
Abstract
Keywords
Introduction
As a systemic metabolic bone disease, osteoporosis (OP) is characterized by decreased bone mass and microstructural damage; as a result, bone fragility increases, and patients become more susceptible to fractures. 1 OP can be categorized into two types: primary and secondary OP. Primary OP (POP) is characterized by an imbalance between bone formation and resorption, ie, greater resorption than formation; therefore, negative bone remodeling and trabecular bone structure destruction are triggered. As a result, bone strength decreases, and fracture risk increases. POP can be further categorized into the following types according to age, physiological degeneration, and pathological changes: postmenopausal OP (type I), senile OP (type II), 2 and idiopathic OP (juvenile onset). In general, some diseases, medications, or other factors result in secondary OP. Because of the increase in the aging population globally, the number of patients with OP and disability is increasing each year; this not only poses significant psychological and economic burdens on patients and society but also incurs considerable healthcare costs. 3 Based on the estimates for 2025, 4 the incidence of osteoporotic fractures will reach 4.5 million cases each year. Furthermore, in Canada, Europe, and the United States alone, direct treatment costs for osteoporotic fractures will range from 500 to 650 billion US dollars. Although anti-OP drugs such as bisphosphonates, calcitonin, parathyroid hormone analogs, and selective estrogen receptor modulators that can increase bone density, improve bone quality, and decrease fracture risk are available, they lead to a greater degree of gastrointestinal reactions and cardiovascular and cerebrovascular diseases as side effects. Furthermore, limitations such as drug resistance and lifelong medication use exist, seriously affecting the clinical efficacy and compliance of patients and hindering the promotion of the use of anti-OP drugs as treatment modalities.
Chinese patent medicine (CPM) is defined as a preparation comprising multiple ingredients, targets, and effects. It is prepared using Chinese medicinal materials, guided by traditional Chinese medicine (TCM) theory, and formulated in specific doses and formulations based on specific prescriptions or standards.5,6 Many recent randomized controlled trials (RCTs) and systematic reviews have verified the efficacy and safety of TCM combined with Western medicine for POP treatment.7‐12 Although many drug types are available for treating POP, a comparative analysis of their effectiveness is lacking; therefore, they are not conducive to clinical promotion or selection of the optimal treatment plan. As an extension of traditional meta-analysis, network meta-analysis is a method in which similar articles are combined, direct and indirect comparisons between different interventions are quantitatively analyzed, and the best scheme is calculated via cumulative probability ranking. This considerably increases the value of RCTs. Accordingly, in this study, we employed a network meta-analysis to compare the effectiveness and safety of different CPMs combined with Western medicine for treating POP to provide strong evidence-based support for clinical treatment.
Results
Study Selection and Baseline Characteristics
Figure 1 illustrates the PRISMA flowchart depicting the steps of literature screening, study selection, and exclusion criteria. First, we retrieved 2157 articles via a search. Then, EndNote X9 was used to automatically combine and manually filter the articles for duplicates, leaving 1032 articles. After reading the titles and abstracts, some articles that were evidently irrelevant to our study or did not meet the inclusion criteria, including those comprising animal cell experiments, surgical articles, case reports, and reviews, were excluded. In total, 204 articles were downloaded for in-depth screening. After reading the full texts, we excluded the articles that did not conform to the inclusion criteria. Finally, 44 RCTs13‐56 were included in this meta-analysis. In these studies, 4859 patients who were diagnosed with POP were included: 2577 in the treatment group and 2282 in the control group. The average age of the included patients was 40–75 years; the most common age range was 55–70 years. The following 12 CPMs were included in these studies: Jintiange capsule (JTG), Guishukang capsule (GSK), Qianggu capsule (QG), Hugu capsule (HG), Qigugu capsule (QGJN), Jinggui Shenqi pill (JGSQ), Liuwei Dihuang pill (LWDH), Zuogui pill (ZGW), Yougui pill (YGW), Qing'e pill (QEW), Gusuibu granule (GSB), and Xianling Gubao capsule (XLGB). For outcomes, 24 articles investigated overall efficacy, 44 articles investigated lumbar spine BMD, 26 articles investigated femoral neck BMD, 18 articles investigated VAS score, 16 articles investigated ALP, and 13 articles investigated adverse reactions. Table 1 summarizes the basic characteristics of the included RCTs.
