
Abstract
Objective
Treatments for steroid-induced osteonecrosis of the knee remains challenging, and there has not been sufficient evidence to support joint preservation surgery. This study evaluated long-term outcomes of osteochondral autologous transplantation (OAT) for steroid-induced osteonecrosis of the knee.
Design
This retrospective case series included patients who underwent OAT for steroid-induced osteonecrosis of the knee from 1998 to 2008. The survivorship and need for secondary surgery were evaluated, and the clinical outcome was evaluated with the International Knee Documentation Committee (IKDC) subjective score. Preoperative and final Kellgren-Lawrence (KL) grade of the femorotibial and patellofemoral joints were individually evaluated.
Results
Fourteen knees of 10 patients whose mean age was 32.5 (95%CI 26.4-38.6) years were included and followed for 14.0 (12.4-15.7) years. The mean lesion size of 6.9 (5.3-8.5) cm2 was repaired using 4 median (minimum 2, maximum 5) osteochondral plugs. No revision surgeries were performed for transplanted osteochondral plugs. The IKDC subjective score improved from 32.9 (24.5-41.3) to 74.2 (61.9-88.5) (P < 0.001). Knee flexion was improved at the final follow-up, and Seiza sitting was finally possible in 9 knees in 7 patients. Although the osteoarthritic change did not progress in femorotibial joint, patellofemoral joint showed early osteoarthritic changes at the final follow-up (mean KL grade: 0.8 [0.5-1.1]).
Conclusions
Prosthetic joint replacement was successfully avoided for at least the first decade by OAT in young patients with steroid-induced osteonecrosis of the knee. The progression of KL grade of the patellofemoral joint is of concern.
Introduction
Osteonecrosis includes 2 distinct entities: one is the osteonecrosis secondary to the subchondral bone insufficiency fracture, which typically occurs in older patients and usually involves one condyle with limited lesion sizes; the other is osteonecrosis secondary to vascular insufficiency in subcortical bone and bone marrow, which often involves young active patients with large lesions.1-3 Among latter, steroid is the most common cause. 3 Corticosteroid-induced osteonecrosis of the knee, which is a serious side effect after high-dose corticosteroid therapy for autoimmune disorders, organ transplantation, or malignancy, is an uncommon disease that severely impairs the patient’s quality of daily living. 4 The most common site of the corticosteroid osteonecrosis is the femoral head, followed by the knee. 5 More recently, magnetic reasoning imaging (MRI) confirms up to 55% of patients with steroid-induced osteonecrosis of the femoral head also have osteonecrosis of the knee. 6 It means that the involvement of the knee is not negligible, and adequate treatment should be considered.
The treatment of the steroid-induced osteonecrosis of the knee is still challenging. Conservative approaches are initially considered and occasionally successful for patients with small lesions; however, nonoperative treatment is associated with a high clinical failure rate.7,8 Although total knee arthroplasty (TKA) is a good treatment option, knee prostheses are less desirable in young and active patients.2,9,10 Joint preservation surgeries, including core decompression, 8 impaction bone grafting, 11 and osteochondral allograft transplantation,12,13 have been performed for young patients. Osteochondral autologous transplantation (OAT) is one of the most common surgical treatments for cartilaginous and osteochondral disease, and good clinical results have been reported for the treatment of diseases, including corticosteroid-induced osteonecrosis of the knee,14,15 as well as focal cartilages lesion, osteochondritis dissecans, and various kind of osteonecrosis of the knee, ankle, elbow, and hip joint.16-22 However, long-term effectiveness or problems of OAT for corticosteroid-induced osteonecrosis of the knee remains unknown. Thus, in this study, the long-term outcomes of OAT for corticosteroid-induced osteonecrosis of the knee with regard to longevity and clinical outcomes were evaluated. We hypothesized that OAT could be used to successfully avoid or postpone prosthetic replacement in young patients with corticosteroid-induced osteonecrosis of the knee.
Methods
This retrospective case series received approval from the ethics committee of our hospital and performed in line with the Helsinki Declaration. Due to the study design, informed consent was waived and opt-out was offered. The patients who underwent OAT for corticosteroid-induced osteonecrosis of the knee between 1998 and 2008 were included. The osteonecrosis was diagnosed by plain radiography, computed tomography (CT), and MRI. Anteroposterior, lateral, and skyline plain radiographs were routinely taken to evaluate the location and severity of the osteochondral lesions. An anteroposterior long-leg radiograph was also taken to evaluate the long leg alignment. The size and depth of the subchondral bone lesions were evaluated by CT, and MRI was used to evaluate the extent of reactive inflammation in the bone marrow as well as the conditions of the cartilage, ligaments, and meniscus. The indication for OAT were as follows: patients who had extensive osteochondral lesions in the single condyle or in the single condyle and patellar groove, who were irresponsive to conservative treatment, and who were young or unwilling to undergo joint replacement surgery. If the femorotibial angle (FTA) was 170° or less, or 180° or more, or if the weightbearing line passed the necrotic lesion in the long leg radiograph, realignment osteotomy was considered. Contraindication of OAT included the following: the coexistence of necrotic lesions in both medial and lateral condyles, knees with ligament abnormalities, large exposure of subchondral bone in the opposite tibia, or end-stage osteoarthritis with Kellgren-Lawrence (KL) grade 4.
