
Abstract
This study aims to compare the therapeutic efficacy of traditional Chinese medicine (TCM) injections in the treatment of coronary microvascular disease (CMVD) through a network meta-analysis. Multiple electronic databases including PubMed, Embase, Cochrane Library, Web of Science, China National Knowledge Infrastructure, Wanfang Database, VIP Database, and Chinese Biomedical Literature Database were retrieved up to November 15, 2023. The search was performed to identify randomized controlled trials (RCTs) on the therapeutic efficacy of TCM injections in combination with conventional Western medicine (CWM) for the treatment of CMVD. The Cochrane risk of bias tool was utilized to appraise the methodological quality of the included studies. Data analysis was performed using R software. A total of 13 RCTs, including 987 patients with CMVD, were included in the analysis. The results suggested that compared to CWM, Danhong [OR = 4.7, 95%CI (2.2, 11), P < 0.05] and Yiqi Fumai Lyophilized Injection [OR = 4, 95%CI (1.3, 14), P < 0.05] in combination with CWM demonstrated improved clinical efficacy in the treatment of CMVD. Danhong Injection [MD = −4.5, 95%CI (−6.4, −2.6), P < 0.05], Sulfotanshinone Sodium Injection [MD = −5.5, 95%CI (−7.1, −3.9), P < 0.05], Shuxuening Injection [MD = −7.9, 95%CI (−9.9, −5.9), P < 0.05], Shuxuetong Injection [MD = −4.4, 95%CI (−5.9, −2.9), P < 0.05], Ginkgo Leaf Extract and Dipyridamole Injection [MD = −3.6, 95%CI (−5.3, −2.0), P < 0.05], in combination with CWM, can reduce the frequency of angina attacks. TCM injections in combination with CWM are superior to CWM alone in the treatment of CMVD. However, further high-quality clinical research is needed to validate the above conclusion.
Keywords
Introduction
Coronary microvascular disease (CMVD) refers to a clinical syndrome characterized by exertional angina or laboratory evidence of myocardial ischemia, resulting from structural and/or functional abnormalities in the coronary arterioles and small arteries, under the influence of various pathogenic factors. 1 X Syndrome (syndrome X) was first proposed by Kemp in 1973, and in 1988, Cannon et al first described it as “microvascular angina” (MA). 2 In 2013, the “European Society of Cardiology Guidelines for the Management of Stable Coronary Artery Disease” officially named this condition as microvascular dysfunction. 3 In 2017, an expert group in China suggested that the term “microvascular dysfunction” does not encompass the structural abnormalities of the microvasculature in this condition. Therefore, they proposed renaming it as CMVD. 1 In 2020, the European Association of Percutaneous Cardiovascular Interventions (EAPCI) and the European Society of Cardiology (ESC) jointly issued an expert consensus on non-obstructive coronary artery disease, which included clinical diagnostic criteria for microvascular angina and diagnostic criteria for invasive technical examinations. 4
The Western medical treatment principles for CMVD mainly involve controlling cardiovascular disease risk factors and using traditional anti-anginal and anti-ischemic medications, which lack specificity. These medications include beta-blockers, nitroglycerin, calcium channel blockers, aspirin, RAAS inhibitors (including ACE inhibitors/ARBs), statins, as well as various non-traditional anti-anginal drugs such as nicorandil, ivabradine, trimetazidine, ranolazine, and mibefradil. 5 During the process of clinical trials and research, it has been found that conventional Western medical treatment may not significantly improve symptoms in patients with CMVD. Literature reports have indicated that calcium channel blockers may not effectively dilate coronary microvessels or correct coronary microvascular ischemia. Nitroglycerin may also not effectively relieve symptoms of coronary microvascular disease. 6 Currently, there is a lack of multicenter, large-sample clinical studies providing high-quality evidence for the treatment of CMVD. As a result, there are limitations in the treatment strategies. 7 Traditional Chinese medicine (TCM) has unique advantages and good therapeutic effects in treating CMVD, making it a potential new strategy for the treatment of CMVD. 8 The treatment for CMVD includes three main components: lifestyle interventions, management of risk factors, and a combination of Western and Chinese medicine. TCM can improve microcirculation through mechanisms such as enhancing endothelial function and promoting the release of vasodilatory substances. 9 CMVD is categorized within TCM as “chest impediment” or “heartache due to chest impediment.” Numerous studies have shown that TCM's individualized treatment based on syndrome differentiation has significant advantages in improving clinical symptoms and reducing adverse outcomes in CMVD. 10 TCM injections, such as Danhong injection and Danshen injection, are strongly recommended for the treatment of heart blood stasis in CMVD. 11 The combination of different TCM injections with conventional Western medicine (CWM) can improve the therapeutic efficacy for stable angina and has a better safety profile. 12
This study utilizes a network meta-analysis method to systematically evaluate the clinical efficacy of different TCM injections combined with CWM in CMVD. The aim is to provide evidence-based support for clinical medication decisions.