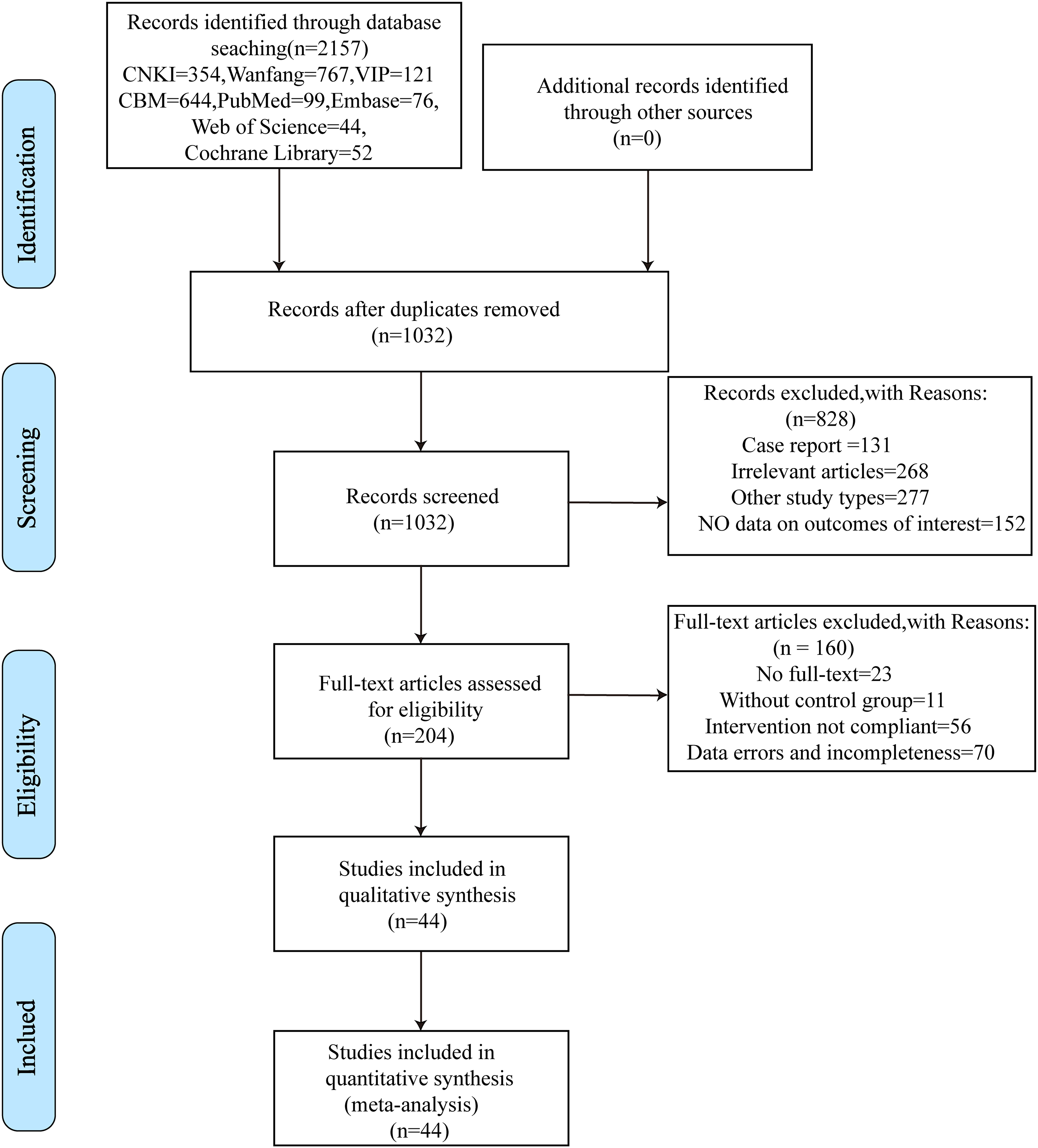
Process for screening the literature.
Basic Characteristics of the Included Articles.

T: experimental group; C: control group; NA: not available; CM: conventional medicine; JTG: Jintiange Capsule; GSK: Gushukang Capsule; QG: Qianggu Capsule; HG: Hugu Capsule; QGJN: Qigu Capsule; JGSQ: Jingui Shenqi Pills; LWDH: Liuwei Dihuang Pill; ZGW: Zuogui Pill; YGW: Yougui Pill; QEW: Qinge Pill; GSB: Gusongbao Granule; XLGB: Xianling Gubao Capsule, same as below; ms: months; ws: weeks; ① Total effective rate; ② Lumbar spine BMD; ③ Femoral Neck BMD; ④ Visual analog scale; ⑤ Alkalinephosphatase; ⑥ Adverse reaction rate.
Quality Evaluation of the Included Articles
All 44 articles included in this study were RCTs. To generate random sequences, the random number table method was used in 16 articles,13,15,20,23,29,31,32,38,40,41,46‐48,50,55,56 the random envelope method was used in 1 study, 22 and a multicenter stratified block randomization method was used in 2 articles.24,28 All these articles were considered to exhibit a “low risk” of bias. Different treatment regimens for grouping were utilized in two articles,26,51 whereas the order of admission was used in 1 study 21 ; these articles were considered to exhibit a “high risk” of bias. No specific randomization methods were reported in the remaining articles, and they were considered to exhibit an “unclear risk” of bias. For allocation concealment, the envelope method was utilized in one study 28 and was considered to exhibit a “low risk” of bias. No specific allocation concealment methods were mentioned in the remaining articles, which were rated as “unclear risk” of bias. Regarding blinding, double-blind methods were utilized in two articles24,28 and were considered to exhibit a “low risk” of bias. However, no specific blinding methods were reported in the remaining articles and were rated as “unclear risk” of bias. The completeness of the outcome data in the included articles was rated as “low risk” of bias. Furthermore, no selective reporting of outcomes was observed; therefore, the study was rated as “low risk” of bias. Other parameters exhibited an unclear risk of bias (Figure 2).

Percentages of the included literature that generated risks of bias.
Total Effective Rate
Network of Evidence
The overall response rates of eight types of CPM, with a total sample size of 2280, were reported in 24 articles.14‐23,25,29,31,32,34,35,40,46,48‐50,52‐54 The evidence network centered on CM, with the absence of a closed loop between intervention measures; therefore, inconsistency tests were not required (Figure 3). In the evidence network diagram, the respective circles represent different intervention measures. Furthermore, the size of the circle represents the sample size of the study, the line represents a direct or indirect comparison between two intervention measures, and the thickness of the line is proportional to the number of included articles. Therefore, there was evidence of direct or indirect comparisons between the different intervention measures; as a result, the basic conditions for the network meta-analysis (similarly hereinafter) were satisfied.

Evidence network diagram of the different outcome indicators.
Conventional meta-Analysis
According to the network evidence plot, most direct comparisons were observed between CPM combined with CM and CM alone. Furthermore, direct comparisons were made between JTG and between JTG and CM. After merging the data, low heterogeneity (P = 0.139, I2 = 24.3%) was observed. According to the data analysis, compared with CM alone, the fixed effects model revealed that CPM combined with CM significantly improved the total effective rate. Furthermore, the difference was statistically significant. However, no statistically significant difference was observed between JTG alone and JTG combined with CM (Figure S1).
Network meta-Analysis
By comparing the eight CPMs, 55 pairwise comparisons were generated. Network meta-analysis revealed that JTG [RR = 1.33, 95% CI (1.21, 1.46)], QEW [RR = 2.57, 95% CI (1.32, 5.00)], XLGB [RR = 1.23, 95% CI (1.15, 1.33)], HG [RR = 1.35, 95% CI (1.17, 1.55)], QGJN [RR = 1.39, 95% CI (1.12, 1.74)], LWDH [RR = 1.21, 95% CI (1.06, 1.38)], and GSK [RR = 1.17, 95% CI (1.08, 1.25)] combined with CM were superior to CM alone for increasing the total effective rate. Compared with XLGB and LWDH combined with CM and JTG, QEW combined with CM exhibited a greater effect on increasing the total effective rate. Moreover, the efficacy of JTG combined with CM and LWDH was significantly greater than that of JTG alone. However, no statistically significant difference was observed in the efficacy of the remaining interventions (Figure 4).