Surgery
The key concept of the OAT surgery was to replace necrotic bone with fatty marrow by autologous osteochondral plugs containing healthy subchondral and cancellous bone with hyaline cartilage on the top, which had the similar mechanical properties to surrounding cartilage. All surgeries were performed under general anesthesia. The diagnostic arthroscopy was performed at first to confirm that the location and size of the lesions were adequate for OAT. The medial or lateral parapatellar approach was used according to the location of the lesions. After removal of necrotic tissue, OAT was performed using the Osteochondral Autograft Transfer System (OATS; Arthrex, Naples, FL) with the open technique using the nonweightbearing area of the medial and/or lateral trochlea of the ipsilateral femur as donor sites. 23 When normal cartilage remained on the lesion, the recipient osteochondral plug was harvested through the cartilage, and necrotic tissue was removed through the hole of recipient plug. 24 The depth of the lesions was carefully evaluated using MRI preoperatively, and the depth of the graft was at least 5 mm deeper, beyond the necrotic zone. The maximum number of osteochondral plugs harvested were 3 plugs from the lateral trochlea and 2 from the medial trochlea. We allowed a 3-mm interval between the plugs to cover the whole single condyle using the plugs from the ipsilateral femur. The operated knee was not immobilized, and after removal of the drain on postoperative day 2, range of motion rehabilitation by a physical therapist and with continuous passive motion was initiated. Weightbearing was prohibited for 3 weeks, and full weightbearing allowed at 7 weeks postoperatively.
Clinical Evaluations
The range of motion of the knee was measured before surgery and at the final follow-up with handheld goniometer. With plain radiographs, the preoperative and final KL grades of the femorotibial (FT) and patellofemoral (PF) joints were individually evaluated in order to detect the occurrence or progression of osteoarthritis. The International Knee Documentation Committee (IKDC) subjective score 25 and the Japanese Orthopaedic Association score for knee osteoarthritis (JOA knee score) 26 were used to evaluate the clinical outcomes before surgery and at the final follow-up.
Statistics