Methods and Data
Literature Search
Computer searches were conducted in databases including PubMed, Embase, Cochrane Library, Web of Science, China National Knowledge Infrastructure (CNKI), Wanfang Database, VIP Database, and China Biomedical Literature Database (SinoMed) up until November 15, 2023. The search was conducted for randomized controlled trials (RCTs) on the combination of TCM injections with CWM for CMVD. The Chinese search terms included “coronary microvascular disease”, “microvascular angina”, “injection”, etc The English search terms included “Microvascular Angina”, “Angina X Syndrome”, etc These terms were combined for the search. The search strategy is detailed in Supplemental Material 1. This study has been registered with PROSPERO (CRD42023486013).
Inclusion and Exclusion Criteria
Inclusion Criteria
Study type: The study design had to be a randomized controlled trial.
Study participants: Adult individuals had to meet the diagnostic criteria for CMVD. 1
Intervention: The control group received CWM (including aspirin, beta-blockers, statins, calcium channel blockers, nitrate drugs, nicorandil, etc). In the observation group, in addition to the treatment regimen used in the control group, Chinese herbal injection therapy was also administered.
Outcome measures: The primary outcome measure was clinical efficacy, classified as follows:
Marked effect: Complete disappearance or substantial reduction (≥80%) of angina symptoms, with a significant decrease in the frequency of angina attacks.
Effective: Significant relief of angina symptoms, with a reduction in the frequency of angina attacks ranging from 50% to less than 80%, along with a noticeable decrease in the severity and duration of the attacks.
Ineffective: No significant improvement in angina symptoms, with a reduction in the frequency of angina attacks of less than 50%.
The secondary outcome measures included the frequency of angina attacks, CRP levels, and the extent of ST-segment depression during exercise stress testing. The study design was a randomized controlled trial.
Exclusion Criteria
Duplicate publications, Animal studies, Case reports, Conference abstracts, Reviews, Full-text unavailable, Studies with no relevant outcomes, Studies on CMVD patients accompanied by other organic diseases.
Data Extraction
Two authors screened the literature based on pre-defined inclusion and exclusion criteria. In case of any discrepancies, they resolved them through discussion or consulted a third party to reach a consensus. The following key data were extracted from the included studies: first author, publication year, country, sample size, gender, age, intervention measures, and outcome measures.
Quality Assessment
The risk of bias was appraised using the latest recommendations from the Cochrane Risk of Bias Assessment Tool 2.0 (ROB 2.0). It includes five main domains: bias in the randomization process, bias due to deviations from intended interventions, bias due to missing outcome data, bias in measurement of the outcome, and bias in selection of the reported result. The quality of the literature was evaluated as “low risk of bias,” “some concerns,” or “high risk of bias.” The research results were cross-checked by two researchers. In case of any discrepancies, they were discussed to reach a consensus, or a third-party opinion was sought.
Data Analysis
The data analysis was conducted utilizing R 4.3.2 (R Foundation for Statistical Computing). A Bayesian network meta-analysis was performed utilizing a priori fuzzy random-effects model. The Markov chain Monte Carlo method was employed to obtain the best combined estimates and probabilities for each treatment strategy. For binary outcome data, the odds ratio (OR) and 95% credible interval (CI) were leveraged to represent the results. For continuous outcomes, the mean difference (MD) and its 95% CI were employed. The probability of the best intervention was estimated by calculating the surface under the cumulative ranking curve (SUCRA). STATA 15.0 software was utilized to generate network plots and funnel plots. In the network plot, each circle represents a drug, and the edges represent existing comparisons. The size of the circles is proportional to the number of patients included. The cumulative probability plots were created using the ggplot2 package.