Network meta-analysis of the effects of the total effective rate.
Lumbar Spine BMD
Network of Evidence
In total, 43 articles13‐24,26‐56 reported data on lumbar spine BMD, with 12 types of CPMs and a total sample size of 4572. The evidence network centered on CM, with no closed loop between the interventions; therefore, no inconsistency test was required (Figure 3).
Conventional Meta-Analysis
The network diagram revealed that most comparisons were observed between CPM combined with CM and CM alone. Furthermore, direct comparisons were made between JTG and JTG combined with CM, GSB and QG/HG, and HG and XLGB. However, owing to the high heterogeneity in the comparisons, sensitivity analysis could not decrease the heterogeneity; therefore, effect sizes were not merged, and only descriptive analysis was performed. The random effects model revealed that except for the comparison between YGW combined with CM and CM, which exhibited no statistical significance, all other CPMs combined with CM could increase lumbar spine BMD compared with CM alone; the differences were considered to be statistically significant. However, no statistically significant differences were detected between JTG and JTG combined with CM, GSB and QG/HG, or HG and XLGB (Figure S2).
Network Meta-Analysis
In total, 136 pairwise comparisons were generated by comparing 12 TCM types. Network meta-analysis revealed that for increasing lumbar spine BMD, ZGW [WMD = 0.10, 95% CI (0.03, 0.18)], QEW [WMD = 0.08, 95% CI (0.02, 0.14)], XLGB [WMD = 0.07, 95% CI (0.01, 0.12)], LWDH [WMD = 0.17, 95% CI (0.05, 0.28)], GSK [WMD = 0.12, 95% CI (0.04, 0.19)], and JTG [WMD = 0.09, 95% CI (0.02, 0.16)] combined with CM were significantly superior to CM alone. However, no significant difference was observed in the efficacy between the other TCM types (P > 0.05) (Figure 5)
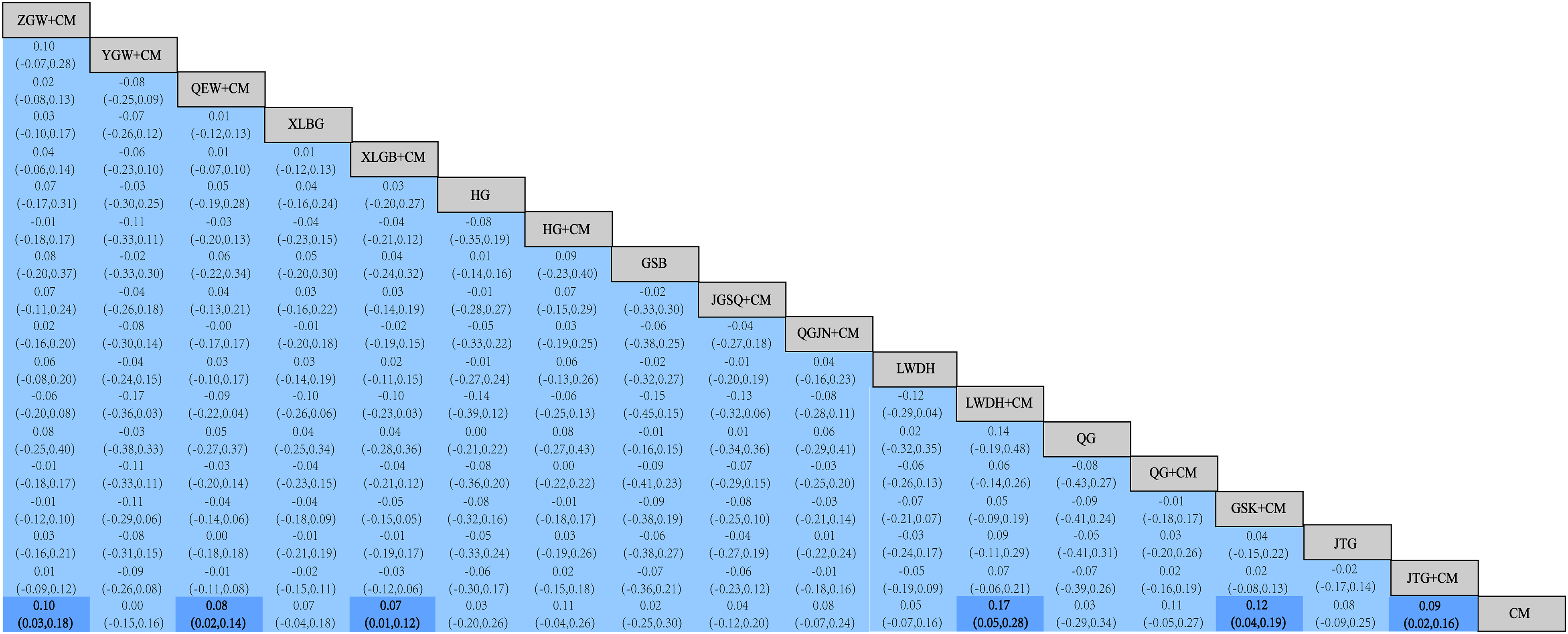
Network meta-analysis of the effects of lumbar spine BMD.
Femoral Neck BMD
Network of Evidence
In total, femoral neck BMD was reported in 26 articles,13,14,17,20‐22,29,32‐37,39,41‐47,52‐55 with 7 CPMs and a total sample size of 2364. The evidence network centered around the CM had no closed loops in the interventions; therefore, no inconsistency check was required (Figure 3).
Conventional Meta-Analysis
According to the evidence network diagram, direct comparisons were made between CPM combined with CM and CM alone. Owing to the high heterogeneity in the comparisons, sensitivity analysis could not decrease the heterogeneity. Therefore, the effect values were not merged, and only a general descriptive analysis was conducted. The random-effects model revealed that, except for LWDH, XLGB, and XLGB combined with CM, which exhibited no significant difference compared with CM in increasing femoral neck BMD, the other CPMs combined with CM significantly improved femoral neck BMD compared with CM alone (Figure S3).