The survivorship of OAT was evaluated with the revision surgery for the transplanted cartilage and with any additional surgeries on the affected knee as an endpoint using the Kaplan-Meier method. To compare preoperative and final range of motion and FTA, the paired t test was used. To compare pre-operative and final KL grades, the IKDC subjective score, and JOA knee score, Wilcoxon matched-pair signed-rank test were used. To evaluate for the factor that affected the clinical outcome, the associations of age at surgery, lesion size, period after surgery, number of multifocal osteonecrosis, KL grade, to IKDC subjective score were determined with simple linear regressions. The IKDC subjective score between knees from systemic lupus erythematosus (SLE) and these of other primary diseases was compared using the Mann-Whitney U test. Data are shown as mean with 95% confidence intervals or median with range, and P values <0.05 were considered significant.
Results
There were 14 knees of 10 patients that met the inclusion criteria. The mean age at the time of surgery was 32.5 years (26.4-38.6 years). Primary diseases included SLE in 5 knees of 3 patients, idiopathic thrombocytopenic purpura in 3 knees of 2 patients, Nephrotic syndrome in 3 knees of 2 patients, leukemia in 1 knee, IgA syndrome in 1 knee, and relapsing polychondritis in 1 knee. A considerable dose of corticosteroid was used for all patients (≥30 mg/d prednisolone). The duration of steroid usage before OAT was 6.9 years (4.5-9.2 years). The patients’ demographic data are shown in Table 1 . FTA ranged from 174° to 179°, and no concomitant surgeries, such as meniscectomy or osteotomy, were performed in these cases.
Demographics of the Patients of Corticosteroid-Induced Osteonecrosis.
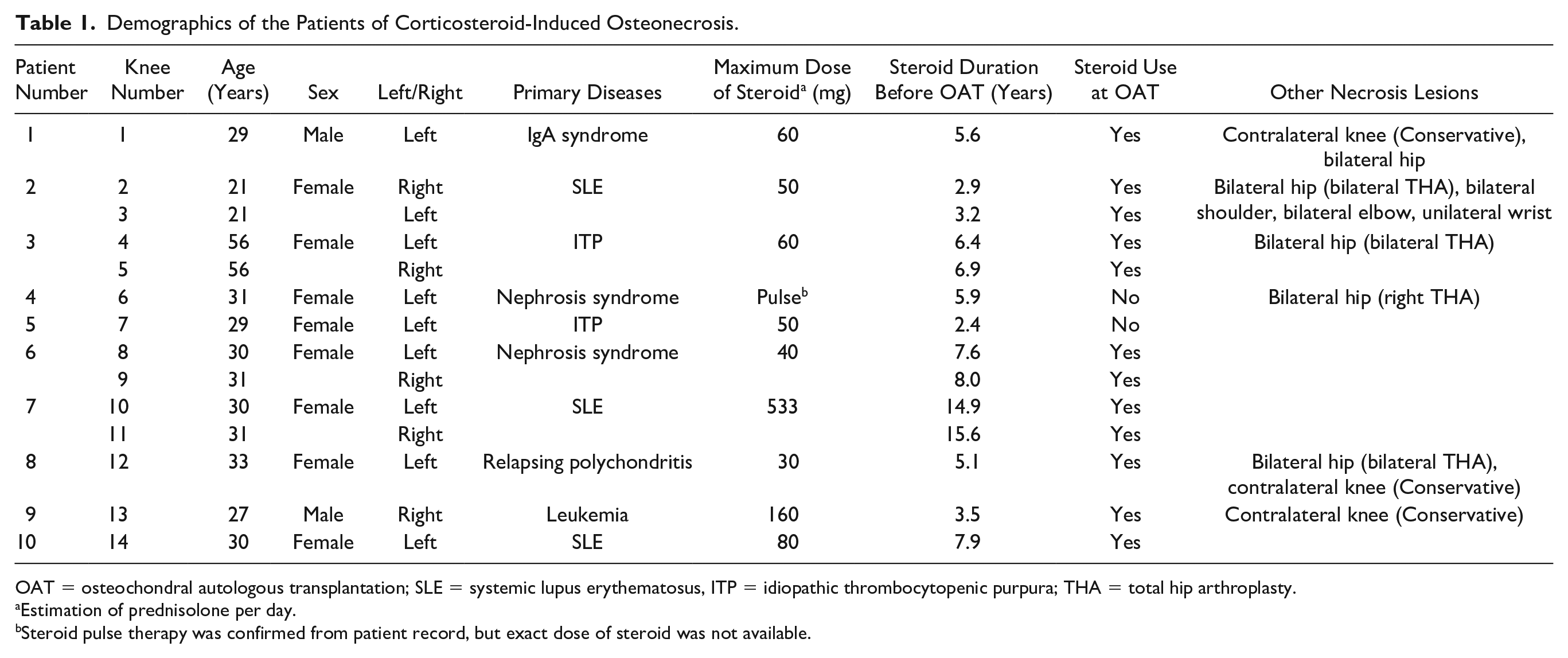
OAT = osteochondral autologous transplantation; SLE = systemic lupus erythematosus, ITP = idiopathic thrombocytopenic purpura; THA = total hip arthroplasty.
Estimation of prednisolone per day.
Steroid pulse therapy was confirmed from patient record, but exact dose of steroid was not available.
The osteochondral lesions were located in the lateral femoral condyle (LFC) in 8 knees, medial femoral condyle in 3 knees, MFC and patellar groove in 2 knees, and LFC and patellar groove in 1 knee. The average lesion size of 6.9 cm2 (5.3-8.5 cm2) was repaired using median 4 (minimum 2, maximum 5) osteochondral plugs whose median diameter was 8.0 mm (minimum 6, maximum 10 mm). There were no patients lost to follow-up and all patients were followed-up for more than 10 years (mean 14.0 years [12.4-15.7 years]) ( Table 2 ).
Condition of the Knee at OAT and Follow-up.
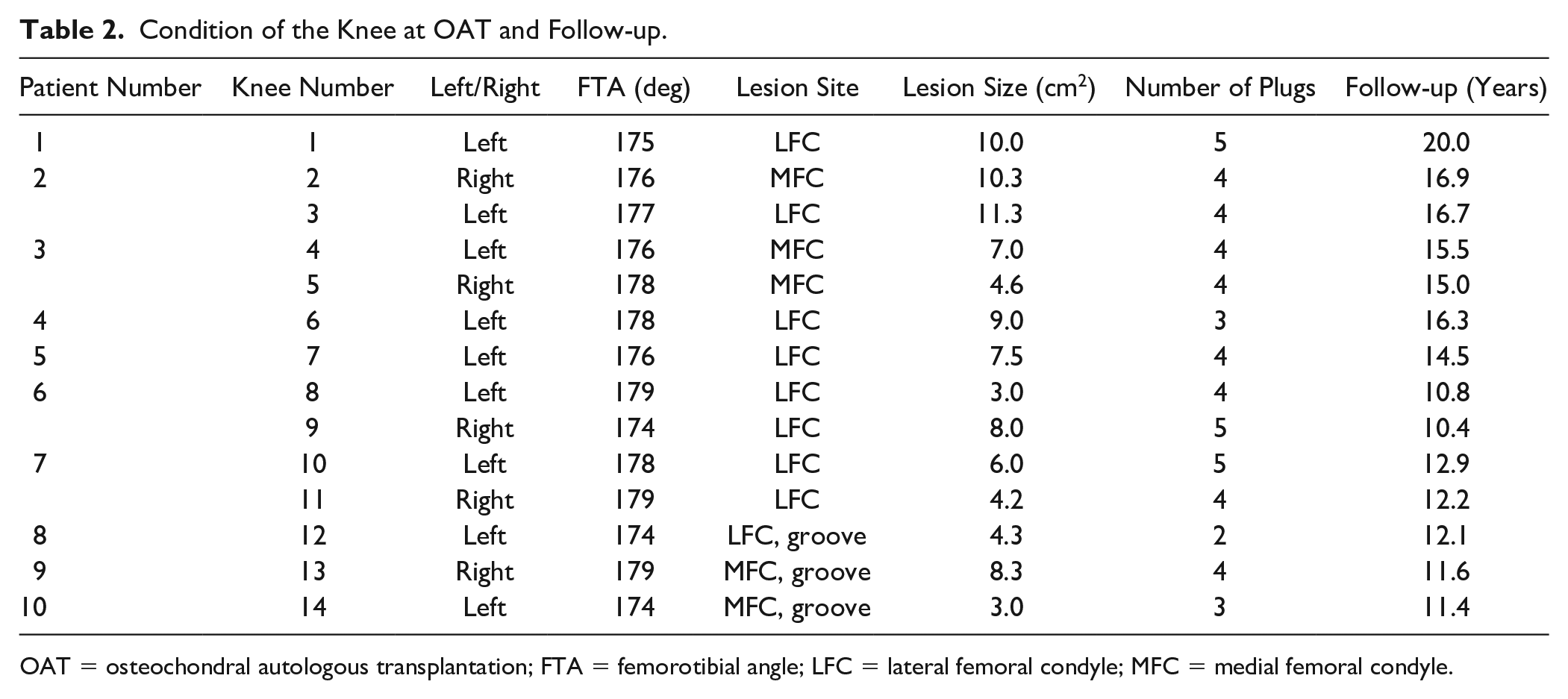
OAT = osteochondral autologous transplantation; FTA = femorotibial angle; LFC = lateral femoral condyle; MFC = medial femoral condyle.
