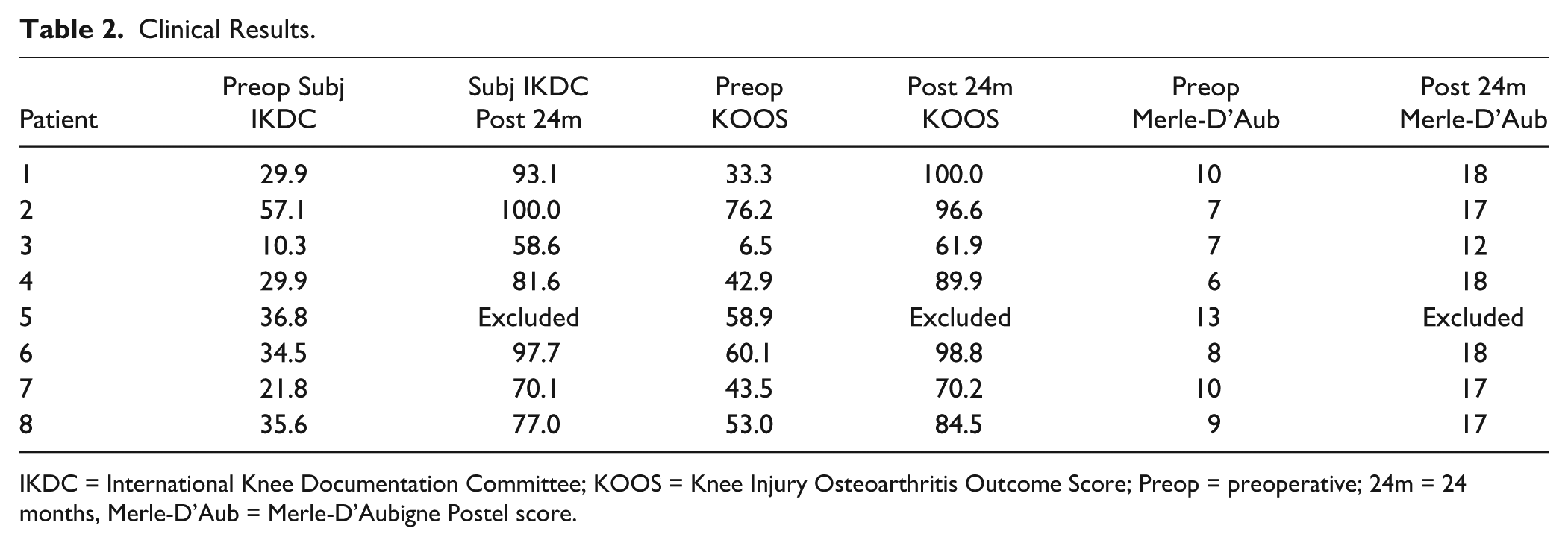
IKDC = International Knee Documentation Committee; KOOS = Knee Injury Osteoarthritis Outcome Score; Preop = preoperative; 24m = 24 months, Merle-D’Aub = Merle-D’Aubigne Postel score.
Discussion
The current study represents the first report of fresh osteochondral allograft transplantation in South America. Prior to this study most of the young patients that suffered from large osteochondral lesions of the knee were elected for total knee arthroplasty, because fresh osteochondral allografts and chondrocyte transplantation were not available for treatment in orthopedics.
Every country has unique regulations that need to be considered, depending on whether the health care system is public or private. There is not a single article in the literature that reports how to establish a protocol for a fresh osteochondral allograft program in a country where the procedure is not yet available. The greatest challenge in this study, in our opinion, was getting the approval of an amendment to the law making fresh allografts legal in Brazil allowing us to treat young patients with large osteochondral lesions. Association and knowledge exchange with an existing university-affiliated tissue bank facilitated setting up a fresh allograft program outside the United States.
The university hospital tissue bank in Hospital das Clínicas in São Paulo is responsible for the biggest national distribution of musculoskeletal tissues throughout the country. One of the tissue bank’s members serves on the bylaw committee that regulates national tissue banks, which facilitated the regulatory process modification.
Since this was the first work with fresh osteochondral allografts in Brazil, we have only included patients from 15 to 45 years old who suffered traumatic or acquired injuries of the knee with lesions larger than 4 cm2. We excluded patients with degenerative diseases, despite the fact that many authors describe allografts in older and younger patients.7,8
All grafts were obtained from organ donors in an operating room after heart, kidney, and liver donation, which differs from the study of Vangsness et al. 9 where only 33% of the procurement took place exclusively in an operating room. Procurement of grafts in morgues, coroner’s facilities or tissue banks is not currently possible in Brazil. This fact limits the number of grafts available for transplantation.
As organ donation for frozen grafts is routine in our country, we had to change the way grafts were harvested and stored so osteochondral grafts could be stored and used as fresh grafts refrigerated at positive temperatures. The main change in the protocol was to harvest the whole joint intact to try to decrease the rate of contamination instead of doing an arthrotomy and exposing the articular surface.
Tissue grafts were sent immediately to the tissue bank and processing occurred within 12 hours of donation. This contributed to the very short time between donation and transplantation (15.3 days), which could contribute for a higher percentage of live chondrocytes when compared with grafts stored for longer periods. Another factor that contributed to this short period of transplantation was that all tissues were harvested in the state of São Paulo, within 150 km from the tissue bank, decreasing the time between donation and processing.
Transplantations were performed with dowel and shell surgical techniques. Instrumentation sets for dowel techniques were not available in the country, so we had to design a set of instruments with a local company to perform the surgical steps for osteochondral plugs. The size of the donor plug should be equal or 1 mm smaller in diameter than the recipient defect. However, our set was a little loose in the beginning, so we had to use a central 3.0 mm Herbert screw in 3 cases in order to fixate the graft. These screws were removed arthroscopically in all 3 cases 12 weeks after transplantation.
Evaluation of all outcome scores (IKDC, KOOS, and Merle D’Aubigne-Postel) improved significantly at 24 months postoperative follow-up (P < 0.05). One patient had a recrudescent infection from a tibial plateau fracture three months after transplantation with graft failure. Radiographic images of all other patients showed incorporation of the grafts without formation of cysts or collapse of the grafts. Patients returned to daily life activities and to low-impact sports. Level of satisfaction with the procedure was high among all patients.
The limitations of the current study include a small sample size, a relatively short time of follow-up, and no control group. Another limitation is that different surgical techniques were evaluated combined, including both dowel and shell techniques, which may have different outcomes due to size and technical issues. Simple and complex salvage procedures were not distinguished in the data analyses due to the small sample size.
We conclude that developing a fresh osteochondral allograft program is feasible and involves several levels of approach. Although being a difficult task, developing an osteochondral allograft program can be accomplished if organ donation and tissue banks are available in the country. The low rate of infection and failure in this small study supports our procurement and testing protocol. Although results of this preliminary study are encouraging, an increase in graft availability is required to disseminate this procedure countrywide.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was obtained from Ethics and Research Project Committee – CAPPesq – Hospital das Clinicas da FMUSP – N° Protocol: 0308/10.
Informed Consent
Written informed consent was obtained from all subjects before the study.