Network Meta-Analysis
Network meta-analysis revealed 45 pairwise comparisons of 7 CPM types. For increasing femoral neck BMD, ZGW [WMD = 0.12, 95% CI (0.05, 0.18)], QEW [WMD = 0.05, 95% CI (0.01, 0.10)], LWDH [WMD = 0.23, 95% CI (0.11, 0.35)], GSK [WMD = 0.11, 95% CI (0.05, 0.18)], and JTG [WMD = 0.11, 95% CI (0.05, 0.17)] combined with CM were more effective than CM alone. Compared with QEW and XLGB combined with CM and XLGB combined with LWDH, LWDH combined with CM was more effective at increasing femoral neck BMD (P < 0.05). However, no significant differences were observed in the efficacy of the other interventions (Figure 6).
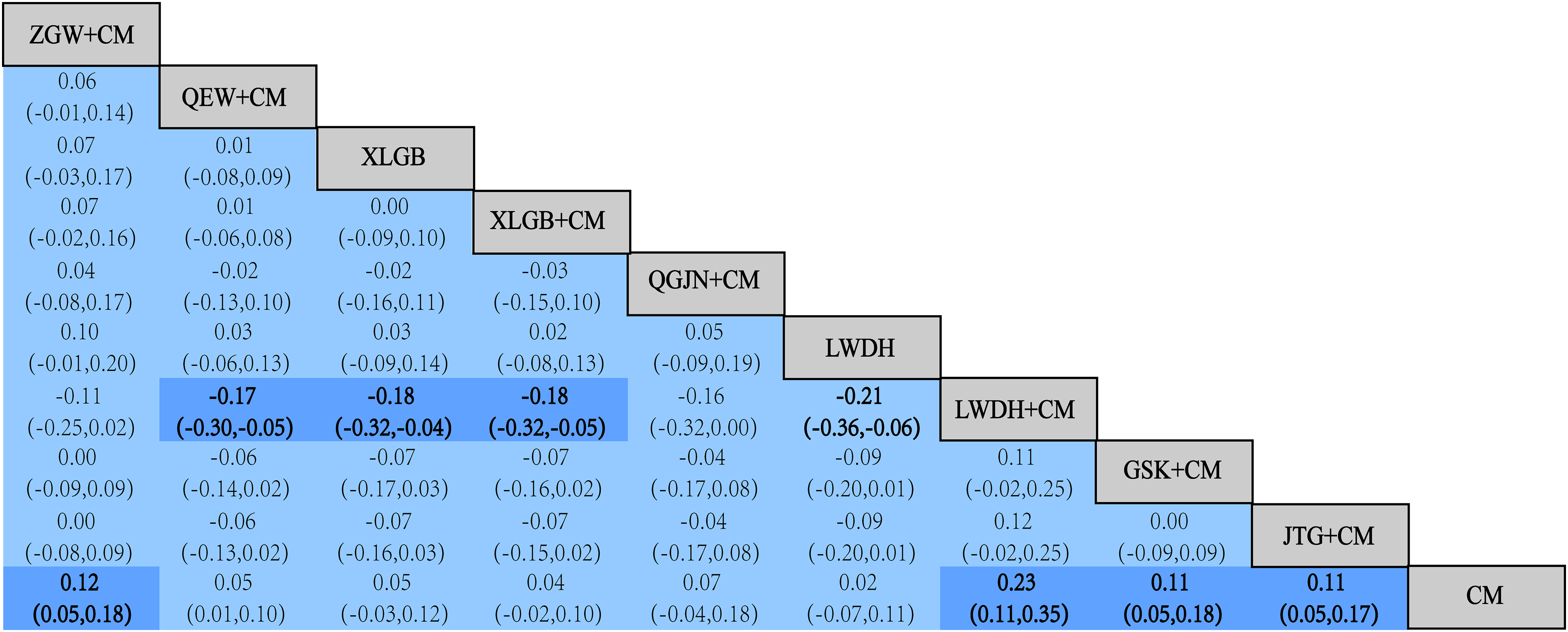
Network meta-analysis of the effects of femoral neck BMD.
VAS Score
Network of Evidence
VAS scores were reported in 18 articles,17,21‐23,29,30,32,38,40,44,46,47,50,51,56 with 1963 participants and 11 CPM types. The evidence network centered around the CM had no closed loops in the interventions; therefore, no inconsistency test was required (Figure 3).
Conventional Meta-Analysis
Based on the network evidence map, most of the direct comparisons were observed between combined CPM and CM, with some additional comparisons between XLGB and HG. However, owing to the high heterogeneity in these comparisons, sensitivity analysis failed to decrease the heterogeneity; therefore, the effect values were not combined, and only descriptive analysis was performed. The random-effects model revealed that GSK, QG, QEW, XLGB, HG, ZGW, JGSQ, JTG, and LWDH combined with CM and XLGB alone were more effective than CM alone in decreasing the VAS score (P < 0.05). However, the difference between XLGB and HG was not statistically significant. Finally, other TCMs combined with CM exhibited similar efficacy in decreasing VAS scores compared with CM alone (Figure S4).
Network Meta-Analysis
In total, 91 pairwise comparisons were generated for 11 CPMs. Network meta-analysis revealed that ZGW [WMD = −1.75, 95% CI (−2.44, −1.06)], YGW [WMD = 0.23, 95% CI (−0.74, 1.20)], QEW [WMD = −1.03, 95% CI (−1.59, −0.46)], XLGB [WMD = −1.52, 95% CI (−2.07, −0.97)], HG [WMD = −1.44, 95% CI (−1.95, −0.92)], JGSQ [WMD = −2.27, 95% CI (−3.41, −1.13)], QGJN [WMD = −0.85, 95% CI (−2.00, 0.30)], LWDH [WMD = −1.77, 95% CI (−2.62, −0.92)], QG [WMD = −1.05, 95% CI (−1.97, −0.13)], GSK [WMD = −1.63, 95% CI (−2.18, −1.09)], and JTG [WMD = −0.99, 95% CI (−1.69, −0.29)] combined with CM and XLGB [WMD = −2.20, 95% CI (−3.28, −1.12)] and HG [WMD = −2.48, 95% CI (−3.85, −1.11)] were superior to CM alone in decreasing VAS scores. Furthermore, ZGW, QEW, XLGB, HG, JGSQ, LWDH, GSK, and JTG combined with CM and XLGB and HG exhibited statistically significant differences compared with YGW combined with CM; however, the differences were not statistically significant for the efficacy of other pairwise comparisons of CPMs (Figure 7).