With the revision surgery on the transplanted cartilage as an endpoint, the survival rate was 100% at 10 years ( Fig. 1A ). One case underwent arthroscopic removal of a loose body at 96 months, and when any surgery on the affected knee was considered an endpoint, the 10-year survival rate was still 92% ( Fig. 1B ). There were no cases who converted to a prosthetic joint during follow-up.
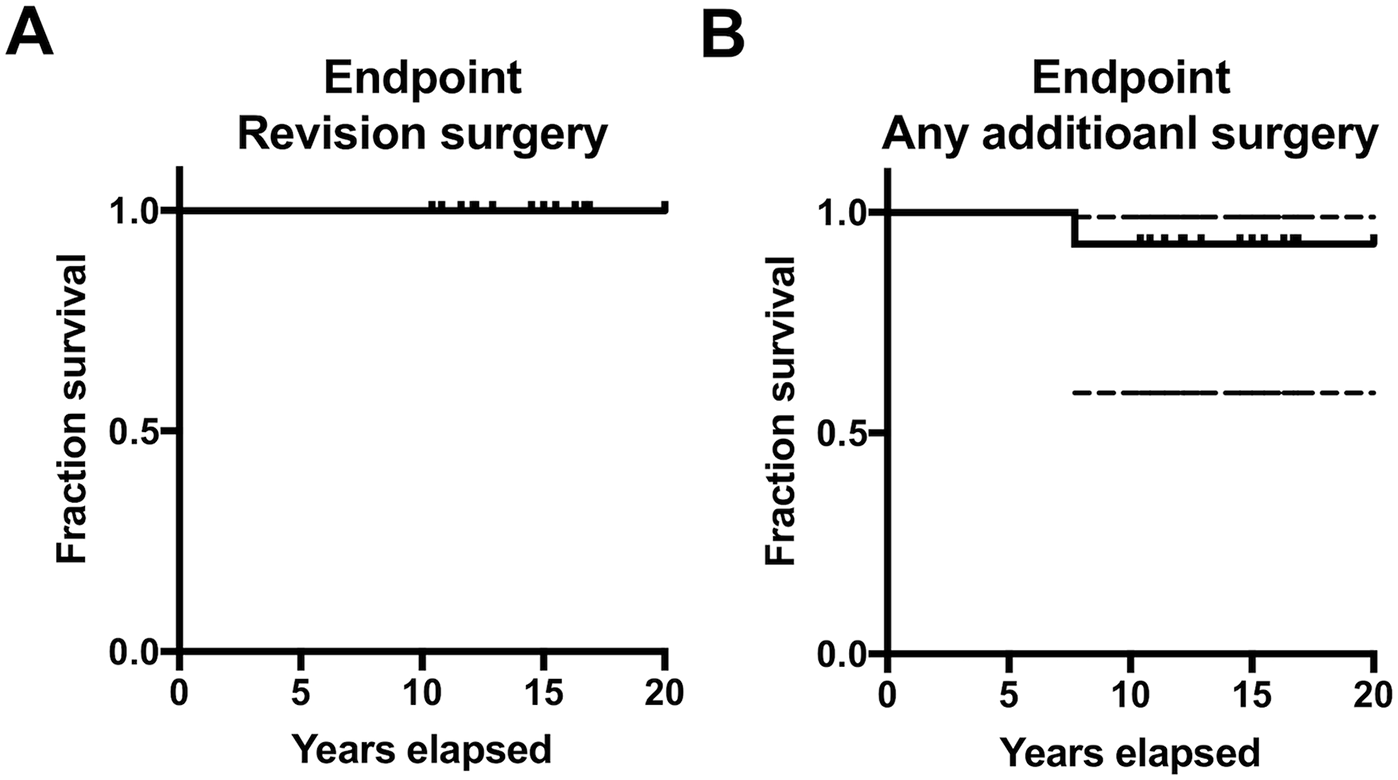
Graphs of Kaplan-Meier method with revision surgery on the transplanted cartilage as the endpoint (
Knee flexion improved from 134° (130° to 139°) to 144 (140° to 147°) at the final follow-up (P = 0.002), and Seiza sitting was possible in 9 knees in 7 patients. The IKDC subjective score improved from 32.9 (24.5-41.3) to 74.2 (61.9-88.5) (P < 0.001), and the JOA knee score also improved from 62.9 (58.0-67.8) to 87.9 (77.9-97.8) (P = 0.001) ( Fig. 2 ). FTA did not change by the final follow-up (preoperative: 176.6° [175.5° to 177.7°], final follow-up: 176.9 [175.7° to 178.0°]). The KL grade of the tibiofemoral joint that was not deteriorated at the final follow-up (preoperative mean: 1.1 [0.6-1.7], final follow-up mean: 1.4 [0.7-2.2]) (P = 0.31) ( Fig. 3A ). On the other hand, there was no arthritic change before surgery in the PF joint (mean KL grade: 0 [interquartile range 0-0]), the early osteoarthritic change was observed at the final follow-up (mean KL grade: 0.8 [0.5-1.1]) (P = 0.002) ( Fig. 3B ). No cases complained of donor site symptoms at the final follow-up.