Results
Data Screening Process and Results
By conducting a preliminary search, a total of 2927 articles were identified. After removing 594 duplicate articles, 2311 articles were further excluded by reading titles and abstracts. After reading the full text, 9 articles were excluded. Finally, 13 articles were included for analysis (Figure 1).

Literature Screening Process.
Included Studies
A total of 13 Chinese articles were incorporated into this study, and no English articles were included. The Chinese herbal injections included Danhong Injection, Shuxuetong Injection, Shuxuening Injection, and Sulfotanshinone Sodium Injection. All the included articles reported the age of the participants and mentioned the duration of intervention, with the shortest treatment duration being 10 days and the longest being 4 weeks. The basic features of the 13 included articles are presented in Table 1.
Characteristics of Included Studies.
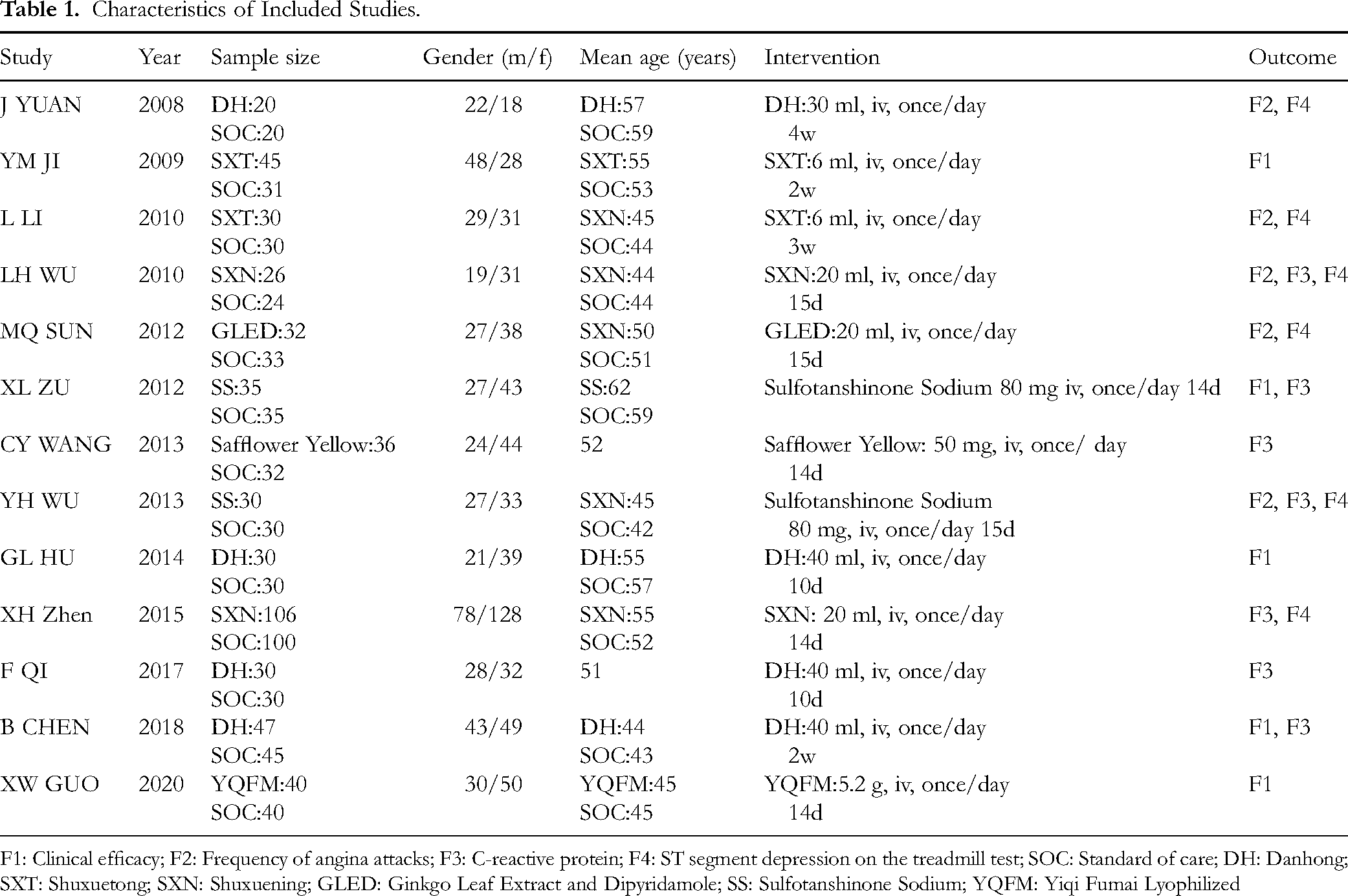
F1: Clinical efficacy; F2: Frequency of angina attacks; F3: C-reactive protein; F4: ST segment depression on the treadmill test; SOC: Standard of care; DH: Danhong; SXT: Shuxuetong; SXN: Shuxuening; GLED: Ginkgo Leaf Extract and Dipyridamole; SS: Sulfotanshinone Sodium; YQFM: Yiqi Fumai Lyophilized
Most eligible studies did not provide specific details about the randomization method, allocation concealment, and blinding. The high risk primarily comes from selective reporting bias. The assessment of risk of bias for the included studies can be found in Figures 1 and 2.