Network meta-analysis of the effects of VAS score.
ALP
Network of Evidence
ALP was reported in 16 articles,14,15,17,19,23,24,28,30,32,33,35,39,49,52,54,55 with 9 CPMs and a total sample size of 2163 ALP. The evidence network centered on CM, with no closed loops between the interventions; therefore, no inconsistency check was required (Figure 3).
Conventional Meta-Analysis
According to the evidence network diagram, most of the direct comparisons were observed for CPM combined with CM and CM alone. Furthermore, direct comparisons were made between GSB and HG and between GSB and QG, as well as between JTG combined with CM and JTG. However, owing to the high heterogeneity in the comparisons, sensitivity analysis failed to decrease the heterogeneity. Therefore, the effect values were not combined, and only a general descriptive analysis was conducted. The random-effects model revealed that LWDH combined with CM and QG exhibited greater effectiveness than CM alone and could effectively decrease serum ALP levels. The differences between GSB and HG and between JTG combined with CM and CM were considered to be statistically significant. Furthermore, no statistically significant difference was reported between QG and GSB. In addition, the combination of other CPMs with routine treatment was comparable to the application of Western medicine alone in decreasing ALP levels (Figure S5).
Network Meta-Analysis
In total, 91 pairwise comparisons were generated for 9 CPMs. Network meta-analysis revealed that ZGW [WMD = 26.36, 95% CI (6.36, 46.36)] and XLGB [WMD = 19.59, 95% CI (1.55, 37.63)] combined with CM exerted better effects than GSB alone on decreasing serum ALP levels. Furthermore, compared with LWDH combined with CM and ZGW [WMD = 23.35, 95% CI (9.68, 37.01)], XLGB [WMD = 16.58, 95% CI (5.98, 27.17)], and JGSQ [WMD = 14.76, 95% CI (0.72, 28.79)] combined with CM were more effective at decreasing serum ALP levels. Moreover, ZGW [WMD = 23.43, 95% CI (6.23, 40.63)] and XLGB [WMD = 16.66, 95% CI (1.78, 31.54)] combined with CM were better than QG alone. ZGW and GSK combined with CM were better than CM alone, and GSK combined with CM was better than GSK alone. In addition, the combination of JTG, as well as the combination of JTG with GSK, with CM was more effective than the combination of LWDH and CM alone. These comparisons revealed statistically significant differences; however, no statistical significance was reported for comparisons of the efficacy of other CPMs (Figure 8).

Network meta-analysis of the effects of ALP.
Incidence of Adverse Events
Network of Evidence
The incidence of adverse reactions was reported in 12 articles,14,20,22,23,25,26,29,31,32,39,42,45 with 1332 participants and 8 CPM types. Fifty-seven adverse reactions were observed in children, primarily gastrointestinal reactions, dizziness, headache, abdominal discomfort, skin rash, and other manifestations. Table S6 summarizes the details. The evidence network centered on CM, with no closed loops in the interventions; therefore, an inconsistency test was not required (Figure 3).
Conventional Meta-Analysis
Based on the network evidence graph, direct comparisons were made between CPM combined with CM and CM alone. After merging the data, the heterogeneity in the articles was <50%. Therefore, a fixed-effects model was used to analyze the data. The efficacy of JTG, GSK, QG, LWDH, QGJN, HG, QEW, and ZGW in decreasing the incidence of adverse reactions was not significantly different from that of CM alone (Figure S6).
Network Meta-Analysis
In total, 36 pairwise comparisons were generated for 8 CPMs. Network meta-analysis revealed that compared with CM combined with QGJN [RR = −1.79, 95% CI (−4.05, 0.47)], LWDH [RR = −0.74, 95% CI (−2.05, 0.57)], QG [RR = −0.75, 95% CI (−2.12, 0.62)], GSK [RR = −0.71, 95% CI (−1.73, 0.31)] and CM alone [RR = −0.40, 95% CI (−1.11, 0.30)], HG combined with CM significantly decreased the incidence of adverse reactions. Furthermore, the other CPMs combined with CM were comparable to CM alone in decreasing the incidence of adverse reactions (Figure 9).

Network meta-analysis of the effects of the incidence of adverse reactions.
SUCRA Probability Ranking
Table 2 presents the SUCRA probability ranking results of the respective endpoints. The probability of reporting overall efficacy decreased in the following order: QEW combined with CM (97.0%) > YGW combined with CM (75.4%) > LWDH (75.0%) > QGJN combined with CM (65.8%) > HG combined with CM (61.8%) > JTG combined with CM (59.9%) > XLGB combined with CM (39.3%) > LWDH combined with CM (35.7%) > GSK combined with CM (24.1%) > JTG (14.9%) > CM (1.7%).
SUCRA Probability Ranking Results for Each Outcome Indicator.

Furthermore, the probability of reporting lumbar spine BMD decreased in the following order: LWDH combined with CM (85.2%) > GSK combined with CM (70.1%) > ZGW combined with CM (65.0%) > HG combined with CM (64.0%) > QG combined with CM (63.7%) > JTG combined with CM (60.0%) > QGJN combined with CM (54.8%) > JTG (52.6%) > XLGB (49.9%) > XLGB combined with CM (45.7%) > QG (40.2%) > LWDH (38.8%) > HG (38.5%) > JGSQ combined with CM (38.0%) > GSB (37.5%) > YGW combined with CM (26.2%) > CM (16.9%).
In addition, the probability of reporting femoral neck BMD decreased in the following order: LWDH combined with CM (97.8%) > ZGW combined with CM (73.2%) > GSK combined with CM (72.9%) > JTG combined with CM (72.4%) > QGJN combined with CM (48.1%) > QEW combined with CM (39.0%) > XLGB (35.0%) > XLGB combined with CM (33.3%) > LWDH (21.5%) > CM (6.8%).