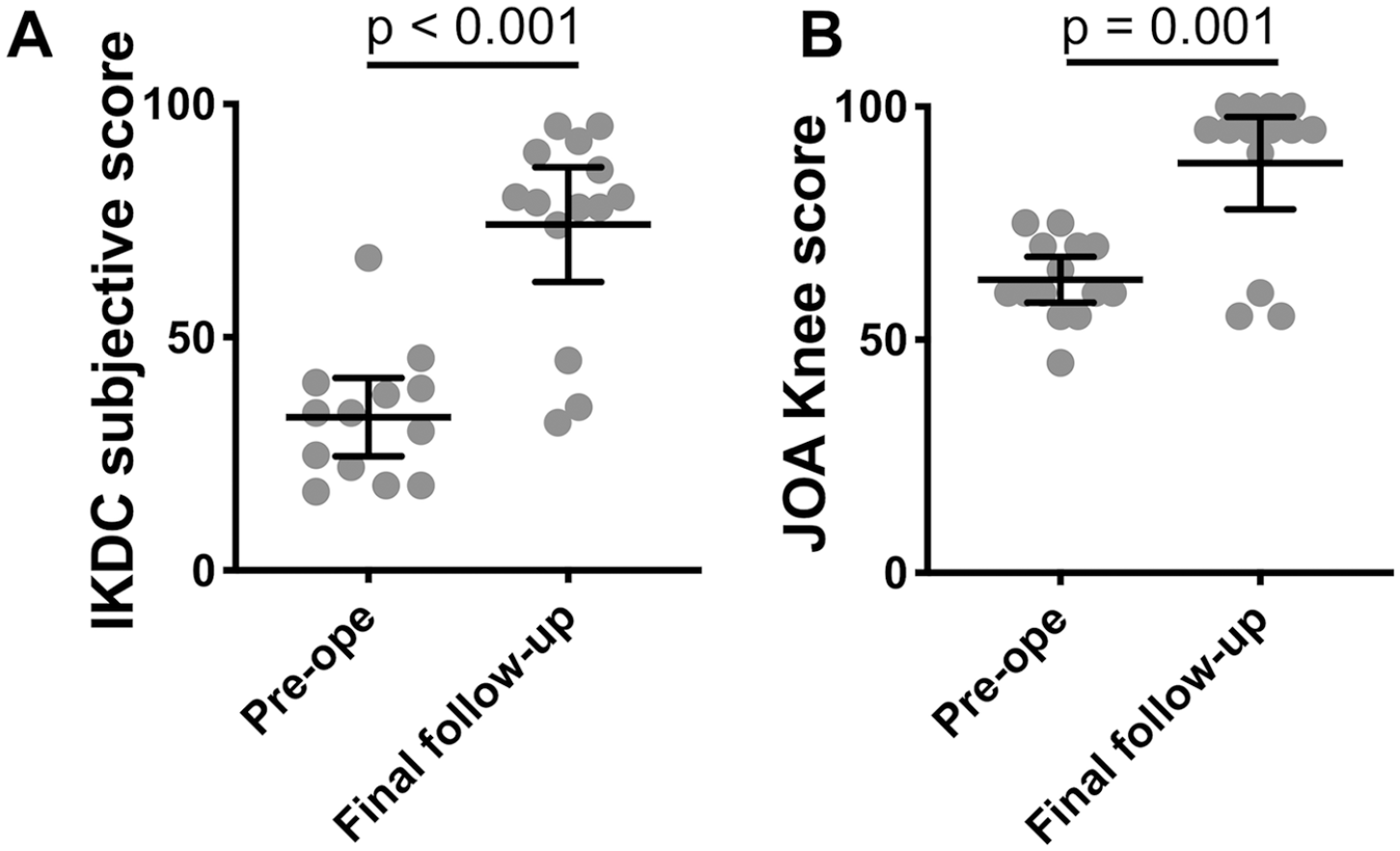
Preoperative (Pre-ope) and final (Final follow-up) The International Knee Documentation Committee (IKDC) subjective scores (
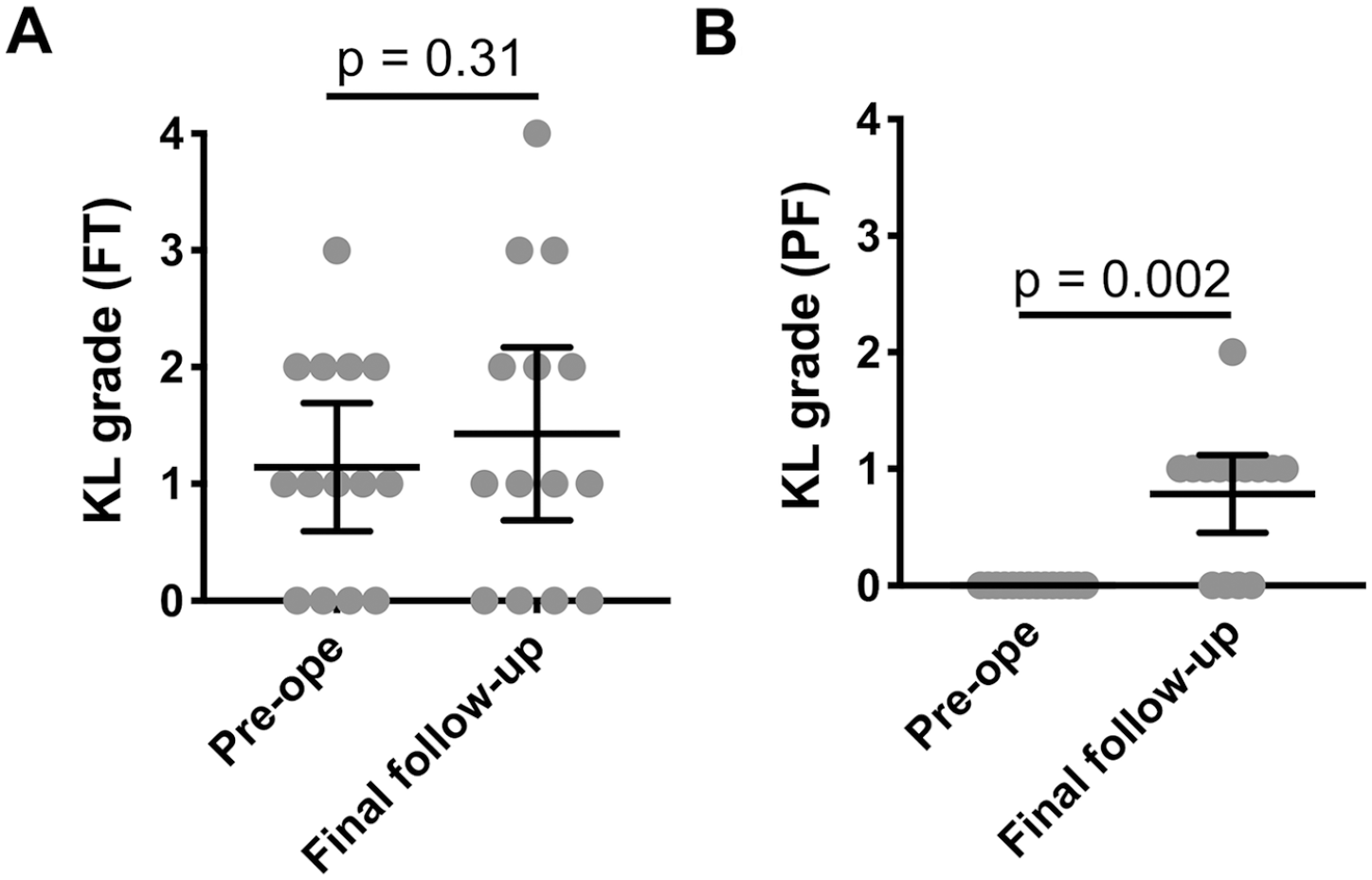
Preoperative (Pre-ope) and final (Final follow-up) Kellgren-Lawrence (KL) grades of femorotibial (FT) (
Although age at surgery, lesion size, period after surgery, KL grade at the final follow-up were not associated with the IKDC subjective score at the final follow-up, the number of affected joints (R2 = 0.67, P < 0.001) showed a negative association to the IKDC