Risk of Bias Graph.
Meta-Analysis Results
Four studies13–16 mentioned the clinical efficacy rate (Figure 3). The network plot (Figure 3A) showed the comparison of different herbal injections, and there was no closed loop. The consistency test results indicated that the data were consistent. The thickness of the lines represents the number of included studies for each intervention, and the size of the circles represents the sample size for each intervention. Compared to CWM alone, the combination of Chinese herbal injections with CWM could improve the clinical efficacy rate in patients with CMVD [Danhong Injection: OR = 4.7, 95% CI (2.2, 11); Yiqi Fumai Lyophilized Injection: OR = 4, 95% CI (1.3, 14); Figure 3C]. However, there was no marked difference in efficacy between Danhong Injection and Yiqi Fumai Lyophilized Injection when combined with CWM (as shown in Supplemental Material 2, Table 1). The cumulative ranking plot showed that Danhong Injection had the highest SUCRA (75.6%), followed by Yiqi Fumai Lyophilized Injection (66.5%), and CWM had the lowest SUCRA (4.3%) (Figure 3B). Heterogeneity analysis indicated no substantial heterogeneity between SOC and DH. Indirect comparison suggested low heterogeneity between Sulfotanshinone Sodium and SOC, and overall consistency across studies was high. Both DH and Sulfotanshinone Sodium may exert significant effects compared with SOC (OR < 1 with 95% CrI not including 1), with consistent effect directions. The low heterogeneity enhanced the credibility of these findings (Figure 3D). Both SXT versus SOC and YQFM versus SOC exhibited low heterogeneity, with each intervention showing a positive effect trend relative to SOC. The low heterogeneity provided robust support for this trend (Figure 3E).

Meta-Analysis of the Clinical Efficacy Rate (A: Network Plot, B: Area Under the Cumulative Probability Curve, C: Forest Plot, D: Heterogeneity Analysis, E: Heterogeneity Analysis).
Five studies17–21 mentioned the frequency of angina attacks (Figure 4). Based on the network plot (Figure 4A), compared to CWM alone, the combination of Chinese herbal injections with CWM could reduce the frequency of angina attacks in patients with CMVD [Danhong Injection: MD = −4.5, 95% CI (−6.4, −2.6); Sulfotanshinone Sodium Injection: MD = −5.5, 95% CI (−7.1, −3.9); Shuxuening Injection: MD = −7.9, 95% CI (−9.9, −5.9); Shuxuetong Injection: MD = −4.4, 95% CI (−5.9, −2.9); Ginkgo Leaf Extract and Dipyridamole Injection: MD = −3.6, 95% CI (−5.3, −2.0); Figure 3C]. Additionally, the efficacy of Shuxuening Injection was superior to that of Shuxuetong Injection and Ginkgo Leaf Extract and Dipyridamole Injection, and the efficacy of Shuxuetong Injection was superior to Ginkgo Leaf Extract and Dipyridamole Injection. However, the differences between the two comparisons were statistically significant. There was no significant difference between Danhong Injection combined with CWM and other Chinese herbal injections combined with CWM (as shown in Supplemental Material 2, Table 2). The cumulative ranking plot showed that Shuxuening Injection had the highest SUCRA (79.9%), followed by Danshenkang II A Sodium Sulfonate Injection (66.5%), and CWM alone had the lowest SUCRA (4.3%) (Figure 4B).

Meta-Analysis of Frequency of Angina Attacks (A: Network Plot, B: Area Under the Cumulative Probability Curve, C: Forest Plot).