The probability of reporting a decrease in the VAS score decreased as follows: HG (88.3%) > HGSQ combined with CM (84.8%) > XLGB (81.5%) > LWDH combined with CM (68.4%) > ZGW combined with CM (68.0%) > GSK combined with CM (62.7%) > XLGB combined with CM (57.0%) > HG combined with CM (52.1%) > QG combined with CM (35.5%) > QEW combined with CM (32.1%) > JTG combined with CM (31.1%) > QGJN combined with CM (29.1%) > CM (5.9%) > YGW combined with CM (3.6%).
The probability of reporting a decrease in the serum ALP concentration decreased in the following order: GSB (90.7%) > LWDH combined with CM (86.2%) > QG (84.6%) > HG (65.4%) > XLGB (58.0%) > JTG combined with CM (52.0%) > CM (49.5%) > LWDH (45.1%) > JGSQ combined with CM (40%) > XLGB combined with CM (49.5%) > JTG (26.6%) > ZGW combined with CM (12.3%) > GSK combined with CM (8.7%).
The probability of reporting adverse reactions decreased in the following order: HG combined with CM (86.4%) > CM (66.9%) > ZGW combined with CM (55.5%) > QG combined with CM (48.2%) > GSK combined with CM (47.8%) > LWDH combined with CM (47.6%) > JTG combined with CM (42.5%) > QEW combined with CM (36.7%) > QGJN combined with CM (18.4%).
Publication Bias
For the outcome measures with a sample size of ≥10 articles, a “comparison-corrected” funnel plot was constructed for bias assessment (Figure 10). The dots on the funnel plot represent pairwise comparisons between two drugs. Furthermore, the colors of the dots represent different drugs, and the number of dots of a particular color represents the number of RCTs included in the analysis. In the absence of a small sample size or publication bias, the dots on the funnel plot were symmetrically and evenly distributed on both sides of the vertical line (X = 0). We observed that the effect sizes of total effective rate, lumbar spine BMD, femoral neck BMD, and adverse reaction incidence were symmetrically distributed around the zero line, suggesting a low risk of bias. However, the funnel plots for the remaining outcome measures were asymmetric with slopes, suggesting small sample effects or publication bias (Figure S7). In addition, the Egger's test P values for the VAS score and ALP concentration were 0.880 and 0.588, respectively; this indicates a small probability of publication bias. Nevertheless, the funnel plots for VAS scores and ALP exhibited differences; therefore, the possibility of publication bias cannot be ruled out.

Comparison-correction funnel plots for total effective rate (A), lumbar spine BMD (B), femoral neck BMD (C), and adverse reaction incidence (D).
Discussion
OP is a common skeletal condition that imposes a significant economic burden on patients and society owing to its high disability and mortality rates, often leading to fragility fractures owing to bone loss.57,58 Although existing anti-OP drugs are effective, they can cause adverse gastrointestinal reactions and nosebleeds and increase the risk of deep vein thrombosis. Accordingly, seeking a treatment plan with fewer adverse reactions and greater safety is vital. Modern studies have revealed that CPM has the advantages of convenience and stable therapeutic effects, enhancing the therapeutic effect of OP; this finding is consistent with the multifactorial nature of this condition and can help decrease the toxic side effects associated with the use of Western medicine. However, with the increasing number of CPM treatments, most studies have focused only on the therapeutic effects of specific CPMs, and comprehensive comparisons are lacking. For clinical doctors, a topic of concern is the selection of more effective and safer drugs for OP treatment from various CPM products. Therefore, in the present study, we applied network meta-analysis as a systematic evaluation method to statistically evaluate the total effective rate, lumbar spine BMD, femoral neck BMD, VAS scores, ALP, and adverse reactions as clinical indicators for different CPMs for OP treatment to provide a basis for medication in clinical settings.
In this study, we conducted a network meta-analysis, included 44 RCTs with widespread baseline characteristics and evaluated the effectiveness and safety of 12 CPMs across 6 outcome measures. Network meta-analysis revealed that QEW was ranked first for increasing the overall effective rate, followed by YGW and LWDH. Furthermore, LWDH was ranked first for increasing lumbar spine BMD, followed by GSK and ZGW. LWDH was also ranked first for increasing femoral neck BMD, followed by ZGW and GSK. In addition, HG was ranked first for decreasing VAS scores, followed by JGSQ and XLGB. Finally, GSB was ranked first for decreasing serum ALP levels, followed by LWDH and QG.
Measuring the BMD of the axial bones (lumbar spine, femoral neck, or total hip) with DXA is vital for evaluating changes in patients with POP before and after treatment. In terms of the lumbar spine and femoral neck BMD, the three CPMs with the greatest efficacy were the LWDH, GSK, and ZGW. Comparisons revealed that all three CPMs contained Rehmanniae Radix Preparata in their formula. In China and other Asian countries, Rehmanniae Radix Praeparata, which is derived from the root of the Scrophulariaceae plant Rehmannia, has been applied with other herbs to treat OP for more than 2000 years. 59 Extensive research suggests the importance of the Wnt/β-catenin signaling pathway in osteoblast maturation and bone formation. 60 In the absence of Wnts, GSK-3β primarily phosphorylates the downstream target β-catenin. Wnt3a binds to the coreceptors Frizzleed and LRP5/6. Accordingly, it induces β-catenin phosphorylation, with LRP5/6 stabilization in the cytoplasm. Nevertheless, GSK-3β can be inhibited, resulting in β-catenin accumulation. Therefore, β-catenin is translocated to the nucleus, where it can bind to TCF/LEF; as a result, downstream target genes are activated, facilitating osteoblast differentiation and proliferation.61,62 Dkk1 and sclerostin can inhibit the Wnt/β-catenin signaling pathway, decreasing osteoblast activity as well as bone formation, thereby causing OP.63,64 Studies have suggested that Rehmanniae Radix Praeparata can inhibit DKK1 and sclerostin expression in castrated rats with OP, thereby decreasing the ratio of phosphorylated β-catenin to total β-catenin, increasing the nuclear translocation of β-catenin, activating TCF/LEF transcription factors, and activating the downstream target gene Runx2, thus exerting osteogenic activity. 