subjective score ( Table 3 ). The final IKDC score of knees with SLE (60.9 [29.2 to −92.6]) was significantly lower than non-SLE knees (81.6 [69.7 to 93.4]) (P = 0.04). A representative case (patient number 1, knee number 1) is shown in ( Fig. 4 ), in which good healing of the cartilage and remodeling of the subchondral bone were seen.
Association With IKDC Subjective Score at Final Follow-up.
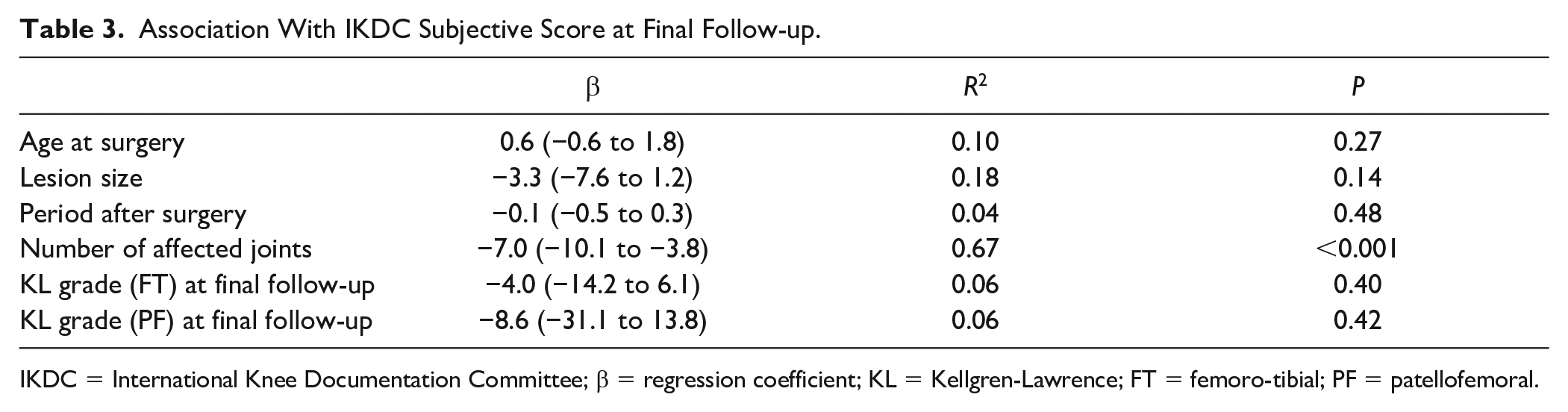
IKDC = International Knee Documentation Committee; β = regression coefficient; KL = Kellgren-Lawrence; FT = femoro-tibial; PF = patellofemoral.