The SUCRA (Surface Under the Cumulative Ranking) Comprehensive Ranking.

F1: Clinical efficacy; F2: Frequency of angina attacks; F3: C-reactive protein; F4: ST segment depression on the treadmill test; DH: Danhong; SOC: Standard of care; SXN: Shuxuening; SXT: Shuxuetong; YQFM: Yiqi Fumai Lyophilized; GLED: Ginkgo Leaf Extract and Dipyridamole
Seven studies14,18,21–25 mentioned CRP and high-sensitivity CRP (hsCRP) (Figure 5). Based on the network plot (Figure 5A), compared to CWM, the combination of Chinese herbal injections with CWM could reduce CRP levels in patients with CMVD. However, there was no statistically significant difference between Chinese herbal injections combined with CWM and CWM alone (as shown in Supplemental Material 2). Heterogeneity analysis identified that the sources of heterogeneity arose from the SOC versus DH and SOC versus HHHSS groups (Figure 5D), the Sulfotanshinone Sodium versus SOC group (Figure 5E), and the SXN versus SOC group (Figure 5F).

Meta-Analysis of CRP and High-Sensitivity CRP (A: Network Plot, B: Area Under the Cumulative Probability Curve, C: Forest Plot, D: Heterogeneity Analysis, E: Heterogeneity Analysis, F: Heterogeneity Analysis).
Six studies17–21,23 mentioned the improvement in ST-segment depression during exercise treadmill testing (Figure 6). Based on the network plot (Figure 6A), compared to CWM, the combination of Chinese herbal injections with CWM could reduce the extent of ST-segment depression during exercise treadmill testing in patients with CMVD. However, there was no statistically significant difference between Chinese herbal injections combined with CWM and CWM alone (as shown in Supplemental Material 2). Heterogeneity analysis showed high heterogeneity in the SXN versus SOC group (Figure 6D) and suggested a potential presence of heterogeneity in the GLED versus SOC group (Figure 6E).

Meta-Analysis of ST-Segment Depression During Exercise Treadmill Testing (A: Network Plot, B: Area Under the Cumulative Probability Curve, C: Forest Plot, D: Heterogeneity Analysis, E: Heterogeneity Analysis).
Evaluation of Publication Bias
We used funnel plots to examine publication bias for clinical efficacy, frequency of angina attacks, CRP, and ST-segment depression during exercise treadmill testing. The results suggest a higher possibility of publication bias for CRP and ST-segment depression during exercise treadmill testing (as shown in Supplemental Material 2, Figures 1–4).
Discussion
This study is the first to delve into the effectiveness of different Chinese herbal injections combined with CWM in patients with CMVD. Previous meta-analyses have found that TCM and Chinese herbal decoctions show improved efficacy in CMVD patients when combined with CWM. However, the use of Chinese herbal injections has not been explored in these studies, which is the novelty of our research.
This study analyzed the efficacy of TCM injections in the treatment of CMVD. The results demonstrated differential advantages of various drugs across key efficacy indicators. For overall clinical efficacy, Danhong Injection showed the best performance, followed closely by Yiqi Fumai Lyophilized Injection. This finding may provide a clear reference for prioritizing treatments in comprehensive disease management. In contrast, regarding symptom-focused outcome measures, specifically the reduction of angina attack frequency, Shuxuening Injection exhibited the most pronounced effect, with Sodium Tanshinone IIA Sulfonate ranking second and Danhong Injection third. These differences in efficacy suggest that clinical drug selection should be guided by treatment goals: Danhong Injection may be prioritized when overall disease control and improvement of comprehensive efficacy are desired, whereas Shuxuening Injection may be preferred when the primary concern is frequent angina attacks and symptom relief.