65 Catalpol, one of the major active ingredients in the TCM agent Rehmannia glutinosa, exhibits various pharmacological activities, including anti-inflammatory, antioxidant, and anti-OP effects. Zhu et al 66 have suggested to facilitate the proliferation of bone marrow stromal stem cells (BMSCs) and prevent ovariectomy-induced bone loss. The authors reported that the osteogenic effect of Catalpol was correlated with Wnt/β-catenin pathway activation because coculture with DKK-1 partially inhibited BMSC osteogenesis. Moreover, as indicated by the results, LWDH exhibited remarkable superiority in increasing lumbar spine and femoral neck BMD because it is a refined prescription comprising Rehmanniae Radix Praeparata, Corni Fructus, Dioscoreae Rhizoma, Alismatis Rhizoma, Moutan Cortex, and Poria. Notably, Liuwei Dihuang Pill, primarily composed of Rehmanniae Radix Praeparata, can activate the Wnt/β-catenin signaling pathway by upregulating the expression of β-catenin and the osteogenic transcription factors Runx2 and Osterix in rats with OP. 67 Nevertheless, existing research on OP has focused considerably on increasing patients’ BMD and decreasing fracture incidence, with the effect of chronic pain on patients’ quality of life being ignored. The VAS score, a pain indicator, indicated that HG was the top treatment; this may be associated with its ability to facilitate bone healing and strengthening. OP decreases bone strength and increases fragility, increasing the susceptibility of microfractures to minor external forces. After bone damage occurs, a series of inflammatory reactions can occur in the surrounding tissue, releasing various pain mediators, including prostaglandin E2,5-hydroxytryptamine, and kinins; these reactions exert some effect on peripheral nociceptors and confer great significance to peripheral pain hypersensitivity. The upregulation of these mediators can increase the sensitivity of neurons to pain-inducing substances.68,69 Studies have revealed that the main ingredient in bone glue, ie, total flavonoids, not only significantly inhibited the decrease in bone density in castrated rats with OP but also inhibited the release of pain mediators such as prostaglandin E2 and 5-hydroxytryptamine, thereby playing an analgesic role. 70 Regarding adverse reactions, adverse reactions to various drug treatments are rare, and these treatments are highly safe. No serious adverse reactions were reported in any of the studies, and most studies revealed mild gastrointestinal reactions, including nausea, vomiting, and abdominal discomfort, as adverse reactions. These symptoms can be alleviated by discontinuing treatment, resting, or undergoing basic symptomatic treatment. Our study results suggest that clinical practitioners select different CPMs or combinations of conventional Western drugs according to the different clinical symptoms and severity of POP to achieve the best therapeutic effect.
Previous research has conducted comparative analyses on the efficacy and safety of various CPMs for the treatment of POP. These studies have assessed a range of clinical outcomes and laboratory parameters, including quality of life, incidence of severe adverse reactions, bone mineral density, clinical efficacy, estradiol levels, and serum calcium concentrations. The findings demonstrate that Chinese patent medicines exhibit significant efficacy in the treatment of osteoporosis. 71 In this study, we compared the efficacy and safety of 12 CPMs combined with CM for POP treatment by performing a network meta-analysis. Our findings provide some degree of rational, targeted, and individualized medication guidance for treating patients with POP in clinical settings. However, this study also has several limitations. First, some articles did not provide information on randomization, blinding, or allocation concealment, possibly decreasing the validity of the research results. Second, heterogeneity was observed in the articles. Factors such as random allocation method, sample size, treatment course, index detection method, and disease stage may affect the accuracy of the results. Third, because the number of included articles was limited, some outcome indicators did not include all the CPMs involved; furthermore, only one study was included, possibly affecting the accuracy of the result ranking. Therefore, additional high-quality studies are warranted to further verify the results of the present study. Fourth, owing to the unclear classification and non-standardized data of all the included RCTs, we failed to conduct a subgroup analysis of the primary risk factors that significantly affect POP development, including age, sex, and etiology. Finally, the SUCRA curve was utilized to estimate the ranking probability of the effectiveness comparisons among different CPMs; however, limitations remained, and the results should be interpreted with caution.
Conclusion
LWDH achieved the most effective results for increasing lumbar spine and femoral neck BMD, whereas HG exhibited the optimal effect in relieving pain. Although our study has several limitations, it provides a reasonable overview and recommendations for applying POP drugs in clinical settings. In the future, the combination of CPM and CM to prevent and treat POP may serve as an effective option owing to its high safety profile and high therapeutic benefits. Accordingly, additional large-sample, multicenter, double-blind, high-quality, and long-term follow-up RCTs, as well as well-designed clinical trials, should be conducted to validate the efficacy of TCM for treating POP. As a result, more accurate evidence-based support can be presented to contribute to POP diagnosis and treatment in clinical settings.
Materials and Methods
Study Protocol and Registration
The present meta-analysis was conducted and reported according to the PRISMA extension statement for reporting systematic reviews involving network meta-analyses of healthcare interventions. It has been preregistered on PROSPERO (registration no. CRD42023407426).
Inclusion Criteria
(a) Study types: Published clinical RCTs limited to the Chinese and English languages.
(b) Participant types: Patients diagnosed with POP according to the criteria of the Chinese Society of Osteoporosis and Bone Mineral Research, 2 with no restrictions on age, sex, or location.
(c) Intervention types: The experimental group was administered CPMs approved for POP treatment by the drug regulatory authority (according to the Clinical Application Guidelines for Chinese Patent Medicine in the Treatment of Osteoporosis) 72 combined with conventional medicine (CM) or without it. The dosage, administration, and duration were not limited. The control group was administered conventional anti-OP drugs, including bisphosphonates, calcitonin, estrogen, and strontium salt, or Chinese herbal medicine (unlike the experimental group). Both groups consistently received other treatments, including lifestyle adjustments and basic calcium and vitamin D supplementation, which are associated with bone health. The dosage, administration, and duration of the abovementioned interventions were not limited. Neither group received additional TCM treatments, such as Chinese medicine injections, external Chinese medicine applications, medicated baths, acupuncture, or massage.
(d) Outcome types: The primary outcomes were the total effective rate, visual analog scale (VAS) score, and bone mineral density (BMD) of the lumbar spine and femur. On the other hand, the secondary outcomes were alkaline phosphatase (ALP) and the incidence of adverse reactions. Notably, the inclusion of one of the abovementioned outcomes was considered sufficient.