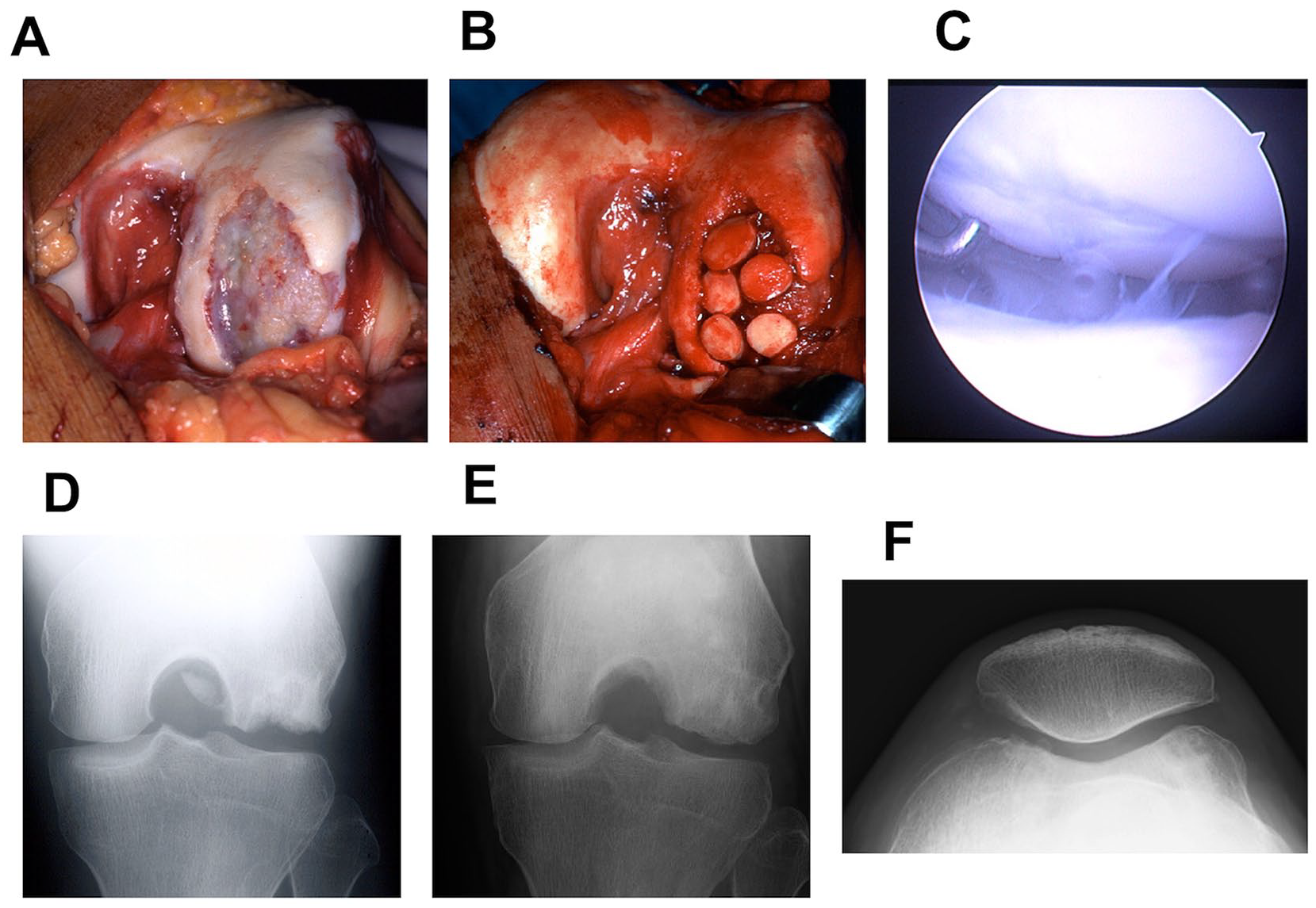
The representative case of the left knee of a 29-year-old male with steroid-induced osteonecrosis of the knee 5.6 years after the systemic steroid treatment (maximum 60 mg/d) against IgA syndrome (patient number 1, knee number 1). The disappearance of most of the cartilage, and a defect of the subchondral bone due to the corticosteroid-induced osteonecrosis in the lateral femoral condyle are shown in (
Discussion
The most important finding of this study was that the OAT for the corticosteroid-induced osteonecrosis of the knee showed good survivorship with improvements of clinical outcomes in long-term follow-up. There were no cases requiring revision surgeries on the transplanted osteochondral plugs during the 10 to 20 years of follow-up. No cases needed a conversion to prosthetic joint replacement within the follow-up period. The progress of osteoarthritis was avoided in the FT joint in many cases, although some degeneration was observed in the PF joint.