In TCM, treatment of CMVD primarily focuses on promoting blood circulation and removing blood stasis, supplemented by tonifying Qi and nourishing Yin (Figure 7). Among these, Danhong Injection is a compound injection composed of effective components from such traditional Chinese herbs as Danshen (Radix Salviae Miltiorrhizae) and Honghua (Flos Carthami). It is a commonly used blood-activating and stasis-resolving medication in clinical practice. 26 The combination of Radix Salviae Miltiorrhizae and Flos Carthami has been shown to have beneficial effects on inflammation, oxidative status, vascular endothelial damage, and myocardial energy metabolism. 27 The main active components of Danhong Injection include Salvianolic Acid A (SAA), Salvianolic Acid B (SAB), Salvianolic Acid C (SAC) extracted from Radix Salviae Miltiorrhizae, as well as flavonoids, hydroxysafflor yellow A (HSYA), and catechins extracted from Flos Carthami. 28 The phenolic acid components in Radix Salviae Miltiorrhizae are the main constituents of Danhong Injection. They can stabilize atherosclerotic plaques, inhibit platelet aggregation, improve endothelial function, and resist lipid peroxidation, while Flos Carthami can dilate the coronary artery, regulate the immune system, improve myocardial ischemia, and exert anti-thrombotic, antioxidant, anti-inflammatory, anti-liver fibrosis, anti-tumor, and analgesic effects. The active components in Danhong Injection can interact with different targets in signal pathways simultaneously, regulating and controlling coagulation, fibrinolysis, lipid metabolism, endothelial cell function, and vascular contraction and dilation pathways, thereby exerting pharmacological effects. 29 They can improve cardiac dysfunction, restore metabolic product levels caused by myocardial ischemia-reperfusion to normal levels, and regulate energy metabolism and oxidative stress, thereby exerting therapeutic effects.

Mechanisms of TCM for CMVD.
Yiqi Fumai Lyophilized Injection is a compound injection made from the purified extracts of three medicinal herbs, namely Hongshen (Red Ginseng), Maidong (Radix Ophiopogonis), and Wuweizi (Fructus Schisandrae). Pharmacological studies have shown that the active components of Yiqi Fumai Lyophilized Injection, possibly through their effects on vascular endothelial cells and smooth muscle cells, can regulate sodium ion reabsorption and interact with the coagulation system and hematopoietic function, thereby exerting a blood-activating and stasis-resolving effect. The active components of Radix Ophiopogonis have anti-inflammatory properties and can regulate immunity and glucose and lipid metabolism. The active components of Red Ginseng and Fructus Schisandrae can control glucose and lipid metabolism pathways and regulate energy metabolism. The overall formula can prevent and treat cardiovascular diseases caused by myocardial ischemia. 30 It is effective in the treatment of conditions such as heart failure and microcirculation disorders caused by ischemia-reperfusion. The MAPK signaling pathway is directly associated with the development of inflammation in cells, vascular smooth muscle cells, and vascular endothelial cells, and with the development of atherosclerosis. It also regulates the progression of various cardiovascular diseases. 31 Tanshinone IIA-sulfonic sodium is also a major component of Danshen. It is a water-soluble substance obtained through sulfonation. The combination of Tanshinone IIA-sulfonic sodium and Isosorbide Dinitrate can significantly improve hemorheology, regulate lipid levels, oxidative stress, and endothelial function in patients with coronary heart disease and angina pectoris, and reduce the degree of inflammation. 32 Shuxuening Injection is a Chinese herbal injection extracted and purified from Ginkgo leaves. It protects the endothelial cells of blood vessels, promotes the secretion of endothelial vasodilators, and balances the ratio of thromboxane to prostacyclin. This improves vascular tone, increases coronary blood flow, slows down heart rate, and reduces myocardial oxygen consumption. It can effectively counteract myocardial ischemia and protect the myocardium from ischemia-reperfusion injury. 33
Limitations of this study are as follows. First, among the 13 included studies, only one study reported specific methods of randomization, and none of the studies described allocation concealment or blinding of outcome assessors, which increased the risk of bias and lowered the overall quality of the evidence. Second, the diagnosis of CMVD is currently complex, and conventional treatment options and medication regimens vary, contributing to clinical heterogeneity. Third, the number of included studies and the sample size were small. Unclear randomization, absence of allocation concealment, and lack of blinding may lead to a high risk of bias and affect the robustness of the conclusions. Without proper randomization, baseline comparability between groups may be insufficient, making it difficult to determine true intervention effects. The lack of allocation concealment could allow investigators or participants to influence group assignments, ultimately introducing selection bias. The absence of blinding may result in performance bias due to differences in intervention implementation or detection bias in outcome assessment. These risks may prevent the results from accurately reflecting the true effects of the interventions, thereby reducing the reliability and generalizability of the conclusions. Thus, more large-scale, high-quality clinical RCTs are needed to confirm the effectiveness and safety of Qi-tonifying and blood-activating herbal medicines in the treatment of CMVD and to provide stronger evidence-based guidance for clinical practice.