Exclusion Criteria
(a) Studies without an RCT design; (b) articles on nonconventional Western medicine interventions; (c) articles without the abovementioned outcomes; (d) articles with incomplete or inaccurate data; (d) repeated publications; however, the ones providing the most sufficient information were retained; (f) incomplete full text; and (g) conference reports, case reports, animal experiments, cell and tissue studies, and systematic reviews.
Literature Search
From March 5, 2004, to March 5, 2024, the CNKI, VIP, Wanfang, PubMed, Embase, Web of Science, and Cochrane Central Register of Controlled Trials databases were searched. The search items were designed based on a combination of Medical Subject Headings and free words. Different search strategies were used for different databases. Tables S1–5 summarize the search strategies used in the abovementioned databases.
Study Selection and Data Extraction
The literature search was independently conducted by four reviewers (QLP, RQW, YKW, and YL). Duplicate publications were screened using Endnote X9 software. The titles and abstracts of the retrieved articles were read to exclude irrelevant articles. Thereafter, the full texts of the remaining articles were read to identify eligible articles. Using Excel 2019, two reviewers independently extracted the data. The following data were extracted: baseline characteristics, factors correlated with risk of bias, interventions, treatment courses, and outcomes. Finally, the fifth reviewer (JH) verified the data. For mistakes, disagreements, and missing or unrecorded data, the authors were contacted to collect the original data.
Quality Evaluation of the Included Articles
The quality of the included articles was independently evaluated by four reviewers (QLP, RQW, YKW, and FC). The Risk of Bias Evaluation Tool recommended in The Cochrane Handbook 73 was used. It comprises seven domains: randomization sequence generation, allocation concealment, participant and personnel blinding, outcome evaluation blinding, incomplete data, selective reporting, and other biases. Each domain can be graded as follows: “low risk,” “high risk,” or “unclear risk.” After data extraction, the results were validated by two reviewers. Any disagreements were resolved by discussion or consultation with a third reviewer.
Statistical Analysis
Stata 15.1 software was used to perform the conventional meta-analysis. Dichotomous variables are expressed as relative risk (RR), whereas continuous data are expressed as the mean difference (MD). Furthermore, the effect size of each variable was indicated using a 95% confidence interval (95% CI). I2 ≤ 50 and p value > 0.1 indicated no significant heterogeneity; therefore, a fixed-effects model was utilized. In contrast, I2 > 50 and p value ≤ 0.1 indicated significant heterogeneity. The source of heterogeneity was investigated via sensitivity and subgroup analyses. A random-effects model was used to perform the data analysis. If severe heterogeneity was observed in the included articles, only descriptive analysis was conducted.
Stata 15.1 was used to conduct network meta-analysis. The correlations among the interventions were revealed by plotting a network diagram of the evidence; then, a league table was generated. The data in the table are presented as RR/MD with 95% CI of the direct pairwise comparisons of the different interventions. If the 95% CI was 0/1, the results were considered insignificant. RR > 1 or MD < 0 indicated greater effectiveness of the row intervention than the column intervention; otherwise, the column intervention was preferred. Moreover, the surface under the cumulative ranking (SUCRA) of the respective interventions was determined, with a larger SUCRA indicating a more effective intervention. A comparison-adjusted funnel plot was generated. Articles with large sample sizes and high precision were distributed at the top and clustered such that the combined effect size was in the center. In contrast, articles with small sample sizes and low precision were symmetrically distributed at the bottom. Funnel plots and Egger's test were used to evaluate publication bias. A roughly symmetrical funnel plot and Egger's test p value > 0.05 indicated no evident publication bias. The quality of the included articles and the risk of bias were evaluated and presented using RevManv 5.4.
Supplemental Material
sj-docx-1-npx-10.1177_1934578X241271671 - Supplemental material for Comparison of the Efficacy and Safety of 12 Chinese Patent Medicines for Treating Primary Osteoporosis Patients: A Systematic Review and Network Meta-Analysis
Supplemental material, sj-docx-1-npx-10.1177_1934578X241271671 for Comparison of the Efficacy and Safety of 12 Chinese Patent Medicines for Treating Primary Osteoporosis Patients: A Systematic Review and Network Meta-Analysis by Qinglin Peng, Jie Han, Ruiqi Wu, Yukun Wu, Feng Chen and Yu Lai in Natural Product Communications
Supplemental Material
sj-docx-2-npx-10.1177_1934578X241271671 - Supplemental material for Comparison of the Efficacy and Safety of 12 Chinese Patent Medicines for Treating Primary Osteoporosis Patients: A Systematic Review and Network Meta-Analysis
Supplemental material, sj-docx-2-npx-10.1177_1934578X241271671 for Comparison of the Efficacy and Safety of 12 Chinese Patent Medicines for Treating Primary Osteoporosis Patients: A Systematic Review and Network Meta-Analysis by Qinglin Peng, Jie Han, Ruiqi Wu, Yukun Wu, Feng Chen and Yu Lai in Natural Product Communications
Footnotes
Acknowledgments
Everyone who contributed significantly to this study has been listed.
Author Contributions
Conceptualization: Qinglin Peng; Resources: Yu Lai, Feng Chen; Methodology: Yukun Wu; Formal analysis and investigation: Ruiqi Wu; Writing - original draft preparation: Ruiqi Wu and Qinglin Peng; Writing - review and editing: Jie Han; Funding acquisition: Jie Han; Supervision: Yukun Wu,Jie Han. All authors read and approved the final manuscript.
Availability of Data and Materials
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
National Natural Science Foundation of China Project (82260858); Guangxi Natural Science Foundation (2024GXNSFAA010243); Pilot project for the construction of high-level key disciplines of traditional Chinese medicine in Guangxi (Guizhong Medical Science and Education Development [2023] No. 13); The construction project of Guangxi Key Research Laboratory of Traditional Chinese Medicine (Guizhong Pharmaceutical Science and Education Development [2023] No. 9); Guangxi Youth Qihuang Scholar Training Program (Guizhong Medical Science and Education Development [2022] No. 13); Guangxi University of Traditional Chinese Medicine “Qihuang Project” High level Talent Team Cultivation Project (202413).
Ethical Approval
This study was approved by the Medical Ethics Committee of Ruikang Hospital Affiliated to Guangxi University of Chinese Medicine (YJS2021-013)*, Guangxi Zhuang Autonomous Region, China.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
There are no human subjects in this article and informed consent is not applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.