The longevity after OAT for corticosteroid-induced osteonecrosis of the knee was acceptable in this study, despite the severe and large damage of the cartilage and subchondral bone due to the necrosis. The advantage of OAT was to promote bone healing by removing necrotic tissues, by excavating through cartilage to healthy cancellous bone, and by replacing with plugs containing autologous tissue. The cartilaginous portion of the plugs also facilitated healing by replacing the cartilage with material having similar mechanical properties to surrounding cartilage. In the long-term survivorship of other treatment options, Early et al. 13 report the survivorship of osteochondral allograft with 33 knees, in which the survivorship was 90% at 5 years and 82% at 10 years. Osteochondral autografts with a depth of approximately 20 mm were used in cases with the deepest lesions, 14 which enabled radical debridement and good blood transport from the bone marrow to the transplanted plugs. The usage of the deep graft may be an advantage of the cylindrical osteochondral plugs. Furthermore, the better survival rate and bone union of autologous transplantation compared to those of allograft transplantation have been well recognized. 27 In unfavorable transplantation beds, a live graft with osteoconductive, osteoinductive, and osteogenic properties may provide better healing. 27
All patients in this study avoided prosthetic joint replacement at the final follow-up. Young and active patients are reluctant to undergo prosthetic joint replacement because of the high revision rate. In the report of TKA for steroid-induced osteonecrosis, the survival rate at 5 years follow up was 84%. 9 In modern TKA for young patients of osteoarthritis, an acceptable 10-year survivorship is 0% to 10% revision. 28 However, in their study of TKA, the patients with OA were about 20 years older than the steroid-induced osteonecrosis cohort in this study, and the survivorship of modern TKA for patients of the third or fourth decades is not evident. In addition, knee flexion was improved in many patients to the degrees where Seiza sitting was possible, which is hardly possible by TKA. The deep knee flexion can be expected by unicompartmental knee arthroplasty, whereas secondary osteonecrosis is the risk factor for the failure. 29 We believe that joint preserving surgery including OAT could satisfy the demands of patients who wanted to keep their lifestyles of floor sitting in non-Western countries.
The IKDC score was not recovered well in all cases. In 3 knees from 2 patients, the scored remained low. In these cases, the scores regarding to function was very unsatisfactory. Although there was no association between knee factors on the IKDC subjective score, patients having multiple joints affected was poorly associated the IKDC score. In terms of primary diseases, patients with SLE had inferior IKDC scores compared to patients without SLE. SLE itself is a risk factor for osteonecrosis, but patients with SLE treated with high-dose corticosteroids have a greater risk of developing osteonecrosis than with the presence of either risk factor alone. 30 Furthermore, SLE on its own causes lupus arthritis, which also involves the knee joint. 31 For patients with SLE and multifocal involvement, joint preservation surgery might not provide enough satisfaction because of their low activity level and possibility of prolonged synovitis.
Donor site morbidity is an important issue after OAT. In a previous report, PF pain related to the graft harvest was observed in 5% of the patients. 32 Even when the osteochondral plugs were harvested from the healthy knee to transplant to the elbow or ankle joint, 85% of the patients were asymptomatic, and no donor site defects required surgical intervention due to persistent symptoms. 33 However, due to the large lesion size compared with isolated cartilage defects or osteochondritis dissecans, in this study, multiple plugs needed to be harvested from the ipsilateral PF joint. Although no patients clearly reported patellofemoral pain, the mean KL grade of the PF joint increased. These patients needed to be followed-up for another 10 to 20 years to monitor the occurrence of PF symptoms due to the further progression of OA in the PF joint.
This study had some limitations that need to be addressed. First, there was no control group in this study, since all patients had severe knee pain and restricted activity in daily living. Thus, a historical control was discussed using previous articles of osteochondral allograft transplantation and TKA. Second, a retrospective cohort study was employed in this study. For a higher level of evidence, a prospective study, including a prospective randomized control trial, would be ideal. Third, the number of patients was small and a diversity existed in primary diseases because corticosteroid-induced osteonecrosis is not as common as osteonecrosis after insufficiency subchondral bone fracture of the knee. Fourth, the follow-up was performed using plain radiography, not MRI. Though radiographical recurrence of osteonecrosis was not observed, the MRI level recurrence was not denied.
In conclusion, long-term outcomes of OAT for steroid-induced were reported, in which none of the patients required revision cartilage operations and no one required arthroplasty intervention. Clinical outcomes were improved by OAT in most patients without progression of the OA in the FT joint. However, the progression of KL grade of the PF joint warned the occurrence of PF symptoms in the future, and further follow-up of the symptoms, recurrence of necrosis and longevity of the transplanted cartilage is warranted.
Footnotes
Authors’ Note
This work has performed at Kyoto University Hospital.
Acknowledgments and Funding
The authors thank Dr. Ryuzo Arai for clinical supports and thoughtful discussion. The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the ethics committee of Kyoto University Hospital (R0987).
Informed Consent
Due to the study design, informed consent was waived and opt-out was offered.
Trial Registration
Not applicable.