Conclusion
Current evidence suggests that the combination of Chinese herbal injections with CWM shows better efficacy in the treatment of CMVD, particularly in reducing the frequency of angina attacks. Among them, Danhong Injection shows potential therapeutic advantages. However, further validation through large-sample RCTs is required. Regarding safety, TCM injections contain macromolecules such as peptides, polysaccharides, and proteins, which may trigger immune responses or hypersensitivity. TCM injections are typically prepared through purification and the addition of excipients, processes that may trigger chemical reactions and generate new allergenic components. These sensitizing components cannot be completely eliminated by current pharmaceutical technologies. Moreover, most TCM injections are compound formulations, and combining different drug components may increase the risk of adverse reactions. Previous studies have not systematically reported hepatic or renal function abnormalities, providing only indirect indications of potential risk. In middle-aged and older adults, the compensatory capacity of the liver and kidney functions is inherently reduced, and some TCM injections require hepatic or renal metabolism. Thus, prolonged or high-dose use may impose additional organ burden. Future multicenter RCTs should include safety endpoints, such as the incidence of hepatic or renal dysfunction and severe allergic reactions, apply blinding to minimize reporting bias, and conduct subgroup analyses to clarify safety differences among TCM injections.
In addition to pharmacological treatment, a healthy E(e)SEEDi lifestyle,34,35 including marine natural products, 36 remains crucial for human cardiovascular health. This integrated approach, combining effective pharmacotherapy with a healthy lifestyle, is important for the prevention and management of CMVD and for promoting overall cardiovascular well-being.
Supplemental Material
sj-docx-1-npx-10.1177_1934578X251401418 - Supplemental material for Efficacy of Different Traditional Chinese Medicine Injections in the Treatment of Coronary Microvascular Disease: A Network Meta-Analysis
Supplemental material, sj-docx-1-npx-10.1177_1934578X251401418 for Efficacy of Different Traditional Chinese Medicine Injections in the Treatment of Coronary Microvascular Disease: A Network Meta-Analysis by Sihan Peng, Jiajun Yu, Junliang Zhou, Weiqin Yang, Yifan Han, Danping Xu and Chaorong Lin in Natural Product Communications
Supplemental Material
sj-docx-2-npx-10.1177_1934578X251401418 - Supplemental material for Efficacy of Different Traditional Chinese Medicine Injections in the Treatment of Coronary Microvascular Disease: A Network Meta-Analysis
Supplemental material, sj-docx-2-npx-10.1177_1934578X251401418 for Efficacy of Different Traditional Chinese Medicine Injections in the Treatment of Coronary Microvascular Disease: A Network Meta-Analysis by Sihan Peng, Jiajun Yu, Junliang Zhou, Weiqin Yang, Yifan Han, Danping Xu and Chaorong Lin in Natural Product Communications
Supplemental Material
sj-docx-3-npx-10.1177_1934578X251401418 - Supplemental material for Efficacy of Different Traditional Chinese Medicine Injections in the Treatment of Coronary Microvascular Disease: A Network Meta-Analysis
Supplemental material, sj-docx-3-npx-10.1177_1934578X251401418 for Efficacy of Different Traditional Chinese Medicine Injections in the Treatment of Coronary Microvascular Disease: A Network Meta-Analysis by Sihan Peng, Jiajun Yu, Junliang Zhou, Weiqin Yang, Yifan Han, Danping Xu and Chaorong Lin in Natural Product Communications
Footnotes
Abbreviations
Acknowledgements
Not applicable.
Ethical Considerations
Not applicable.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Author Contributions
Sihan Peng: Conceptualization, Methodology, Validation, Formal analysis, Writing – Original Draft; Jiajun Yu: Software, Validation, Formal analysis, Investigation, Writing – Review & Editing; Junliang Zhou: Validation, Formal analysis, Investigation, Writing – Review & Editing; Weiqin Yang: Investigation, Data Curation, Writing – Review & Editing; Yifan Han: Investigation, Data Curation, Writing – Review & Editing; Danping Xu: Conceptualization, Methodology, Writing – Review & Editing, Supervision; Chaorong Lin: Conceptualization, Methodology, Writing – Review & Editing, Supervision. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Sanming Project of Medicine in Shenzhen, Traditional Chinese Medicine Bureau of Guangdong Province, (grant number No. SZZYSM202202012).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.